
Abstract
Purpose
Radiotherapy (RT) and temozolomide (TMZ) for glioblastoma (GBM) has resulted in longer survival. Uncertainties exist regarding quality of survival. This study aims to determine the rate of patients returning to previous employment (EM) following treatment.
Methods
Eligible patients were diagnosed with GBM, aged 18–70 years, and treated with intensity-modulated radiotherapy to 60 Gray and TMZ (EORTC Protocol) between July 2007 and July 2011. EM was defined as paid work. Exclusion criteria included patients without histological confirmation of WHO grade IV glioblastoma, those not in paid employment in the 2-month period prior to diagnosis, or mothers of pre-school aged children not working. Data were collected on EM prior (EM pre) and after RT at 6 and 12 months (EM 6 m, EM 12 m). Rate of EM was analysed in regards to baseline performance status (ECOG), neurological deficits (MRC scale) and median survival.
Results
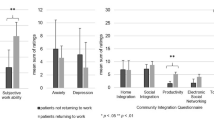
One hundred twelve patients were identified with median follow-up of 15.5 months and median survival 18 months (95%CI, 15–21 months). Seventy-one patients were working prior to diagnosis and eligible for analysis. Twenty patients returned to work (28 %) by EM 6 months and 19 patients (27 %) by EM 12 months. EM 6 months was strongly associated with ECOG and MRC status, with only 1 of 37 patients (3 %) with neurological deficit returning to work compared with 21 of 36 (58 %) intact patients. Of good performance status patients not returning to work, factors included presence of income insurance, family financial support or treatment-related symptoms.
Conclusion
A modest proportion of patients with GBM return back to work at 6 and 12 months following radiotherapy with the majority demonstrating the lowest level of neurological deficit prior to RT.
Implications for Cancer Survivors
Return to work following treatment does occur but it is not a common outcome.


Similar content being viewed by others


Notes
Source: “Statistics on Incidence, Survival Rates and Mortality Associated with Brain Tumours in Australia”, Information Paper for the Australian Brain Tumour Advocacy Group, Denise Chang, June 2003.
References
Chandana SR, Movva S, Arora M, Singh T. Primary brain tumors in adults. Am Fam Physician. 2008;77(10):1423–30.
Dobes M, Khurana VG, Shadbolt B, Jain S, Smith SF, Smee R, et al. Increasing incidence of glioblastoma multiforme and meningioma, and decreasing incidence of Schwannoma (2000–2008): findings of a multicenter Australian study. Surg Neurol Int. 2011;2:176.
Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJB, Janzer RC, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–66.
Rønning PA, Helseth E, Meling TR, Johannesen TB. A population-based study on the effect of temozolomide in the treatment of glioblastoma multiforme. Neuro-oncology. 2012;14(9):1178–84.
Johnson DR, O’Neill BP. Glioblastoma survival in the United States before and during the temozolomide era. J Neurooncol. 2012;107(2):359–64.
Steinbach J, Blaicher H, Herrlinger U, Wick W, Nagele T, Meyermann R, et al. Surviving glioblastoma for more than 5 years: the patient’s perspective. Neurology. 2006;66(2):239–42.
Remer S, Murphy M. The challenges of long-term treatment outcomes in adults with malignant gliomas. Journal of Oncology Nursing. 2004;8(4):368–76 [Review] [36 refs][Erratum appears in Clin J Oncol Nurs. 2004 Oct;8(5):448].
Hahn C, Dunn R, Logue P, King J, Edwards C, Halperin E. Prospective study of neuropsychologic testing and quality-of-life assessment of adults with primary malignant brain tumors. Journal of Radiation Oncology. 2003;55(4):992–9.
Efficace F, Bottomley A. Assessing HRQOL: a neglected issue for high-grade glioma. The Lancet Oncology. 2003;4(1):11–2.
Mauer M, Stupp R, Taphoorn MJB, Coens C, Osoba D, Marosi C, et al. The prognostic value of health-related quality-of-life data in predicting survival in glioblastoma cancer patients: results from an international randomised phase III EORTC Brain Tumour and Radiation Oncology Groups, and NCIC Clinical Trials Group study. Br J Cancer. 2007;97(3):302–7.
Meyers C, Hess K. Multifaceted end points in brain tumor clinical trials: cognitive deterioration precedes MRI progression. Neuro-Oncology. 2003;5(2):89–95.
Kleinberg L, Wallner K, Malkin MG. Good performance status of long-term disease-free survivors of intracranial gliomas. Int J Radiat Oncol Biol Phys. 1993;26(1):129–33.
Main DS, Nowels CT, Cavender TA, Etschmaier M, Steiner JF. A qualitative study of work and work return in cancer survivors. Psycho-Oncology. 2005;14(11):992–1004.
Lyons M, Orozovic N, Davis J, Newman J. Doing-being-becoming: occupational experiences of persons with life-threatening illnesses. Journal of Occupational Therapy May. 2002;56(3):285–95.
Freedman RI, Fesko SL. The meaning of work in the lives of people with significant disabilities: consumer and family perspectives. Journal of Rehabilitation. 1996;62(3):49–55.
Feuerstein M, Todd BL, Moskowitz MC, Bruns GL, Stoler MR, Nassif T, et al. Work in cancer survivors: a model for practice and research. Journal of Cancer Survivorship. 2010;4(4):415–37.
de Boer AM, Taskila T, Ojajärvi A, van Dijk FH, Verbeek JM. Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA. 2009;301(7):753–62.
Dyck PJ, Boes CJ, Mulder D, Millikan C, Windebank AJ, Dyck PJB, et al. History of standard scoring, notation, and summation of neuromuscular signs. A current survey and recommendation. J Peripher Nerv Syst. 2005;10(2):158–73.
Statistics c = AU; o = Commonwealth of A ou = Australian B of. Details—about this release [Internet]. [cited 2013 Jul 25]. Available from: http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/1220.01997?OpenDocument
Taphoorn MJ, Stupp R, Coens C, Osoba D, Kortmann R, van den Bent MJ, et al. Health-related quality of life in patients with glioblastoma: a randomised controlled trial. The Lancet Oncology. 2005;6(12):937–44.
Giovagnoli A. Quality of life in patients with stable disease after surgery, radiotherapy, and chemotherapy for malignant brain tumour. J Neurol Neurosurg Psychiatry. 1999;67(3):358–63.
Schipper H, Clinch J, McMurray A, Levitt M. Measuring the quality of life of cancer patients: the Functional Living Index-Cancer: development and validation. J Clin Oncol. 1984;2(5):472–83.
Ganz PA, Haskell CM, Figlin RA, La Soto N, Siau J. Estimating the quality of life in a clinical trial of patients with metastatic lung cancer using the Karnofsky performance status and the Functional Living Index–Cancer. Cancer. 1988;61(4):849–56.
Butler Jr JM, Case LD, Atkins J, Frizzell B, Sanders G, Griffin P, et al. A phase III, double-blind, placebo-controlled prospective randomized clinical trial of d-threo-methylphenidate HCl in brain tumor patients receiving radiation therapy. Int J Radiat Oncol Biol Phys. 2007;69(5):1496–501.
Spelten ER, Sprangers MAG, Verbeek JHA. Factors reported to influence the return to work of cancer survivors: a literature review. Psycho-Oncology. 2002;11(2):124–31.
Kaleita TA, Wellisch DK, Cloughesy TF, Ford JM, Freeman D, Belin TR, et al. Prediction of neurocognitive outcome in adult brain tumor patients. J Neurooncol. 2004;67(1–2):245–53.
Calvio L, Feuerstein M, Hansen J, Luff GM. Cognitive limitations in occupationally active malignant brain tumour survivors. Occup Med (Lond). 2009;59(6):406–12.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gzell, C., Wheeler, H., Guo, L. et al. Employment following chemoradiotherapy in glioblastoma: a prospective case series. J Cancer Surviv 8, 108–113 (2014). https://doi.org/10.1007/s11764-013-0311-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-013-0311-9