
Abstract
Background
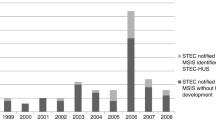
Hemolytic Uremic Syndrome (HUS) was made reportable in British Columbia (BC) in 1998 to detect, control and prevent verotoxigenic Escherichia coli (VTEC) cases. Concerns about under-reporting of HUS cases triggered the assessment of the sensitivity and timeliness of the reporting process in order to guide recommendations around reportability of this syndrome in BC.
Methods
The BC hospitalization database was used to estimate the total number of HUS cases from April 30, 1998 to December 31, 2005. HUS and VTEC cases reported in the integrated Public Health Information System (iPHIS), and HUS cases reported by a surveillance form were linked to hospitalized cases. The proportion of HUS cases detected by each of the surveillance processes was assessed. The time interval between onset of diarrhea and reporting of HUS and VTEC cases to the BC Centre for Disease Control was compared.
Results
57 HUS cases were hospitalized. Sensitivity of reporting through the surveillance form and through iPHIS was 7.0% and 19.3%, respectively. The median time interval between onset of diarrhea and reporting of both HUS and VTEC cases to iPHIS was seven days. The median time interval for reporting HUS cases via the surveillance form was 25 days.
Conclusions
HUS cases were severely under-reported, the timeliness of reporting of these cases had no advantage when compared to the reporting of VTEC cases, and no public health action aimed at reducing the transmission of VTEC infections resulted from this surveillance system. The reportability of HUS in BC needs to be reconsidered, or its surveillance considerably improved.
Résumé
Contexte
Afin de détecter, de traiter et de prévenir les cas d’infection à E. coli producteur de vérotoxine (ECPV), la Colombie-Britannique a rendu obligatoire la déclaration du syndrome hémolytique urémique (SHU) en 1998. Par crainte que les cas de SHU soient sous-déclarés, il a été décidé d’évaluer la sensibilité et l’opportunité du processus de notification en vue de formuler des recommandations sur la déclaration du syndrome dans la province.
Méthode
D’après la base de données des hospitalisations de la C.-B., nous avons estimé le nombre total de cas de SHU survenus entre le 30 avril 1998 et le 31 décembre 2005. Les cas de SHU et d’ECPV déclarés dans le système intégré d’information sur la santé publique (SIISP) et les cas de SHU déclarés sur des fiches de surveillance ont été reliés aux cas hospitalisés. Nous avons calculé la proportion des cas de SHU détectés par chacun des processus de surveillance. Nous avons ensuite comparé l’intervalle entre l’apparition d’une diarrhée et la déclaration des cas de SHU et d’ECPV au BC Centre for Disease Control.
Résultats
Cinquante-sept cas de SHU ont été hospitalisés. La sensibilité des déclarations sur les fiches de surveillance et dans le SIISP était de 7 % et de 19,3 %, respectivement. L’intervalle médian entre l’apparition de la diarrhée et la déclaration des cas de SHU et d’ECPV au SIISP était de sept jours. L’intervalle médian de déclaration des cas de SHU sur les fiches de surveillance était de 25 jours.
Conclusion
Les cas de SHU étaient fortement sous-déclarés, la déclaration des cas de SHU était beaucoup moins rapide que pour les cas d’ECPV, |et le système de surveillance du SHU n’a entraîné aucune mesure de santé publique visant à réduire la transmission des infections à ECPV. Il faudrait soit revoir la pertinence de déclarer les cas de SHU en C.-B., soit améliorer considérablement le système de surveillance du syndrome.
Similar content being viewed by others

References
Proulx F, Sockett P. Prospective surveillance of Canadian children with the haemolytic uraemic syndrome. Pediatr Nephrol 2005;29:786–90.
Cummings KC, Mohle-Boetani JC, Werner SB, Vugia DJ. Population-based trends in pediatric hemolytic uremic syndrome in California, 1994–1999: Substantial underreporting and public health implications. Am J Epidemiol 2002;155(10):941–48.
Chang HGH, Tserenpuntsag B, Kacica M, Smith PF, Morse DL. Hemolytic uremic syndrome incidence in New York. Emerg Infect Dis 2004;10(5):928–31.
Tserenpuntsag B, Chang HG, Smith PF, Morse DL. Hemolytic uremic syndrome risk and Escherichia coli O157:H7. Emerg Infect Dis 2005;11(12):1955–57.
Tarr PI, Gordon CA, Chandler WL. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet 2005;365:1073–86.
McCarthy TA, Barett NL, Hadler JL, Salsbury B, Howard RT, Dingman DW, et al. Hemolytic-Uremic Syndrome and Escherichia coli O121 at a lake in Connecticut, 1999. Pediatrics 2001;108:59–66.
Garg AX, Suri RS, Barrowman N, Rehman F, Matsell D, Rosas-Arellano MP, et al. Long-term renal prognosis of diarrhea-associated hemolytic uremic syndrome: A systematic review, meta-analysis, and meta-regression. JAMA 2003;290(10):1379–81.
Amirlak I, Amirlak B. Haemolytic uraemic syndrome: An overview. Nephrology 2006;11:213–18.
Heyman DL. Control of Communicable Diseases Manual, 18th edition. Washington, DC: American Public Health Association, 2003;160–64.
British Columbia Annual Summary of Reportable Diseases: Annual Report 2005. Vancouver, BC: British Columbia Centre for Disease Control, 2005.
Centers for Disease Control and Prevention. Updated guidelines for evaluating public health surveillance systems: Recommendations from the guidelines working group. MMWR 2001;50(13):1–25.
Begue RE, Mehta DI, Blecker U. Escherichia coli and the hemolytic-uremic syndrome. South Med J 1998;91(9):798–804.
Statistics Canada. Profile series. Profile of age and sex for Canada, provinces, territories, census divisions and census subdivisions: 2001 Census. Ottawa, ON: Statistics Canada, 2002.
Decludt B, Bouvet P, Marian-Kurkdjian P, Grimont F, Grimont PAD, Hubert B, Loirat C. Haemolytic uraemic syndrome and shiga toxin-producing Escherichia coli infection in children in France. Epidemiol Infect 2000;124:215–20.
Author information
Authors and Affiliations
Corresponding author
Additional information
Acknowledgements: British Columbia Ministry of Health, Canadian Field Epidemiology Program, British Columbia Health Authorities staff, British Columbia Centre for Disease Control Laboratory Services.
Rights and permissions
About this article
Cite this article
Laberge, K., Galanis, E. Evaluation of the Surveillance of Hemolytic Uremic Syndrome in British Columbia. Can J Public Health 99, 286–289 (2008). https://doi.org/10.1007/BF03403756
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03403756