
Abstract
Purpose
To compare the simultaneous haemodynamic effects, sympathetic activation and cardiac risks associated with desflurane used in a balanced technique, with those of isoflurane anaesthesia.
Methods
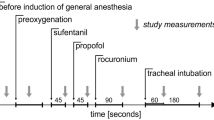
A prospective, randomized, open label study was conducted at a University medical centre. Forty patients undergoing major non-cardiac surgery were randomized to receive either desflurane or isoflurane as the primary anaesthetic agent. After premedication, fentanyl and thiopentone were administerediv. Anaesthesia was increased up to 1.0 MACET in O2 via controlled mask ventilation and maintained at 1.0 MAC before tracheal intubation. Maintenance consisted of N2O, O2 and desflurane or isoflurane for 10 min. During the study, HR and arterial BP were continuously measured, as were ECG ST-segments and ventricular dysrhythmias using a 3-channel Holter ECG recorder Left ventricular global and regional function were measured using precordial echocardiography. Serial plasma catecholamine concentrations were measured.
Results
For both groups, HR was maintained without increases over baseline values while systolic BP showed a progressive decrease during induction. Use of beta blockade during induction was higher in the desflurane (7/20 = 35%) than in the isoflurane group (1/20 = 5%),P = 0.04. The plasma norepinephrine concentrations progressively increased in the desflurane group but not in the isoflurane group. Four patients in the desflurane and three in the isoflurane group developed transient worsening of regional function but no change in mean left ventricular ejection fraction area and no ECG ischaemia occurred during anaesthetic induction.
Conclusions
Desflurane differs from isoflurane in that sympathetic stimulation persisted despite blunting of potential hyperdynamic haemodynamic responses by narcotic and beta blockade. However; this sympathetic activation did not appear to increase cardiac risks.
Résumé
Objectif
Comparer simultanément les effets hémodynamiques, l’activation sympathique et les risques cardiaques associés à l’utilisation du desflurane ou de l’isoflurane utilisés selon une technique anesthésique balancée.
Méthodes
Une étude prospective, randomisée et ouverte a été menée dans un centre hospitalo-universitaire. Quarante patients devant subir une chirurgie majeure non cardiaque ont été répartis de façon aléatoire en deux groupes, l’un recevant du desflurane et l’autre de l’isoflurane comme agent anesthésique principal. Après une prémédication, on a procédé à l’injection intraveineuse de fentanyl et de thiopental. L’anesthésie a été augmentée jusqu’à 1,0 MACET avec O2 à l’aide d’une ventilation contrôlée par masque et maintenue par la suite à 1,0 MAC avant l’intubation trachéale. Le maintien était assuré par l’utilisation du N2O, de l’oxygène et de l’isoflurane ou du desflurane pendant 10 minutes. Durant l’étude, la FC, et la TA ont été mesurées en continu, de même le segment ST à l’ECG et les dysrythmies ventriculaires qui ont été enregistrées à l’aide d’un moniteur ECG de Holter à 3 canaux. Les fonctions ventriculaires gauches globales et régionales ont été évaluées en utilisant un échocardiographe précordial. Des concentrations plasmatiques sériées de catécholamines ont été mesurées.
Résultats
Pour les deux groupes, la FC s’est maintenue sans augmentation par rapport aux valeurs de départ, alors que la TA systolique décroissait progressivement durant la phase d’induction. L’utilisation de bloqueurs durant l’induction était plus fréquente dans le groupe sous desflurane (7/20 = 35 %) que dans le groupe sous isoflurane (1/20 = 5 %),P = 0,04. Les concentrations plasmatiques de norépinéphrine ont augmenté progressivement dans le groupe desflurane mais non dans le groupe isoflurane. Quatre patients sous desflurane et trois sous isoflurane ont développé une dégradation transitoire de la fonction régionale, mais aucun changement ne s’est produit au niveau de la fraction moyenne d’éjection du ventricule gauche et aucune ischémie à l’ECG n’est survenue pendant l’induction de l’anesthésie.
Conclusion
Le desflurane diffère de l’isoflurane en ce que la stimulation sympathique persiste malgré la tentative d’émousser les réponses hémodynamiques hyperdynamiques potentielles par l’usage d’un narcotique et d’un bêta bloqueur Cependant, cette activation sympathique n’a pas semblé accroître les risques de problèmes cardiaques.
Article PDF
Similar content being viewed by others
References
Helman JD, Leung JM, Bellows WH, et al. The risk of myocardial ischemia in patients receiving desflurane versus sufentanil anaesthesia for coronary artery bypass graft surgery. Anesthesiology 1992; 77: 47–62.
Ebert TJ, Muzi M. Sympathetic hyperactivity during desflurane anesthesia in healthy volunteers. Anesthesiology 1993; 79: 444–53.
Weiskopf RB, Eger EI II, Noorani M, Daniel M. Fentanyl, esmolol, and clonidine blunt the transient cardiovascular stimulation induced by desflurane in humans. Anesthesiology 1994; 81: 1350–5.
Thomson IR, Bowering JB, Hudson RJ, Frais MA, Rosenbloom M. A comparison of desflurane and isoflurane in patients undergoing coronary artery surgery. Anesthesiology 1991; 75: 776–81.
Parsons RS, Jones RM, Wrigley SR, MacLeod KGA, Platt MW. Comparison of desflurane and fentanyl-based anaesthetic techniques for coronary artery bypass surgery. Br J Anaesth 1994; 72: 430–8.
Leung JM, Levine EH. Left ventricular end-systolic cavity obliteration as a estimate of intraoperative hypovolemia. Anesthesiology 1994; 81: 1102–9.
Bergquist BD, Leung JM, Bellows WH. Transesophageal echocardiography in myocardial revascularization: I. Accuracy of intraoperative real-time interpretation. Anesth Analg 1996; 82: 1132–8.
American Society of Echocardiography Committee on standards, subcommittee on quantitation of two-dimensional echocardiograms. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. J Am Soc Echocardiogr 1989; 2: 358–67.
Leung JM, O’Kelly B, Browner WS, et al. Prognostic importance of postbypass regional wall-motion abnormalities in patients undergoing coronary artery bypass graft surgery. Anesthesiology 1989; 71: 16–25.
Yasuda N, Weiskopf RB, Cahalan MK, et al. Does desflurane modify circulatory responses to stimulation in humans? Anesth Analg 1991; 73: 175–9.
Weiskopf RB, Eger EI II, Daniel M, Noorani M. Cardiovascular stimulation induced by rapid increases in desflurane concentration in humans. Results from activation of tracheopulmonary and systemic receptors. Anesthesiology 1995; 83: 1173–8.
Muzi M, Ebert TJ, Hope WG, Robinson BJ, Bell LB. Site(s) mediating sympathetic activation with desflurane. Anesthesiology 1996; 85: 737–47.
Bunting HE, Kelly MC, Milligan KR. Effect of nebulized lignocaine on airway irritation and haemodynamic changes during induction of anaesthesia with desflurane. Br J Anaesth 1995; 75: 631–3.
Gormley WP, Murray JM, Trinick TR. Intravenous lidocaine does not attenuate the cardiovascular and catecholamine response to a rapid increase in desflurane concentration. Anesth Analg 1996; 82: 358–61.
Weiskopf RB, Moore MA, Eger EI II, et al. Rapid increase in desflurane concentration is associated with greater transient cardiovascular stimulation than with rapid increase in isoflurane concentration in humans. Anesthesiology 1994; 80: 1035–45.
Daniel M, Eger EI II, Weiskopf RB, Noorani M. Propofol fails to attenuate the cardiovascular response to rapid increases in desflurane concentration. Anesthesiology 1996; 84: 75–80.
Grant J, Scrutton M. Novel -adrenoreceptors primarily responsible for inducing human platelet aggregation. Nature 1979; 277: 659–61.
Parker SD, Breslow MJ, Frank SM, et al. Catecholamine and cortisol responses to lower extremity revascularization: correlation with outcome variables. Crit Care Med 1995; 23: 1954–61.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported in part by the Pretenure award and a research award from the Academic Senate, University of California, San Francisco.
Rights and permissions
About this article
Cite this article
Leung, J.M., Pastor, D.A. Dissociation between haemodynamics and sympathetic activation during anaesthetic induction with desfluranes. Can J Anaesth 45, 533–540 (1998). https://doi.org/10.1007/BF03012703
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012703