
Abstract
The increased risk of sepsis in patients following splenectomy has been well documented. Fear of over-whelming post-splenectomy sepsis (OPSI) has resulted in a generalised trend towards splenic salvage among surgeons. However, splenorrhaphy and attempts at splenic salvage may of themselves predispose to significant morbidity, sometimes more serious than increased susceptibility to infection associated with splenectomy. This study aims to assess the risk of splenectomy and subsequent asplenia.
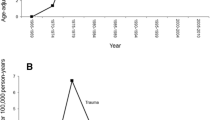
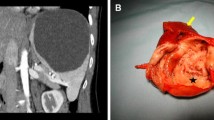
We reviewed 246 patients who underwent splenectomy over a 16 year period. Indications for splenectomy were considered under the following headings: haematological (N = 116), trauma (N = 69), visceral carcinoma (N = 28), incidental (N = 13) and miscellaneous (N = 20).
There were 28 deaths in the series, primarily among those in the intra-abdominal carcinoma (13) and multiple trauma (13) groups. Two deaths were recorded among patients undergoing elective splenectomy for benign disease. Thrombo-embolic complications were recorded in nine patients; respiratory tract infection in 36 patients and intra-abdominal abscess in two patients. Two cases of post-splenectomy pneumococcal septicaemia were documented, neither of which was fatal.
While not an entirely benign procedure, splenectomy can be performed relatively safely, especially when performed for benign disease in an adult population.
Similar content being viewed by others

References
Brooks, D. H. Surgery of the spleen. Surg. Clin. North. Amer. 1975; 55(2): 287–300.
Sherman, R. Rationale for and methods of splenic preservation following trauma. Surg. Clin. North. Amer. 1981; 61 (1): 127–134.
Quittenbaum, K. S. Commentarii de splenie hypertrophie et historia extirpationis. Rostock, 1836.
Kocher, E. T. Textbook of operative surgery (English 3rd. edition), Eds. Stiles, H. J., Paul, C. B., London, A., Black, C. 1911, 565–566.
Pearce, R. M., Krumbhaar, E. B., Frazier, C. H. The history of extirpation of the spleen. In Pearce, R. M. et al, eds., The spleen and anaemia: experimental and clinical studies. Philadelphia; JB Lippincott, 1918; 3–10.
Morris, D. H., Bullock, F. D. The importance of the spleen in the resistance to infection: Ann, Surg. 1919; 70: 513–5.
King, H., Schumacker, H. B. Susceptibility to infection after splenectomy performed in infancy. Ann. Surg. 1952; 136: 239–40.
Diamond, L. K. Splenectomy in childhood and the hazard of overwhelming infection. Pediatrics 1969; 5: 886–9.
Van Wyck D. B. Overwhelming post-splenectomy infection: the clinical syndrome. Lymphology 1983; 16: 107–14.
Singer, D. B. Post-splenectomy sepsis. Perspect. Pediatr. Pathol. 1973; 1: 285.
Horan, M., Colebatch, J. H. Relation between splenectomy and subsequent infection: a clinical study. Arch Dis. Child. 1962; 37: 398.
Walker, W. Splenectomy in childhood: a review of cases in England and Wales, 1960-1964. Br. J. Surg. 1976; 63:36–43.
Shaw, J. H. F., Print, C. G. Post-splenectomy sepsis. Br. J. Surg. 1989; 76: 1074–81.
O’Neal, B. J., McDonald, J. C. The risk of sepsis in the asplenic adult. Ann. Surg. 1981; 194: 775.
Lucas, C. E. Splenic trauma: choice of management. Ann. Surg. 1991; 213(2): 98–112.
Holdsworth, R. J., Irving, A. D., Cuschieri, A. Post-splenectomy sepsis and its mortality rate: actual versus perceived risks. Br. J. Surg. 1991; 78: 1031–8.
Beal, S. L., Spisso, J. M. The risk of splenorrhaphy. Arch. Surg. 1988; 123: 1158–63.
Coil, J. A., Dickerman, J. D.,Boulton, E. Increased susceptibility of splenectomized mice to infection after exposure to an aerosolized suspension of type III streptococcus pneumoniae. Infect. Immunol. 1978; 21: 412–6.
Constantopoulos, A., Najjar, V. A., Wish, J. B., Necheles, T. H., Stolbach, L. L. Defective phagocytosis due to tuftsin deficiency in splenectomized subjects. Am. J. Dis. Child. 1973; 125: 663–5.
Koren, A., Haasz, R., Tiatler, A., Katzuni, E. Serum immunoglobulin levels in children after splenectomy. Am. J. Dis. Child. 1984; 138: 53–5.
Hosea, S. W., Brown, E. J., Hamburger, M. I., Frank, M. M. Opsonic requirements for intravascular clearance after splenectomy. N. Engl. J. Med. 1981; 304: 245–50.
Likhite, V. V. Opsonin and leukophilic gamma globulin in chronically splenectomized rats with and without heterotropic autotransplanted splenic tissue. Nature 1975; 253: 742–4.
DiPadova, F., Durig, M., Harder, F. et al. Impaired antipneumococcal antibody production in patients without spleens. Br. Med. J. 1985; 290: 14–6.
Aaberge, I. S., Heier, H. E., Hem, E. et al. IgM and IgG response to pneumococcal vaccine in normal individuals and individuals splenectomized due to trauma. Acta Pathol. Microbiol. Immunol. Scand. 1984; 92: 11–6.
Cogbill, T. H., Moore, E. E., Jurkovich, G. J., Morris, J. A., Mucha, P., Shackford, S. R. Non-operative management of blunt splenic trauma: a multicentre experience. J. Trauma 1989: 10: 1312–7.
Mucha, P., Daly, R. C., Farnell, M. B. Selective management of blunt splenic trauma. J. Trauma 1986; 26: 970–8.
Wisner, D. H., Blaisdell, F. W. When to save the ruptured spleen. Surgery 1992; 111(2): 121–2.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
O’Sullivan, S.T., Reardon, C.M., O’Donnell, J.A. et al. “How Safe is Splenectomy?”. I.J.M.S. 163, 374–378 (1994). https://doi.org/10.1007/BF02942831
Issue Date:
DOI: https://doi.org/10.1007/BF02942831