
Abstract
This review analyzes the literature dealing with cardiopulmonary function during and pulmonary function following laparoscopic cholecystectomy in order to describe the patterns of changes in these functions and the mechanisms involved as well as to identify areas of concern and lacunae in our knowledge. Information was obtained from a Medline literature search and the annual meeting supplements of Anesthesiology, Anesth Analg, Br J Anaesth, and Can J Anaesth. The principal findings were that changes in cardiovascular Junction due to the insufflation are characterized by an immediate decrease in cardiac index and an increase in mean arterial blood pressure and systemic vascular resistance. In the next few minutes there is partial restoration of cardiac index and resistance but blood pressure and heart rate do not change. The pattern is the result of the interaction between increased abdominal pressure, neurohumoral responses and absorbed CO2. Pulmonary junction changes are characterized by reduced compliance without large alterations in PaO2, but tissue oxygenation can be adversely affected due to reduced O2 delivery. A major difficulty in maintaining normocarbia is due to the abdominal distention reducing pulmonary compliance and to CO2 absorption. End tidal CO2 tension is not a reliable index of PaCO2, particularly in ASA III–IV patients. The pattern of lung function following LC is characterized by a transient reduction in lung volumes and capacities with a restrictive breathing pattern and the loss of the abdominal contribution to breathing. Atelectasis also occurs. These changes are qualitatively similar to but of a lesser magnitude than those following “open” abdominal operations. It is concluded that the changes in cardiopulmonary function during laparoscopic upper abdominal surgery lead us to suggest judicious invasive monitoring and careful interpretation in ASA III–IV patients. Lung function following extensive procedures in sick patients has not been reported.
Résumé
Ce survol analyse la littérature portant sur la fonction cardiopulmonaire pendant et la fonction pulmonaire après la cholecystectomie laparoscopique dans le but d’en décrire le profil des changements et les mécanismes engagés, et identifier les domaines d’intérêt particuliers et les lacunes de nos connaissances. Les renseignements ont été compilés à partir des données de Medline et des suppléments d’Anesthesiology, Anesth Analg, Br J Anaesth, et Can J Anaesth. Les répercussions cardio-vasculaires causées par l’insufflation sont caractérisées par une chute immediate de l’index cardiaque et une augmentation de la pression artérielle moyenne et de la résistance vasculaire ont constitué les constatations les plus importantes. Dans les minutes qui suivent, l’index cardiaque et la résistance se rétablissent partiellement, mais la pression artérielle et la fréquence cardiaque ne changent pas. Cet état résulte de l’interaction entre l’augmentation de la pression abdominale, les réponses neuro-humorales et le CO2 absorbé. Les changements de la fonction pulmonaire sont caractérisés par une baisse de la compliance sans modifications significatives de la PaO2, mais l’oxygénation des tissus peut être désavantagée par la baisse du transport de l’O2. Le maintien de la CO2 téléexpiratoire représente un problème majeur à cause de la distension l’abdominale qui réduit la compliance pulmonaire et par la réabsorption du CO2. Le CO2 téléexpiratoire évalue mal la PaCO2 spécialement chez les patients ASA III et IV. L’état de la fonction pulmonaire est caractérisé par une réduction transitoire des volumes et des capacités pulmonaires avec un profil restrictif et une perte de la contribution abdominale à la respiration. Il existe aussi de l’atélectasie. Ces changements sont identiques à ceux qui suivent la cholécystectomie traditionnelle mais à un moindre degré. Les répercussions sur la fonction cardio-pulmonaire pendant la chirurgie laparoscopique haute nous incitent à suggérer un monitorage effractif pertinent interprété avec perspicacité chez les patients ASA III et IV. On n’a pas fait d’observation sur la fonction pulmonaire de patients tarés après des interventions complexes.
Article PDF
Similar content being viewed by others
References
Joris JL, Noirot DP, Legrand MJ, Jacquet NJ, Lamy ML. Hemodynamic changes during laparoscopic cholecystectomy. Anesth Analg 1993; 76: 1067–71.
Breton G, Poulin E, Fortin C, Mamazza J, Robert J. Evaluation clinique et hémodynamique des cholécystectomies par voie laparoscopique. Ann Chir 1991; 45: 783–90.
Reid CW, Martineau RJ, Hull KA, Miller DR. Haemodynamic consequences of abdominal insufflation with CO2 laparoscopic cholecystectomy. Can J Anaesth 1992; 39 A132.
Cunningham AJ, Turner J, Rosenbaum S, Rqfferty T. Transoesophageal echocardiographic assessment of haemodynamic function during laparoscopic cholecystectomy. Br J Anaesth 1993; 70: 621–5.
Westerband A, Van De Water JM, Amzallag M, et al. Cardiovascular changes during laparoscopic cholecystectomy. Surg Gynecol Obstet 1992; 175: 535–8.
McLaughlin JG, Bonnell BW, Scheeres DE, Dean RJ. The adverse hemodynamic effects related to laparoscopic cholecystectomy. Anesthesiology 1992; 77: A70.
Liu SY, Lieghton T, Davis I, Klein S, Lippmann M, Bongard F. Prospective analysis of cardiopulmonary responses to laparoscopic cholecystectomy. J Laparoendosc Surg 1991; 1: 241–6.
Iwase K, Takenaka H, Yagura A, et al. Hemodynamic changes during laparoscopic cholecystectomy in patients with heart disease. Endoscopy 1992; 24: 771–3.
Fox LG, Hein HAT, Gawey BJ, Hellman CL, Ramsay MAE. Physiologic alterations during laparoscopic cholecystectomy in ASA III & IV patients. Anesthesiology 1993; 79: A55.
Safran D, Sgambati S, Orlando R III. Laparoscopy in high-risk cardiac patients. Surg Gynecol Obstet 1993; 176: 548–54.
Feig BW, Berger DH, Dupuis JF, et al. Hemodynamic effects of CO2 abdominal insufflation (CAI) during laparoscopy in high-risk patients. Anesth Analg 1994; 78: S109.
Goodale RL, Beebe DS, McNevin MP, et al. Hemodynamic, respiratory, and metabolic effects of laparoscopic cholecystectomy. Am J Surg 1993; 166: 533–7.
Joris J, Honore P, Lamy M. Changes in oxygen transport and ventilation during laparoscopic cholecystectomy. Anesthesiology 1992; 77: A149.
Aoki T, Tanii M, Takahashi K, Tateda T, Miyazawa A. Cardiovascular changes and plasma catecholamine levels during laparoscopic surgery. Anesth Analg 1994; 78: S8.
Felber AR, Blobner M, Goegler S, Senekowitsch R, Jelen-Esselborn S. Plasma vasopressin in laparoscopic cholecystectomy. Anesthesiology 1993; 79: A32.
Joris J, Lamy M. Neuroendocrine changes during pneumoperitoneum for laparoscopic cholecystectomy. Br J Anaesth 1993; 70: A33.
Mealy K, Gallagher H, Barry M, Lennon F.Traynor O, Hyland J. Physiological and metabolic responses to open and laparoscopic cholecystectomy. Br J Surg 1992; 79: 1061–4.
Mullet CE, Viale JP, Sagnard PE, et al. Pulmonary CO2 elimination during surgical procedures using intraor extraperitoneal CO2 insufflation. Anesth Analg 1993; 76: 622–6.
Wurst H, Schulte-Steinberg H, Finsterer U. Pulmonary CO2-elimination in laparoscopic cholecystectomy. A clinical study (German). Anaesthesist 1993; 42: 427–34.
Lister DR, Rudston-Brown B, Warriner B, McEwan J, Chan M, Walley KR. Carbon dioxide absorption is not linearly related to intraperitoneal carbon dioxide insufflation pressures in pigs. Anesthesiology 1994; 80: 129–36.
Rasmussen JP, Dauchot PJ, DePalma RG, et al. Cardiac function and hypercarbia. Arch Surg 1978; 113: 1196–1200.
Marshall BE, Cohen PJ, Klingenmaier CH, Neigh JL, Pender JW. Some pulmonary and cardiovascular effects of enflurane (Ēthrane) anaesthesia with varying\(Pa_{CO_2 } \) in man. Br J Anaesth 1971; 43: 996–1002.
Rademaker BMP, Odoom JA, deWit LT, Kalkman CJ, en Brink SA, Ringers J. Haemodynamic effects of pneumoperitoneum for laparoscopic surgery: a comparison of CO2 with N2O insufflation. Eur J Anaesthesiol (in press).
Bongard FS, Pianim NA, Leighton TA, et al. Helium insufflation for laparoscopic operation. Surg Gynecol Obstet 1993; 177: 140–6.
Litwin DEM, Girotti MJ, Poulin EC, Mamazza J, Nagy AG. Laparoscopic cholecystectomy: trans-Canada experience with 2201 cases. Can J Surg 1992; 35: 291–6.
Fujii Y, Tanaka H, Tsuruoka S, Toyooka H, Amaha K. Middle cerebral arterial blood flow velocity increases during laparoscopic cholecystectomy. Anesth Analg 1994; 78: 80–3.
Duale C, Bazin JE, Ferrier C, Ruiz F, Schoeffler P. Hemodynamic effects of laparoscopic cholecystectomy in patients with coronary disease. Br J Anaesth 1993; 72: A31.
Gannendahl P, Ljungqvist O, Odeberg S, Sollevi A. Computerized vecto cardiography during laparoscopic cholecystectomy. Anesthesiology 1993; 79: A512.
Beique F, Ramsey JG. The pulmonary artery catheter: a new look. Seminars in Anesthesia 1994; 13: 14–25.
Taylor E, Feinstein R, White PF, Soper N. Anesthesia for laparoscopic cholecystectomy. Is nitrous oxide contraindicated? Anesthesiology 1992; 76: 541–3.
Dhoste K, Karayan J, Lacoste L, Lehuedé MS, Fusciardi J. Haemodynamic changes during laparoscopic cholecystectomy in the elderly. Br J Anaesth 1993; 72: A32.
Wahba RWM. Perioperative functional residual capacity. Can J Anaesth 1991; 38: 384–400.
Heneghan CPH, Bergman NA, Jones JG. Changes in lung volume and\(\left( {PA_{O_2 } - Pa_{O_2 } } \right)\) during anaesthesia. Br J Anaesth 1984; 56: 437–45.
Feinstein R, Ghouri A. Change in pulmonary mechanics during laparoscopic cholecystectomy. Anesth Analg 1993; 76: S102.
Monk TG, Weldon BC, Lemon D. Alterations in pulmonary function during laparoscopic surgery. Anesth Analg 1993; 76: S274.
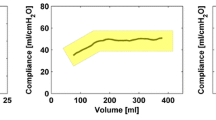
Mäkinen M-T. Dynamic lung compliance during laparoscopic cholecystectomy. Anesth Analg 1994; 78: S261.
Grissom TE, Gootos PJ, Brown TR. Pulmonary compliance is not affected by changes in position during laparoscopic surgery. Anesthesiology 1993; 79: S491.
Feig BW, Berger DH, Dougherty TB, et al. Pulmonary effects of CO2 abdominal insufflation (CAI) during laparoscopy in high-risk patients. Anesth Analg 1994; 78: S108.
Wahba RWM, Mamazza J. Ventilatory requirements during laparoscopic cholecystectomy. Can J Anaesth 1993; 40: 206–10.
Chiche JD, Joris J, Lamy M. PEEP for treatment of intraoperative pneumothorax during laparoscopic fundoplication. Br J Anaesth 1994; 72: A38.
Wittgen CM, Andrus CH, Fitzgerald SD, Baudendistel LJ, Dahms TE, Kaminski DL. Analysis of the hemodynamic and ventilatory effects of laparoscopic cholecystectomy. Arch Surg 1991; 126: 997–1001.
Blobner MA, Felber AR, Gögler S, Weigl EM, Jelen-Esselborn S. Carbon dioxide uptake from pneumoperitoneum during laparoscopic cholecystectomy. Anesthesiology 1992; 77: A37.
Raemer DB, Francis D, Philip JH, Gabel RA. Variation inPCo2 between arterial blood and peak expired gas during anesthesia. Anesth Analg 1983; 62: 1065–9.
Bhavani-Shankar K, Moseley H, Kumar AY, Delph Y. Capnometry and anaesthesia. Can J Anaesth 1992; 39: 617–32.
Wittgen CM, Naunheim KS, Andrus CH, Kaminski DL. Preoperative pulmonary function evaluation for laparoscopic cholecystectomy. Arch Surg 1993; 128: 880–5.
Fitzgerald SD, Andrus CH, Baudendistel LJ, Dahms TE, Kaminski DL. Hypercarbia during carbon dioxide pneumoperitoneum. Am J Surg 1992; 163: 186–90.
Leighton T, Pianim N, Liu S-Y, Kono M, Klein S, Bongard F. Effectors of hypercarbia during experimental pneumoperitoneum. Am Surg 1992; 58: 717–21.
Smith RS, Fry WR, Tsoi EKM, et al. Gasless laparoscopy and conventional instruments. The next phase of minimally invasive surgery. Arch Surg 1993; 128: 1102–7.
Wahba RWM, Don HF, Craig DB. Post-operative epidural analgesia: effects on lung volumes. Can Anaesth Soc J 1975; 22: 519–27.
Frazee RC, Roberts JW, Okeson GC, et al. Open versus closed laparoscopic cholecystectomy. A comparison of postoperative pulmonary function. Ann Surg 1991; 214: 651–4.
Poulin EC, Mamazza J, Breton G, Fortin CL, Wahba R, Ergina P. Evaluation of pulmonary function in laparoscopic cholecystectomy. Surg Laparosc Endosc 1992. 2: 292–6.
Joris J, Cigarini I, Legrand M, et al. Metabolic and respiratory changes after cholecystectomy performed via laparotomy or laparoscopy. Br J Anaesth 1992; 69: 341–5.
Rademaker BM, Ringers J, Odoom JA, de Wit LT, Kalkman CJ, Oosting J. Pulmonary function and stress response after laparoscopic cholecystectomy: comparison with subcostal incision and influence of thoracic epidural analgesia. Anesth Analg 1992; 75: 381–5.
Liu J, Ding Y, White PF, Feinstein R, Shear JM. Effects of ketorolac on postoperative analgesia and ventilatory function after laparoscopic cholecystectomy. Anesth Analg 1993; 76: 1061–6.
Schauer PR, Luna J, Ghiata AA, Gien ME, Warren JM, Sirinek KR. Pulmonary function after laparoscopic cholecystectomy. Surg 1993; 114: 389–99.
Putensen-Himmer G, Putensen C, Lammer H, Lingnau W, Aigner F, Benzer H. Comparison of postoperative respiratory function after laparoscopic or laparotomy for cholecystectomy. Anesthesiology 1992; 77: 675–80.
Johnson D, Litwin D, Osachoff J, et al. Postoperative respiratory function after laparoscopic cholecystectomy. Surg Laparosc Endosc 1992; 2: 221–6.
Neilsen PR, Brushøj J, Sonnenschein C. Pulmonary function after laparoscopic cholecystectomy. Br J Anaesth 1994; 72: A36.
Strandberg A, Tokics L, Brismar B, Lundquist H, Hedenstierna G. Atelectasis during anaesthesia and in the postoperative period. Acta Anaesthesiol Scand 1986; 30: 154–8.
Couture JG, Chartrand D, Gagner M, Bellemare F. Diaphragmatic and abdominal muscle activity after endoscopic cholecystectomy. Anesth Analg 1994; 78: 733–9.
Erice F, Fox GS, Salib YM, Romano E, Meakins JL, Magder SA. Diaphragmatic function before and after laparoscopic cholecystectomy. Anesthesiology 1994; 79: 966–75.
Sharma R, Clergue F, Jansson E, Reiz S. Diaphragmatic function after laparoscopic cholecystectomy. Br J Anaesth 1994; 72: A34.
Sharma SK, Joshi GP. Laparoscopic cholecystectomy versus open cholecystectomy: postoperative analgesic and antiemetic requirements. Anesth Analg 1994; 78: S386.
Wiesel S, Grillas R. Laparoscopic versus open cholecystectomy: PCA morphine requirements. Anesth Analg 1993; 76: S465.
Tousignant G, Wiesel S, Laporta D, Sigman H. The effect of age on recovery of pulmonary function after laparoscopic cholecystectomy. Anesth Analg 1992; 74: S321.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Wahba, R.W.M., Béïque, F. & Kleiman, S.J. Cardiopulmonary function and laparoscopic cholecystectomy. Can J Anaesth 42, 51–63 (1995). https://doi.org/10.1007/BF03010572
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03010572