
Abstract
Background
Implantation of the atrial flow regulator (AFR) to create an interatrial left-to-right shunt has been shown to be safe and feasible to reduce intracardiac filling pressures in patients with heart failure (HF).
Objectives
We aimed to assess the effect of AFR implantation on 12-month mortality and hospitalization rates in patients with reduced (HFrEF) or preserved HF (HFpEF).
Methods
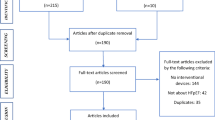
One-year follow-up data from 34 subjects enrolled at a single PRELIEVE center were analyzed. The 12-month predicted mortality was calculated using the Meta-Analysis Global Group in Chronic Heart Failure (MAGGIC) risk score. Patients were divided into two groups, according to their history of hospitalizations for HF.
Results
Study data of 34 patients (HFrEF: 24 [70.6%]; HFpEF: 10 [29.4%]) were assessed. Median follow-up duration was 355 days. In total, 14 (41.2%) patients were hospitalized during the follow-up period and 6 (17.6%) of these patients were hospitalization for HF (HHF). A total of 24 hospitalizations occurred in this period and 8 (33%) hospitalizations were for HHF. The median baseline MAGGIC score was 23 and the median predicted mortality was 13.4/100 patient years. Observed mortality was 3.1/100 patient years. The observed survival (97%) was 10.3% (95% confidence interval 3.6–17.5%, p = 0.004) better than the predicted survival (86.6%).
Conclusion
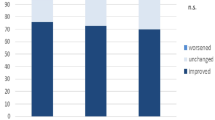
Our results suggest that AFR implantation has favorable effects on mortality in patients with heart failure, regardless of ejection fraction. Furthermore, compared to baseline, left ventricular filling pressure (assessed by echocardiography) decreased significantly without right side volume overload at the 1‑year follow-up.
Zusammenfassung
Hintergrund
Die Implantation eines Atrial Flow Regulator (AFR), um einen interatrialen Links-Rechts-Shunt zu erzeugen, hat sich als sicher und machbar erwiesen, um den intrakardialen Füllungsdruck bei Patienten mit Herzinsuffizienz zu verringern.
Ziele
Das Ziel war, den Einfluss der AFR-implantation auf die 12-Monats-Sterblichkeit und die Hospitalisierungsrate bei Patienten mit einer Herzinsuffizienz mit reduzierter (HFrEF) oder erhaltener Ejektionsfraktion (HFpEF) festzustellen.
Methoden
Dafür wurden die Nachbeobachtungsdaten von 34 an der PRELIEVE-Studie beteiligten Personen in einem Zentrum über einen Zeitraum von 12 Monaten analysiert. Die Einjahresmortalität wurde mit dem MAGGIC-Risk-Score (Meta-Analysis Global Group in Chronic Heart Failure) berechnet. Die Patienten wurden entsprechend den vorangegangenen Krankenhausaufenthalten wegen Herzinsuffizienz in zwei Gruppen unterteilt.
Ergebnisse
Es wurden die Studiendaten von 34 Patienten (HFrEF: 24 [70,6 %]; HFpEF: 10 [29,4 %]) ausgewertet. Der mittlere Nachbeobachtungszeitraum betrug 355 Tage. Insgesamt kam es bei 14 (41,2 %) Patienten in dem Nachbeobachtungszeitrum zu Klinikeinweisungen, bei 6 (17,6 %) dieser Patienten war Herzinsuffizienz der Grund für die Hospitalisierung. Insgesamt gab es in diesem Zeitraum 24 Klinikaufenthalte, bei 8 (33 %) war der Grund Herzinsuffizienz. Das mittlere baseline-Risiko des MAGGIC-Score lag bei 23 und der Median der prognostizierten Mortalität bei 13,4/100 Patientenjahre. Die beobachtete Mortalität lag bei 3,1/100 Patientenjahre. Das beobachtete Überleben (97 %) war 10,3 % (95 % Konfidenzintervall: 3,6–17,5 %, p = 0,004) besser als das prognostizierte Überleben (86,6 %).
Schlussfolgerung
unsere Ergebnisse legen nahe, dass sich die AFR-implantation unabhängig von der Ejektionsfraktion günstig auf die Sterblichkeit bei Patienten mit Herzinsuffizienz auswirkt. Überdies nahm im Vergleich zur Baseline bei der Nachuntersuchung nach einem Jahr der linksventrikuläre Füllungsdruck (durch Echokardiographie gemessen) deutlich ab, ohne eine rechtsventrikuläre Volumenüberlastung zu verursachen.




Similar content being viewed by others

References
Tomasoni D, Adamo M, Anker MS, von Haehling S, Coats AJ, Metra M (2020) Heart failure in the last year: progress and perspective. ESC Heart Fail 7(6):3505–3530. https://doi.org/10.1002/ehf2.13124
Ahmed A, Allman RM, Fonarow GC, Love TE, Zannad F, Dell’Italia LJ, White M, Gheorghiade M (2008) Incident heart failure hospitalization and subsequent mortality in chronic heart failure: a propensity-matched study. J Card Fail 14(3):211–218
Teo K, Montague T, Ackman M, Barnes M, Taylor C, Mansell G, Greenwood P, Prosser A, Tsuyuki R, Nilsson C (1996) Mortality risk and patterns of practice in 4606 acute care patients with congestive heart failure – the relative importance of age, sex, and medical therapy. Arch Intern Med 156(15):1669–1673
Heywood JT, Jermyn R, Shavelle D, Abraham WT, Bhimaraj A, Bhatt K, Sheikh F, Eichorn E, Lamba S, Bharmi R (2017) Impact of practice-based management of pulmonary artery pressures in 2000 patients implanted with the CardioMEMS sensor. Circulation 135(16):1509–1517
Adamson PB (2009) Pathophysiology of the transition from chronic compensated and acute decompensated heart failure: new insights from continuous monitoring devices. Curr Heart Fail Rep 6(4):287
Cotter G, Metra M, Milo-Cotter O, Dittrich HC, Gheorghiade M (2008) Fluid overload in acute heart failure—re-distribution and other mechanisms beyond fluid accumulation. Eur J Heart Fail 10(2):165–169
Emani S, Burkhoff D, Lilly SM (2020) Interatrial shunt devices for the treatment of heart failure. Trends Cardiovasc Med. https://doi.org/10.1016/j.tcm.2020.09.004
De Rosa R, Schranz D (2018) Creation of a restrictive atrial left-to-right shunt: a novel treatment for heart failure. Heart Fail Rev 23(6):841–847
Paitazoglou C, Özdemir R, Pfister R, Bergmann MW, Bartunek J, Kilic T, Lauten A, Schmeisser A, Zoghi M, Anker S, Sievert H, Mahfoud F (2019) The AFR-PRELIEVE trial: a prospective, non-randomised, pilot study to assess the Atrial Flow Regulator (AFR) in heart failure patients with either preserved or reduced ejection fraction. EuroIntervention 15(5):403–410. https://doi.org/10.4244/EIJ-D-19-00342
Kaye DM, Petrie MC, McKenzie S, Hasenfuβ G, Malek F, Post M, Doughty RN, Trochu JN, Gustafsson F, Lang I (2019) Impact of an interatrial shunt device on survival and heart failure hospitalization in patients with preserved ejection fraction. ESC Heart Fail 6(1):62–69
Harper RW, Mottram PM, McGaw DJ (2002) Closure of secundum atrial septal defects with the Amplatzer septal occluder device: techniques and problems. Cathet Cardiovasc Intervent 57(4):508–524
Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) (2012) The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. Eur Heart J 33(14):1750–1757
Pocock SJ, Ariti CA, McMurray JJ, Maggioni A, Køber L, Squire IB, Swedberg K, Dobson J, Poppe KK, Whalley GA (2013) Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J 34(19):1404–1413
Zuckerman RB, Sheingold SH, Orav EJ, Ruhter J, Epstein AM (2016) Readmissions, observation, and the hospital readmissions reduction program. N Engl J Med 374(16):1543–1551
Dunlay SM, Redfield MM, Weston SA, Therneau TM, Long KH, Shah ND, Roger VL (2009) Hospitalizations after heart failure diagnosis: a community perspective. J Am Coll Cardiol 54(18):1695–1702
Malik A, Gill GS, Lodhi FK, Tummala LS, Singh SN, Morgan CJ, Allman RM, Fonarow GC, Ahmed A (2020) Prior heart failure hospitalization and outcomes in patients with heart failure with preserved and reduced ejection fraction. Am J Med 133(1):84–94
Green CP, Porter CB, Bresnahan DR, Spertus JA (2000) Development and evaluation of the Kansas City Cardiomyopathy Questionnaire: a new health status measure for heart failure. J Am Coll Cardiol 35(5):1245–1255
Joseph SM, Novak E, Arnold SV, Jones PG, Khattak H, Platts AE, Dávila-Román VG, Mann DL, Spertus JA (2013) Comparable performance of the Kansas City Cardiomyopathy Questionnaire in patients with heart failure with preserved and reduced ejection fraction. Circ Heart Fail 6(6):1139–1146
Soto GE, Jones P, Weintraub WS, Krumholz HM, Spertus JA (2004) Prognostic value of health status in patients with heart failure after acute myocardial infarction. Circulation 110(5):546–551
Pokharel Y, Khariton Y, Tang Y, Nassif ME, Chan PS, Arnold SV, Jones PG, Spertus JA (2017) Association of serial Kansas City Cardiomyopathy Questionnaire assessments with death and hospitalization in patients with heart failure with preserved and reduced ejection fraction: a secondary analysis of 2 randomized clinical trials. JAMA Cardiol 2(12):1315–1321
Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, Kocovic DZ, Packer M, Clavell AL, Hayes DL (2002) Cardiac resynchronization in chronic heart failure. N Engl J Med 346(24):1845–1853
Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, Garrigue S, Kappenberger L, Haywood GA, Santini M (2001) Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med 344(12):873–880
Abraham WT, Zile MR, Weaver FA, Butter C, Ducharme A, Halbach M, Klug D, Lovett EG, Müller-Ehmsen J, Schafer JE (2015) Baroreflex activation therapy for the treatment of heart failure with a reduced ejection fraction. JACC Heart Fail 3(6):487–496
Ferreira JP, Duarte K, Graves TL, Zile MR, Abraham WT, Weaver FA, Lindenfeld J, Zannad F (2016) Natriuretic peptides, 6‑min walk test, and quality-of-life questionnaires as clinically meaningful endpoints in HF trials. J Am Coll Cardiol 68(24):2690–2707
Ritzema JL, Richards AM, Crozier IG, Frampton CF, Melton IC, Doughty RN, Stewart JT, Eigler N, Whiting J, Abraham WT (2011) Serial Doppler echocardiography and tissue Doppler imaging in the detection of elevated directly measured left atrial pressure in ambulant subjects with chronic heart failure. JACC Cardiovasc Imaging 4(9):927–934
Hirata K, Hyodo E, Hozumi T, Kita R, Hirose M, Sakanoue Y, Nishida Y, Kawarabayashi T, Yoshiyama M, Yoshikawa J (2009) Usefulness of a combination of systolic function by left ventricular ejection fraction and diastolic function by E/E’ to predict prognosis in patients with heart failure. Am J Cardiol 103(9):1275–1279
Sartipy U, Dahlström U, Edner M, Lund LH (2014) Predicting survival in heart failure: validation of the MAGGIC heart failure risk score in 51043 patients from the Swedish Heart Failure Registry. Eur J Heart Fail 16(2):173–179
Acknowledgements
We would like to thank to our cathlab workers for their devoted supports.
Funding
The study was supported by Occlutech International AB.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available in the Clinicaltrials.gov repository, https://clinicaltrials.gov/ct2/show/NCT03030274?term=AFR&draw=2&rank=2.
Code availability
N/A
Author information
Authors and Affiliations
Contributions
NB (designed the analysis, performed the analysis, wrote the paper), İÇ (collected data, contributed data, wrote the paper), EK (designed the study, performed analysis, wrote the paper), AE (designed the study, review, supervision), MU (collected data, review, supervision), RÖ (designed the study, review and editing, supervision).
Corresponding author
Ethics declarations
Conflict of interest
N. Bakhshaliyev, İ. Çelikkale, A. Enhoş, E. Karaçöp, M. Uluganyan and R. Özdemir declare that they have no competing interests.
Study protocol was approved by local ethical committee. All studies performed were in accordance with the ethical standards indicated in each case. Consent for publication: N/A. Consent to participate: Obtained from all participants.
Rights and permissions
About this article

Cite this article
Bakhshaliyev, N., Çelikkale, İ., Enhoş, A. et al. Impact of atrial flow regulator (AFR) implantation on 12-month mortality in heart failure. Herz 47, 366–373 (2022). https://doi.org/10.1007/s00059-021-05063-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-021-05063-w