
Abstract
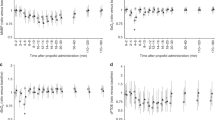
Tracheal intubation is frequently required in neonatal anaesthetic practice. Awake intubation is one method of securing the airway and in certain circumstances, for many anaesthetists, can be preferable to intubation following induction of anaesthesia. Previous studies have inferred that the elevation in anterior fontanelle pressure observed during tracheal intubation in neonates was caused by an increase in cerebral blood flow although it was never measured. In this study, direct methods were used to observe changes in the cerebral circulation. Thirteen neonates, ASA I to III (E), aged from 1 to 34 days of age were studied. Patients were randomized to receive either tracheal intubation awake or following induction of anaesthesia with thiopentone 5 mg · kg− 1 and succinylcholine 2 mg · kg−1. Heart rate, systolic arterial blood pressure, anterior fontanelle pressure, cerebral blood flow velocity (using transcranial Doppler sonography) and oxygen saturation were recorded at the following intervals: baseline (not crying), after intravenous atropine 0.02 mg · kg− 1, during laryngoscopy, immediately after insertion of the endotracheal tube, one and five minutes later. The use of atropine masked the cardiovascular responses to intubation. Whereas the change in anterior fontanelle pressure from baseline was different between the groups (P < 0.05), the cerebral blood flow velocity variables were not. The rise in anterior fontanelle pressure seen in the awake group may be attributed to a reduction of the venous outflow from the cranium thereby increasing cerebral blood volume and sub-sequently the intracranial pressure.
Résumé
En anesthésie néonatale, l’intubation endotrachéale est souvent nécessaire. L’intubation éveillée est utilisée pour le maintien de la perméabilité des voies respiratoires et dans certaines circonstances, plusieurs anesthésistes la préfèrent à l’intubation sous anesthésie générale. Auparavant des études ont conclu que l’augmentation de la pression de la fontanelle antérieure observée pendant l’intubation endotrachéale du nouveau-né était due à une augmentation du débit sanguin cérébral bien qu’on ne l’ait jamais mesurée. Dans cette étude, des méthodes directes sont utilisées pour l’observation des changements de la circulation cérébrale. Treize nouveaux-nés, ASA I à III (E), âgés de I à 34 jours font partie de l’étude. Ils sont répartis au hasard pour subir une intubation endotrachéale soit éveillés, soit sous anesthésie au thiopentone 5 mg · kg− 1et à la succinykholine 2 mg · kg− 1. La fréquence cardiaque, la tension artérielle systolique, la pression de la fontanelle antérieure, la vélocité du débit sanguin cérébral (par sonographie intracrânienne au Doppler) et la saturation en oxygène sont enregistrées aux intervals suivants: ligne de base (sans pleurs de l’enfant), après atropine iv 0,02 mg· kg− 1, pendant la laryngoscopie, immédiatement après l’insertion du tube endotrachéal et une et cinq minutes plus tard. L’utilisation de l’atropine masque la réponse cardiovasculaire à l’intubation. Alors que les variations de la pression de la fontanelle antérieure mesurées différent de la ligne de base diffèrent entre les groupes (P < 0,05), les variables de la vélocité du débit sanguin cérébral ne diffèrent pas. L’élévation de la pression de la fontanelle antérieure constatée chez le groupe éveillé est possiblement attribuable à une baisse du drainage veineux intracrânien avec augmentation consécutive du volume sanguin cérébral et subséquemment de la pression intracrânienne.
Article PDF
Similar content being viewed by others

References
Kelly MA, Finer NN. Nasotracheal intubation in the neonate: physiologic responses and effects of atropine and pancuronium. J Paediatr 1984; 105: 303–9.
Moorthy SS, Greenspan CD, Dierdof SF, Spmgue D. Cerebral blood flow increases and femoral blood flow decreases during laryngoscopy and tracheal intubation. Anesthesiology 1992; 77: A73.
Motoyama E. Endotracheal intubation.In: Motoyama EK, Davis PJ (Eds.). Smith’s Anesthesia for Infants and Children. 5th ed. St-Louis: CV Mosby Co., 1990.
Bissonnette B, Sullivan PJ. Pyloric stenosis. Can J Anaesth 1991; 38: 668–76.
Friesen RH, Honda AT, Thieme RE. Changes in anterior fontanelle pressure in pre-term neonates during tracheal intubation. Anesth Analg 1987; 66: 874–8.
Stow PJ, McLeod ME, Burrows FA, Creighton RE. Anterior fontanelle pressure responses to tracheal intubation in the awake and anaesthetized infant. Br J Anaesth 1988; 60: 167–70.
Aaslid R, Markwalder TM, Nornes H. Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries. J Neurosurg 1982; 57: 769–74.
Pilato MA, Bissonnette B, Lerman J. Transcranial Doppler: response of cerebral blood-flow velocity to carbon dioxide in anaesthetized children. Can J Anaesth 1991; 38: 37–42.
Carpenter M, Sutin J. Human Neuroanatomy. 8th ed. Baltimore: Williams & Wilkins Inc, 1983.
Bunegin L, Albin MS, Rauschhuber R, Marlin AE. Intracranial pressure measurement from the anterior fontanelle utilizing a pneumoelectronic switch. Neurosurgery 1987; 20: 726–31.
Myerberg DZ, York C, Chaplin ER, Gregory GA. Comparison of noninvasive and direct measurements of intracranial pressure. Pediatrics 1980; 65: 473–6.
McDonald MM, Kioops BL, Johnson ML, et al. Timing and antecedents of intracranial hemorrhage in the newborn. Pediatrics 1984; 74: 32–6.
Markwalder TM, Grolimund P, Seiler RW, Roth F, Aaslid R. Dependency of blood flow velocity in the middle cerebral artery on end-tidal carbon dioxide partial pressure — a transcranial ultrasound Doppler study. J Cereb Blood Flow Metab 1984; 4: 368–72.
Bode H, Wais U. Age dependence of flow velocities in basal cerebral arteries. Arch Dis Child 1988; 63: 606–11.
Stoelting RK. Circulatory changes during direct laryngos-copy and tracheal intubation: influence of duration of laryngoscopy with or without prior lidocaine. Anesthesiology 1977; 47: 381–4.
Unni VKN, Johnston RA, Young HSA, McBride RJ. Prevention of intracranial hypertension during laryngos-copy and endotracheal intubation: use of a second dose of thiopentone. Br J Anaesth 1984; 56: 1219–23.
Bedford R, Winn H, Tyson G, Park T, Jane J. Lidocaine prevents increased ICP after endotracheal intubation.In: Shulman K, Marmarou A, Miller JD, Becker DP, Hochwald GM, Brock M (Eds.). Intracranial Pressure IV, New York: Springer-Verlag 1980; 595–8.
Aaslid R. The Doppler principle applied to measurement of blood flow velocity in cerebral arteries.In: Aaslid R (Ed.). Transcranial Doppler Sonography, New York: Springer-Verlag, 1986: 22–38.
Hennerici M, Rautenberg W, Sitzer G, Schwartz A. Transcranial Doppler ultrasound for the assessment of intracranial arterial flow velocity — Part 1. Examination technique and normal values. Surg Neurol 1987; 27: 439–48.
Pierce EC Jr,Lambertson CJ, Deutsch S, et al. Cerebral circulation and metabolism during thiopental anesthesia and hyperventilation in man. J Clin Invest 1962; 41: 1664–71.
Donegan JH, Traystman RJ, Koehler RC, Jones MD Jr,Rogers MC. Cerebrovascular hypoxic and autoregulator responses during reduced brain metabolism. Am J Physiol 1985; 249: H421–6.
Shapiro K, Marmarou A. Mechanisms of intracranial hypertension in children.In: McLaurin RL, Venes J, Schut L et al. (Eds.). Pediatric Neurosurgery, Philadelphia: W.B. Saunders, 1989; 338–46.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Millar, C., Bissonnette, B. Awake intubation increases intracranial pressure without affecting cerebral blood flow velocity in infants. Can J Anaesth 41, 281–287 (1994). https://doi.org/10.1007/BF03009904
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03009904