
Abstract
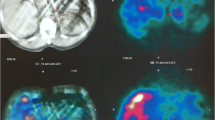
A case of unusual clinical manifestation of pheochromocytoma in a type 2A multiple endocrine neoplasia (MEN2A) patient is presented. A 27-year-old man affected by MEN2A syndrome, complaining of anxiety and depression, was admitted in our Division. Past medical history included a total thyroidectomy for medullary carcinoma in 1985, and left adrenalectomy for pheochromocytoma in 1994. Blood pressure was 130/85 mmHg without orthostatic hypotension and pulse rate was 72 beats/min. Laboratory data revealed thyroid hormones and carcinoembryonic antigen (CEA) in the normal range and high basal serum calcitonin levels (158 pg/ml). Plasma catecholamines and vanillylmandelic acid resulted in normal levels but epinephrine/norepinephrine ratio was elevated (0.65). The glucagon stimulation test showed positive clinical and biochemical response. Magnetic resonance imaging (MRI) and meta-iodobenzylguanidine (MIBG) scintiscan confirmed the presence of bilateral adrenal masses. Bilateral adrenalectomy by laparoscopic anterior approach was performed. Histology was consistent with adrenal pheochromocytomas. After surgical approach, psychiatric findings disappeared and did not recur at follow-up in spite of no medication for two years. In conclusion, bilateral pheochromocytoma is more frequent in MEN2A syndrome and probably understimated if the follow-up is not prolonged. In these cases clinical features are often aspecific and basal hormonal data may be normal in a great number of patients. Therefore long-term observation is justified in these patients. Pheochromocytoma was described as the “great mimic” for the numerous subjective manifestations. Differential diagnosis among typical features of neuropsychiatric disorders and pheochromocytoma must be considered.
Similar content being viewed by others

References
Bouloux P.G., Fakeeh M. Investigation of pheochromocytoma. Clin. Endocrinol. (Oxf.) 1995, 43: 657–664.
Gagel R.F., Tashjan A.H., Cummings T., Papathanasopoulos N., Kaplan M., DeLellis R.A., Wolfe H.J., Reichlin S. The clinical outcome of prospective screening for multiple endocrine neoplasia type 2A. N. Engl. J. Med. 1988, 318: 478–484.
Gagner M. Laparoscopic adrenalectomy. Surg. Clin. North Am. 1996, 76: 3, 523–537.
Filipponi S., Guerrieri M., Arnaldi G., Giovagnetti M., Masini A.M., Lezoche E., Mantero F. Laparoscopic adrenalectomy: a report on 50 operations. Eur. J. Endocrinol. 1998, 138: 548–553.
Bonnin F., Schlumberger M., Gardet P., Tenembaum F., Lumbroso J., Leclere J., Comoy E., Megnigbeto A., Travagli J.P., Parmentier C. Screening for adrenal medullary disease in patients with medullary thyroid carcinoma. J. Endocrinol. Invest. 1994, 17: 253–257.
Evans D.B., Lee J.E., Merrell R.C., Hickey R.C. Adrenal medullary disease in multiple endocrine neoplasia type 2. Appropriate management. Endocrinol. Metab. Clin. North Am. 1994, 23: 167–176.
Grossman E., Goldstein D.S., Hoffman A., Keiser H.R. Glucagon and clonidine testing in the diagnosis of pheochromocytoma. Hypertension 1991, 17: 733–741.
El-Matri A., Slim R., Smerli S., Ayed H.B. Pheochromocytome avec troubles psychiatriques. Un cas. Nouv. Presse Med. 1978, 7: 1467–1470.
Goldenberg M. Pheochromocytoma and essential hypertensive vascular disease. Arch. Intern. Med. 1950, 86: 823–836.
Aquilar-Parada E., Rivadeneyra J., Torres-Leon A.G., Serrano P.A. Pseudopheochromocytoma. J.A.M.A. 1971, 218: 884–885.
Lefebvre H., Noblet C., Moore N., Wolf L.M. Pseudo-pheochromocytoma after multiple drug interactions involving the selective monoamine oxidase inhibitor selegiline. Clin. Endocrinol. (Oxf.) 1995, 42: 95–98.
Duarte J., Sempere A.P., Cabezas C., Calvo T., Claveria L.E. Pseudo-pheochromocytoma in a patient with Parkinson’s disease. Ann. Pharmacother. 1996, 30: 546.
Bravo E.L. Evolving concepts in the pathophysiology, diagnosis and treatment of pheochromocytoma. Endocr. Rev. 1994, 15: 356–368.
Chakravorty S.G., De Souza C.J., Doongaji D.R. A psychiatric evaluation of referred cancer and medical patients: a comparative study. Indian J. Cancer 1993, 30: 55–60.
Berard R.M., Boermeester F. Psychiatric syntomatology in adolescents with cancer. Pediatr. Hematol. Oncol. 1998, 15: 211–214.
Holland J.C., Mastrovito R. Psychologic adaptation to brest cancer. Cancer 1980, 46 (Suppl. 4): 1045–1052.
Meurisse M., Joris J., Hamoir E., Hubert B., Charlier C. Laparoscopic removal of pheochromocytoma. Why? When? And Who? (Reflections on one case report). Surg. Endosc. 1995, 9: 431–436.
Moley J.F. Medullary thyroid cancer. Surg. Clin. North Am. 1995, 75: 405–420.
Murat A., GETC (Group d’Etude des Tumeurs a Calcitonine). Delection des lesions residuelles et des metastases du cancer medullaire de la thyroide. Ann. Endocrinol. (Paris) 1996, 57: 27–32.
Tisell L.E., Dilley W.G., Wells S.A. Progression of postoperative residual medullary thyroid carcinoma as monitored by plasma calcitonin levels. Surgery 1996, 119: 34–39.
Calender A., Giraud S., Schuffenecker I., Lenoir G.M., Gaudray P., Courseaux A., Porchet N., Aubert J.P., Zhang C.X. Genetic testing in presymptomatic diagnosis of multiple endocrine neoplasia. Horm. Res. 1997, 47: 199–210.
Eisenhofer G., Lenders J.W., Linehan W.M., Walther M.M., Goldstein D.S., Keiser H.R. Plasma normetanephrine and metanephrine for detecting pheochromocytoma in von Hippel-Lindau disease and multiple endocrine neoplasia type 2. N. Engl. J. Med. 1999, 340: 1872–1879.
Gokce O., Gokce C., Gunel S., Arisoy S., Arisoy E., Huseyinoglu K., Kismet K., Ucar O. Pheochromocitoma presenting with headache, panic attacks and jaundice in a child. Headache 1991, 31: 473–475.
Carre A. Panic attack: viewpoint of the internist. Encephale 1996, 5: 11–12.
Lambert M.T. Pheochromocitoma presenting as exacerbation of post traumatic stress disorder symptomology. Int. J. Psychiatry Med. 1992, 22: 265–268.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guerrieri, M., Filipponi, S., Arnaldi, G. et al. Unusual clinical manifestation of pheochromocytoma in a MEN2A patient. J Endocrinol Invest 25, 53–57 (2002). https://doi.org/10.1007/BF03343961
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03343961