
Summary
Conclusion
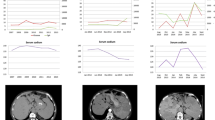
Following resection of a nonfunctioning neuroendocrine carcinoma of the pancreas, subsequent metastases, in the absence of a primary cancer (resected), developed the capacity to secrete ACTH and create the Cushing syndrome.
Background
Although neuroendocrine carcinomas of the pancreas may produce one or more hormones and may switch secretion to a different hormone, no report is identified of a metastasis, in the absence of the primary tumor, developing de novo the capacity to secrete ACTH.
Methods
A nonfunctioning islet cell carcinoma was resected and immunochemically stained for multiple hormones. Three years later hepatic metastases were partially resected and stained as before.
Results
The primary cancer stained negative for ACTH and cortisol, positive for serotonin, and focally positive for gastrin. Three years later, after the development of a florid Cushing syndrome, the metastasis stained strongly for ACTH and negative for serotonin.
Similar content being viewed by others


References
Scarpelli DG. The pancreas, inPathology, 2nd ed, Rubin E, Farber JL, eds. JB Lippincott, Philadelphia, PA, 1994; p. 803.
Doppman JL, Nieman LR, Cutler GB Jr, Chrousos GP, Fraker DL, Norton JA, Jensen RT. Adrenocorticotropic hormone-secreting islet cell tumors: Are they always malignant?Radiology 1994; 190: 59–64.
Schneider C, Mittelmeier HO, Gebhardt C. Cushing’s syndrome from a neuroendocrine pancreatic tumor.Leber Magen Darm 1992; Nov 22(6): 234–236.
Sandler M, Rubin PC, Reid JL, Smith GD. Oat cell carcinoma in the pancreas: An unusual cause of Cushing’s syndrome. Br J Hosp Med 1992; 47(7): 537–538.
Gullo O, DeGiorgio R, D’Errico A, Grigioni W, Parenti M, Corinaldesi R. Pancreatic exocrine carcinoma producing adrenocorticotropic hormone.Pancreas 1992; 7: 172–176.
Walter RM, Ensinck JW, Ricketts H, Kendall JW, Williams RH. Insulin and ACTH production by a streptozotocin responsive islet cell carcinoma.Am J Med 1973; 55: 567.
Hammar S, Sale G. Multiple hormone producing islet cell carcinomas of the pancreas.Hum Pathol 1975; 6(3): 349–362.
Ohneda A, Otsuki M, Fujiya H, Yaginuma N, Kokubo T, Ohtani H.Diabetes 1979; 28: 962.
Asa S, Kovacs K, Killinger DW, Marcon N, Platts M. Pancreatic islet cell carcinoma producing gastrin, ACTH, α-endorphin, somatostatin and calcitonin.Am J Gastroenterol 1980; 74: 30–35.
Vieweg WVR, Graber AL, Cerchio GM. Pancreatic islet cell carcinoma with hyperinsulinism and probably ectopic ACTH-MSH secretion.Arch Intern Med (Chicago) 1969; 124: 731
Curnow RT, Carey RM, Taylor A, Johanson A, Murad F. Somatostatin inhibition of insulin and gastrin hypersecretion in pancreatic islet-cell carcinoma.New Engl J Med 1975; 292: 1385–1386.
Souquet JC, Sassolas G, Forichon J, Champetier P, Partenzky C, Chayvialle JA. Clinical and hormonal effects of a long-lasting somatostatin analogue in pancreatic endocrine tumors and in carcinoid syndrome.Cancer 1987; 59: 1654–1660.
Bertagna X, Favrod-Coune C, Escourolle H, Beuzeboc P, Christoforov B, Girard F, Luton JP. Suppression of ectopic adrenocorticotropin secretion by the long-acting somatostatin analog octreotide.J Clin Endocrinol Metab 1989; 66(5) 988–991.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Zhu, L., Domenico, D.R. & Howard, J.M. Metastatic pancreatic neuroendocrine carcinoma causing Cushing’s syndrome. Int J Pancreatol 19, 205–208 (1996). https://doi.org/10.1007/BF02787369
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02787369