
Abstract
Purpose
To evaluate the efficacy and effectiveness of red blood cell leukoreduction in reducing postoperative infection, mortality and cancer recurrence, two meta-analyses of randomized controlled trials (RCTs) were conducted.
Methods
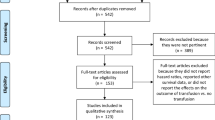
A systematic search of the scientific literature was conducted. The pooled relative risk ratio (RR) of developing an adverse postoperative outcome with either leukoreduced or non-leukoreduced blood was calculated using a random effects model. To better estimate the efficacy of leukoreduction, a second analysis of transfused patients only was conducted.
Results
Ten RCTs met inclusion criteria and eight provided separate data for patients randomized and transfused. The mean percentage of patients randomized but not transfused was 34%. For postoperative infection, the overall pooled RR was 0.76 [(95% confidence interval (CI): 0.54–1.08] for the “all patients randomized” analysis. For the “only patients transfused” analysis, the pooled RR became clinically and statistically significant (RR = 0.60 (95% CI: 0.38–0.93). For mortality, the pooled RR for the “all patients randomized” analysis was 0.71 (95% CI: 0.45–1.13) and 0.61 (95% CI: 0.36–1.04) for the “only patients transfused” analysis. When analyzing either all patients randomized or all patients transfused, there was no statistically significant difference in cancer recurrence rates (one study only).
Conclusion
We demonstrated that patients who were transfused leukoreduced red blood cells might benefit from a decrease in postoperative infections. A decrease in mortality may have been realized if more patients had been enrolled in the various randomized trials. Including all patients randomized, regardless of whether or not they were actually transfused diluted the observed clinical benefit of leukoreduction.
Résumé
Objectif
Dans le but d’évaluer l’efficacité de la réduction leucocytaire à diminuer l’infection postopératoire, la mortalité et la récurrence du cancer, nous avons réalisé deux méta-analyses d’études randomisées et contrôlées (ERC).
Méthode
Une recherche systématique des publications scientifiques a été réalisée. Le risque relatif (RR) de subir des complications postopératoires avec du sang réduit ou non en leucocytes a été calculé au moyen d’un modèle à effets aléatoires. Afin de mieux estimer l’efficacité de la réduction leucocytaire, une seconde analyse des patients transfusés a été faite.
Résultats
Dix ERC répondaient aux critères d’inclusion et huit portaient sur des patients randomisés et transfusés. Le pourcentage moyen de patients randomisés mais non transfusés était de 34 %. Le RR global d’une infection postopératoire était de 0,76 [(intervalle de confiance de 95 % (IC) : 0,54–1,08] pour l’analyse où «tous les patients sont randomisés». Dans l’analyse des «seuls patients transfusés», le RR est devenu cliniquement et statistiquement significatif (RR = 0,60 (IC de 95 % : 0,38–0,93). Le RR de mortalité dans l’analyse de «tous les patients randomisés» était de 0,71 (IC 95 % : 0,45–1,13) et de 0,61 (IC 95 % : 0,36–1,04) dans l’analyse des «seuls patients transfusés». Les analyses de tous les patients randomisés et de tous les patients transfusés n’ont pas montré de différence statistiquement significative de récurrence du cancer (une étude seulement).
Conclusion
Les patients qui reçoivent du sang réduit en leucocytes sont moins susceptibles d’avoir des infections postopératoires. Une baisse de la mortalité aurait pu être réalisée si plus de patients avaient participé aux diverses études randomisées. Quand on inclut tous les patients randomisés, peu importe qu’ils aient été transfusés ou non, on observe une dilution des avantages cliniques de la réduction leucocytaire.
Article PDF
Similar content being viewed by others
References
Opelz G, Sengar DP, Mickey MR, Terasaki PI. Effect of blood transfusions on subsequent kidney transplants. Transplant Proc 1973; 5: 253–9.
Miller JP, Mintz PD. The use of leukocyte-reduced blood components. Hematol Oncol Clin North Am 1995; 9: 69–90.
McAlister FA, Clark HD, Wells PS, Laupacis A. Perioperative allogeneic blood transfusion does not cause adverse sequelae in patients with cancer: a meta-analysis of unconfounded studies. Br J Surg 1998; 85: 171–8.
Vamvakas E. Transfusion-associated cancer recurrence and postoperative infection: meta-analysis of randomized, controlled clinical trials. Transfusion 1996; 36: 175–86.
Vamvakas EC, Blajchman MA. Universal WBC reduction: the case for and against. Transfusion 2001; 41: 691–712.
Vamvakas EC, Blajchman MA. Deleterious clinical effects of transfusion-associated immunomodulation: fact or fiction? Blood 2001; 97: 1180–95.
Fergusson D, Aaron SD, Guyatt G, Hebert P. Post-randomisation exclusions: the intention to treat principle and excluding patients from analysis. BMJ 2002; 325: 652–4.
Lau J. Meta-Analyst977. Boston, MA: New England Medical Center; 1995.
Nielsen HJ, Hammer JH, Krarup AL, et al. Prestorage leukocyte filtration may reduce leukocyte-derived bioactive substance accumulation in patients operated for burn trauma. Burns 1999; 25: 162–70.
Houbiers JG, Brand A, van de Watering LM, et al. Randomised controlled trial comparing transfusion of leucocyte-depleted or buffy-coat-depleted blood in surgery for colorectal cancer. Lancet 1994; 344: 573–8.
Jensen LS, Kissmeyer-Nielsen P, Wolff B, Qvist N. Randomised comparison of leucocyte-depleted versus buffy-coat-poor blood transfusion and complications after colorectal surgery. Lancet 1996; 348: 841–5.
van de Watering LM, Hermans J, Houbiers JG, et al. Beneficial effects of leukocyte depletion of transfused blood on postoperative complications in patients undergoing cardiac surgery. A randomized clinical trial. Circulation 1998; 97: 562–8.
Titlestad IL, Ebbesen LS, Ainsworth AP, Lillevang ST, Ivist N, Georgsen J. Leukocyte-depletion of blood components does not significantly reduce the risk of infectious complications. Results of a double-blinded, randomized study. Int J Colorectal Dis 2001; 16: 147–53.
Jensen LS, Andersen AJ, Christiansen PM, et al. Postoperative infection and natural killer cell function following blood transfusion in patients undergoing elective colorectal surgery. Br J Surg 1992; 79: 513–6.
Tartter PI, Mohandas K, Azar P, Endres J, Kaplan J, Spivack M. Randomized trial comparing packed red cell blood transfusion with and without leukocyte depletion for gastrointestinal surgery. Am J Surg 1998; 176: 462–6.
van Hilten JA, Brand A;TACTICS Reasearch Group. A multi-center prospective randomized trial of buffy coat depleted- and leukocyte filtered erythrocyte transfusions in vascular- and gastrointestinal oncologic surgery. Vox Sang 2002; 83(Suppl 1): 453–6.
Bracey AW, Radovancevic R, Nussmeier NA, et al. Leukocyte-reduced blood in open heart surgery patients: effects on outcome. Transfusion 2002; 42(Suppl): 5S (abstract).
Wallis JP, Chapman CE, Orr KE, Clark SC, Forty JR. Effect of WBC reduction of transfused RBCs on postoperative infection rates in cardiac surgery. Transfusion 2002; 42: 1127–34.
Dzik WH, Anderson JK, O’Neill EM, Assmann SF, Kalish LA, Stowell CP. A prospective, randomized clinical trial of universal WBC reduction. Transfusion 2002; 42: 1114–22.
van de Watering LM, Brand A, Houbiers JG, et al. Perioperative blood transfusions, with or without allogeneic leucocytes, relate to survival, not to cancer recurrence. Br J Surg 2001; 88: 267–72.
Bordin JO, Bardossy L, Blajchman MA. Growth enhancement of established tumors by allogeneic blood transfusion in experimental animals and its amelioration by leukodepletion: the importance of the timing of the leukodepletion. Blood 1994; 84: 344–8.
Blajchman MA, Bardossy L, Carmen RA, Goldman M, Heddle NM, Singal DP. An animal model of allogeneic donor platelet refractoriness: the effect of the time of leukodepletion. Blood 1992; 79: 1371–5.
Shanwell A, Kristiansson M, Remberger M, Ringden O. Generation of cytokines in red cell concentrates during storage is prevented by prestorage white cell reduction. Transfusion 1997; 37: 678–84.
Kristiansson M, Soop M, Shanwell A, Sundqvist KG. Prestorage versus bedside white blood cell filtration of red blood cell concentrates. Effects on the content of cytokines and soluble tumor necrosis factor receptors. J Trauma 1996; 40: 379–83.
Hébert PC, Fergusson D, Blajchman MA, et al. Clinical outcomes following institution of the Canadian universal leukoreduction program for red blood cell transfusions. JAMA 2003; 289: 1941–9.
Fergusson D, Hebert PC, Lee SK, et al. Clinical outcomes following institution of universal leukoreduction of blood transfusions for premature infants. JAMA 2003; 289: 1950–6.
Baron JF, Gourdin M, Bertrand M, et al. The effect of universal leukodepletion of packed red blood cells on postoperative infections in high-risk patients undergoing abdominal aortic surgery. Anesth Analg 2002; 94: 529–37.
Author information
Authors and Affiliations
Corresponding author
Additional information
D. Fergusson and M.P. Khanna are recipients of the Canadian Blood Services Doctoral Graduate Fellowship Award. Paul Hébert is a Career Scientist of the Ontario Ministry of Health.
Rights and permissions
About this article
Cite this article
Fergusson, D., Khanna, M.P., Tinmouth, A. et al. Transfusion of leukoreduced red blood cells may decrease postoperative infections: two meta-analyses of randomized controlled trials. Can J Anesth 51, 417–424 (2004). https://doi.org/10.1007/BF03018302
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018302