
Abstract
Background
The level selected for amputation should generally be the lowest compatible with tissue viability, with a reasonable expectation of wound healing in patients with arterial obstructive leg and foot disease, but determining the amputation level of an ischemic lower limb remains controversial. The general consensus is that a decisive and final decision about the amputation level should be made intraoperatively based on the extent of hemorrhage from the incised skin and soft tissue, and the degree of viability of the stump.
Objective
To estimate the extent of such hemorrhage, and thus suggest the level of amputation preoperatively, the author applied three-phase bone scintigraphy (TPBS) to assess the blood flow in the small arteries and capillary vessels.
Method
TPBS was performed in patients scheduled to undergo lower limb amputation in an attempt to determine the appropriate amputation level preoperatively, objectively, and visually. Imaging results of this examination were compared with the clinical findings in three cases of arterial obstructive foot disease.
Results
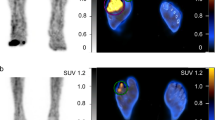
The “capillary phase” depicted the perfusion of blood from the small arteries to the capillary vessels. Decreased accumulation in the capillary phase appeared as two distinctive states: one of clinically remarkable necrosis and the other of decreased blood flow in the small arteries and capillary vessels. The latter inevitably causes necrosis and infection postoperatively.
Conclusion
The results of this study suggest that TPBS is an extremely useful tool in the evaluation of physiological dysfunction and the likely amputation level in patients with arterial obstructive leg and foot disease.
Similar content being viewed by others


References
McCollough III NC. Principles of amputation surgery in vascular disease. InSurgery of the Musculoskeletal System, 2nd ed., New York; Churchill Livingstone, vol. 4 sec. 12, 1983: 25–42.
Burgess EM, Marsden FW. Major lower extremity amputations following arterial reconstruction.Arch Surg 1974; 108: 655–660.
Hunter GA, Waddell JP. Management of the patient requiring leg amputation for peripheral vascular disease.Can Med Assoc J 1976; 115: 634–638.
Romano RL, Burgess EM. Level selection in lower extremity amputations.Clin Orthop 1971; 74: 177–184.
Moore WS. Determination of amputation level. Measurement of skin blood flow with xenon (Xe133).Arch Surg 1973; 107: 798–802.
Gilfillan RS, Leeds FH, Spotts RR. The prediction of healing in ischemic lesions of the foot. A comparison of Doppler ultrasound and elevation reactive hyperemia.J Cardiovasc Surg (Torino) 1985; 26: 15–20.
Burgess EM, Romano RL, Zettl JH, Schrock RD Jr. Amputations of the leg for peripheral vascular insufficiency.J Bone Joint Surg Am 1971; 53: 874–890.
Kihn RB, Warren R, Beebe GW. The “geriatric” amputee.Ann Surg 1972; 176: 305–314.
Mooney V, Wagner FW Jr. Neurocirculatory disorders of the foot.Clin Orthop 1977; 122: 53–61.
Rosenberg N. Midleg amputation in patients with necrotic leg muscles.Arch Surg 1960; 81: 614–617.
Makino N, Ishigaki T, Sakuma S, Takamatsu K, Tsunoda K, Nakamura R. Three-phase bone scintigraphy of Kienbock disease.KAKU IGAKU (Jpn J Nucl Med) 1992; 29: 1419–1427. (in Japanese)
Ritter MM, Richter WO, Leinsinger G, Kirsch CM, Schwandt P. Granulocytes and three-phase bone scintigraphy for differentiation of diabetic gangrene with and without osteomyelitis.Diabetes-Care 1992; 15: 1014–1019.
Larsson J, Agardh CD, Apelqvist J, Stenstrom A. Local signs and symptoms in relation to final amputation level in diabetic patients. A prospective study of 187 patients with foot ulcers.Acta Orthop Scand 1994; 65: 387–393.
Wang CL, Wang M, Liu TK. Predictors for wound healing in ischemic lower limb amputation.J Formos Med Assoc 1994; 93: 849–854.
Siegel ME, Stewart CA, Wagner W, Sakimura I. A new objective criterion for determining, noninvasively, the healing potential of an ischemic ulcer.J Nucl Med 1981; 22: 187–189.
Lassen NA, Lindbjerg J, Munck O. Measurement of blood flow through skeletal muscle by intramuscular injection of Xe-133.Lancet 1964; 1: 686–689.
Young AE, Henderson BA, Couch NP. Muscle perfusion and the healing of below knee amputations.Surg Gynecol Obstet 1978; 146: 533–534.
Brown ML, Holder LE. Selected topics in orthopedic bone scanning. InSkeletal Nuclear Medicine, 1st ed., St. Louis; C. V. Mosby Co., 1996: 261–290.
Cameron GG, Greyson ND, Cumming WA, Lloyd GR, Birch JR. The case of the missing vault: a “cold” bone lesion following electrical burn.Clin Nucl Med 1981; 6: 30–33.
Bozkurt MF, Ugur O. Assessment of penile bone graft viability by bone scintigraphy: a case report.Ann Nucl Med 2000; 14: 377–378.
Kao PF, Tzen KY, Chang LY, Yang JY.99mTc-MDP scintigraphy in high-voltage electrical burn patients.Nucl Med Commun 1997; 18: 846–852.
Chang LY, Yang JY. The role of bone scans in electric burns.Burns 1991; 17: 250–253.
Delpassand ES, Dhekne RD, Barron BJ, Moore WH. Evaluation of soft tissue injury by Tc-99m bone agent scintigraphy.Clin Nucl Med 1991; 16: 309–314.
Mehta RC, Wilson MA. Frostbite injury: prediction of tissue viability with triple-phase bone scanning.Radiology 1989; 170: 511–514.
Schauwecker DS. The role of nuclear medicine in osteomyelitis. InSkeletal Nuclear Medicine 1st ed., St. Louis; C. V. Mosby Co., 1996: 183–202.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Masaoka, S. Evaluation of arterial obstructive leg and foot disease by three-phase bone scintigraphy. Ann Nucl Med 15, 281–287 (2001). https://doi.org/10.1007/BF02987847
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02987847