
Abstract
Influenza virus infections cause severe illness worldwide. Vaccination reduces the morbidity and mortality of influenza. The efficacy of vaccines varies due to antigenic differences between the circulating influenza strains and the vaccine. Neuraminidase inhibitors are effective for prophylaxis and treatment of influenza infections, and the emergence of drug resistant mutants is an important challenge. Full-length nucleotide and deduced amino acid sequences of the hemagglutinin and neuraminidase genes of three 2009 pandemic influenza A/H1N1 isolates were compared with the vaccine strain and some strains from different countries. Phylogenetic analysis for hemagglutinin and neuraminidase showed they were related to their vaccine strain, with an average of 99.56 and 99.53% sequence identity, respectively. No genetic indication of resistance to neuraminidase inhibitors was found. Although genomic analysis of hemagglutinin and neuraminidase genes of Iranian strains in comparison to the corresponding vaccine strain revealed some mutations, none of these were identified in functionally important receptor-binding sites.
Similar content being viewed by others


Introduction
Influenza A viruses are respiratory pathogens that can cause moderate to severe illness in humans. Annual epidemics and pandemics (occurring at 10- to 50-year intervals) cause millions of cases of severe illness and deaths worldwide. Influenza epidemics are mostly due to the accumulation of point mutations (antigenic drift) in hemagglutinin, HA, and neuraminidase, NA (particularly in HA), and influenza pandemics are mainly due to emergence of a new influenza subtype (antigenic shift) in the human population [1].
The major influenza virus component determining epidemiological dynamics is the predominant surface glycoprotein HA on the viral envelope, which serves as the attachment protein, determining whether the virus is able to bind to and infect cells of different species by attaching to sialic acid receptors on the cells [2].
NA plays a critical role in the spread of the influenza viruses. It facilitates the elution of progeny virions from infected cells and prevents their self-aggregation by cleaving terminal sialic acid from glycoconjugates [3]. Neuraminidase inhibitors (zanamivir and oseltamivir) are effective antiviral drugs for the treatment and prophylaxis of influenza infections [4]. H275Y is the molecular marker of oseltamivir resistance [5].
In the 20th century, three influenza pandemics occurred: the H1N1 Spanish Flu in 1918, the H2N2 Asian Flu in1957 and the H3N2 Hong Kong Flu in 1968 [6].
Now, influenza pandemics of the 21st century are a real threat. In late April 2009, infection of humans with influenza virus A(H1N1)v emerged in Mexico and the USA [7]. The transmissibility of pandemic H1N1 virus is higher than that of the seasonal H1N1, and the proportion of infected children with clinical symptoms is twice as high as that of the adults [8].
These patients show symptoms of acute respiratory illness, including fever, cough, and headache, associated with diarrhea and vomiting in some cases [7]. The virus spread rapidly throughout the world, which warranted the declaration of “Pandemic (H1N1) 2009” by the WHO on June11, 2009 [10]. As of November 15, there had been over 526,060 infected individuals and at least 6,770 confirmed human deaths worldwide [10].
The effective ways to reduce the influenza morbidity and mortality are vaccination and antiviral drugs. One major challenge is that the efficacy of influenza vaccines varies from year to year due to antigenic differences between the HA and NA genes of circulating influenza strains and the vaccine [11, 12]. Another challenge is the emergence of drug-resistant mutants. Identifying potentially oseltamivir-resistant viruses is important because it is the only oral drug currently recommended for prophylaxis and treatment of influenza infections [5].
Investigating molecular changes in antigenic determinants of HA and NA as well as mutations conferring resistance to oseltamivir are essential goals, especially now that we are facing pandemic influenza threats.
Materials and methods
Respiratory specimens (throat swabs) from patients with clinical diagnosis of acute respiratory infection were collected within seven days of onset of clinical symptoms. The specimens were sent to the National Influenza Centre in School of Public Health of Tehran University of Medical Sciences by the Iran Ministry of Health and Medical Education.
Specimens were inoculated onto MDCK cells for virus isolation. Three isolates of pandemic H1N1 influenza viruses (collected in July 2009) were available for sequencing. The names and abbreviations of isolates, the dates of sample collection and the accession numbers of their complete HA and NA sequences in GenBank are listed in Table 1.
RNA extraction was performed on cell culture supernatants using a NucleoSpin® RNA virus extraction kit (Machery-Nagel Company, Germany) according to the manufacturer’s instructions.
RNA was transcribed to cDNA at 37°C for 2 h using the MMULV RT enzyme and random hexamer primers.
Amplification of the full-length HA and NA genes was carried out using two sets of forward and reverse primers to amplify two overlapping fragments for each gene (Table 2). The resulting amplicons were sequenced.
BioEdit version 7.0.0 DNA analysis software [13] was used to analyze sequences. Phylogenetic trees were constructed by using the TREECON package version 1.3 b [14], applying Kimura’s two-parameter method and the neighbor-joining method with bootstrap analysis (1,000 replicates).
Results
Three 2009 Pandemic influenza A/H1N1 isolates collected from different provinces of Iran were used in this study. The full-length nucleotide and deduced amino acid sequences of their HA and NA genes were compared with the vaccine strain and some strains from different countries.
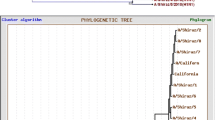
In accordance with the branching in the phylogenetic tree, the HA genes of Iranian pandemic H1N1 viruses were closely related (Fig. 1). They had an average of 99.56% sequence identity to the vaccine strain and 99.3–100% similarity to isolates from different countries.

Phylogenetic tree of the hemagglutinin (HA) gene of Iranian pandemic H1N1 isolates (in italics), the vaccine strain (in bold), and some isolates from other countries
Although genomic analysis of HA genes of Iranian strains in comparison to the corresponding vaccine strain revealed eight mutations, of which four were non-synonymous, none of these were identified in known functionally important receptor-binding sites or cleavage sites. As for the vaccine strain, seven potential glycosylation sites in the HA protein were found in Iranian strains.
The phylogenetic tree of the NA genes of the Iranian isolates showed that they were closely related to each other and the vaccine strain with an average of 99.53% sequence identity (Fig. 2).

Phylogenetic tree of the neuraminidase (NA) gene of Iranian pandemic H1N1 isolates, the vaccine strain, human isolates from other countries, and some swine isolates. The vaccine strain is shown in bold
Analysis of the NA amino acid sequence showed conserved residues in both catalytic sites and framework sites for all isolates. All Iranian isolates had four mutations in the rest of the gene compared to the vaccine strain, three of which were non-synonymous.
Furthermore, one isolate had three more mutations, of which one of them was silent. Substitutions conferring resistance to neuraminidase inhibitors (NAIs) were not observed in the NA genes of the Iranian isolates. In the NA protein, eight potential glycosylation sites were found.
Discussion
In the present study, the nucleotide and deduced amino acid sequences of the HA and NA genes of three Iranian pandemic H1N1 isolates were compared to those of the WHO-recommended vaccine strain, A/California/7/2009 (H1N1)v.
Genetic relationships of the HA genes of Iranian isolates with the vaccine and some strains from other countries were examined by neighbor-joining analysis with 1000 bootstrapped replicates. This showed that the isolates were related to their vaccine strains, with an average of 99.56% sequence identity. As shown in Fig. 1, our phylogenetic analysis revealed that the HA genes of Iranian pandemic H1N1 influenza viruses are closely related to each other and to those of the vaccine strain.
As in other studies, nucleotide alignment of the HA gene using BioEdit software revealed that residues that make contact with sialic acid (Y94, KGVTA133-137, W153, V155, H183, S186, L194 and Q226) [15] and residues in cleavage site (PSIQSR 325-330) [16] were conserved among all strains.
Although evaluation of evolutionary trends of A(H1N1) influenza virus hemagglutinin revealed predominant roles in determining receptor-binding specificity of A(H1N1) HA, and positive selection of HA 190 and 225 in A(H1N1) strains [17], no mutations were detected in Iranian isolates (collected in July 2009), isolates selected from other countries or the vaccine strain.
In HA, seven potential glycosylation sites (positions 14, 26, 90, 279, 290, 484 and 543) were detected in the vaccine strain and all Iranian isolates. The specific polypeptide for N-linked glycosylation is defined as (Asn-X-Ser/Thr), where X can be any amino acid except proline or aspartic acid [18].
Deem and Pan modified the epitope regions of H1-subtype influenza from Caton et al. [19]. They introduced five epitopes (A–E) for HA glycoprotein with A/California/04/2009 numbering [11].
Our isolates had eight mutations in comparison with the vaccine strain. C256T, T616A, A849G, A970G and C1395T were detected in all three isolates; G829A and A1050G just in A/Lorestan/1599/2009(H1N1) and C1424T in A/Ghom/1550/2009(H1N1). Four of these mutations were nonsynonymous: P86S in antigenic site E, S206D in antigenic siteD, D277N in antigenic site C and I324 V. D277N was detected only in A/Lorestan/1599/2009(H1N1), and the others were found in all three Iranian isolates.
On November 20, the Norwegian Institute of Public Health informed WHO of a mutation (D225G) detected in three H1N1 viruses isolated from two fatal cases of pandemic influenza and one patient with severe illness. This mutation might have occurred sporadically and spontaneously. Preliminary genetic sequencing performed by WHO influenza collaborating centers revealed no significant changes in the pandemic (H1N1) 2009 virus, and it was similar to the vaccine strain, which meant there had been no significant reassortment with other influenza viruses. However, small changes, such as receptor-binding domain changes were not ruled out. In addition to Norway, this mutation has been observed in Brazil, China, Japan, Mexico, Ukraine, and the US [9].
The D225G mutation allows the virus to bind to receptors on cells lining the lungs. It could affect transmission or tropism and also affect vaccine reactivity [20, 21]. However, no evidence currently suggests that these mutations lead to an unusual increase in the number of infections or severe and fatal cases [9].
In our study, this mutation was not detected. However, our relatively small sample size limited the power of our analysis, and further investigation needs to be done on a greater number of isolates.
Like HA, our analysis on the NA gene of Iranian pandemic H1N1 isolates compared to the WHO-recommended vaccine strain revealed that they had an average of 99.53% sequence identity to the vaccine strain and 99.8% similarity to some isolates from different countries and were closely related to them in the phylogenetic tree (Fig. 2).
Molecular analysis showed the expected conserved residues in both catalytic sites and framework sites for all isolates [3, 22]. Although all Iranian isolates had four mutations in the rest of the gene compared to the vaccine strain, C12A, G316A, A742G and G1044A, three of them were nonsynonymous: N4K, V106I and N248D, and the second and third mutations were also found in isolates from other countries (data not shown).
Furthermore, A/Lorestan/1599/2009 had two more substitutions: F74L and V81G, the former one was also found in one isolate from Colombia (A/Bogota/0466N/2009).
Eight glycosylation sites were found in the NA of isolates (at positions 50, 58, 63, 68, 88, 146, 235 and 386 positions).
A genetic marker of oseltamivir drug resistance in NA is the H275Y mutation. This mutation occurs at or near the active site of the enzyme, and it was predicted previously that mutant viruses would be less viable than sensitive ones [23].
Systematic surveillance conducted by the Global Influenza Surveillance Network, supported by WHO Collaborating Centres and other laboratories have detected sporadic incidents of H1N1 pandemic viruses that showed resistance to oseltamivir. By the 25th of September, 28 resistant viruses had been detected and characterized worldwide [24].
In this study, the H275Y mutation was not observed in the NA gene of Iranian pandemic isolates.
References
Hidayatullah TA (2009) Cloning and expression of antigenic sites of Hemagglutinin of Influenza A virus. IJIB 6(3):137–142
Mpolya EA, Furuse Y, Nukiwa N, Suzuki A, Kamigaki T and Oshitani H (2009) Pandemic (H1N1) 2009 virus viewed from an epidemiological triangle model. JDR l.4(5):356–364
Richarda M, Del′eagea C, Barth′el′emya M, Linb YP, Hay A, Linaa B et al (2008) Impact of influenza A virus neuraminidase mutations on the stability, activity, and sensibility of the neuraminidase to neuraminidase inhibitors. J Clin Virol 41:20–24
Moscona A (2005) Neuraminidase inhibitors for influenza. NEJM 353(13):1363–1373
Sheu TG, Deyde VM, Okomo-Adhiambo M, Garten RJ, Xu X, Bright RA et al (2008) Surveillance for neuraminidase inhibitor resistance among human influenza A and B viruses. AAC 52(9):3284–3292
Kilbourne AD (2006) Influenza pandemics of the 20th century. Emerg Infect Dis 12(1):9–14
Naffakh N, Werf S (2009) An outbreak of swine-origin influenza A(H1N1) virus with evidence for human-to-human transmission. Microb Infect. doi:10.1016/j.micinf
Donga H, Zhangb Y, Xionga H, Yana A, Dingc G, Chenag Y et al. (2009) Detection of human novel influenza A (H1N1) viruses using multi-fluorescent real-time RT-PCR. Virus Res 47:85–90
WHO (2009) Pandemic (H1N1) 2009 briefing note 17. Public health significance of virus mutation detected in Norway. 20 November. http://www.who.int
WHO (2009) Pandemic (H1N1) 2009, update 75. http://www.who.int
Deem MW, Pan K (2009) The epitope regions of H1-subtype influenza A, with application to vaccine efficacy. PEDS 22(9):543–546
Smith DJ, Lapedes AS, Jong JC, Bestebroer TM, Rimmelzwaan GF, Osterhaus ADME et al (2004) Mapping the antigenic and genetic evolution of influenza virus. Science 305(5682):371–376
Hall TA (1999) BioEdit: a user-friendly biological sequence alignment editor and analysis program for Windows 95/98/NT. Nucl Acids Symp Ser 41:95–98
Van de Peer Y, De Wachter R (1997) Construction of evolutionary distance trees with TREECON for Windows: accounting for variation in nucleotide substitution rate among sites. Comput Applic Biosci 13:227–230
Padlan EA (2009) The pandemic 2009 (H1N1) swine influenza virus is mild compared to the pandemic 1918 (H1N1) virus because of a proline-to-serine substitution in the receptor- binding site of its hemagglutinin: a hypothesis. Med Hypotheses 73(5):770–780. doi:10.1016/j.mehy.2009.09.034
Zambon MC (1999) Epidemiology and pathogenesis of influenza. JAC 44:3–9
Shen, J, Ma1, J, Wang, Q (2009) Evolutionary Trends of A(H1N1) Influenza Virus Hemagglutinin Since 1918. PLoS one. 4(11):e7789, 1–10 (http://www.plosone.org)
Helenius A, Aebi M (2004) Roles of N-linked glycans in the endoplasmic reticulum. Annu Rev Biochem 73:1019–1049
Caton AJ, Brownlee GG, Yewdell JW (1982) The antigenic structure of the influenza virus A/PR/8/34 haemagglutinin (H1 subtype). Cell 31:417–427
Racaniello V (2009) The D225G change in 2009 H1N1 influenza virus is not a concern. http://www.virology.ws (24 November)
Tumpey T, Maines T, Van Hoeven N, Glaser L, Solorzano A, Pappas C et al (2007) A two-amino acid change in the hemagglutinin of the 1918 influenza virus abolishes transmission. Science 315(5812):655–659
Chutinimitkul S, Chieochansin T, Payungporn S, Samransamruajkit R, Hiranras T, Theamboonlers A et al (2007) Molecular characterization and phylogenetic analysis of H1N1 and H3N2 human influenza A viruses among infants and children in Thailand. Virus Res 132:122–131
Dharan NJ, Gubareva LV, Meyer J, Okomo-Adhiambo M, McClinton RC, Marshall SA et al (2009) Infections with oseltamivir-resistant influenza A(H1N1) virus in the United States. JAMA 301(10):1034–1041
Antiviral use and the risk of drug resistance. Pandemic (H1N1) 2009. Weekly update 66. http://www.who.int/csr/disease/swineflu/notes/h1n1_antiviral_use_20090925/en/index.html
Acknowledgments
We would like to thank the entire staff of the National Influenza Centre, Tehran. University of Medical Sciences, for helping us with the research.
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jandaghi, N.Z.S., Azad, T.M., Naseri, M. et al. Molecular and genetic characteristics of hemagglutinin and neuraminidase in Iranian 2009 pandemic influenza A(H1N1) viruses. Arch Virol 155, 717–721 (2010). https://doi.org/10.1007/s00705-010-0629-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00705-010-0629-9