
Abstract
Purpose
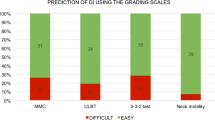
To determine the ability to predict difficult visualization of the larynx (DVL) from the following preoperative airway predictive indices, in isolation and combination: modified Mallampati test (MMT), thyromental distance (TMD), sternomental distance (SMD), horizontal length of the mandible (HLM) and inter-incisor gap(IIG).
Methods
Three hundred and eighty consecutive patients undergoing general anesthesia were evaluated using the MMT, TMD, SMD, HLM and IIG and the cut-off points for the airway predictors were Mallampati III and IV; # 6.5 cm, # 13.5 cm, # 9.0 cm and # 4.0 cm respectively. During direct laryngoscopy, the laryngeal view was graded using the Cormack and Lehane (CL) classification. CL grades III and IV were considered difficult visualization. Sensitivity, specificity and positive predictive value for each airway predictor in isolation and in combination were determined. Logistic regression analysis was used to determine independent predictors of DVL. Results: Difficulty to visualize the larynx was found in 13 (3.4%) patients. The sensitivity, specificity and the positive predictive value for the five airway predictors were: MMT (61.5%; 98.4%; 57.1 %), TMD (15.4%; 98.1%; 22.2%), SMD (0%; 100%; 0%), HLM (30.8%, 76.0%; 4.3%) and IIG (30.8%; 97.3%; 28.6%). The best combination of predictors was MMT/TMD/IIG with a sensitivity, specificity and positive predictive value of 84.6%; 94.6%; 35.5% respectively. Logistic regression analysis showed that weight, MMT, IIG and TMD were independent predictors of DVL.
Conclusion
MMT, TMD and IIG appear to provide the optimal combination in prediction of DVL in a West African population.
Résumé
Objectif
Déterminer la capacité de prédire les difficultés de visuali-sation du larynx (DVL) à partir des indices préopératoires suivants, pris isolément et en combinaison : le test de Mallampati modifié (TMM), la distance thyromentonnière (DTM), la distance sternomentionnière (DSM), la longueur horizontale de la mandibule (LHM) et l’espace inter-incisive (EII).
Méthode
Nous avons évalué 380 patients consécutifs devant subir une anesthésie générale en utilisant le TMM, la DTM, la DSM et l’EII; les points limites des prédicteurs d’intubation ont été les classes de Mallampati III et IV; # 6,5 cm, # 13,5 cm, # 9,0 cm et # 4,0 cm respectivement. La visualisation laryngoscopique directe a été cotée selon la classification de Cormack et Lehane (CL). Les classes de CL III et IV étaient une visualisation difficile. La sensibilité, la spécificité et la valeur prédictive positive de chaque prédicteur d’intubation pris isolé-ment et en combinaison ont été déterminés. On a déterminé les pré-dicteurs indépendants des DVL par l’analyse de régression logistique.
Résultats
La visualisation du larynx a été difficile chez 13 (3,4 %) patients. La sensibilité, la spécificité et la valeur prédictive positive des cinq prédicteurs d’intubation ont été : le TMM (61,5 %; 98,4 %; 57,1 %), la DTM (15,4 %; 98,1 %; 22,2 %), la DSM (0 %; 100 %; 0 %), la LHM (30,8 %; 76,0 %; 4,3 %) et l’EII (30,8 %; 97,3 %; 28,6 %). La meilleure combinaison de prédicteurs a été TMM/DTM/EII avec une sensibilité, une spécificité et une valeur pré-dictive positive de 84,6 %; 94,6 %; 35,5 % respectivement. L’analyse de régression logistique a montré que le poids, le TMM, l’EII et la DTM étaient des prédicteurs indépendants des DVL.
Article PDF
Similar content being viewed by others


References
Caplan RA, Benumof JL, Berry FA, et al. Practice guidelines for the management of the difficult airway. A report by the American Society of Anesthesiologist Task Force on the Management of the Difficult Airway. Anesthesiology 1993; 78:597–602.
Crosby ET, Cooper RM, Douglas MJ, et al. The unanticipated difficult airway with recommendations for management. Can J Anaesth 1998; 45:757–76.
Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology 1990; 72:828–33.
Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: a prospec- tive study. Can Anaesth Soc J 1985; 32:429–34.
Benumof JL. Management of the difficult adult airway. With special emphasis on awake tracheal intubation. Anesthesiology 1991; 75:1087–110.
White A, Kander PL. Anatomical factors in difficult direct laryngoscopy. Br J Anaesth 1975; 47:468.
Cobley M, Vaughan RS. Recognition and management of difficult airway problems. Br J Anaesth 1992; 68:90–7.
Wilson ME, Spiegelhalter D, Robertson JA, Lesser P. Predicting difficult intubation. Br J Anaesth 1988; 61:211–6.
King TA, Adams AP. Failed tracheal intubation. Br J Anaesth 1990; 65:400–14.
Mathew M, Hanna LS, Aldrete JA. Pre-operative indices to anticipate difficult tracheal intubation. Anesth Analg 1989; 68:S187 (abstract).
Frerk CM. Predicting difficult intubation. Anaesthesia 1991; 46:1005–8.
Savva D. Prediction of difficult tracheal intubation. Br J Anaesth 1994; 73:149–53.
Rose DK, Cohen MM. The airway: problems and predictions in 18,500 patients. Can J Anaesth 1994; 41:372–83.
Samsoon GL, Young JR. Difficult trachea intubation: a retrospective study. Anaesthesia 1987; 42:487–9.
Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984; 39:1105–11.
Tse JC, Rimm EB, Hussain A. Predicting difficult endotracheal intubation in surgical patients scheduled for general anesthesia: a prospective blind study. Anesth Analg 1995; 81:254–8.
Ramadhani SA, Mohamed LA, Rocke DA, Gouws E. Sternomental distance as the sole predictor of difficult laryngoscopy in obstetric anaesthesia. Br J Anaesth 1996; 77:312–6.
Ita CE, Eshiet AI, Akpan SG. Recognition of the difficult airway in normal Nigerian adults (a prospective study). West Afr J Med 1994; 13:102–4.
Karkouti K, Rose DK, Ferris LE, Wigglesworth DF, Meisamai-Fard T, Lee H. Inter-observer reliability of ten tests used for predicting difficult tracheal intubation. Can J Anaesth 1996; 43:554–9.
Tham EJ, Gildersleve CD, Sanders LD, Mapleson WW, Vaughan RS. Effects of posture, phonation and observer on Mallampati classification. Br J Anaesth 1992; 68:32–8.
Nath G, Sekar M. Predicting difficult intubation — a comprehensive scoring system. Anaesth Intensive Care 1997; 25:482–6.
Bilgin H, Ozyurt G. Screening test for predicting difficult intubation. A clinical assessment in Turkish patients. Anaesth Intensive Care 1998; 26:382–6.
Arne J, Descoins P, Fusciardi J, et al. Preoperative assessment for difficult intubation in general and ENT surgery: predictive value of a clinical multivariate risk index. Br J Anaesth 1998; 80:140–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Merah, N.A., Wong, D.T., Ffoulkes-Crabbe, D.J. et al. Cardiothoracic anesthesia, respiration and airway modified mallampati test, thyromental distance and inter-incisor gap are the best predictors of difficult laryngoscopy in West Africans. Can J Anesth 52, 291–296 (2005). https://doi.org/10.1007/BF03016066
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016066