
Abstract
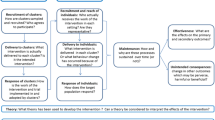
For quality improvement (QI) projects, the Translating Research into Practice (TRiP) framework is an ideal model for developing and addressing topics locally (see Fig. 6.1) (Pronovost et al. BMJ 337:a1714, 2008). The TRiP framework is a four-step process that evaluates best practices with the goal of creating strategies for implementation at a local level. Using high-quality evidence, the TRiP framework utilizes multidisciplinary collaboration to incorporate knowledge translation for broader dissemination of knowledge into practice. Each step focuses on systems of care rather than care of individual patients with engagement of multidisciplinary teams to assume ownership of the QI project. Finally, this framework encourages adaptation so that the QI intervention can meet the culture of the implementing group when expanded regionally or nationally (Pronovost et al. BMJ 337:a1714, 2008). At the Johns Hopkins Hospital, we have successfully utilized this framework to reduce central line-associated blood stream infections (Pronovost et al. BMJ 340:c309, 2010) and improve prescription of risk-appropriate venous thromboembolism (VTE) prophylaxis (Streiff et al. BMJ 344:e3935, 2012). For this purposes of this chapter we will give examples of these successful interventions, though each step can be applied to meet different quality improvement goals.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
Similar content being viewed by others

References
Aboagye JK, Lau BD, Schneider EB, Streiff MB, Haut ER. Linking processes and outcomes: a key strategy to prevent and report harm from venous thromboembolism in surgical patients. JAMA Surg. 2013;148(3):299–300. doi:10.1001/jamasurg.2013.1400.
Bilimoria KY, Chung J, Ju MH, et al. Evaluation of surveillance bias and the validity of the venous thromboembolism quality measure. JAMA. 2013;310(14):1482–9. doi:10.1001/jama.2013.280048.
Campbell R. The five "rights" of clinical decision support. J AHIMA. 2013;84(10):42–7; quiz 48.
Fan E, Laupacis A, Pronovost PJ, Guyatt GH, Needham DM. How to use an article about quality improvement. JAMA. 2010;304(20):2279–87. doi:10.1001/jama.2010.1692.
Garonzik-Wang JM, Brat G, Salazar JH, et al. Missing consent forms in the preoperative area: a single-center assessment of the scope of the problem and its downstream effects. JAMA Surg. 2013;148(9):886–9. doi:10.1001/jamasurg.2013.354.
Goldhaber SZ, Tapson VF, DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004;93(2):259–62.
Haut ER, Pronovost PJ. Surveillance bias in outcomes reporting. JAMA. 2011;305(23):2462–3.
Haut ER, Lau BD, Kraenzlin FS, et al. Improved prophylaxis and decreased preventable harm with a mandatory computerized clinical decision support tool for venous thromboembolism (VTE) prophylaxis in trauma patients. Arch Surg. 2012;10(147):901–7.
Haut ER, Lau BD, Kraus PS, et al. Preventability of hospital-acquired venous thromboembolism. JAMA Surg. 2015;150(9):912. doi:10.1001/jamasurg.2015.1340.
Holzmueller CG, Pronovost PJ. Organising a manuscript reporting quality improvement or patient safety research. BMJ Qual Saf. 2013;22(9):777–85. doi:10.1136/bmjqs-2012-001603.
Johnbull EA, Lau BD, Schneider EB, Streiff MB, Haut ER. No association between hospital-reported perioperative venous thromboembolism prophylaxis and outcome rates in publicly reported data. JAMA Surg. 2014;149(4):400–1. doi:10.1001/jamasurg.2013.4935.
Kardooni S, Haut ER, Chang DC, et al. Hazards of benchmarking complications with the National Trauma Data Bank: numerators in search of denominators. J Trauma. 2008;64(2):273–7. doi:10.1097/TA.0b013e31816335ae; discussion 277–9.
Lau BD, Haut ER. Practices to prevent venous thromboembolism: a brief review. BMJ Qual Saf. 2014;23(3):187–95.
Lau BD, Haider AH, Streiff MB, et al. Eliminating health care disparities with mandatory clinical decision support: the venous thromboembolism (VTE) example. Med Care. 2015a;53(1):18–24. doi:10.1097/MLR.0000000000000251.
Lau BD, Streiff MB, Pronovost PJ, Haider AH, Efron DT, Haut ER. Attending physician performance measure scores and resident physicians’ ordering practices. JAMA Surg. 2015b;150(8):813–4. doi:10.1001/jamasurg.2015.0891.
Lau BD, Arnaoutakis GA, Streiff MB, et al. Individualized performance feedback to surgical residents improves appropriate venous thromboembolism (VTE) prophylaxis prescription and reduces potentially preventable VTE: a prospective cohort study. Ann Surg. 2015c. [Epub ahead of print]. http://www.ncbi.nlm.nih.gov/pubmed/26649586.
Lau BD, Streiff MB, Hobson DB, et al. Beneficial “Halo Effects” of surgical resident performance feedback. J Surg Res. 2016. http://www.ncbi.nlm.nih.gov/pubmed/26649586 .
Monn MF, Haut ER, Lau BD, et al. Is venous thromboembolism in colorectal surgery patients preventable or inevitable: one institution’s experience. J Am Coll Surg. 2013;216(3):395–401.
Pierce CA, Haut ER, Kardooni S, et al. Surveillance bias and deep vein thrombosis in the national trauma data bank: the more we look, the more we find. J Trauma. 2008;64(4):932–6. doi:10.1097/TA.0b013e318166b808; discussion 936–7.
Pronovost PJ, Berenholtz SM, Goeschel CA, et al. Creating high reliability in health care organizations. Health Serv Res. 2006;41(4 Pt 2):1599–617. doi: HESR567 [pii].
Pronovost PJ, Berenholtz SM, Needham DM. Translating evidence into practice: a model for large scale knowledge translation. BMJ. 2008;337:a1714. doi:10.1136/bmj.a1714.
Pronovost PJ, Goeschel CA, Colantuoni E, et al. Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study. BMJ. 2010;340:c309. doi:10.1136/bmj.c309.
Shermock KM, Lau BD, Haut ER, et al. Patterns of non-administration of ordered doses of venous thromboembolism prophylaxis: implications for novel intervention strategies. PLoS One. 2013;8(6):e66311. doi:10.1371/journal.pone.0066311.
Streiff MB, Carolan H, Hobson DB, et al. Lessons from the Johns Hopkins Multi-Disciplinary Venous Thromboembolism (VTE) Prevention Collaborative. BMJ. 2012;344:e3935.
Timmel J, Kent PS, Holzmueller CG, Paine L, Schulick RD, Pronovost PJ. Impact of the Comprehensive Unit-based Safety Program (CUSP) on safety culture in a surgical inpatient unit. Jt Comm J Qual Patient Saf. 2010;36(6):252–60.
Zeidan AM, Streiff MB, Lau BD, et al. Impact of a venous thromboembolism prophylaxis "smart order set": improved compliance, fewer events. Am J Hematol. 2013;88(7):545–9. doi:10.1002/ajh.23450.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Lau, B.D., Haut, E.R. (2017). How to Address a Quality Problem. In: Kelz, R., Wong, S. (eds) Surgical Quality Improvement. Success in Academic Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-23356-7_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-23356-7_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23355-0
Online ISBN: 978-3-319-23356-7
eBook Packages: MedicineMedicine (R0)