
The Post-Traumatic Growth Journey of Women Who Have Survived Intimate Partner Violence: A Synthesized Theory Emphasizing Obstacles and Facilitating Factors


Abstract
:1. Introduction
Purpose of the Theory Development and the Main Question
2. Materials and Methods
2.1. Design of the Theory Development
2.2. The Method of Theory Synthesis
2.3. Steps in the Theory Synthesis
3. Results
3.1. Description of the Theory
3.1.1. Component 1: Trauma before IPV
3.1.2. Component 2: Influences of Former Traumas on the Experience of IPV
3.1.3. Component 3: Experience of IPV
3.1.4. Component 4: Consequences of IPV
3.1.5. Component 5: Obstacles on the PTG Journey
3.1.6. Component 6: Facilitators on the PTG Journey
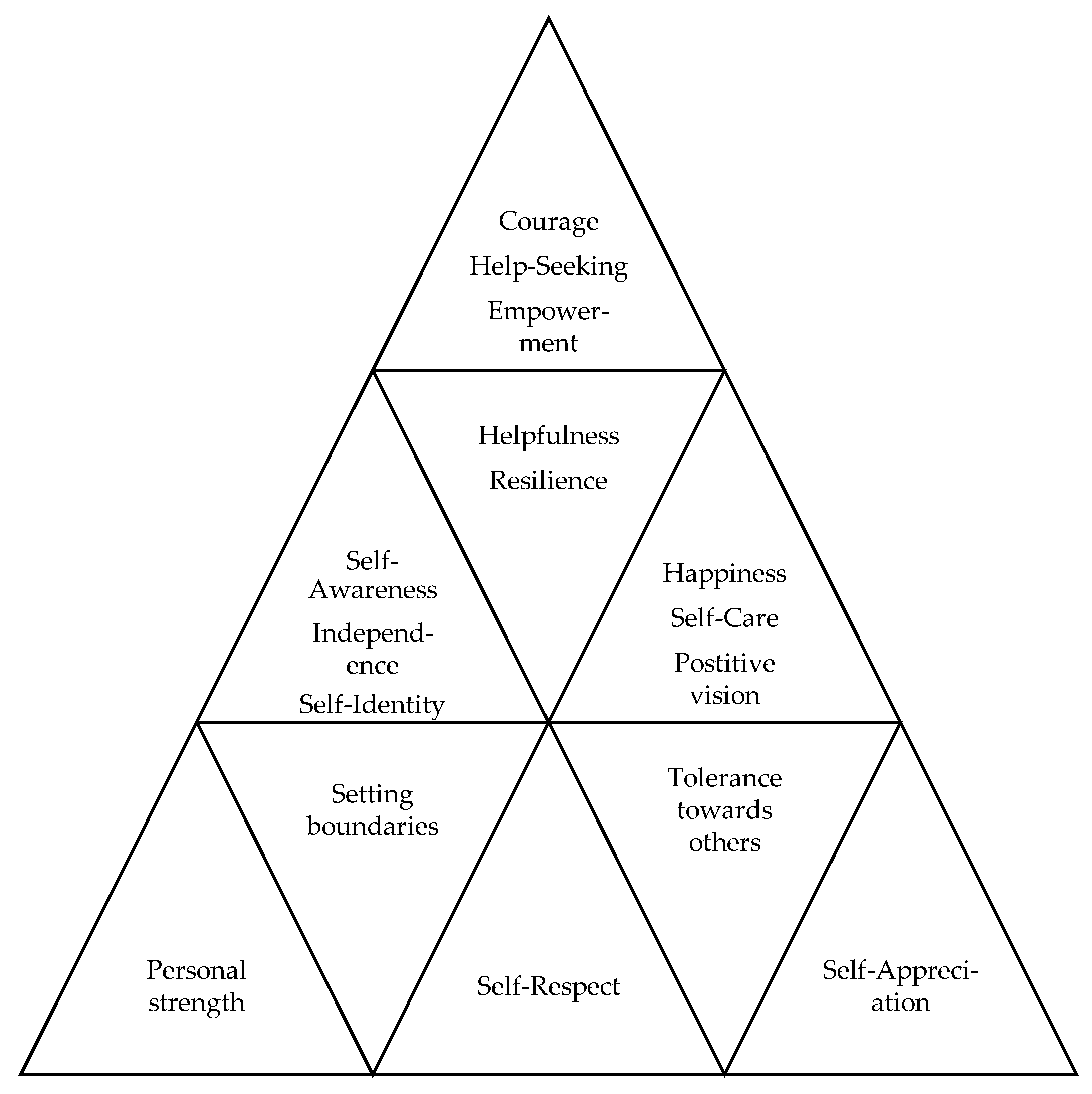
3.1.7. Component 7: Post-Traumatic Growth Following IPV
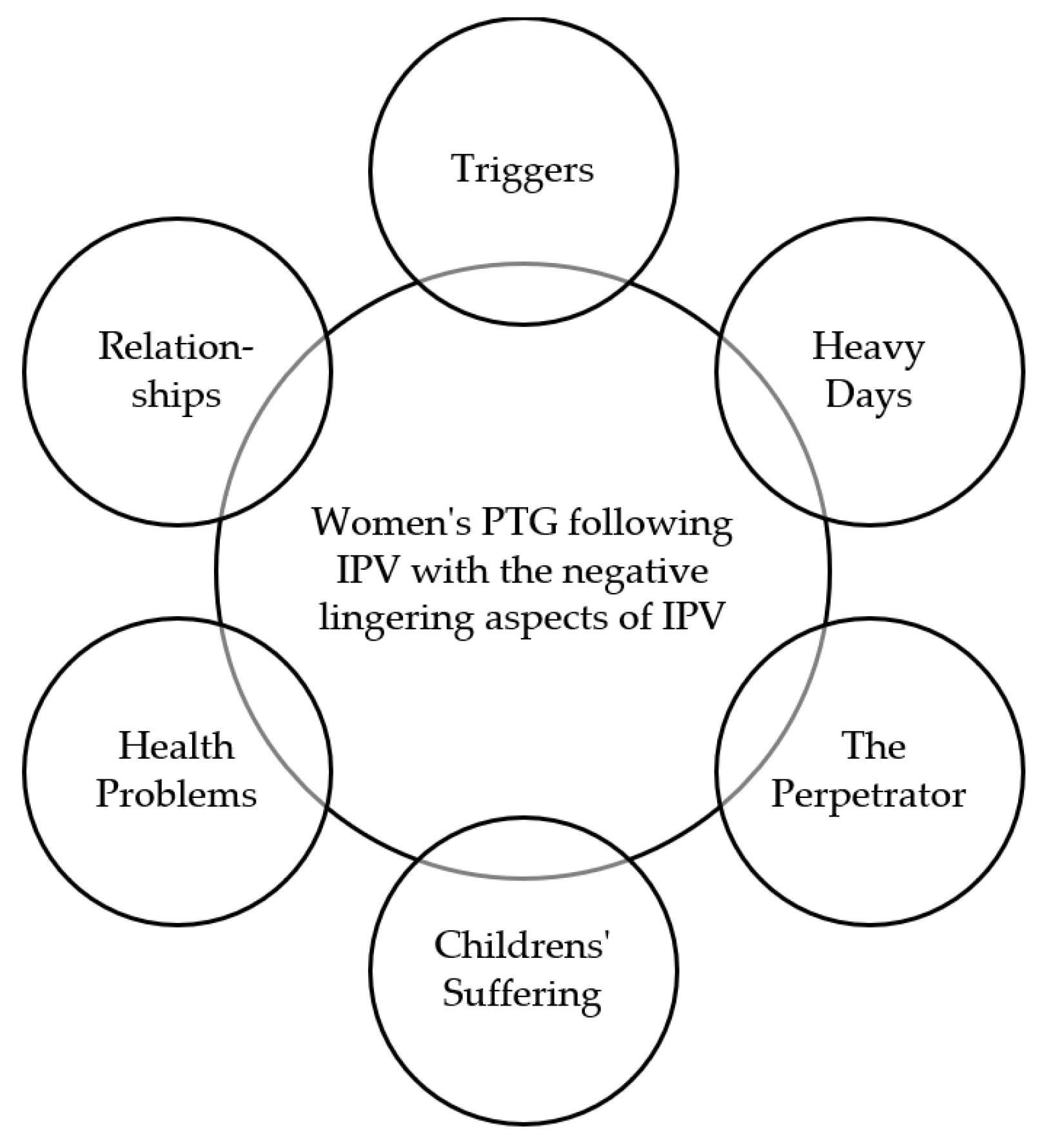
3.1.8. Component 8: Lingering Effects of IPV in PTG
4. Discussion
4.1. Limitation of the Theory Development
4.2. Future Research and Theory Development Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- D’Amore, C.; Martin, S.L.; Wood, K.; Brooks, C. Themes of Healing and Posttraumatic Growth in Women Survivors’ Narratives of Intimate Partner Violence. J. Interpers. Violence 2021, 36, NP2697–NP2724. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Violence against Women. 2021. Available online: https://www.who.int/en/news-room/fact-sheets/detail/violence-against-women (accessed on 2 May 2022).
- World Health Organization. Violence against Women: Intimate Partner and Sexual Violence against Women; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/329889/WHO-RHR-19.16-eng.pdf?ua=1 (accessed on 18 April 2022).
- Russo, N.F.; Pirlott, A. Gender-Based Violence: Concepts, Methods, and Findings. Ann. N. Y. Acad. Sci. 2006, 1087, 178–205. [Google Scholar] [CrossRef] [PubMed]
- Krahé, B. Violence against women. Curr. Opin. Psychol. 2018, 19, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Sanjel, S. Gender-Based Violence: A Crucial Challenge for Public Health. Kathmandu Univ. Med J. 2015, 11, 179–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, D.E.; Vigod, S.; Riazantseva, E. New Developments in Intimate Partner Violence and Management of Its Mental Health Sequelae. Curr. Psychiatry Rep. 2016, 18, 4. [Google Scholar] [CrossRef]
- World Health Organization. Researching Violence against Women: Practical Guidelines for Researchers and Activists; World Health Organization: Geneva, Switzerland, 2005; Available online: https://apps.who.int/iris/bitstream/handle/10665/42966/9241546476_eng.pdf (accessed on 18 April 2022).
- World Health Organization. Global and Regional Estimates of Violence against Women: Prevalence and Health Effects of Intimate Partner Violence and Non-Partner Sexual Violence; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/bitstream/handle/10665/85239/?sequence=1 (accessed on 18 April 2022).
- Stark, L.; Ager, A. A Systematic Review of Prevalence Studies of Gender-Based Violence in Complex Emergencies. Trauma Violence Abus. 2011, 12, 127–134. [Google Scholar] [CrossRef]
- Ali, P.A.; Dhingra, K.; McGarry, J. A literature review of intimate partner violence and its classifications. Aggress. Violent Behav. 2016, 31, 16–25. [Google Scholar] [CrossRef]
- Johnson, M.P. Gender and types of intimate partner violence: A response to an anti-feminist literature review. Aggress. Violent Behav. 2011, 16, 289–296. [Google Scholar] [CrossRef]
- McHugh, M.C.; Frieze, I.H. Intimate Partner Violence: New Directions. Ann. N. Y. Acad. Sci. 2006, 1087, 121–141. [Google Scholar] [CrossRef]
- Mijatovic-Jovanovic, V.; Cankovic, S.; Milijasevic, D.; Ukropina, S.; Jovanovic, M.; Cankovic, D. Health consequences of domestic violence against women in Serbia. Vojn. Pregl. 2020, 77, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Heise, L.; Ellsberg, M.; Gottmoeller, M. A global overview of gender-based violence. Int. J. Gynecol. Obstet. 2002, 78, S5–S14. [Google Scholar] [CrossRef]
- Campbell, J.C. Health consequences of intimate partner violence. Lancet 2002, 359, 1331–1336. [Google Scholar] [CrossRef]
- Yim, I.S.; Kofman, Y.B. The psychobiology of stress and intimate partner violence. Psychoneuroendocrinology 2019, 105, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K. Intimate Partner Violence (IPV) and Neurological Outcomes: A Review for Practitioners. J. Aggress. Maltreatment Trauma 2019, 28, 807–825. [Google Scholar] [CrossRef]
- Loxton, D.; Dolja-Gore, X.; Anderson, A.E.; Townsend, N. Intimate partner violence adversely impacts health over 16 years and across generations: A longitudinal cohort study. PLoS ONE 2017, 12, e0178138. [Google Scholar] [CrossRef] [Green Version]
- Zara, G.; Gino, S. Intimate Partner Violence and its Escalation Into Femicide. Frailty thy Name Is “Violence against Women”. Front. Psychol. 2018, 9, 1777. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Multi-Country Study on Women’s Health and Domestic Violence against Women: Summary Report of Initial Results on Prevalence, Health Outcomes and Women’s Responses; World Health Organization: Geneve, Switzerland, 2005; Mise en page 1; Available online: ceid.org.tr (accessed on 18 April 2022).
- Chiesa, A.E.; Kallechey, L.; Harlaar, N.; Ford, C.R.; Garrido, E.F.; Betts, W.R.; Maguire, S. Intimate partner violence victimization and parenting: A systematic review. Child Abus. Negl. 2018, 80, 285–300. [Google Scholar] [CrossRef]
- Van Heugten, K.; Wilson, E. Witnessing intimate partner violence: Review of the literature on coping in young persons. Aotearoa New Zealand Soc. Work 2008, 20, 52–62. [Google Scholar] [CrossRef]
- Kishton, R.; Sinko, L.; Ortiz, R.; Islam, N.; Fredrickson, A.; Sheils, N.E.; Buresh, J.; Cronholm, P.F.; Matone, M. Describing the Health Status of Women Experiencing Violence or Abuse: An Observational Study Using Claims Data. J. Prim. Care Community Health 2022, 13. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, J.; Fang, H.; Wan, Y. Intimate Partner Violence: A Bibliometric Review of Literature. Int. J. Environ. Res. Public Health 2020, 17, 5607. [Google Scholar] [CrossRef]
- Elghossain, T.; Bott, S.; Akik, C.; Obermeyer, C.M. Prevalence of intimate partner violence against women in the Arab world: A systematic review. BMC Int. Health Hum. Rights 2019, 19, 29. [Google Scholar] [CrossRef] [PubMed]
- Duvvury, N.; Callan, A.; Carney, P.; Raghavendra, S. Intimate partner violence: Economic costs and implications for growth and development. In Women’s Voice, Agency, and Participation Research Series; World Bank: Washington, DC, USA, 2013; Available online: https://openknowledge.worldbank.org/handle/10986/16697 (accessed on 15 May 2022).
- Stylianou, A.M. Economic Abuse within Intimate Partner Violence: A Review of the Literature. Violence Vict. 2018, 33, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Keane, T. The criterion a problem revisited: Controversies and challenges in defining and measuring psychological trauma. J. Trauma. Stress 2007, 20, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Ding, C.; Tang, Y.-L.; Wu, S.; Yang, D. Effects of social supports on posttraumatic stress disorder symptoms: Moderating role of perceived safety. Psychol. Trauma Theory Res. Pract. Policy 2014, 6, 724–730. [Google Scholar] [CrossRef]
- Boals, A.; Riggs, S.A.; Kraha, A. Coping with Stressful or Traumatic Events: What Aspects of Trauma Reactions are Associated with Health Outcomes? Stress Health 2012, 29, 156–163. [Google Scholar] [CrossRef]
- Brown, R.C.; Berenz, E.C.; Aggen, S.H.; Gardner, C.O.; Knudsen, G.P.; Reichborn-Kjennerud, T.; Kendler, K.S.; Amstadter, A.B. Trauma exposure and Axis I psychopathology: A cotwin control analysis in Norwegian young adults. Psychol. Trauma Theory Res. Pract. Policy 2014, 6, 652–660. [Google Scholar] [CrossRef] [Green Version]
- Dar, M.A.; Wani, R.A.; Margoob, M.A.; Hussain, A.; Rather, Y.H.; Chandel, R.K.; Malla, A.A. Trauma and traumatic stress: The long-term effects of childhood traumatic stress. Malays. J. Psychiatry Ejournal 2015, 23, 114–123. Available online: http://www.mjpsychiatry.org/index.php/mjp/article/viewFile/327/240 (accessed on 15 May 2022).
- Anderson, K.M.; Renner, L.M.; Danis, F.S. Recovery: Resilience and growth in the aftermath of domestic violence. Violence Women 2012, 18, 1279–1299. [Google Scholar] [CrossRef] [Green Version]
- Olff, M.; Langeland, W.; Gersons, B.P.R. The psychobiology of PTSD: Coping with trauma. Psychoneuroendocrinology 2005, 30, 974–982. [Google Scholar] [CrossRef]
- Wozniak, J.D.; Caudle, H.E.; Harding, K.; Vieselmeyer, J.; Mezulis, A.H. The effect of trauma proximity and ruminative response styles on posttraumatic stress and posttraumatic growth following a university shooting. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 227–234. [Google Scholar] [CrossRef]
- May, C.L.; Wisco, B.E. Defining trauma: How level of exposure and proximity affect risk for posttraumatic stress disorder. Psychol. Trauma Theory Res. Pract. Policy 2016, 8, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Pooley, J.A.; Cohen, L.; O’Connor, M.; Taylor, M. Posttraumatic stress and posttraumatic growth and their relationship to coping and self-efficacy in Northwest Australian cyclone communities. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Sinko, L.; James, R.; Hughesdon, K. Healing After Gender-Based Violence: A Qualitative Metasynthesis Using Meta-Ethnography. Trauma Violence Abus. 2021, 1524838021991305. [Google Scholar] [CrossRef]
- Pico-Alfonso, M.A. Psychological intimate partner violence: The major predictor of posttraumatic stress disorder in abused women. Neurosci. Biobehav. Rev. 2005, 29, 181–193. [Google Scholar] [CrossRef]
- Reisenhofer, S.; Taft, A. Women’s journey to safety—The Transtheoretical model in clinical practice when working with women experiencing Intimate Partner Violence: A scientific review and clinical guidance. Patient Educ. Couns. 2013, 93, 536–548. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Gray, K.A. Leave or Stay? Battered women’s decision after intimate partner violence. J. Interpers. Violence 2008, 23, 1465–1482. [Google Scholar] [CrossRef]
- Carman, M.J.; Kay-Lambkin, F.; Burgman, I. Long-Term Recovery from Intimate Partner Violence: Definitions by Australian Women. J. Fam. Violence 2022, 1–14. [Google Scholar] [CrossRef]
- Calhoun, L.G.; Tedeschi, R.G. The foundations of post-traumatic growth: An expanded framework. In Handbook of Posttraumatic Growth: Research and Practice, 2nd ed.; Calhoun, L.G., Tedeschi, R.G., Eds.; Routledge: London, UK, 2014; pp. 1–23. [Google Scholar]
- Tedeschi, R.G.; Calhoun, L. Posttraumatic growth: A new perspective on psychotraumatology. Psychiatr. Times 2004, 21, 58–60. [Google Scholar]
- Abel, L.; Walker, C.; Samios, C.; Morozow, L. Vicarious posttraumatic growth: Predictors of growth and relationships with adjustment. Traumatology 2014, 20, 9–18. [Google Scholar] [CrossRef]
- Barton, S.; Boals, A.; Knowles, L. Thinking about Trauma: The Unique Contributions of Event Centrality and Posttraumatic Cognitions in Predicting PTSD and Posttraumatic Growth. J. Trauma. Stress 2013, 26, 718–726. [Google Scholar] [CrossRef]
- Coroiu, A.; Körner, A.; Burke, S.; Meterissian, S.; Sabiston, C.M. Stress and posttraumatic growth among survivors of breast cancer: A test of curvilinear effects. Int. J. Stress Manag. 2017, 23, 84–97. [Google Scholar] [CrossRef] [Green Version]
- De Castella, R.; Simmonds, J.G. “There’s a deeper level of meaning as to what suffering’s all about”: Experiences of religious and spiritual growth following trauma. Ment. Health Relig. Cult. 2013, 16, 536–556. [Google Scholar] [CrossRef]
- Jin, Y.; Xu, J.; Liu, H.; Liu, D. Posttraumatic Stress Disorder and Posttraumatic Growth among Adult Survivors of Wenchuan Earthquake After 1 Year: Prevalence and Correlates. Arch. Psychiatr. Nurs. 2014, 28, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Purc-Stephenson, R.J. The Posttraumatic Growth Inventory: Factor structure and invariance among persons with chronic diseases. Rehabil. Psychol. 2014, 59, 10–18. [Google Scholar] [CrossRef]
- Stagg, R. The nadir experience: Crisis, transition, and growth. Transpers. Psychol. Rev. 2014, 46, 72–91. [Google Scholar]
- Su, Y.-J.; Chen, S.-H. Emerging posttraumatic growth: A prospective study with pre- and posttrauma psychological predictors. Psychol. Trauma Theory Res. Pract. Policy 2015, 7, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Taku, K.; Cann, A.; Tedeschi, R.G.; Calhoun, L.G. Core beliefs shaken by an earthquake correlate with posttraumatic growth. Psychol. Trauma Theory Res. Pract. Policy 2015, 7, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Tedeschi, R.G.; Calhoun, L.G. The posttraumatic growth inventory: Measuring the positive legacy of trauma. J. Trauma. Stress 1996, 9, 455–471. [Google Scholar] [CrossRef]
- Gracia, E.; Lila, M.; Santirso, F.A. Attitudes toward Intimate Partner Violence against Women in the European Union: A Systematic Review. Eur. Psychol. 2020, 25, 104–121. [Google Scholar] [CrossRef]
- Nishi, D.; Matsuoka, Y.; Kim, Y. Posttraumatic growth, posttraumatic stress disorder and resilience of motor vehicle accident survivors. Biopsychosoc. Med. 2010, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Han, K.-M.; Park, J.Y.; Park, H.E.; An, S.R.; Lee, E.H.; Yoon, H.-K.; Ko, Y.-H. Social support moderates association between posttraumatic growth and trauma-related psychopathologies among victims of the Sewol Ferry Disaster. Psychiatry Res. 2019, 272, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Salter, E.; Stallard, P. Posttraumatic growth in child survivors of a road traffic accident. J. Trauma. Stress 2004, 17, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, M.; Pfefferbaum, B. Posttraumatic Growth as a Response to Natural Disasters in Children and Adolescents. Curr. Psychiatry Rep. 2018, 20, 37. [Google Scholar] [CrossRef]
- Amiri, H.; Nakhaee, N.; Nagyova, I.; Timkova, V.; Okhovati, M.; Nekoei-Moghadam, M.; Zahedi, R. Posttraumatic growth after earthquake: A systematic review and meta-analysis. Int. J. Soc. Psychiatry 2021, 67, 867–877. [Google Scholar] [CrossRef] [PubMed]
- Sattler, D.N.; Claramita, M.; Muskavage, B. Natural Disasters in Indonesia: Relationships among Posttraumatic Stress, Resource Loss, Depression, Social Support, and Posttraumatic Growth. J. Loss Trauma 2018, 23, 351–365. [Google Scholar] [CrossRef]
- Chan, C.S.; Rhodes, J.E. Religious coping, posttraumatic stress, psychological distress, and posttraumatic growth among female survivors four years after Hurricane Katrina. J. Trauma. Stress 2013, 26, 257–265. [Google Scholar] [CrossRef]
- Zavala, C.; Waters, L.; Arslan, G.; Simpson, A.; del Prado, P.N.; Gargurevich, R. The role of strength-based parenting, posttraumatic stress, and event exposure on posttraumatic growth in flood survivors. Psychol. Trauma Theory Res. Pract. Policy 2022. [Google Scholar] [CrossRef]
- Subandi, M.A.; Achmad, T.; Kurniati, H.; Febri, R. Spirituality, gratitude, hope and post-traumatic growth among the survivors of the 2010 eruption of Mount Merapi in Java, Indonesia. Aust. J. Emerg. Manag. 2014, 18, 19–26. [Google Scholar]
- Pan, Y.; Zhao, H.; Xu, H.; Rn, Y.H.; Dong, C.; Rn, Y.P.; Rn, H.Z.; Rn, H.X.; Rn, C.D.P. Post accidental injury: Mediating roles of emotional expressivity, rumination, and posttraumatic growth. Nurs. Health Sci. 2022, 24, 236–244. [Google Scholar] [CrossRef]
- Lee, D.; Yu, E.-S.; Kim, N.H. Resilience as a mediator in the relationship between posttraumatic stress and posttraumatic growth among adult accident or crime victims: The moderated mediating effect of childhood trauma. Eur. J. Psychotraumatol. 2020, 11, 1704563. [Google Scholar] [CrossRef]
- Mutisya, S.S.; Owuor, B. Counseling as a predictor of posttraumatic growth among the Garissa University terrorist attack survivors. Afr. J. Clin. Psychol. 2018, 1, 1–22. [Google Scholar]
- Tsai, J.; El-Gabalawy, R.; Sledge, W.H.; Southwick, S.M.; Pietrzak, R.H. Post-traumatic growth among veterans in the USA: Results from the National Health and Resilience in Veterans Study. Psychol. Med. 2015, 45, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Veronese, G.; Pepe, A.; Massaiu, I.; De Mol, A.-S.; Robbins, I. Posttraumatic growth is related to subjective well-being of aid workers exposed to cumulative trauma in Palestine. Transcult. Psychiatry 2017, 54, 332–356. [Google Scholar] [CrossRef] [PubMed]
- McLean, C.P.; Handa, S.; Dickstein, B.D.; Benson, T.A.; Baker, M.T.; Isler, W.C.; Peterson, A.L.; Litz, B.T. Posttraumatic growth and posttraumatic stress among military medical personnel. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 62–68. [Google Scholar] [CrossRef]
- Semeijn, J.; Van Ruysseveldt, J.; Vonk, G.; Van Vuuren, T. In flight again with wings that were once broken; effects of post-traumatic growth and personal resources on burnout recovery. Int. J. Work. Health Manag. 2019, 12, 387–403. [Google Scholar] [CrossRef]
- Ulloa, E.; Guzman, M.L.; Salazar, M.; Cala, C. Posttraumatic Growth and Sexual Violence: A Literature Review. J. Aggress. Maltreat. Trauma 2016, 25, 286–304. [Google Scholar] [CrossRef]
- Kılıç, C.; Magruder, K.M.; Koryürek, M.M. Does trauma type relate to posttraumatic growth after war? A pilot study of young Iraqi war survivors living in Turkey. Transcult. Psychiatry 2016, 53, 110–123. [Google Scholar] [CrossRef]
- Yılmaz, G.; Üstün, B.; Günüşen, N.P. Effect of a nurse-led intervention programme on professional quality of life and post-traumatic growth in oncology nurses. Int. J. Nurs. Pr. 2018, 24, e12687. [Google Scholar] [CrossRef]
- Waugh, A.; Kiemle, G.; Slade, P. What aspects of post-traumatic growth are experienced by bereaved parents? A systematic review. Eur. J. Psychotraumatol. 2018, 9, 1506230. [Google Scholar] [CrossRef]
- Kim, M.-G.; Han, S.-W. A Systematic Review and Meta-analysis on the Factors Related to Post-traumatic Growth of Fire Officials. J. Health Informatics Stat. 2020, 45, 373–384. [Google Scholar] [CrossRef]
- Brooks, S.; Amlôt, R.; Rubin, G.J.; Greenberg, N. Psychological resilience and post-traumatic growth in disaster-exposed organisations: Overview of the literature. BMJ Mil Health 2020, 166, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.-S.; Dong, Z.-J.; Wu, X.-Q.; Zhang, L.; Yan, R.-Y.; Ma, J.; Zeng, Y. COVID-19-related post-traumatic growth in the general public: A cross-sectional study from Yunnan, China. Psychol. Health Med. 2022, 27, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Duran, B. Posttraumatic growth as experienced by childhood cancer survivors and their families: A narrative synthesis of qualitative and quantitative research. J. Pediatr. Oncol. Nurs. 2013, 30, 179–197. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.; Lee, Y. The Experience of Posttraumatic Growth for People with Spinal Cord Injury. Qual. Health Res. 2008, 18, 877–890. [Google Scholar] [CrossRef]
- Yang, S.-K.; Ha, Y. Exploring the Relationships between Posttraumatic Growth, Wisdom, and Quality of Life in Older Cancer Survivors. Asian Pac. J. Cancer Prev. 2019, 20, 2667–2672. [Google Scholar] [CrossRef]
- Haroosh, E.; Freedman, S. Posttraumatic growth and recovery from addiction. Eur. J. Psychotraumatol. 2017, 8, 1369832. [Google Scholar] [CrossRef]
- Grace, J.J.; Kinsella, E.L.; Muldoon, O.T.; Fortune, D.G. Post-traumatic growth following acquired brain injury: A systematic review and meta-analysis. Front. Psychol. 2015, 6, 1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askay, S.W.; Magyar-Russell, G. Post-traumatic growth and spirituality in burn recovery. Int. Rev. Psychiatry 2009, 21, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Cui, C.; Wang, K.; An, J.; Jin, C. Current status and influencing factors of post-traumatic growth in maintenance hemodialysis. Int. J. Nurs. Sci. 2017, 4, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Hanetz-Gamliel, K. Associations between the cause of loved one’s death, mourner’s psychological distress and ongoing rela-tionship with the deceased, and mourner’s posttraumatic growth. Omega J. Death Dying 2022, 00302228211068303. [Google Scholar] [CrossRef]
- Chan, K.J.; Young, M.Y.; Sharif, N. Well-being after trauma: A review of posttraumatic growth among refugees. Can. Psychol. Can. 2016, 57, 291–299. [Google Scholar] [CrossRef]
- Baillie, S.E.; Sellwood, W.; Wisely, J.A. Post-traumatic growth in adults following a burn. Burns 2014, 40, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Blackie, L.E.; Hitchcott, N.; Joseph, S. Looking for Post-Traumatic Growth in Perpetrators of the 1994 Genocide in Rwanda: A Discussion of Theoretical and Ethical Issues. J. Perpetrator Res. 2017, 1, 64–84. [Google Scholar] [CrossRef] [Green Version]
- Rahayu, D.; Hamidah, H.; Hendriani, W. Post-traumatic Growth among Domestic Violence Survivors: A Systematic Review. J. Educ. Health Community Psychol. 2019, 8, 138–158. [Google Scholar] [CrossRef] [Green Version]
- Bryngeirsdottir, H.S.; Halldorsdottir, S. The challenging journey from trauma to post-traumatic growth: Lived experiences of facilitating and hindering factors. Scand. J. Caring Sci. 2021. [Google Scholar] [CrossRef]
- Bryngeirsdottir, H.S.; Halldorsdottir, S. “I’m a winner, not a victim”: The facilitating factors of post-traumatic growth among women who have suffered intimate partner violence. Int. J. Environ. Res. Public Health 2022, 19, 1342. [Google Scholar] [CrossRef]
- Bryngeirsdottir, H.S.; Halldorsdottir, S. Fourteen Main Obstacles on the Journey to Post-Traumatic Growth as Experienced by Female Survivors of Intimate Partner Violence: “It Was All So Confusing”. Int. J. Environ. Res. Public Health 2022, 19, 5377. [Google Scholar] [CrossRef]
- Walker, L.O.; Avant, K.C. Strategies for Theory Construction in Nursing, 6th ed.; Pearson: New York, NY, USA, 2019. [Google Scholar]
- American Psychiatric Association. Posttraumatic Stress Disorder. In Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; pp. 271–280. [Google Scholar]
- Marchand, A.; Nadeau, C.; Beaulieu-Prévost, D.; Boyer, R.; Martin, M. Predictors of posttraumatic stress disorder among police officers: A prospective study. Psychol. Trauma Theory Res. Pract. Policy 2015, 7, 212–221. [Google Scholar] [CrossRef]
- Kolassa, I.-T.; Ertl, V.; Eckart, C.; Kolassa, S.; Onyut, L.P.; Elbert, T. Spontaneous remission from PTSD depends on the number of traumatic event types experienced. Psychol. Trauma Theory Res. Pract. Policy 2010, 2, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, B.; Schumacher, S.; Winkel, B.; Imboden, C.; Wittmann, L. The “building block” effect of prior trauma for psychological outcome in victims of a natural disaster. Eur. Psychiatry 2016, 33, S214–S215. [Google Scholar] [CrossRef]
- Li, Y.; Herbell, K.; Bloom, T.; Sharps, P.; Bullock, L.F. Adverse Childhood Experiences and Mental Health among Women Experiencing Intimate Partner Violence. Issues Ment. Health Nurs. 2020, 41, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.G.; Cromer, L.D.; DePrince, A.P.; Freyd, J.J. The role of cumulative trauma, betrayal, and appraisals in understanding trauma symptomatology. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 110–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hing, N.; O’Mullan, C.; Mainey, L.; Nuske, E.; Breen, H.; Taylor, A. Impacts of Male Intimate Partner Violence on Women: A Life Course Perspective. Int. J. Environ. Res. Public Health 2021, 18, 8303. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; Singh, T. Gender-Based Violence during COVID-19 Pandemic: A Mini-Review. Front. Glob. Women’s Health 2020, 1. [Google Scholar] [CrossRef]
- Alcantud, P.M.; Campdepadrós-Cullell, R.; Fuentes-Pumarola, C.; Mut-Montalvà, E. ‘I think I will need help’: A systematic review of who facilitates the recovery from gender-based violence and how they do so. Health Expect. 2021, 24, 1–7. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Step | Description | Overview of What We Did |
|---|---|---|
| Step 1 | The key concepts and key statements from the studies and the databases, used to develop the theory, are specified and explained. | We used our own studies and extensive databases (see Table 2 and Table 3) and analyses of them in the theory synthesis. These contain information about how female survivors of IPV who had reached PTG described their journey to PTG, how they perceived their PTG, and how the lingering effects of their former traumatic experience influenced their PTG. |
| Step 2 | The key concepts and key statements used to develop the theory are compared to the literature, to identify and define their relation to other factors. | The key concepts and key statements identified in step one were used when comparing the main concepts used in the theory to the literature of PTG among female survivors of IPV. Most of the articles from the literature were partially related to the women’s journey to PTG, their experience of PTG, and the lingering effects of their prior traumatic experience in life on their experience of PTG. |
| Step 3 | The key concepts and key statements of the theory and their relations are presented in text, figure(s), or table(s). | After comparing the detailed descriptions of female survivors’ journey to PTG following IPV, their experience of the facilitators and the obstacles on the journey as well as of PTG and the lingering effects of their prior traumatic experience on their PTG. We present the results in text, figures, and tables. |
| Authors and Date | Title | Published |
|---|---|---|
| Bryngeirsdottir and Halldors-dottir, 2021 [92] | The Challenging Journey from Trauma to Post-Traumatic Growth: Experiences of Facilitating and Hindering Factors | Scandinavian Journal of Caring Sciences 00, 1–17 |
| Bryngeirsdottir and Halldors-dottir, 2022 [93] | “I’m a Winner, Not a Victim”: The Facilitating Factors of Post-Traumatic Growth among Women Who Have Suffered Intimate Partner Violence | International Journal of Environmental Research and Public Health 19, 1342. Special Issue: Environment and Behavior |
| Bryngeirsdottir and Halldors-dottir, 2022 [94] | Fourteen Main Obstacles on the Journey to Post-Traumatic Growth as Experienced by Female Survivors of Intimate Partner Violence | International Journal of Environmental Research and Public Health 19, 5377. Special Issue: Violence against Women as an Interdisciplinary Challenge in Public Health |
| Research Data | Number of Interviews | Main Criteria for Participation | Word Count |
|---|---|---|---|
| Qualitative interviews | 13 | Icelandic men and women who self-reported PTG following traumas | 90.172 (M = 6.936) |
| Qualitative interviews | 22 | Icelandic female IPV survivors who self-reported PTG following traumas caused by IPV | 199.386 (M = 9.063) |
| SUMMARY | 35 interviews | 289.558 (M = 8.273) |
| Concepts | Definitions |
|---|---|
| Trauma | An unexpected and threatening event experienced by an individual that he or she cannot stop, control, or influence in any way. Trauma negatively affects the basic experience of living in a safe and predictable world and can even negatively affect the individual’s worldview. |
| Intimate Partner Violence (IPV) | Controlling, dominating and/or violent behaviors in an intimate relationship that causes the victim physical, psychological, sexual, financial, or social harm. |
| Facilitators of PTG | Personal, social and/or systematic constructive components that are likely to be beneficial to the progress of PTG among female survivors of IPV. For example, these may be internal factors of the woman, i.e., personal abilities, mindset, social wellbeing, former experience of trauma; the attitude and reaction of the woman, the perpetrator, children, loved ones, and other people; and environmental factors, i.e., personal social support, systematic social support, and organized supporting resources. |
| Obstacles to PTG | Personal, social, and/or systematic destructive components, which are likely to cause a delay in, or prevent, the progress of PTG among female survivors of IPV. These are, for example, feelings of shame; suicidal thoughts; fragile self-identity; insecurity; feeling alone and isolated; triggers; mixed negative feelings; emotional connection to others; physical and psychological health; personal circumstances and social surroundings; the perpetrator; the children; and law and the institutional social system. |
| Post-Traumatic Growth (PTG) | Following the experience of trauma and through the individual’s internal need for change, the woman has managed to process the suffering caused by the trauma. The personal changes experienced include confronting one’s own feelings more freely, consciously nourishing inner strength, having deeper relations to others, experiencing personal growth, living a more wholesome life, and having deeper self-knowledge as well as a stronger self-image. Furthermore, the individual enjoys increased social activity, positivity, and patience and has feelings of freedom, power, and energy, without any regrets. Moreover, the individual feels like a winner in life, is less stressed, more appreciative of one’s own self, others, and life in general, seeing new possibilities in life, having found a new vision as well as deeper inner peace and wisdom. Even though the negative influences of trauma can be present, the positive factors of post-traumatic growth are dominant. Post-traumatic growth can be likened to a personal resurrection in life following psychological trauma. |
| Lingering Effects of IPV | The negative, long-term effects of traumatic experience are intertwined with one’s PTG. The person becomes aware of these effects, learns to accept them and how to endure them, responding to them in the best and most suitable way, knowing that the effects will pass and/or everything will be all right. |
| Former Traumas as a Child or Young Adult | Negative Results of Former Traumas | Influence of Former Traumas on Reacting to Traumatic Situations | Influences of Former Traumas on IPV |
|---|---|---|---|
| As a child Neglect, poverty, sexual abuse, bullying, witnessing IPV at home, alcohol abuse by parents, illness, or death of a relative, dependent atmosphere at home, parents’ divorce, apathetic and absent parents, demanding parents, stigmatization by community (i.e., because of adverse conditions at home), taking on too much responsibility for their age, difficulties at school. As a young adult Violent relationship, rape, bullying, assault, oppression, threats, property damage, breach of confidentiality, infidelity, divorce, custody dispute, neglect of children, post-partum depression, sickness of loved ones, death of loved ones, financial concerns, accidents, loss of health, codependence, drug abuse by herself or former spouse, alcohol abuse by the survivor or former spouse, bankruptcy. | Fragile self-image, lower feelings of self-worth, shift in personal boundaries, depressed defensive responses, diminished trust in other people, dependence, excessive feeling of responsibility, shame, anxiety, perfectionism, rebelliousness, forbidden to complain, having to succeed no matter what, insecurity, feeling of rejection, grief, suicidal attempts, muscle tension, fear, stress, feeling of guilt, sleep problems, reticence, nervous breakdown. | Destructive reaction to traumas, trouble in processing trauma in a constructive way. Feeling vulnerable or adapted to traumatic situations avoiding confronting the real situations. Snowball-effects of past and current traumas sometimes ending in traumatic breakdown. | Increased danger of being abused, reducing possibilities of leaving violent and life-threatening situations. |
| The Female Survivors’ Lived Experience of IPV: A Summary | |
|---|---|
| Female IPV Survivors | We theorize, based on the aforementioned findings, that being a female victim of IPV can be compared to being held as a hostage in a violent relationship against your will. The woman feels captured and dependent on the perpetrator, where most things are conditional, him deciding what is “right” and what is “wrong”, and her “bad behavior” having serious, unpredictable consequences. The woman often feels like she is being silenced, since her opinion does not matter, her words do not have meaning, her needs are ignored, and her will and reactions to the situation seem not to be relevant. Due to the perpetrator’s gaslighting, as well as his unpredictable mood and behaviour, the woman often becomes exhausted when trying to please the perpetrator. She seems to continuously move and reset her personal boundaries, losing a small piece of her self-identity every time she does so. In the end, her boundaries are likely to be completely shattered; the woman experiences complete vulnerability and hopelessness, and gives up. Often, she cannot choose whom she meets, she cannot confide in anyone, and there is no one left to back her up or defend her. The perpetrator often has full access to her whenever he wants, threatening her and abusing her in the ways he pleases. Even though the woman is likely to be terrified, she cannot expect anyone to come and rescue her since the violent situation is frequently concealed; the woman may feel like she has been sworn to secrecy and that no one can know of the violence. The woman’s physical and psychological health is often systematically threatened as well as her wellbeing. In the end, she is likely to suffer serious health problems if the situation is either long-term or even permanent. |
| Intrapersonal Consequences of IPV | Interpersonal Consequences of IPV |
|---|---|
| Experiences feelings of fear, grief, anger, shame, helplessness, and betrayal. Feeling of not being herself anymore, having been conquered, defeated, and overpowered. Experiences fear of acknowledging the violence. Easily triggered, feels tired, stressed, suicidal, feels like she has lost so much, and feels uncertain about the future. Suffers insomnia due to anxiety and fear, never knows what will happen next, feels insecure, lacks appetite, suffers pain due to physical injuries. Feels like someone is constantly watching her, feels ashamed of letting the relationship go on for so long. Experiences difficulties in performing usual activities of daily life. | Experiences social isolation, has stopped seeing friends, has stopped seeing family, and has stopped communicating with other people. Does not know how to behave, fakes her feelings, fakes her wellbeing, and pretends to be happy. Feels emotionally absent to other people, experiences lack of interest in sex, as well as lack of interest in romantic relationships |
| Main Obstacles | Examples |
|---|---|
| Negative feelings towards own self | Feels ashamed, blames herself, feeling of being less worthy, experiences self-stigmatization, suicidal thoughts, injured self-identity, disrupted body image, insecurity, anger, and loneliness. |
| Triggers | Incidents related to the experience of IPV that negatively affect the woman’s feelings and wellbeing, e.g., sees a car that resembles the perpetrator’s car, reads a column in the paper that diminishes victims of IPV. |
| Conflicting states of mind | Experiences relief vs. regret, strength vs. vulnerability, joy vs. misery, and comfort vs. displeasure. |
| Negative feelings on behalf of their children | Feels sad because of what the children have endured due to the violent relationship. Feels angry because of continuing destructive behavior of the perpetrator towards the children. |
| Problems in connecting to other people | Experiences lack of trust, avoidance of emotional connections, fear of romantic relations and loss of own social standards. Often overreacts to other people’s behaviours, actions, words, mimics, tone of voice and body posture. |
| Health issues | Feels tired, in pain, has trouble sleeping, feels tense, depressed, anxious, endures physical diseases, physical and/or mental breakdown, and burnout. |
| Challenging personal circumstances | Experiences lack of housing, financial problems, loss of working capability, and social isolation. |
| Self-destructive behaviour | Talks to herself in a hostile and hurtful way. Blames herself for her situation. |
| The perpetrator | Continues harassing, stalking, showing threatening, frightening, violent behaviour, financial abuse, and escalating psychological violence. |
| Mixed feelings towards the perpetrator | Has nightmares, experiences flashbacks and fear, finds it hard to let go. Can be obsessed with the man. |
| Negative feelings towards laws, regulations, and the social support system | Feels powerless within ‘the system’, the divorce/separation takes a long time, the division of assets is unfair, the man stays in control, the woman is forced to settle with the perpetrator about their assets and children, she is forced to send the children to the perpetrator against their will, experiences fear of child protection services taking her children away, the perpetrator uses the children to blackmail the woman, while still married to the perpetrator or cohabitated with him, by law, the woman does not receive the support and benefits that she is entitled to as a single mother. |
| Main Facilitators | Examples |
|---|---|
| Personal competence and skills | Positive attitude, personal strength, and resilience. |
| State of mind | Confronting the experience of violence. Rejecting current situation. Deciding to seek help. Setting goals for a better life and PTG. Taking control of own life. Deciding not to be a victim. |
| Social welfare | Safe living conditions. Safe place to live. Financial security. Professional support. |
| Previous experience of trauma | Earlier experiences of processing trauma, resulting in increased inner strength |
| Self-perspective | Chooses where to seek help. Has self-compassion. Gives herself the time needed. Treats herself right |
| Perspective to loved ones and other people | Considers behaviour towards others and the behaviour from others. Encourages good relations. Sets boundaries. |
| Perspective to the perpetrator | Sets boundaries. Prevents him from being in control. |
| Various personal support | Informal support. Systematic support. Organized resources. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bryngeirsdottir, H.S.; Arnault, D.S.; Halldorsdottir, S. The Post-Traumatic Growth Journey of Women Who Have Survived Intimate Partner Violence: A Synthesized Theory Emphasizing Obstacles and Facilitating Factors. Int. J. Environ. Res. Public Health 2022, 19, 8653. https://doi.org/10.3390/ijerph19148653
Bryngeirsdottir HS, Arnault DS, Halldorsdottir S. The Post-Traumatic Growth Journey of Women Who Have Survived Intimate Partner Violence: A Synthesized Theory Emphasizing Obstacles and Facilitating Factors. International Journal of Environmental Research and Public Health. 2022; 19(14):8653. https://doi.org/10.3390/ijerph19148653
Chicago/Turabian StyleBryngeirsdottir, Hulda S., Denise Saint Arnault, and Sigridur Halldorsdottir. 2022. "The Post-Traumatic Growth Journey of Women Who Have Survived Intimate Partner Violence: A Synthesized Theory Emphasizing Obstacles and Facilitating Factors" International Journal of Environmental Research and Public Health 19, no. 14: 8653. https://doi.org/10.3390/ijerph19148653