
Abstract
Plague caused by Yersinia pestis is a zoonotic infection, i.e., it is maintained in wildlife by animal reservoirs and on occasion spills over into human populations, causing outbreaks of different entities. Large epidemics of plague, which have had significant demographic, social, and economic consequences, have been recorded in Western European historical documents since the sixth century. Plague has remained in Europe for over 1400 years, intermittently disappearing, yet it is not clear if there were reservoirs for Y. pestis in Western Europe or if the pathogen was rather reimported on different occasions from Asian reservoirs by human agency. The latter hypothesis thus far seems to be the most plausible one, as it is sustained by both ecological and climatological evidence, helping to interpret the phylogeny of this bacterium.
Similar content being viewed by others

Keywords
When traveling around in Europe today, we can still find monuments everywhere evoking the ancient pestilences, monuments such as churches, chapels, columns, and altarpieces [1]. In addition, historical hospitals and lazarettos, and other buildings,Footnote 1 recall the past plagues, as do plenty of paintings, tableaus, pictures, sculptures, and wax reliefs. Plague is also depicted in certain famous novels, such as Boccaccio’s The Decameron, Manzoni’s I Promessi Sposi, Daniel Defoe’s A Journal of the Plague Year, and Camus’ La Peste, as well as in fables such as “Les Animaux Malades de la Peste” by La Fontaine. The terms “pest,” “plague,” and “pestilence” are also so commonly incorporated in expressions and proverbs in any European languageFootnote 2 that, more or less consciously, the collective memory refers to past epidemics continuously. Even in drugstores we can find memories of the past plagues: from antiquity onward perfumes were often used as medicine and additionally in the Middle Ages to ward off the bubonic plague. This medicinal property was, for instance, attributed to the original Eau de Cologne that was launched in Cologne in 1709 by Giovanni Maria Farina (and is still commercialized to this day).Footnote 3 Although perfumes were not efficient disinfectants, their scent at least might have helped to reduce the unbearable odors linked to the pestilence. In vivid depictions by contemporary chroniclers, painters, and sculptors, victims were often portrayed as affected by strong coughing followed by hemoptysis (i.e., spitting of blood) and sometimes exhibiting suppurative lymphadenopathy (buboes) or necrotic extremities. Plague victims were depicted as suddenly falling down dead in the street, their bodies carted off by carriage and thrown in large plague pits containing a number of corpses deposited in layers “like lasagna.”Footnote 4 The smell must have been truly horrific and not easily masked by the use of perfume.
Besides leaving a horrific and distressing impression, plague had a long-lasting impact on the history of Europe (in terms of social, political, and economical developments) as over centuries it repeatedly hit cities and villages, with devastating demographic consequences. The Black Death itself (1346–1353) has been estimated to have reduced the population in the affected areas of Europe by about one third, by the middle of the fourteenth century. A second plague epidemic occurred in 1358 in parts of Italy and Germany and spread to large parts of Europe (e.g., to Norway in 1359–1361), whereas a third epidemic spread in the mid-1370s (again including Norway). As a result, for areas of Europe where estimates are available, we know that by 1400, the population in these areas decreased to less than half of what it was before the Black Death [2, 3]. The sequence of plague epidemics continued in Western Europe until the mid-seventeenth century. In countries for which records are available, we know that there were between 20 and 30 epidemics of plague during the course of 300 years. The population of Europe was kept low during this whole period and only started to increase substantially again after the mid-seventeenth century.
1.1 Three Historical Plague Pandemics
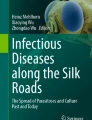
“Plague,” “pestilence,” and “pest” are general terms often used in the past to describe catastrophic events. By reviewing historical records, historians have proposed that only three pandemics (Fig. 1.1) were effectively consistent with the infectious disease currently called plague, caused by the gram-negative coccobacillus Yersinia pestis. A caveat here is that, as we go further back in time, historic sources become more rare and more succinct, which limits our ability to tie a particular pathogen to an epidemic. We cannot therefore exclude the possibility that there have been earlier pandemics of plague, but can merely assert that there is currently no clear historic evidence for such pandemics.

Spatial distribution of the three plague pandemics. The distinction among the three plague pandemics and their classification is still under debate. We use here the historical definition of the three plague pandemics without taking into consideration the genetic differentiation of the distinct strains causing the outbreaks. Black dots indicate the known distribution of plague outbreaks in the period of the first pandemic (Source: Little and Rome [5] in main text), red dots those during the second pandemic (Source: Schmid et al. [79] in main text, Haesser 1875 [87], Ilmoni 1853 [88], Walløe 1995 [89]) and colored shadows those during the third pandemic. (The dataset used for the third pandemic was obtained from worldwide WHO records, and other published papers or databases. The compilation of this catalog was supported by the NSFC Project No.31420103913)
The first plague pandemic, as described by Procopius, started in the middle of the sixth century in Egypt and spread rapidly to the whole Mediterranean Basin. From Pelusium on the Nile Delta, it reached Constantinople by ship in 541–542 CE: this first outbreak, which marks the onset of the first pandemic, is generally referred to as the “Justinian plague” due to the name of the Byzantine emperor at the time, Justinian. Although the source of this pandemic is not known, contemporaneous chronicles placed the origin of the plague in Axum, in the southeastern region of Africa, which was an important naval and trading connection to the East. India has also been proposed by historians as a possible source for this plague, as well as the Great Steppe region in Asia [4]. As for its spreading, few reports attest to the presence of plague in the northern part of Europe, but it is generally considered that plague quickly spread to the Rhine region and Ireland [5]. Repeated cycles of plague epidemics are known to have occurred in Europe following the Justinian outbreak and to have continued until 750 CE.
The second pandemic began with the devastating outbreak of the fourteenth century, now referred to as the Black Death (1346–1353). From Caffa on the Caspian Sea, plague spread to all of Europe and persisted there with a series of intermittent epidemics until the middle of the eighteenth century, after which it virtually disappeared from the continent [6]. The last official epidemic is considered to have occurred in Moscow in 1771, although other outbreaks were also recorded later and the pandemic may have persisted in parts of EuropeFootnote 5 until the end of the nineteenth century [7]. The origin of the Black Death is not well known, but according to historical records, the disease may have traveled with Mongol armies to the Crimea where it was further transported via Genoese ships to the West. Inscriptions found on Nestorian graves near Lake Issyk-Kul in Kyrgyzstan (1338–1339), Central Asia, refer to an unknown epidemic, but there is no direct proof that it was due to plague.
Historians regard the third pandemicFootnote 6 to have started in 1772 in Yunnan Province, southwest China, infecting approximately 2.6 million people and causing 2.2 million deaths in China alone [8]. The pandemic’s time of origin is still debated – there is evidence of the presence of plague in China at least as far back as 1644 and 1754, but from 1772 onward, continuous records of epidemics were reported. From Yunnan Province, plague spread to the southeast coast and reached Beihai in 1867. Plague was recorded in Taiwan Province in 1869 and Hainan Island in 1882. In February 1894, plague spread to Guangzhou Province (Canton) and resulted in the death of approximately 70,000 people. In the same year, the infection reached Hong Kong and from there spread globally via maritime shipping [9]. In northeast China, plague killed tens of thousands of people between the years of 1910 and 1920 [9]. Europe was not significantly infected during this pandemic,Footnote 7 whereas Asia, America, Australia, and Africa were impacted. In these years, plague reached at least two new continents where the disease had never been recorded before: Australia and South and North America.
Officially, the third pandemic is still ongoing, although human cases are mainly limited to those resulting from contact with rodents from wildlife plague reservoirs, followed by small localized outbreaks [10]. Nevertheless, the number of human cases is substantial: between 1954 and 1997, the World Health Organization (WHO) received reports of plague from 38 countries, with notification of 80,613 cases and 6587 deaths.Footnote 8 In some places like Madagascar, where plague was introduced in 1898, epidemics have struck nearly every year: in early 2015 the death toll was 79 and in early 2016, it was 63 out of at least 174 detected cases.Footnote 9 Plague continues to be closely monitored, as it is listed by the WHO in its report on the global surveillance of epidemic-prone infectious diseases,Footnote 10 along with eight other diseases which pose important public health threats. Its prevalence is controlled in endemic regions of 478 countries, regions which cover substantial areas. In China alone, where 24 human cases of plague were reported from 2009 to 2014, the endemic area covers approximately 1.5 million km2.
1.2 A Brief History of the Study of Plague
From antiquity until the nineteenth century, medical knowledge based its explanation for infectious diseases on the miasmatic theory. This theory postulated that diseases and epidemics were caused by poisoned air (miasma) and were detectable by the accompanying foul smell. The miasma was thought to contain dangerous particles, particles originating from decomposing biological matter and dispersed by the winds under particular astrological and climatic conditions. This bad air then entered the human body through the skin’s open pores and produced disease, plague included.
In order to combat the spread of plague, several measures were taken based on the medical knowledge of the day. To reduce the risk of dangerous particles entering the skin’s pores to begin with, warm baths were discouraged and thermal and common baths were in general closed during plague outbreaks.Footnote 11 The belongings of victims as well as their clothing were also considered poisoned, and contact with the fur of pets was not recommended – in fact the historical records show that cats were killed during plague outbreaks. In the late Middle Ages, other measures were introduced in places such as Ragusa (and later Milan and Venice) to fight the spread of the infection. These measures included the implementation of quarantine and cordon sanitaire and the prohibition of human assemblages (e.g., [11]).
From the middle of the eighteenth century, the early part of the Enlightenment era, scientific and medical information about plague started to be collected in a more rational and empirical way, in contrast to previous data which was largely anecdotal. Evidence for this shift can be found in a large number of annotations related to plague by scholars in different fields: medicine (symptoms, disease progression, autoptic evidenceFootnote 12), epidemiology (ethnic groups and social classes involved, age, gender, and type of exposed worker), ecology (seasonality of the outbreaks, climatic conditions, susceptible animals and their ecological niches), hygiene (information about public and private hygiene, infections within the household, effectiveness of measures such as quarantine and cordon sanitaire), and geography (places of origin and spread of the plague). Experiments were even carried out in the nineteenth century, mostly to determine the susceptibility of different animals to plague [12], but also in some cases to test susceptibility in humans. The goal of these experiments was primarily to disclose the nature and the mechanisms of the human contagion and assess whether it was a contagious disease at all.Footnote 13 As a result, a large body of accurate knowledge on the disease and how it spread was accumulated, even before the dawn of the bacteriological era (see, e.g., de Merens).
At the end of the nineteenth century, thanks to Robert Koch and Louis Pasteur, the introduction of a new discipline, medical bacteriology, provided a challenge to the miasma theory, though consensus was not reached immediately. During the plague of Hong Kong in 1894, the etiological agent of the epidemic was discovered by Alexander Yersin: following the advice in his publication [13], plague was officially recognized as an infectious disease produced by the bacterium Pasteurella pestis. The bacterium’s name was later changed to Yersinia pestis in the 1950s, in part to honor Yersin’s contributions, but also as microbiologists needed a new family name due to changes in the systematic division. The discovery of Y. pestis, supported by microscopical and experimental evidence, led to a drastic change in medical plague perspectives, as the medical community realized that a microorganism – and not polluted air – was the culprit of the common symptoms of the pathology.
From the clinical point of view, three different presentations of the plague were eventually recognized: bubonic, septicemic, and pneumonic. In bubonic plague, small numbers of Y. pestis penetrate a lymphatic vessel, interact with macrophages, and rapidly migrate to the local draining lymph nodeFootnote 14 where they multiply and give rise to enlarged purulent abscesses called “buboes” [14]. In the attempt to fight against the pathogen, the body reacts with a severe inflammatory response and symptoms such as fever, headache, confusion, or delirium. The period of incubation is generally 1–2 weeks and symptoms can persist some days. Without any antibiotic treatment, about 40–70 % of those affected by bubonic plague die because of cardiotoxins released from the buboes. Bubonic plague can also evolve into septicemic plague, which results in a high-level bacteremia and septicemia, characterized by hemorrhagic and necrotic spots on the skin and rapidly followed by septicemic shock and exitus. Septicemic plague will also develop as primary form if Y. pestis is injected directly into a blood vessel. Pneumonic plague can either develop when Y. pestis is directly inhaled, causing a fatal pneumonia, or it can emerge as a secondary form from either bubonic or septicemic plague; in any case, and as with septicemic plague, this severe form of the disease is always fatal and kills its victims within 2–3 days after the onset of the first symptoms.
Returning now to the outbreak in Hong Kong in 1894, Yersin made another important observationFootnote 15: he noted that the streets were littered with dead black rats (Rattus rattus). A similar observation was also annotated by the Japanese physician Ogata Masanori on Formosa in 1897: he defined the outbreak as a “rat pest” and showed that rat fleas (Xenopsylla cheopis) carried the plague bacillus. Shortly after, in 1898, the French physician Paul-Louis Simond refined this concept: besides the unusually large number of dead rats on the streets of Karachi, he also reported the presence of lesions on the legs and feet of plague patients that could have been caused by the bite of a hematophagous insect, likely the flea. With a very simple experiment, using the infected fleas of an infected rat, he showed that the bacillus could be transmitted by the bites of the rat fleas to a healthy rat. However, Simond’s conclusion that plague can be transmitted to humans by the bites of infected fleas was only accepted about 10 years later by medical authorities, when independent experiments irrefutably confirmed his results: when a rat is dead and its blood temperature decreases, its infected fleas abandon the cadaver and infest the next host, a rat or another mammal, humans not excluded, and transmit the plague bacillus with their bites.
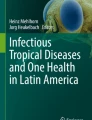
This advancement in scientific understanding was what public health authorities needed to effectively implement measures in the fight against plague. Worldwide, following the motto “avoid the rat-flea-human transmission chain,” massive rat-proofing measures were instituted [15]. In maritime vessels (Fig. 1.2) and port facilities, rats were caught and killed, vessels were fumigated, and insecticides were used in any suspected area, while putative infected patients were isolated in quarantine stations. Hygiene was improved in areas close to wharves, as streets were cleansed and houses disinfected as soon as new cases were reported. The population was alerted and kept informed via newspaper advertisements, posters, and pamphlets. Throughout the outbreaks, some rudimentary types of vaccines were tentatively inoculated, although supplies soon ran out among the public in panic [16]. Thanks to all these measures and the introduction of antibiotics, plague was stopped in the middle of the twentieth century in several of the countries where it had been imported from Hong Kong or India, for instance, in Australia and in Europe. But plague did not disappear from the world.

Rat guards for ships. With the ordinance of July 9, 1912 in the United States, the use of rat guards for plague control became widespread on commercial vessels. A rat guard is a sort of round metal “shield,” placed over mooring lines to make it nearly impossible for rats to climb over and get onto or off the vessel when docked (Credit: Thomas Bredel). Black rats were very common on all commercial ships from far back in history (and up to 1940s). Black rats on ships were likely the main way the third pandemic spread from Hong Kong to India and later to the rest of the world. Possibly, black rats on vessels also were responsible for the rapid spread of plague during the second pandemic in the Mediterranean, along the coasts of Northern Europe as well as on rivers
1.3 Plague Is a Zoonosis: A Disease Transmitted Between Animals and Humans
Despite the measures introduced to combat it globally, plague has still persisted. In the United States, the WHO reported about 999 confirmed or probable human plague cases for the period between 1900 and 2010, mostly in the bubonic form. In recent decades, a range of 1–17 human cases per year has been reported in the United States, typically in the rural West (Fig. 1.1). The reason for the persistence of plague was disclosed in the first years of the twentieth century. Although plague quickly disappeared from the great harbors of California, three human cases were reported in the rural part of this state: some suspected that burrowing communities of wild rodents had picked up the plague bacillus by contact with infected rats and their fleas in the Californian ports. Two scientists, Wherry [17] and McCoy [18], provided evidence for this theory with the isolation of Y. pestis in California ground squirrels (Spermophilus beecheyi) from the same region. Today, the region west of the 100th meridian is regarded by the WHO as one of the largest world reservoirs of wild rodent plague. In these types of regions, also called plague foci, plague is enzootic, i.e., it persists in communities of partially resistant rodents (reservoir species) and in their fleas.
In wildlife, different modes of transmission impact the rate at which plague spreads in varying ways. For example, in the United States, ever since the first introduction of plague in 1894, transfer among animals has been estimated to occur at a rate of about 25 km (16 miles) per year [19]. This dissemination has been partially accelerated by human agency, but is mainly due to the life patterns of ground-burrowing wild rodents: as a rule, young rodents abandon their familial burrow and wander across country, sometimes over several miles to seek a new home [20]. As they move across an extensive range, they can join other communities and foster the dissemination of plague mediated by fleas transferred in the new burrows. Direct transmission is also not unusual, and it is believed that Y. pestis can be passed across mucous membranes and broken skin. The pneumonic form of plague may also be directly disseminated among animals in respiratory droplets (although this is not the case with rodents [21]). Additionally, Y. pestis can be orally transmitted via bites or by eating infected meals. Carnivores and omnivores may be infected by eating the tissue from contaminated animals and thereby contribute to maintaining plague in a region and occasionally transmit the pathology to humans. But since predators generally live isolated or in small communities, this mechanism cannot influence the modality and speed of dissemination of plague to a larger extent than the transmission among rodents does [22]. It has also been proposed that the dissemination of the plague bacterium can be due to its persistence in the soil of infected burrows (the so-called telluric hypothesis [23]), and a study seems to demonstrate that Y. pestis can remain viable and virulent after 40 weeks of incubation in sterilized humidified sand [24]. Survival in soil would be a model alternative to enzoonoticsFootnote 16 for explaining the perseverance of plague in a region during inter-epizootic periods, but the matter is still controversial. Independent of the source of contagion in wildlife, by 1940 about 34 species of rodents and even more species of fleas were discovered to be infected by Y. pestis in the United States alone [20].
Elsewhere in the world, animal reservoirs for plague were already observed in Mongolia as early as 1895 and were later also discovered in other parts of Asia, Africa, and South America. In present-day China, 86 species of vertebrate host (including 14 major rodent hosts) and 63 species of arthropod vector (including the major flea vector) have so far been identified [25, 26].
Different local hosts, vectors, and Y. pestis strains give rise to different natural plague foci, which can be classified into 12 types and 19 subtypes [27, 28]. In Europe and its surrounding regions, known plague foci only exist in Iran, Georgia, Russia, Armenia, Azerbaijan [29], and North AfricaFootnote 17, in territories placed on the desert belt or at the boundaries with deserts. In plague foci, epizootic periods may occasionally alternate with enzootic periods, inducing the death of a large number of plague hosts. Typically, three conditions are considered necessary for the development of an epizootic: more susceptible hosts, a large number of bacteria in the infected mammals (fatal high-level bacteremia), and a large number of infected fleas [30]. Several factors which regulate the interactions between the plague bacillus and its hosts and vectors can influence the alternation of enzootic/epizootic plague cycles [31]. However, the trophic cascade hypothesis, driven by a typical climatic pattern, seems to be the most appropriate model, especially in the plague sylvatic foci of the Asiatic desert belt [32–35]. A trophic cascade occurs when increased precipitation produces greater plant growth, which in turn results in an abundance of food production for epizootic rodents. This phenomenon leads to an increased animal population density and consequently to a greater number of fleas [34] and plague bacteria. If this period of plenty is followed by a severe drought, some individuals (the ones more susceptible or possibly debilitated by starvation) in the wild rodent populations develop septicemia and die of plague. The infected fleas on these individuals, after partaking of blood meals rich in Y. pestis bacteria, abandon the cold corpses of the victims and crowd onto the survivors, thereby contributing to the self-maintaining process of the epizootic. Depending on climatic conditions, the trophic cascade can simultaneously occur on a landscape scale in regions that have a similar biotope to one another yet are geographically separated (the Moran effect [36, 37]).
During an epizootic period, the chance of infective contact is higher, and transmission between animals and humans more readily occurs. In regions where plague is present in the sylvatic cycle, humans can acquire plague by direct contact with infected animals (by skinning or eating them or by accidental flea bites [10]). Once infected, the person in question can transport the disease back to his or her village or city. But plague can also be introduced into the urban cycle by wild rodents scavenging for food, as what happened in Los Angeles during the epidemic of 1924–1925, when both infected ground squirrels and rats were detected in the city [38]. With the exception of some communities of rats in Madagascar (which have become resistant to plague [39]), rats are generally very susceptible to the disease, which can lead to great die-offs such as the one observed by Yersin in Hong Kong, marking the onset of an epidemic among humans. Moreover, other commensal, peridomestic, and domestic animals are sensitive to plague and can directly – or indirectly with the mediation of their parasites – transmit the bacillus to humans. Domestic cats and dogs are known to carry plague, although dogs tend to have a higher resistance to the bacteria in comparison to cats and thus do not develop the high-level bacteremia, which is generally considered to be necessary for transmission.Footnote 18 In contrast, cats are quite susceptible and can transmit plague by ectoparasites or respiratory droplets. Camels, often used in caravans to transport humans and goods in Asia, the Near East, and North Africa along the desert belt, can become infected when their feed is contaminated by dead rodents or their excretions.Footnote 19 Camel-to-human contagion episodes have repeatedly been demonstrated, in particular related to the practice among nomads of eating dead animals regardless of the cause of death [40]. Finally, as early as the 1940s, observed outbreaks in rural settlements in Iran led researchers to suggest that plague epidemics can also be directly promoted by wild rodents without any mediation of commensal or peridomestic animals [41].
1.4 Plague Is a Vector-Borne Infectious Disease
Given the persistence of plague in enzootic animals in several continents and the recurrent epizootic episodes driven by climatic conditions, we should expect epidemics to strike with some regularity. Fortunately, since the 1920s, the majority of human plague cases reported by the WHO have been sporadic, and these cases have originated by humans coming into casual contact with wild rodents within enzootic foci [38]. Only in some places – recently primarily in Africa – has human plague infection more frequently developed into larger epidemics. Intriguingly, we still do not understand exactly how the mechanisms underlying the spread and maintenance of human contagion operate once plague has entered the urban cycle.
In the urban cycle, one source of interpersonal transmission is via the inhalation of infected respiratory droplets of pneumonic plague (aerosol transmission). However, epidemics of pneumonic plague are rare and only spread rapidly in localized and contained outbreaks (1–117 cases [42–44]). The largest known outbreaks of primary pneumonic plague occurred in Manchuria in 1910–1911, 1917–1918, and 1920–1921, with 60,000, 16,000, and 9000 deaths, respectively [45]. Contagion via inhalation seems to require particular conditions to effectively spread, such as crowded and poorly ventilated spaces and a cold climate.
In addition to aerosol transmission, casual contact with infected (animal or human) tissue represents a real risk of infection for humans. Contagion by direct contact could cause a contained spread to occur among relatives and close communities of people who take care of their dead [46], but it is unknown to what extent this mechanism can maintain an epidemic, since death practices and rituals are usually abandoned after a short period of time.
So if aerosol transmission and contagion by direct contact alone are unlikely to maintain plague epidemics in human populations, what can? The experience of the last pandemic has shown that the great pathogenicity of Y. pestis, unique within the Enterobacteriaceae family, can be explained by an adaptation to two different systems and different temperatures: on the one hand, the blood, lymphoid, and reticuloendothelial systems of mammalian hosts (body temperature, typically 37 °C) and, on the other hand, the digestive tract of various flea species at ambient temperature [47, 48]. In other words, both mammalian hosts and ectoparasites can be the promoters of any pestilence, which leads us back to the role fleas play in the spread of plague.
In nature, there are about 80 species of fleas that can be infected by Y. pestis [49], and in the 1950s, mathematical models were first used to calculate the vector efficiency of different flea species [50, 51]. The results indicated that X. cheopis was the most efficient vector for the transmission of plague, likely due to the underlying mechanism of infection. Taking a closer look at the mechanism, it is thought that fleas in general become infected with Y. pestis after taking blood meals from mammals with high-level bacteremia or septicemia. Y. pestis bacteria are generally eliminated by fleas via the digestion process, but in some flea species, such as X. cheopis, another mechanism can be activated. In this alternative mechanism, Y. pestis can survive and multiply in the stomach (midgut) of an infected flea and form agglomerates of bacterial cells that can attach to the proventriculus, a valve-like chamber between the midgut and esophagus [52]. After an 8–16-day incubation period [53], this agglomerate of Y. pestis bacteria, protected by a biofilm, can efficiently block the proventriculus and hence block the passage of blood meal in the gut. As the digestive tract is blocked, the flea repeatedly attempts to feed but can only regurgitate into the bitten host a number of bacteria that are dislodged from the biofilm [30, 54].
Although considered the most efficient method of transmission, this method does have its own limitations [30]. First, a high bacterial load is required to cause the digestive tract of fleas to become blocked. Second, even if this condition is satisfied, only 50 % of the individual infected fleas can be effectively blocked. Third, only 45 % of the flea bites of an individual blocked flea are effective in transmitting the bacterium. Fourth, a prerequisite for efficient flea-borne transmission is the maintenance of the vectorial capacity of the infected flea in question [55], but the proventricular blockage quickly leads to dehydration of the flea and subsequently death by starvation [49]. For this reason, the infective period of a blocked flea is only a few days. In addition, the median number of Y. pestis cells transmitted by blocked X. cheopis is less than 100 [21]. Intriguingly, this is an efficient enough number to transmit disease, since less than ten to twenty bacteria were demonstrated experimentally to produce plague in mammal hosts [30]. This observation therefore paves the way for other hypotheses regarding possible mechanisms of infection: poor vectors should not be discarded as insignificant in the dissemination of plague [47].
Indeed, alternative flea-borne mechanisms for mammalian infection have been demonstrated to be efficient enough in maintaining plague in host populations. The ground squirrel flea, Oropsylla montana, the primary vector for plague transmission to humans in North America, transmits Y. pestis by so-called “early-phase” transmission (EPT [53, 56]), which does not require the 8–16 days of extrinsic incubation period necessary to develop an efficient proventricular blockage [53]. The mechanism of this early-phase transmission is not fully understood: it could be due to mechanical transmission of few Y. pestis bacilli surviving on the bloodstained mouthparts of fleas between consecutive feedings or, more likely, be driven by regurgitation of the infectious remnants from a previous blood meal [53]. This model was proposed for fleas that do not develop proventricular blockage, such as the so-called human flea,Footnote 20 Pulex irritans. Recent findings on an outbreak in Madagascar support the role of P. irritans in causing outbreaks of plague in the absence of infected X. cheopis [57]. The EPT model seems to support the idea that plague is a self-sustained vector-borne infectious disease in humans, an alternative mode of transmission first proposed by Blanc and Baltazard [41, 58] and often reproposed in the literature [e.g., 49, 59–61]. Blanc and Baltazard [41] also showed that human body lice (Pediculus humanus) from plague victims had Y. pestis in the gut and could infect shaven guinea pigs. Therefore, when considering plague epidemic transmission in humans, body lice, which can be transmitted by the exchange of clothing and can infect humans through feeding and feces, could also be a good vector candidate [62, 63]. What plague research shows us is that the methods and scale of transmission are varied and complex for this vector-borne disease.
1.5 Discrepancies Between the Third Pandemic and the Two First Pandemics
When taking into account the evidence collected on plague since the end of the nineteenth century, doubt has been cast on the actual nature of the first two pandemics. Discrepancies observed in the historical records regarding the description of the symptoms can be attributed to the belief in the miasmatic theory (see a debate about this in [3]). But besides the symptoms, Cohn [7] recognized a series of additional discrepancies between the current third pandemic and the first and second ones. The most surprising anomaly regards the absence of rats: no historical report on the past pestilences mentions dead rats, although other animals are specifically mentioned as having died of plague (e.g., pigs in Boccaccio’s The Decameron). Paintings and other artistic representations as well don’t hint at the presence of urban rodents, although as described by Yersin [13] and other scholars, the phenomenon could hardly have been overseen. Further, black rats and X. cheopis were proposed to have been absent or very rare in some regions of Medieval Europe [61, 64], a hypothesis which has recently received support from archeological evidence [60]. Moreover, plague caused by black rats and blocked fleas like X. cheopis is efficient but slow, but we know that previous pestilences were fast movers [7]: sophisticated modeling methods have demonstrated that the Black Death spread by 1.5–6 km per day [65]. Yet another discrepancy is that the plague of the third pandemic has historically mostly been a plague of the harbors, whereas the two first ones penetrated rapidly beyond docklands. Finally, as observed by Cohn, outbreaks during the first and second pandemics could hit at any time of the year “before usually settling into a summer pattern for the southern Mediterranean and the Near East, that is during the hottest and driest points of the year, the least hospitable season for the most efficient flea vector of Y. pestis – X. cheopis” [7].
1.6 Y. pestis Was the Causative Agent of All Known Plague Pandemics
While Yersin [13] was strongly convinced that the bacterium he had isolated was also responsible for the first and second pandemics, his assertion was repeatedly challenged over the last decades due to the arguments cited above. The debate was recently settled by two molecular studies carried out on human skeletons from plague pits of the first [66] and the second pandemics [67]. The results were later independently confirmed by other studies [68, 69]. Following the theory that a septicemic event could have preceded the exitus and using the technique of ancient DNA analysis based on the retrieval of genetic material from the teeth, scientists were able to isolate Y. pestis DNA from putative victims buried in multiple or mass graves. By using the same genetic markers employed for the characterization of extant strains, they could also properly classify the ancient strains. In particular, the identification of single nucleotide polymorphisms (SNPs) allowed the reconstruction of phylogenetic trees [70–72] and the placement of the genealogical position of the ancient strains in relationship to the modern ones. This method unveiled essential information: first, it was confirmed that the strains of the first and second pandemics, strains that are now extinct, were ancestral to those responsible for the third pandemic (referred to as 1.ORI). This finding also confirmed the historical information of a recent introduction of Y. pestis 1.ORI strains in North America and Madagascar in newly established reservoirs. Second, related but different clones of Y. pestis were simultaneously circulating in Europe during the historical outbreaks [67, 69, 72]. Finally, it could be postulated that the origin of the bacteria responsible for the three pandemics was probably in Asia, although some scholars have proposed that the etiological agent of the third pandemic developed in Europe before it was introduced into China [69].
1.7 The Ecological and Climatic Dynamics of Plague
Since humans are an endpoint for the bacterium, it is not surprising that the historical strains of Y. pestis are now extinct. Instead, the genetic variability observed in extant strains [71, 72] mostly represents the evolution that occurred in wildlife reservoirs under the effect of different population dynamics over time, such as population expansions and contractions, isolation by distance phenomena, and episodes of bottlenecks or founder effects. As plague is primarily a zoonosis, its dynamics cannot be understood unless we understand the dynamics of the disease in its wildlife reservoir [10, 73].
Ecological studies of the plague system have shown that in order for the disease to spill over to humans, the abundance of the host wild rodent population needs to be above a certain threshold for a few years [74] and simultaneously spread out over a large geographic area [35]. The dynamic link between wildlife plague reservoirs and human populations has been studied by Samia et al. [32]. Their study demonstrated that, in addition to the wildlife threshold, another threshold exists: the plague bacterium spills over into the human population particularly when the ratio between fleas (the vector) and rodents (the host) is itself above a certain threshold. Biologically, this implies that the flea population on each individual rodent host becomes highly crowded, likely leading to higher flea mobility. Yet external drivers such as climate also play a role in the outbreak and dissemination of plague.
One of the most important external drivers in the outbreak of plague is climate, which affects both the location of plague foci and the intensity of the epidemic. For Central Asia it has been demonstrated that an increase of 1 °C will lead to a doubling of the prevalence of plague in its host [33] (see also [75, 76]). It has also been shown that climate variation primarily affects the behavior of the fleas (the vector) and their population dynamics [32]. In northern and southern China, the locations of natural plague foci are separately distributed, and the effects of climate factors on plague dynamics may show spatial heterogeneity between these two different regions. As regards the effect climate has on the intensity of an outbreak, Xu et al. [76] investigated the association of human plague intensity with proxy data on climate condition, using spatial and temporal human plague records in China from 1850 to 1964. The results demonstrated that the nonlinear responses of plague intensity to dry/wet conditions were different in northern and southern China [76]. Subsequently, by using a two-dimensional wavelet analysis, clustering groups were more precisely identified in the same database, and at least four well-defined independent foci were identified. In addition, environmental differences between plague territories – including but not limited to climate factors – were defined using ecological niche modeling [77]. A previous study has shown that the spatial temporal dynamics of plague are associated with a time-lagged global climate index [78]. The study employed cross-wavelet analysis to reveal that increasing rates of human plague oscillate in phase with the southern oscillation indexFootnote 21 (SOI), but in antiphase with the sea surface temperature (SST) over periods of 2–4 years and approximately 8 years (6–10 years), respectively. This suggests that El Niño and the Southern Oscillation (ENSO)-driven climate variation might be an important factor for the outbreak of human plague in China [78].
Climate factors not only influence the outbreak of plague but also drive its spatial spread. The pattern of plague dissemination in China has been studied using two methods: nearest neighbor approach, a novel method which deals with both short- and long-distance transmissions, and trend surface analysis. These two methods were also used to investigate the spread of plague in Europe and the western United States [75]. The results indicated that the spread of plague has been slower on mainland China than it was in Europe during the Black Death and has been in the western United States since the 1900s. Factors such as floods and the presence of major roads, rivers, and coastlines accelerated the spread of plague and shaped transmission patterns [75, 79]. Additionally, the spread of climate-driven plague has been found to occur on a large spatial scale, on an intercontinental or global one. Research by Schmid et al. [79], synthesizing the ecologically dynamic effects of climate variation, indicates that plague in Europe has probably been repeatedly introduced from Central Asia in response to climatic effects occurring in Central Asia – not ones locally in Western Europe.
As already discussed, climate may impact plague due to its ability to initiate a trophic cascade, as climate affects the plant-rodent-flea-pathogen system in natural plague foci. For instance, surveillance data of two types of natural plague foci in Inner Mongolia has shown that plague epizootics in the Mongolian gerbil (Meriones unguiculatus) were driven by the effect of climate variation on the growth of local vegetation and consequently the density of the host population [80]. Furthermore, this phenomenon shows similarities with what has been observed in great gerbil (Rhombomys opimus) plague foci in pre-Balkhash, Kazakhstan: the prevalence of plague in rodents increases with warmer springs and wetter summers [33].
1.8 The Historical Plagues Could Have Been Self-Sustained Vector-Borne Pandemics
It has long been assumed that previous pandemics were initiated by the arrival of black rats originating from Asian enzootic regions, allowing the establishment of new plague reservoirs in European wildlife. In particular, the Black Death period is often considered to have started as an isolated episode of plague introduced into the local fauna which then, with enzootic-epizootic cycles, led to the reinfection of human populations over the course of four centuries. Nevertheless, the locations of the foci responsible for the plague pandemics, as well as the nature of the mammalian reservoirs responsible for them, have never been established. To this day, there is speculation around these questions, as well as to what caused the disappearance of those putative foci from Western Europe. Plague has affected Europe and Constantinople until the nineteenth century, yet later plague episodes at the time of the third pandemic have been clearly attributed to introductions from outside, either directly from China or indirectly from Asia and Africa, and not to reactivation of local reservoirs. At present, there is no plague focus in Western Europe [81].
Both the topography and climate of Western Europe consistently differ from those of all other plague foci of the world, which makes it difficult to explain the presence of a local reservoir in the past. Perhaps because of this reason, it was often proposed that no wild rodents but the commensal or peridomestic rats themselves developed a reservoir for plague in Europe by acquiring immunity to the disease, as has been seen in present-day Malagasy populations of black rats and brown rats (Rattus norvegicus) [28]. The disappearance of the black rat from most European countries could explain the absence of current rat reservoirs, but we currently find high numbers of the brown rat in present-day Europe. Yet the brown rat was only introduced to European countries in the late eighteenth century, and there is no evidence that it was present in Western Europe during previous plague outbreaks, so its role remains uncertain. Additionally, while immunity could explain the absence of a mass die-off of rats in the historical records, it does not explain the lack of annual recurrence of outbreaks in Europe which are otherwise typical of endemic regions. For instance, in Madagascar, plague has resurfaced nearly every yearFootnote 22 since 1980 in the same localities, despite plague surveillance and the use of insecticides and antibiotics. Even in the Malagasy port city of Mahajanga, where there were no environmental conditions for the establishment of a permanent reservoir, outbreaks of plague that were not preceded by an epizootic of rats were recorded annually for a decade between 1991 and 1999 [81]. In contrast, in Medieval Europe, the recurrence of plague in the same localities typically showed epidemiological cycles of up to 3 years of outbreak followed by 11 years of disappearance [12].
Assuming that in Europe there once were well-established plague foci, Wagner et al. [69] proposed that Y. pestis strains from European foci reinfected wild rodents in China. The conclusion reached is one possible interpretation of the Y. pestis extant phylogeny, but there is another possible explanation [71, 72], which suggests that plague did not establish itself in permanent reservoirs in Europe, but rather was imported again and again from Asian reservoirs. This interpretation of the phylogeny of Y. pestis strains is now supported by new climatological data [79], refining the hypothesis of recurrent reintroductions to Europe from the outside by developing a new consistent model: on several occasions, geographically widespread climatic patterns in Asia were observed to precede the reintroduction of plague in Europe by about 15 years [79], namely, a pluvial period followed by a drought. This climatic pattern, which could have started the trophic cascade described in Sect. 1.3, has also been observed at the time of the Black Death, confirming that this model is credible. Fifteen years is not a long time for spillover from a reservoir to occur and for plague to spread over large distances in the Middle Ages. Yet, once the necessary time had elapsed for epizootics to develop, plague could have been picked up on the trading routes of the Silk Road by caravans and their camels and traveled with humans from one caravanserai to the next or from city to city. At the start of the Black Death, a similar process occurred, as plague spread from city to city, moving by human agency from Astrakhan near the Caspian Sea to the Crimea, Constantinople, Messina, and the Mediterranean harbors of Europe over a period of 4 years – a considerable amount of time [82]. In Asian human settlements, plague could have started new epidemics before being transported to Europe by other caravans or by maritime vessels, epidemics of which we have no historical record.
The proposed model of recurrent introductions of plague into Europe doesn’t completely exclude the role of rats (perhaps often reintroduced into European harbors by maritime vessels [64]). Rather, it dismisses the notion that black rats and their fleas (X. cheopis) are necessary to explain the recurrence of pestilences in Europe. Moving away from previous assumptions about plague reservoirs in Europe, the resulting model proposes a different scenario for the historic pandemics: plague as a self-supporting system of infection, recirculating for a while in human European populations after its importation from enzootic places in Central Asia. Following maritime and fluvial routes or mainland roads, bubonic plague might have spread with humans, at their speed, possibly by means of hematophagous parasites. Since humans move in different directions, it is even theoretically possible under this model that strains of Y. pestis were reintroduced by humans in the Chinese reservoirs, as proposed by Wagner et al. [69].
Indeed, multiple historical records strongly suggest that traveled routes were responsible for the spread of plague. These records directly attribute the entrance of plague into a healthy settlement to soldiers, pilgrims, seamen, merchants, or travelers coming from regions with plague (the so-called Case 1). From the symptoms described in the reports of contemporaneous chroniclers, pneumonic plague is also often recognizable, which could have been responsible for some outbreaks or single cases of human-to-human transmission. The time between first symptoms and death is 2 days, which is rather short, but the time between being infected and dying is 2 days plus 3–4 days. Therefore, the possibility that infected people could carry and spread pneumonic plague over long distances seems plausible [42]. A single traveler infected by bubonic plague could have covered at least 40 km (25 miles) by land and an even greater distance by sea, before developing symptoms or dying. Additionally, the arrival via commercial routes of plague-infested belongings and clothing of people who had died of the disease has also often been linked to the further spread of plague. An example of this can be seen in the case of the tailor George Viccars, who first contracted bubonic plague in Eyam (in 1665) after having imported from London clothing from people claimed by the plague [83].
It has been suggested by Cohn [7] that the seasonality of plague in Europe was not consistent with the temperatures usually required to activate the mechanism of transmission mediated by X. cheopis. However, as previously mentioned, there are at least 80 known species of fleas that can transport plague besides X. cheopis. The early-phase transmission mechanism [53, 56], proposed specifically for these other flea species, could potentially explain the rapid spread of human plague across the European continent during the second pandemic. Additionally, there are several other potential vectors yet to be discovered, and the absence of seasonality in northern Europe suggests that other parasites, e.g., human body lice, could have been vectors for this region, while the inverse seasonality [75] observed in temperate regions (compared to desert belt ones) suggests that fleas were the likely vectors in southern Europe.
The model of frequent reintroductions, which negates the need for the presence of a local plague reservoir, can also easily explain the differences observed between the second and the third pandemic: no droughts were consistently connected with past outbreaks in Europe [7, 79] since drought wasn’t necessary to introduce wild rodents into the urban cycle – simply put there was no local plague reservoir of wild rodents in Europe to start with. Finally, the model of (vector-borne) human-to-human transmission explains why plague is largely absent from the European continent today (with the exception of the regions already mentioned) – the absence of local rodent reservoirs diminishes the possibility of accidental contact, and the potential for the importation of plague from outside of Europe is severely limited by present-day regulations, improved communications, and improved environmental and personal hygienic conditions.
We have come a long way since the days when people believed that plague was caused by poisonous air. Yet, despite the large number of studies and the data that exists on Y. pestis and plague, not everything is decoded. Even more work is required to clarify what happened in the past pandemics, particularly during the first one where little historical information is available. In the case of the second pandemic, two recent aDNA studies [84, 85] have proposed that the phylogeny of Y. pestis strains from the eighteenth century demonstrates a continuity of plague in local Western European reservoirs from the time of the Black Death. However, in the discussion, the authors had to admit that this genetic continuity could not unambiguously be interpreted as proof for ancient reservoirs within Europe. This is especially questionable when considering the plague of 1720–1722 in Marseille [85], a city which was an active harbor and a place of recurrent epidemics. From historical recordsFootnote 23 it is known that plague was imported in 1720 from outside of Marseille, from regions closer to and economically connected with Asia [86]. In any case, regardless of which pandemic is under discussion, further genetic studies are required to refine the phylogenetic information on ancient strains, in order to support or refute certain theories, and other studies (e.g., ecological, climatological at different scales, historical, epidemiological, microbiological) are essential to correctly interpret the genetic information available.Footnote 24
Notes
- 1.
Among the monuments recalling plague, we can mention Castel Sant’Angelo in Rome, which was originally the mausoleum of Hadrian and was converted into a castle at the beginning of the fourteenth century. Legend holds that the Archangel Michael appeared atop the mausoleum in 590 CE, sheathing his sword as a sign of the end of the plague in Rome. Other monuments of note include five plague churches in Venice, erected between the fifteenth and seventeenth centuries as vows for deliverance from some of the 70 epidemics of plague recorded in this port to the Levant. Of particular relevance is the School and Church of San Rocco (1485–1550), decorated with paintings by Tintoretto of Saint Roch’s life. St. Roch, the Christian saint especially invoked against the plague, set out from Montpellier as a mendicant pilgrim for Rome during a poorly defined epidemic of plague in the second half of the fourteenth century. He could heal sick people in the public hospitals by prayer, the sign of the cross, and the touch of his hand. To St. Roch is devoted also the Rochuscapelle in Bingen on the Rhine, a chapel erected by the city in 1677 in thanksgiving for surviving the plague of the year before. The festival of St. Roch, which is still held there every year, was notably celebrated by Goethe (Sankt-Rochus-Fest zu Bingen, Hamburger Ausgabe, Band 10, Am 16. August 1814). Other monuments of importance include the Pestsäule of Vienna, erected by Emperor Leopold I in 1687 to celebrate the end of the epidemic, and again in Vienna, a city repeatedly ravaged by the plague, one can see the Karlskirche, built after the plague of 1713 and dedicated to the plague saint, St. Carlo Borromeo. In Florence the loggia Orsanmichele (originally housing a grain market) was transformed into a church to protect the picture of the Virgin who was claimed to have saved the city from the Black Death of 1348. Also in Florence, as a consequence of the plague which badly hit the city during the second half of the fourteenth century, the cultural period of the Rinascimento (Renaissance, from the Italian for “rebirth”) took root and spread, eventually characterizing European history of the fifteenth–seventeenth centuries.
- 2.
Some examples are “to avoid or hate someone or something like the plague” (Italian idiomatic expression); “to stink like the plague” and “the choice between plague and cholera” (German idiomatic expressions); “A Sunday’s child never dies of the plague” and “He who trusts a woman and leads an ass will never be free from plague” (French proverbs); “Nothing is ever well done in a hurry, except flying from the plague or from quarrels, and catching fleas” (Italian proverb); “Plague seize the hindmost” (Latin proverb); “Lies are the plague of speech” and “Forgetfulness is the plague of knowledge” (Arabic proverbs); “A stupid friend is a greater plague than a wise enemy” (Turkish proverb); “An honest wife is a treasure that lasts, a sad wife is worse than the plague” and “A new doctor is a plague on the country” (Sicilian proverbs); “It is better to murder during time of plague” (English proverb); and “If God should listen to rooks, he should send a plague to horses” (Bulgarian proverb).
- 3.
Farina, Jean-Marie (1825). Précis sur les propriétés médicales de l’Eau de Cologne. Warin-Thierry.
- 4.
di Coppo Stefani, Marchionne (1903). Cronica Fiorentina. Citta di Costella: Lapi. 88 pp.
- 5.
In this text, Europe is defined as a geographical entity: the northwestern peninsula of the larger landmass known as Eurasia, separated from Asia by the Ural Mountains, the Ural River, and the crest of the Caucasus Mountains.
- 6.
The distinction between the second and third pandemic is relevant for the western European countries where the last epidemics of the second pandemic occurred in the eighteenth century; these include the Baltic pandemic of 1709–1713, the devastating plague of Messina in 1743, and the plague of Moscow in 1770–1771. Smaller outbreaks were recorded at, e.g., Noja and Malta, ca. 1815. In Eastern Europe there were repeated epidemics throughout the eighteenth and nineteenth centuries.
- 7.
Several countries in Europe have reported outbreaks of plague (see also Fig. 1.1), the first being Portugal in 1899 with the epidemic of Oporto, which likely arrived from Alexandria (Echenberg, Myron (2007). Plague ports: the global urban impact of bubonic plague, 1894–1901. New York: New York University Press. 366 pp.). Generally, the outbreaks in Europe were rapidly brought under control, with a low number of confirmed cases and deaths.
- 8.
World Health Organization. WHO Report on global surveillance of epidemic-prone infectious diseases – plague [cited 2013 Apr 15]. http://www.who.int/csr/resources/publications/plague/CSR_ISR_2000_1/en/index5.html
According to another interpretation, the third pandemic, caused by Y. pestis biovar Orientalis, ended at the middle of the last century when the WHO received notification of less than 2000–3000 human cases (during the period 1954–1997). By this interpretation, we are currently in a period of endemic plague caused by representatives of different biovars, including Orientalis (for indication about the phylogeny of current strains, see [70–72]).
- 9.
- 10.
- 11.
Erasmus in 1526 observed: “Twenty-five years ago, nothing was more fashionable in Brabant than public baths; today there are none, the new plague has taught us to avoid them.” Cited by Ashenburg, K. (2007). The dirt on clean: an unsanitized history. New York: North Point Press.
- 12.
Records of autopsies can be found even earlier, see Cohn, Samuel K., Jr. (2010). Cultures of plague: medical thinking at the end of the Renaissance. Oxford: Oxford University Press. 342 pp.
- 13.
Contemporaneous descriptions might have been based on the miasma framework, but seem to have been very aware that plague was contagious through human interactions. This is according to records collected in Horrox, Rosemary (1994). The Black Death. Manchester: Manchester University Press. 364 pp.
- 14.
New observations support the theory that it is not the bacteria engulfed by local macrophages that cause infection. Rather, it is the few bacteria that are freely transported to the lymph nodes within minutes after a victim is bitten which are responsible. Gonzalez R.J., Lane M.C., Wagner N.J., Weening E.H., Miller V.L. (2015). Dissemination of a highly virulent pathogen: tracking the early events that define infection. PLoS Pathogens, 11(1):e1004587.
- 15.
Yersin also observed that the disease was equally carried by many other mammals, including water buffaloes.
- 16.
The terms “enzootic” and “epizootic” are equivalent to nonhuman endemic and epidemic conditions, respectively.
- 17.
- 18.
A case of dog-to-human transmission of pneumonic plague was recently reported (Runfola J.K., House J., Miller L., et al. (2015). Outbreak of human pneumonic plague with dog-to-human and possible human-to-human transmission – Colorado, June–July 2014. Morbidity and Mortality Weekly Report, 64:429–434).
- 19.
Records from the former USSR detail 38 plague outbreaks among camels within the period 1907–1967. http://cns.miis.edu/opapers/pdfs/130904_soviet_antiplague_pdf
- 20.
P. irritans is a cosmopolitan insect with a wide host spectrum, even though its common name suggests a primary affiliation with humans.
- 21.
The SOI is a standardized index calculated on sea level pressure differences between Tahiti and Australia and gives information about large-scale fluctuations in air pressure across the tropical Pacific. Abnormalities of the SST in the same part of the ocean can drive El Niño (and La Niña) episodes. El Niño (La Niña) and the Southern Oscillation (ENSO) affects weather conditions in many parts of the world by sufficient modifications of the atmosphere.
- 22.
- 23.
- 24.
This is the goal of an ERC Advanced Grant (MedPlag – The medieval plagues: ecology, transmission modalities and routes of the infections. Project No.324249), of which the authors are either members or partners (Barbara Bramanti is the PI). We would like to acknowledge the ERC for support and Samuel K. Cohn Jr., Andrey Anisimov, and Boris V. Schmid for relevant comments and suggestions. The authors are indebted to Sari C. Cunningham for her valuable improvement of the manuscript.
References
Avery H. Plague churches, monuments and memorials. Proc R Soc Med. 1966;59(2):110–6.
Hatcher J. The Black Death: an intimate history. London: Weidenfeld & Nicolson; 2010.
Walløe L. Medieval and modern bubonic plague: some clinical continuities. Med Hist Suppl. 2008;52(27):59–73.
Rosen W. Justinian’s flea: plague, empire, and the birth of Europe. London: Penguin; 2007.
Little LK, Rome AAI. Plague and the end of antiquity: the pandemic of 541–750. Cambridge: Cambridge University Press in association with The American Academy in Rome; 2007.
Galvani AP, Slatkin M. Evaluating plague and smallpox as historical selective pressures for the CCR5-Δ32 HIV-resistance allele. Proc Natl Acad Sci. 2003;100(25):15276–9.
Cohn Jr SK. Epidemiology of the Black Death and successive waves of plague. Med Hist Suppl. 2008;52(27):74–100.
Liu Y. The atlas of plague and its environment in the People’s Republic of China. Beijing: Science Press; 2000.
Lien-Teh W, Chun J, Pollitzer R, Wu C. Plague: a manual for medical and public health workers. Am J Public Health Nations Health. 1936;26(10):1049–50.
Stenseth NC, Atshabar BB, Begon M, Belmain SR, Bertherat E, Carniel E, Gage KL, Leirs H, Rahalison L. Plague: past, present, and future. PLoS Med. 2008;5(1):e3.
Cipolla CM. Cristofano e la peste: un caso di storia del sistema sanitario in Toscana nell’età di Galileo, vol. 166. Bologna: Il mulino; 1976.
Vasold M. Die Pest. Ende eines Mythos. Theiss Verlag, Stuttgart; 2003.
Yersin A. La peste bubonique à Hong Kong. Archives de médecine navale et coloniale. 1894;62:256–61.
Shannon JG, Bosio CF, Hinnebusch BJ. Dermal neutrophil, macrophage and dendritic cell responses to Yersinia pestis transmitted by fleas. PLoS Pathog. 2015;11(3):e1004734.
Barnett SA. Rat control in a plague outbreak in Malta. J Hyg. 1948;46(1):10–8.
Mafart B, Brisou P, Bertherat E. Epidémiologie et prise en charge des épidémies de peste en Méditerranée au cours de la seconde guerre mondiale. Bulletin de la Société de Pathologie Exotique (1990). 2004;97(4):306–10.
Wherry WB. Plague among the ground squirrels of California. J Infect Dis. 1908;5(5):485–506.
McCoy GW. Plague among ground squirrels in America. J Hyg. 1910;10(4):589–601.
Benedictow OJ. Yersinia pestis, the bacterium of plague, arose in East Asia. Did it spread westwards via the Silk Roads, the Chinese maritime expeditions of Zheng He or over the vast Eurasian populations of sylvatic (wild) rodents? J Asian Hist. 2013;47(1):1–31.
McNeill WH. Plagues and peoples, A peregrine book, vol. 2. Harmondsworth: Penguin; 1979. p. 99.
Lorange EA, Race BL, Sebbane F, Hinnebusch BJ. Poor vector competence of fleas and the evolution of hypervirulence in Yersinia pestis. J Infect Dis. 2005;191(11):1907–12.
Salkeld DJ, Stapp P. Seroprevalence rates and transmission of plague (Yersinia pestis) in mammalian carnivores. Vector Borne Zoonotic Dis. 2006;6(3):231–9.
Mollaret HH. Remarques sur la communication de MM. Brygoo et Dodin à propos de la peste tellurique et de la peste de fouissement, Données malgaches. Bull Soc Pathol Exot Filiales (Paris). 1965;58(2):140–54.
Ayyadurai S, Houhamdi L, Lepidi H, Nappez C, Raoult D, Drancourt M. Long-term persistence of virulent Yersinia pestis in soil. Microbiology. 2008;154(Pt 9):2865–71.
Gong Z, Yu X, Liu Q, Ye R, Lu L, Xu l, Zhang J, Li C, Bai X, Fang X. Ecological-geographic landscapes of natural plague foci in China VI. Biological characteristics of natural vectors of Yersinia pestis. Chin J Epidemiol. 2012;33(008):818–22.
Qin C, Xu L, Zhang R, Liu Q, Li G, Fang X. Ecological-geographic landscapes of natural plague foci in China V. Biological characteristics of major natural reservoirs of Yersinia pestis. Chin J Epidemiol. 2012;33(7):692–7.
Fang X, Xu L, Liu Q, Zhang R. Ecological-geographic landscapes of natural plague foci in China I. Eco-geographic landscapes of natural plague foci. Chin J Epidemiol. 2011;32(12):1232–6.
Chanteau S, Ratsifasoamanana L, Rasoamanana B, Rahalison L, Randriambelosoa J, Roux J, Rabeson D. Plague, a reemerging disease in Madagascar. Emerg Infect Dis. 1998;4(1):101–4.
Anisimov AP, Lindler LE, Pier GB. Intraspecific diversity of Yersinia pestis. Clin Microbiol Rev. 2004;17(2):434–64.
Hinnebusch BJ. The evolution of flea-borne transmission in Yersinia pestis. Curr Issues Mol Biol. 2005;7(2):197–212.
Gage KL, Kosoy MY. Natural history of plague: perspectives from more than a century of research. Annu Rev Entomol. 2005;50(50):505–28.
Samia NI, Kausrud KL, Heesterbeek H, Ageyev V, Begon M, Chan KS, Stenseth NC. Dynamics of the plague-wildlife-human system in Central Asia are controlled by two epidemiological thresholds. Proc Natl Acad Sci. 2011;108(35):14527–32.
Stenseth NC, Samia NI, Viljugrein H, Kausrud KL, Begon M, Davis S, Leirs H, Dubyanskiy VM, Esper J, Ageyev VS, et al. Plague dynamics are driven by climate variation. Proc Natl Acad Sci U S A. 2006;103(35):13110–5.
Reijniers J, Davis S, Begon M, Heesterbeek JA, Ageyev VS, Leirs H. A curve of thresholds governs plague epizootics in Central Asia. Ecol Lett. 2012;15(6):554–60.
Kausrud KL, Viljugrein H, Frigessi A, Begon M, Davis S, Leirs H, Dubyanskiy V, Stenseth NC. Climatically driven synchrony of gerbil populations allows large-scale plague outbreaks. Proc R Soc B Biol Sci. 2007;274(1621):1963–9.
Hudson PJ, Cattadori IM. The Moran effect: a cause of population synchrony. Trends Ecol Evol. 1999;14(1):1–2.
Koenig WD. Global patterns of environmental synchrony and the Moran effect. Ecography. 2002;25(25):283–8.
Caten JL, Kartman L. Human plague in the United States, 1900–1966. J Am Med Assoc. 1968;205(6):333–6.
Tollenaere C, Rahalison L, Ranjalahy M, Duplantier JM, Rahelinirina S, Telfer S, Brouat C. Susceptibility to Yersinia pestis experimental infection in wild Rattus rattus, reservoir of plague in Madagascar. Ecohealth. 2010;7(2):242–7.
Mustafa I. Bacterial diseases of dromedaries and bactrian camels. Rev Sci Tech Int Off Epizoot. 1987;6:391–405.
Blanc G, Baltazard M. Rôle des ectoparasites humains dans la transmission de la peste. Bull Acad Natl Med. 1942;126:446–8.
Gani R, Leach S. Epidemiologic determinants for modeling pneumonic plague outbreaks. Emerg Infect Dis. 2004;10(4):608–14.
Butler T. Plague gives surprises in the first decade of the 21st century in the United States and worldwide. Am J Trop Med Hyg. 2013;89(4):788–93.
Richard V, Riehm JM, Herindrainy P, Soanandrasana R, Ratsitoharina M, Rakotomanana F, Andrianalimanana S, Scholz HC, Rajerison M. Pneumonic plague outbreak, northern Madagascar, 2011. Emerg Infect Dis. 2015;21(1):8–15.
Teh WL. The second pneumonic plague epidemic in Manchuria, 1920–21: I. A general survey of the outbreak and its course. J of Hyg (Lond). 1923;21(3):262–88.
Persson B. Pestens gåta: Farsoter i det tidiga 1700-talets Skåne, vol. 5. Lund: Lund University; 2001.
Perry RD, Fetherston JD. Yersinia pestis – etiologic agent of plague. Clin Microbiol Rev. 1997;10(1):35–66.
Prentice MB, Rahalison L. Plague. Lancet. 2007;369(9568):1196–207.
Pollitzer R. Plague. Geneva: World Health Organization; 1954.
Pollitzer R. Plague studies. IX. Epidemiology. Bull World Health Organ. 1953;9(1):131–70.
Burroughs AL. Sylvatic plague studies: the vector efficiency of nine species of fleas compared with Xenopsylla cheopis. J Hyg (Lond). 1947;45(3):371–96.
Bacot AW, Martin CJ. LXVII. Observations on the mechanism of the transmission of plague by fleas. J Hyg (Lond). 1914;13(Suppl):423–39.
Eisen RJ, Dennis DT, Gage KL. The role of early-phase transmission in the spread of Yersinia pestis. J Med Entomol. 2015;52(6):1183–92.
Jarrett CO, Deak E, Isherwood KE, Oyston PC, Fischer ER, Whitney AR, Kobayashi SD, DeLeo FR, Hinnebusch BJ. Transmission of Yersinia pestis from an infectious biofilm in the flea vector. J Infect Dis. 2004;190(4):783–92.
Carniel E. Subtle genetic modifications transformed an enteropathogen into a flea-borne pathogen. Proc Natl Acad Sci U S A. 2014;111(52):18409–10.
Eisen RJ, Bearden SW, Wilder AP, Montenieri JA, Antolin MF, Gage KL. Early-phase transmission of Yersinia pestis by unblocked fleas as a mechanism explaining rapidly spreading plague epizootics. Proc Natl Acad Sci U S A. 2006;103(42):15380–5.
Ratovonjato J, Rajerison M, Rahelinirina S, Boyer S. Yersinia pestis in Pulex irritans fleas during plague outbreak, Madagascar. Emerg Infect Dis. 2014;20(8):1414–5.
Baltazard M, Bahmanyar M, Mostachfi P, Eftekhari M, Mofidi C. Recherches sur la peste en Inde. Bull World Health Organ. 1960;23(2–3):169–215.
Laudisoit A, Leirs H, Makundi RH, Van Dongen S, Davis S, Neerinckx S, Deckers J, Libois R. Plague and the human flea, Tanzania. Emerg Infect Dis. 2007;13(5):687–93.
Hufthammer AK, Walløe L. Rats cannot have been intermediate hosts for Yersinia pestis during medieval plague epidemics in northern Europe. J Archaeol Sci. 2013;40(4):1752–9.
Drancourt M, Houhamdi L, Raoult D. Yersinia pestis as a telluric, human ectoparasite-borne organism. Lancet Infect Dis. 2006;6(4):234–41.
Houhamdi L, Raoult D. Different genes govern Yersinia pestis pathogenicity in Caenorhabditis elegans and human lice. Microb Pathog. 2008;44(5):435–7.
Houhamdi L, Lepidi H, Drancourt M, Raoult D. Experimental model to evaluate the human body louse as a vector of plague. J Infect Dis. 2006;194(11):1589–96.
Davis DE. The scarcity of rats and the Black Death: an ecological history. J Interdiscip Hist. 1986;16(3):455–70.
Christakos G, Olea RA, Yu HL. Recent results on the spatiotemporal modelling and comparative analysis of Black Death and bubonic plague epidemics. Public Health. 2007;121(9):700–20.
Harbeck M, Seifert L, Hänsch S, Wagner DM, Birdsell D, Parise KL, Wiechmann I, Grupe G, Thomas A, Keim P, Zöller L, Bramanti B, Riehm JM, Scholz HC. Yersinia pestis DNA from skeletal remains from the 6th century AD reveals insights into Justinianic Plague. PLoS Pathog. 2013;9(5):e1003349.
Haensch S, Bianucci R, Signoli M, Rajerison M, Schultz M, Kacki S, Vermunt M, Weston DA, Hurst D, Achtman M, Carniel E, Bramanti B. Distinct clones of Yersinia pestis caused the Black Death. PLoS Pathog. 2010;6(10):e1001134.
Bos KI, Schuenemann VJ, Golding GB, Burbano HA, Waglechner N, Coombes BK, McPhee JB, DeWitte SN, Meyer M, Schmedes S, Wood J, Earn DJ, Herring DA, Bauer P, Poinar HN, Krause J. A draft genome of Yersinia pestis from victims of the Black Death. Nature. 2011;478(7370):506–10.
Wagner DM, Klunk J, Harbeck M, Devault A, Waglechner N, Sahl JW, Enk J, Birdsell DN, Kuch M, Lumibao C, Poinar D, Pearson T, Fourment M, Golding B, Riehm JM, Earn DJ, Dewitte S, Rouillard JM, Grupe G, Wiechmann I, Bliska JB, Keim PS, Scholz HC, Holmes EC, Poinar H. Yersinia pestis and the plague of Justinian 541–543 AD: a genomic analysis. Lancet Infect Dis. 2014;14(4):319–26.
Achtman M, Morelli G, Zhu P, Wirth T, Diehl I, Kusecek B, Vogler AJ, Wagner DM, Allender CJ, Easterday WR, Chenal-Francisque V, Worsham P, Thomson NR, Parkhill J, Lindler LE, Carniel E, Keim P. Microevolution and history of the plague bacillus, Yersinia pestis. Proc Natl Acad Sci U S A. 2004;101(51):17837–42.
Morelli G, Song Y, Mazzoni CJ, Eppinger M, Roumagnac P, Wagner DM, Feldkamp M, Kusecek B, Vogler AJ, Li Y, Cui Y, Thomson NR, Jombart T, Leblois R, Lichtner P, Rahalison L, Petersen JM, Balloux F, Keim P, Wirth T, Ravel J, Yang R, Carniel E, Achtman M. Yersinia pestis genome sequencing identifies patterns of global phylogenetic diversity. Nat Genet. 2010;42(12):1140–3.
Cui Y, Yu C, Yan Y, Li D, Li Y, Jombart T, Weinert LA, Wang Z, Guo Z, Xu L, Zhang Y, Zheng H, Qin N, Xiao X, Wu M, Wang X, Zhou D, Qi Z, Du Z, Wu H, Yang X, Cao H, Wang H, Wang J, Yao S, Rakin A, Li Y, Falush D, Balloux F, Achtman M, Song Y, Wang J, Yang R. Historical variations in mutation rate in an epidemic pathogen, Yersinia pestis. Proc Natl Acad Sci U S A. 2013;110(2):577–82.
Ben-Ari T, Neerinckx S, Gage KL, Kreppel K, Laudisoit A, Leirs H, Stenseth NC. Plague and climate: scales matter. PLoS Pathog. 2011;7(9):e1002160.
Davis S, Trapman P, Leirs H, Begon M, Heesterbeek JAP. The abundance threshold for plague as a critical percolation phenomenon. Nature. 2008;454(7204):634–7.
Xu L, Stige LC, Kausrud KL, Ben AT, Wang S, Fang X, Schmid BV, Liu Q, Stenseth NC, Zhang Z. Wet climate and transportation routes accelerate spread of human plague. Proc R Soc B Biol Sci. 2014;281(1780):20133159.
Xu L, Liu Q, Stige LC, Ben Ari T, Fang X, Chan KS, Wang S, Stenseth NC, Zhang Z. Nonlinear effect of climate on plague during the third pandemic in China. Proc Natl Acad Sci U S A. 2011;108(25):10214–9.
Ben-Ari T, Neerinckx S, Agier L, Cazelles B, Xu L, Zhang Z, Fang X, Wang S, Liu Q, Stenseth NC. Identification of Chinese plague foci from long-term epidemiological data. Proc Natl Acad Sci U S A. 2012;109(21):8196–201.
Zhang Z, Li Z, Tao Y, Chen M, Wen X, Xu L, Tian H, Stenseth NC. Relationship between increase rate of human plague in China and global climate index as revealed by cross-spectral and cross-wavelet analyses. Integr Zool. 2007;2(3):144–53.
Schmid BV, Büntgen U, Easterday WR, Ginzler C, Walløe L, Bramanti B, Stenseth NC. Climate-driven introduction of the Black Death and successive plague reintroductions into Europe. Proc Natl Acad Sci U S A. 2015;112(10):3020–5.
Xu L, Schmid BV, Liu J, Si X, Stenseth NC, Zhang Z. The trophic responses of two different rodent-vector-plague systems to climate change. Proc Biol Sci. 2015;282(1800):20141846.
Vogler AJ, Chan F, Nottingha R, Andersen G, Drees K, Beckstrom-Sternberg SM, Wagner DM, Chanteau S, Keim P. A decade of plague in Mahajanga, Madagascar: insights into the global maritime spread of pandemic plague. mBio. 2013;4(1):e00623–12.
Wheelis M. Biological warfare at the 1346 Siege of Caffa. Emerg Infect Dis. 2002;8(9):971–5.
Coleman MP. A plague epidemic in voluntary quarantine. Int J Epidemiol. 1986;15(3):379–85.
Seifert L, Wiechmann I, Harbeck M, Thomas A, Grupe G, Projahn M, Scholz HC, Riehm JM. Genotyping Yersinia pestis in historical plague: evidence for long-term persistence of Y. pestis in Europe from the 14th to the 17th century. PLoS One. 2016;11(1):e0145194.
Bos KI, Herbig A, Sahl J, Waglechner N, Fourment M, Forrest SA, Klunk J, Schuenemann VJ, Poinar D, Kuch M, Golding GB, Dutour O, Keim P, Wagner DM, Holmes EC, Krause J, Poinar HN. Eighteenth century Yersinia pestis genomes reveal the long-term persistence of an historical plague focus. eLife. 2016. doi:10.7554/eLife.12994.
Devaux CA. Small oversights that led to the Great Plague of Marseille (1720–1723): lessons from the past. Infect Genet Evol. 2013;14:169–85.
Haesser H. Lehrbuch der Geschichte der Medizin und der epidemischen Krankheiten. Jena: Hermann Duft Verlag; 1875 (Dritte Bearbeitung, Band 1, 2 und 3).
Ilmoni I. Bidrag til Nordens sjukdoms-historia [Contributions to the history of diseases in the Nordic countries]. Helsingfors [Helsinki]: J Simelii Arfvingar;1846, 1849, 1853 (1, 2 ock 3).
Walløe L. Plague and population: Norway 1350–1750. Avhandlinger (Norske videnskapsakademi), new series, No. 17. Oslo: University of Oslo, Department of Physiology; 1995.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Bramanti, B., Stenseth, N.C., Walløe, L., Lei, X. (2016). Plague: A Disease Which Changed the Path of Human Civilization. In: Yang, R., Anisimov, A. (eds) Yersinia pestis: Retrospective and Perspective. Advances in Experimental Medicine and Biology, vol 918. Springer, Dordrecht. https://doi.org/10.1007/978-94-024-0890-4_1
Download citation
DOI: https://doi.org/10.1007/978-94-024-0890-4_1
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-024-0888-1
Online ISBN: 978-94-024-0890-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)