
Abstract
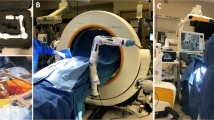
Introduction: Various minimally invasive spine surgery (MISS) techniques have been developed with the goal of reducing approach-related soft-tissue trauma and its associated complications. However, there is still a debate on some of the potential drawbacks of MISS techniques, such as their longer operating times and increased intraoperative radiation. A solution to these disadvantages could be the implementation of new technologies, such as computer-assisted navigation (CAN) and surgical robotics. We compare the standard fluoroscopy MISS technique with our experience with time per screw and X-ray exposure for pedicle screw placement using the Brainlab Cirq passive robotic arm assistance coupled with the Brainlab Curve navigation system.
Methods: In the Cirq robot-assisted group (Group I), 109 screws were placed in 24 prospectively analyzed patients. In the fluoroscopy-guided group, 108 screws inserted into 20 consecutive patients were analyzed retrospectively (Group II). The duration of surgery, the time to place one screw, the X-ray exposition, and the pedicle screw accuracy for each patient were recorded and reviewed.
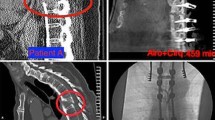
Results: In total, 217 screws were analyzed. The treated levels ranged from T10 to S1. In Group I, 104 screws were grade A (95.4%) and five were grade B (4.6%). In Group II, 96 screws were grade A (88.89%); ten were grade B (9.26%); one was grade C (0.93%), and one was grade D (0.93%). While the screws placed by using the Cirq system were more accurate overall, there was no statistical significance when the two groups were compared, p = 0.3724. There was no significant difference in radiation exposure between the two groups, p = 0.5482; however the radiation exposure for the surgeon was very limited with the Cirq system. There was a significant reduction in the operation length (p = 0.0183) and the time per screw (p < 0.0001) for Group I.
Conclusions: The CAN systems and emerging robotic platforms have the potential to diminish the main disadvantages of MISS techniques—longer operation times and X-ray exposure, at least for the surgical team.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
Similar content being viewed by others

References
Burneikiene S, Roeca C, Nelson L, Mason A, Villavicencio A. Minimally invasive versus open transforaminal lumbar interbody fusion. Surg Neurol Int. 2010;1(1):12. https://doi.org/10.4103/2152-7806.63905.
Walker CT, Xu DS, Godzik J, Turner JD, Uribe JS, Smith WD. Minimally invasive surgery for thoracolumbar spinal trauma. Ann Transl Med. 2018;6(6):102. https://doi.org/10.21037/atm.2018.02.10.
Phan K, Rao PJ, Kam AC, Mobbs RJ. Minimally invasive versus open transforaminal lumbar interbody fusion for treatment of degenerative lumbar disease: systematic review and meta-analysis. Eur Spine J. 2015;24(5):1017–30. https://doi.org/10.1007/s00586-015-3903-4.
Gertzbein SD, Robbins SE. Accuracy of pedicular screw placement in vivo. Spine. 1990;15(1):11–4. https://doi.org/10.1097/00007632-199001000-00004.
Vazan M, Gempt J, Meyer B, Buchmann N, Ryang Y-M. Minimally invasive transforaminal lumbar interbody fusion versus open transforaminal lumbar interbody fusion: a technical description and review of the literature. Acta Neurochir. 2017;159(6):1137–46. https://doi.org/10.1007/s00701-017-3078-3.
Brodano GB, Martikos K, Lolli F, et al. Transforaminal lumbar interbody fusion in degenerative disk disease and spondylolisthesis grade I. J Spinal Disord Tech. 2015;28(10):E559–64. https://doi.org/10.1097/BSD.0000000000000034.
Schizas C, Tzinieris N, Tsiridis E, Kosmopoulos V. Minimally invasive versus open transforaminal lumbar interbody fusion: evaluating initial experience. Int Orthop. 2009;33(6):1683–8. https://doi.org/10.1007/s00264-008-0687-8.
Fayed I, Tai A, Triano M, et al. Robot-assisted percutaneous pedicle screw placement: evaluation of accuracy of the first 100 screws and comparison with cohort of fluoroscopy-guided screws. World Neurosurg. 2020;143:e492–502.
Yang JS, He B, Tian F, et al. Accuracy of robot-assisted percutaneous pedicle screw placement for treatment of lumbar spondylolisthesis: a comparative cohort study. Med Sci Monit. 2019;25:2479–87.
Vaccaro AR, Harris JA, Hussain MM, et al. Assessment of surgical procedural time, pedicle screw accuracy, and clinician radiation exposure of a novel robotic navigation system compared with conventional open and percutaneous freehand techniques: a cadaveric investigation. Glob Spine J. 2020;10(7):814–25.
Kim CW, Lee Y-P, Taylor W, Oygar A, Kim WK. Use of navigation-assisted fluoroscopy to decrease radiation exposure during minimally invasive spine surgery. Spine J. 2008;8(4):584–90. https://doi.org/10.1016/j.spinee.2006.12.012.
Fomekong E, Safi SE, Raftopoulos C. Spine navigation based on 3-dimensional robotic fluoroscopy for accurate percutaneous pedicle screw placement: a prospective study of 66 consecutive cases. World Neurosurg. 2017;108:76–83. https://doi.org/10.1016/j.wneu.2017.08.149.
Fan Y, Du J, Zhang J, Liu S, Xue X, Huang Y, Zhang J, Hao D. Comparison of accuracy of pedicle screw insertion among 4 guided technologies in spine surgery. Med Sci Monit. 2017;23:5960–8. https://doi.org/10.12659/MSM.905713.
Hicks JM, Singla A, Shen FH, Arlet V. Complications of pedicle screw fixation in scoliosis surgery. Spine. 2010;35(11):E465–70. https://doi.org/10.1097/BRS.0b013e3181d1021a.
Gautschi OP, Schatlo B, Schaller K, Tessitore E. Clinically relevant complications related to pedicle screw placement in thoracolumbar surgery and their management: a literature review of 35,630 pedicle screws. Neurosurgical Focus. 2011;31(4):E8. https://doi.org/10.3171/2011.7.FOCUS11168.
Lonjon N, Chan-Seng E, Costalat V, Bonnafoux B, Vassal M, Boetto J. Robot-assisted spine surgery: feasibility study through a prospective case-matched analysis. Eur Spine J. 2016;25(3):947–55. https://doi.org/10.1007/s00586-015-3758-8.
Li H-M, Zhang R-J, Shen C-L. Accuracy of pedicle screw placement and clinical outcomes of robot-assisted technique versus conventional freehand technique in spine surgery from nine randomized controlled trials. Spine. 2020;45(2):E111–9. https://doi.org/10.1097/BRS.0000000000003193.
Further Reading
Theocharopoulos N, Perisinakis K, Damilakis J, Papadokostakis G, Hadjipavlou A, Gourtsoyiannis N. Occupational exposure from common fluoroscopic projections used in orthopaedic surgery. J Bone Jt Surg Am. 2003;85(9):1698–703. https://doi.org/10.2106/00004623-200309000-00007.
Acknowledgments
Part of this study was made in close collaboration with the Technical University of Sofia in the framework of the Operational Program “Science and Education for Smart Growth 2014–2020” and “Construction and Development of Centers of Excellence”—2018: National Center for Mechatronics and Clean Technologies—BG05M2OP001-1.001-0008-С01.
Special thanks go to Dr. Ilina Iordanova for her valuable input in this study.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Ethics declarations
All procedures performed in studies involving human participants were carried out in accordance with the ethical standards of the institutional committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the local institutional ethics committee of University Hospital “Pirogov.”
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gabrovsky, N., Ilkov, P., Laleva, M. (2023). Cirq Robotic Assistance for Thoracolumbar Pedicle Screw Placement: Overcoming the Disadvantages of Minimally Invasive Spine Surgery. In: Visocchi, M. (eds) The Funnel: From the Skull Base to the Sacrum. Acta Neurochirurgica Supplement, vol 135. Springer, Cham. https://doi.org/10.1007/978-3-031-36084-8_59
Download citation
DOI: https://doi.org/10.1007/978-3-031-36084-8_59
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-36083-1
Online ISBN: 978-3-031-36084-8
eBook Packages: MedicineMedicine (R0)