
Abstract
Aim
We aim to discuss cases with gastrointestinal stromal tumor and leiomatosis peritoneal dissemeniata LPD regarding their diagnosis and surgical management with pitfalls related. We also aim to focus on management of multiple nodular serosal lesions.
Method
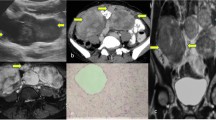
Two cases are presented. Both were diagnosed as advanced ovarian cancer on CT and ultrasound imaging by multiple nodular peritoneal lesions, omental cake and adnexal masses. Tumor markers were normal in both cases. Both were scheduled for exploratory laparotomy. One patient diagnosed with neurofibromatosis type I.
Results
Midline laparotomy was done for one case revealing normal adnexa with multiple fibroid uterus, peritoneal solid masses with large mesenteric and omental masses related to the small intestine. Total hysterectomy with bilateral salpingo-oophorectomy, total omentectomy and resection anastomosis for the small intestine with removal of macroscopic lesions were done. Midline line laparotomy was done for the second case revealing free adnexa with subserous vascular fibroids and omental fibroid solid masses. Total hysterectomy with bilateral salpingo-oophorectomy and total omentectomy and removal of macroscopic peritoneal lesions seen were done. The second case was diagnosed as Disseminated Peritoneal Leiomyomatosis, and the other case was diagnosed with multiple uterine fibroid and metastatic GIST on histopathology.
Conclusion
Disseminated Peritoneal Leiomyomatosis and metastatic GIST can be similar on imaging and operative findings. Also they are similar to other lesions especially peritoneal carcinomatosis as in advanced ovarian cancer. These pathologies should be kept on mind when encountering multiple solid nodular masses in the visceral and parietal wall peritoneum and the omentum on imaging and intra-operative especially with normal associated tumor markers of ovarian cancer as serum CA125. Surgical and postoperative management differ according to the pathology. These pathologies should be confirmed by histopathology and immunohistochemistry. Frozen section is highly needed in these cases to optimize management.


Similar content being viewed by others


References
Al-Talib A, Tulandi T. Pathophysiology and possible iatrogenic cause of leiomyomatosis peritonealis disseminata. Gynecol Obstet Invest. 2010;69(4):239–44.
Fletcher C, Berman J, Corless C, et al. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol. 2002;33:459–65.
Levy AD, Remotti HE, Thompson WM, et al. Gastrointestinal stromal tumors: radiologic features with pathologic correlation. Radiographics. 2003;23(2):283–304. https://doi.org/10.1148/rg.232025146 (Pubmed citation).
Kumar V, Abbas AK. Robbins and cotran pathologic basis of disease. Philadelphia: W B Saunders Co; 2005. ISBN 0721601871.
King DM. The radiology of gastrointestinal stromal tumours (GIST). Cancer Imaging. 2005;5:150–6. https://doi.org/10.1102/1470-7330.2005.0109.
Maki RG. Gastrointestinal stromal tumors (GIST) and their management. Gastrointest Cancer Res. 2007;1(4 Suppl 2):S81–4.
Warakaulle DR, Gleeson F. MDCT appearance of gastrointestinal stromal tumors after therapy with imatinib mesylate. AJR Am J Roentgenol. 2006;186(2):510–5. https://doi.org/10.2214/AJR.04.1516.
Lassau N, Lamuraglia M. Chami L et al. Gastrointestinal stromal tumors treated with imatinib: monitoring response with contrast-enhanced sonography. AJR Am J Roentgenol. 2006;187(5):1267–73. https://doi.org/10.2214/ajr.05.1192.
Haaga JR, Boll D. CT and MRI of the whole body. Maryland: Mosby; 2011. ISBN 0323053750.
Weissleder R, Wittenberg J, Harisinghani MMGH. Primer of diagnostic imaging. Maryland: Mosby; 2011. ISBN 0323065384.
Fortman BJ. Torricelli-Bernoulli sign in an ulcerating gastric leiomyosarcoma. AJR Am J Roentgenol. 1999;173(1):199–200. https://doi.org/10.2214/ajr.173.1.10397126.
Choi H, Charnsangavej C, de Castro Faria S, et al. CT evaluation of the response of gastrointestinal stromal tumors after imatinib mesylate treatment: a quantitative analysis correlated with FDG PET findings. AJR Am J Roentgenol. 2004;183(6):1619–28.
Fasih N, Prasad shanbhogue AK, Macdonald DB, et al. Leiomyomas beyond the uterus: unusual locations, rare manifestations. Radiographics. 2008;28(7):1931–48. https://doi.org/10.1148/rg.287085095.
Rosica G, Santilli G, Bucari D, et al. A case of disseminated peritoneal leiomyomatosis and diffuse uterine leiomyomatosis. Clin Exp Obstet Gynecol. 2011;38(1):84–7.
Elagwany AS, Rady HA, Abdeldayem TM. A case of parasitic leiomyoma with serpentine omental blood vessels: an unusual variant of uterine leiomyoma. J Taibah Univ Med Sci. 2014;9(4):338–40.
Kökçü A, Alvur Y. Bariş YS et-al. Leiomyomatosis peritonealis disseminata. Acta Obstet Gynecol Scand. 1994;73(1):81–3.
Clement PB, Young RH. Atlas of gynecologic surgical pathology: expert consult: online (Atlases in Diagnostic Surgical Pathology). Saunders. ISBN: B00GC3C45I.
Levy AD, Shaw JC, Sobin LH. Secondary tumors and tumorlike lesions of the peritoneal cavity: imaging features with pathologic correlation. Radiographics. 2009;29(2):347–73. https://doi.org/10.1148/rg.292085189.
Author information
Authors and Affiliations
Contributions
Elagwany had done the diagnoses and surgery along with writing the article.
Corresponding author
Ethics declarations
Conflict of interest
All authors have nothing to declare.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from the patient included in the study.
Rights and permissions
About this article

Cite this article
El-Agwany, A.S., Meleis, M.H. Disseminated Peritoneal Leiomyomatosis and Metastatic GIST: Differential Diagnosis Dilemma Regarding Multiple Nodular Serosal Lesions and Management. Indian J Gynecol Oncolog 16, 17 (2018). https://doi.org/10.1007/s40944-018-0185-x
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40944-018-0185-x