
Abstract
Background
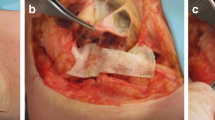
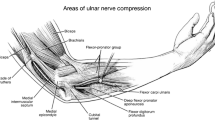
Fibrous bands (FB) are structures that cross the ulnar nerve (UN), distal to the cubital tunnel (CT). In surgical decompression of the UN in the elbow region, by endoscopy, these FB significantly impact UN visibility. The aim of the current study was to characterize the anatomical characteristics of these FB distal to the CT.
Methodology
Eighteen formalinized upper limbs were dissected, nine right and nine left, within the Department of Anatomy of the Federal University of the State of Rio de Janeiro (UNIRIO). The dissections were performed with micro techniques, under a magnifying glass and a microscope. Classical UN exposure was established in the elbow region.
Results
Of the 18 upper limbs studied, 50% lacked any FB. When present, both the number and location of the FB varied, as near to the cubital tunnel as 3 cm past the UN’s entrance into the tunnel, and as far away as almost 11 cm distal to it. Overall, there were no FB on either the left or right side in three cadavers (33.3%), FB on both the left and right side in three, and FB only on the left in three, meaning that FB were twice as common in left limbs (n = 6) as on the right (n = 3).
Conclusions
Our study identified FB in 50% of the dissected limbs, all within 3–11 cm of the CT, though their number and location varied. Further studies are necessary to describe FB variations associated with compressive neuropathies of the UN distal to the CT.




Similar content being viewed by others

References
Bultmann C, Hoffmann R (2009) Endoscopic decompression of the ulnar nerve in cubital tunnel syndrome. Oper Orthop Traumatol 21(2):193–205
Cobb TK (2010) Endoscopic cubital tunnel release. J Hand Surg Am 35(10):1690–1697
Degeorges R, Masquelet AC (2002) The cubital tunnel: anatomical study of its distal part. Surgical Radiolog Anat 24(3–4):169–176
Hoffmann R, Lubahn J (2013) Endoscopic cubital tunnel release using the Hoffmann technique. J Hand Surg [Am] 38(6):1234–1239
Hoffmann R, Siemionow M (2006) The endoscopic management of cubital tunnel syndrome. J Hand Surg Br 31(1):23–29
Kroonen LT (2012) Cubital tunnel syndrome. Orthop Clin N Am 43(4):475–486
Mirza A, Reinhart MK, Bove J, Litwa J (2011) Scope-assisted release of the cubital tunnel. J Hand Surg [Am] 36(1):147–151
Mirza A, Mirza JB, Lee BK, Adhya S, Litwa J, Lorenzana DJ (2014) An anatomical basis for endoscopic cubital tunnel release and associated clinical outcomes. J Hand Surg [Am] 39(7):1363–1369
Moore KL, Dalley AF, Agur AMR (2014) Upper limb. In: Clinically oriented anatomy. Guanabara Koogan, Brazil, pp 670–819
Nagle DJ, Patel RM, Paisley S (2012) Endoscopic detection of compressing fascial bands around the ulnar nerve within the FCU. Hand 7(1):103–107
Palmer BA, Hughes TB (2010) Cubital tunnel syndrome. J Hand Surg [Am] 35(1):153–163
Siemionow M, Agaoglu G, Hoffmann R (2007) Anatomic characteristics of a fascia and its bands overlying the ulnar nerve in the proximal forearm: a cadaver study. J Hand Surg Eur 32(3):302–307
Simsek S, Er U, Demirci A, Sorar M (2011) Operative illustrations of the Osborne’s ligament. Turk Neurosurg 21(2):269–270
Tsai TM, Bonczar M, Tsuruta T, Syed AS (1995) A new operative technique: cubital tunnel decompression with endoscope assistance. Hand Clin 11(1):71–80
Tsai T, Chen I, Majd ME, Lim B (1999) Cubital tunnel release with endoscopic assistance: results of a new technique. J Hand Surg [Am] 24(1):21–29
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Our study has been approved by the appropriate ethics committee.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Comments
An interesting cadaveric study confirming and elaborating on prior studies demonstrating the presence of fibrous bands extending as far distally as 11 cm in the forearm that may result in entrapment of the ulnar nerve. Such a possibility is why I always take a no. 4 Penfield dissector and pass it far both distally and proximally along the course of the ulnar nerve after exposing and decompressing it to assure myself of an adequate decompression. It will be interesting to correlate these findings with ultrasound imaging studies in patients and determine their clinical significance, perhaps with careful NCV incing studies, both in clinic and intraoperatively, that may demonstrate a drop in nerve conduction velocity and/or amplitude across these entrapped segments of ulnar nerve. At present, this is an interesting finding that warrants further investigation to determine its clinical significance and potential impact on clinical outcome.
Michel Kliot
CA, USA
Rights and permissions
About this article

Cite this article
Guedes-Correa, J.F., Brown, R.S. An anatomical study of so-called fibrous bands around the ulnar nerve distal to the cubital tunnel. Acta Neurochir 160, 1591–1596 (2018). https://doi.org/10.1007/s00701-018-3562-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-018-3562-4