
A Portable Real-Time Ringdown Breath Acetone Analyzer: Toward Potential Diabetic Screening and Management

 ,
,
Abstract
:1. Introduction
2. Experimental
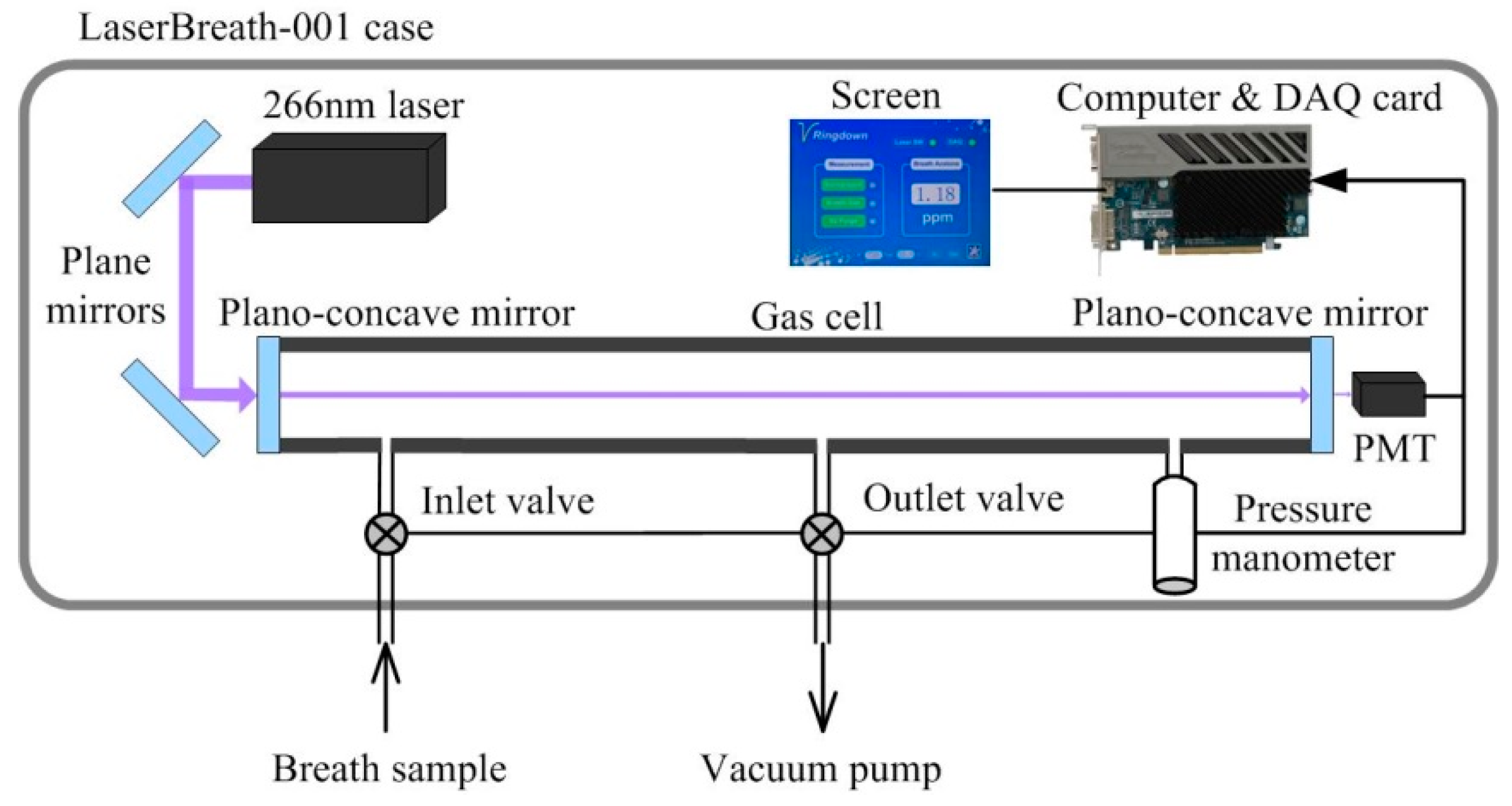
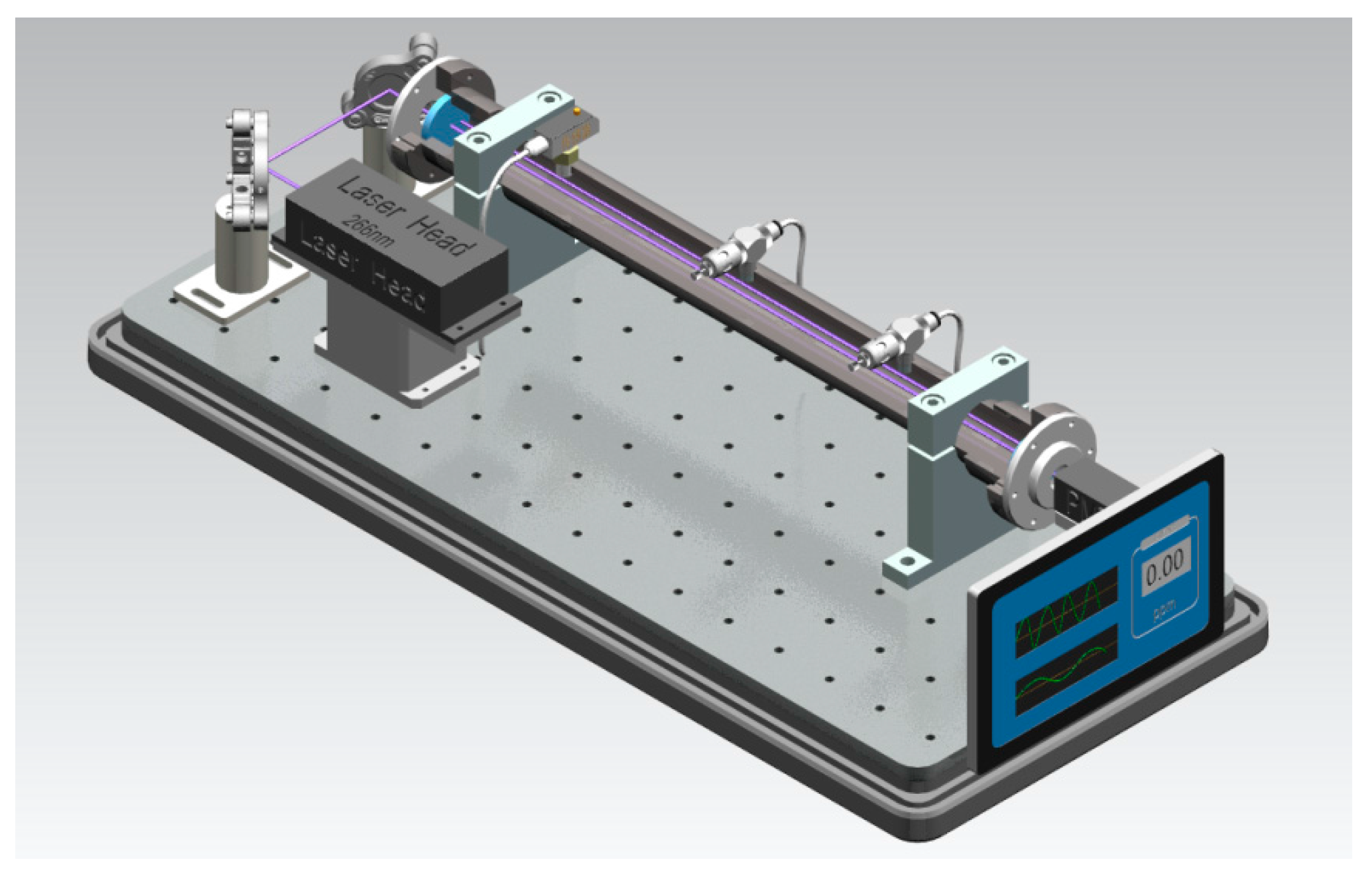
2.1. Ringdown Breath Acetone Analyzer
2.2. Measuring Method
2.3. Breath Analysis Volunteers and Patients
3. Results and Discussion
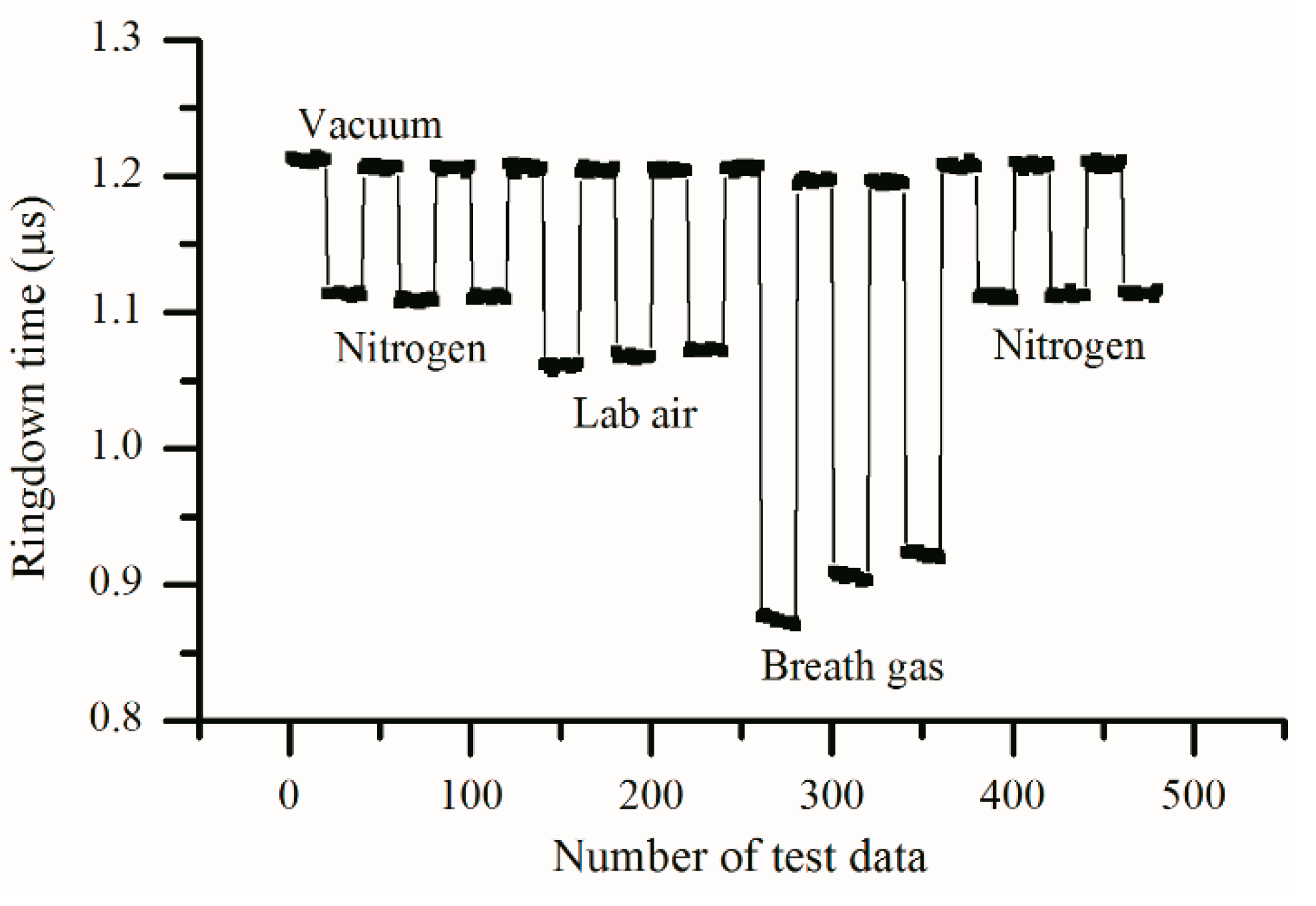
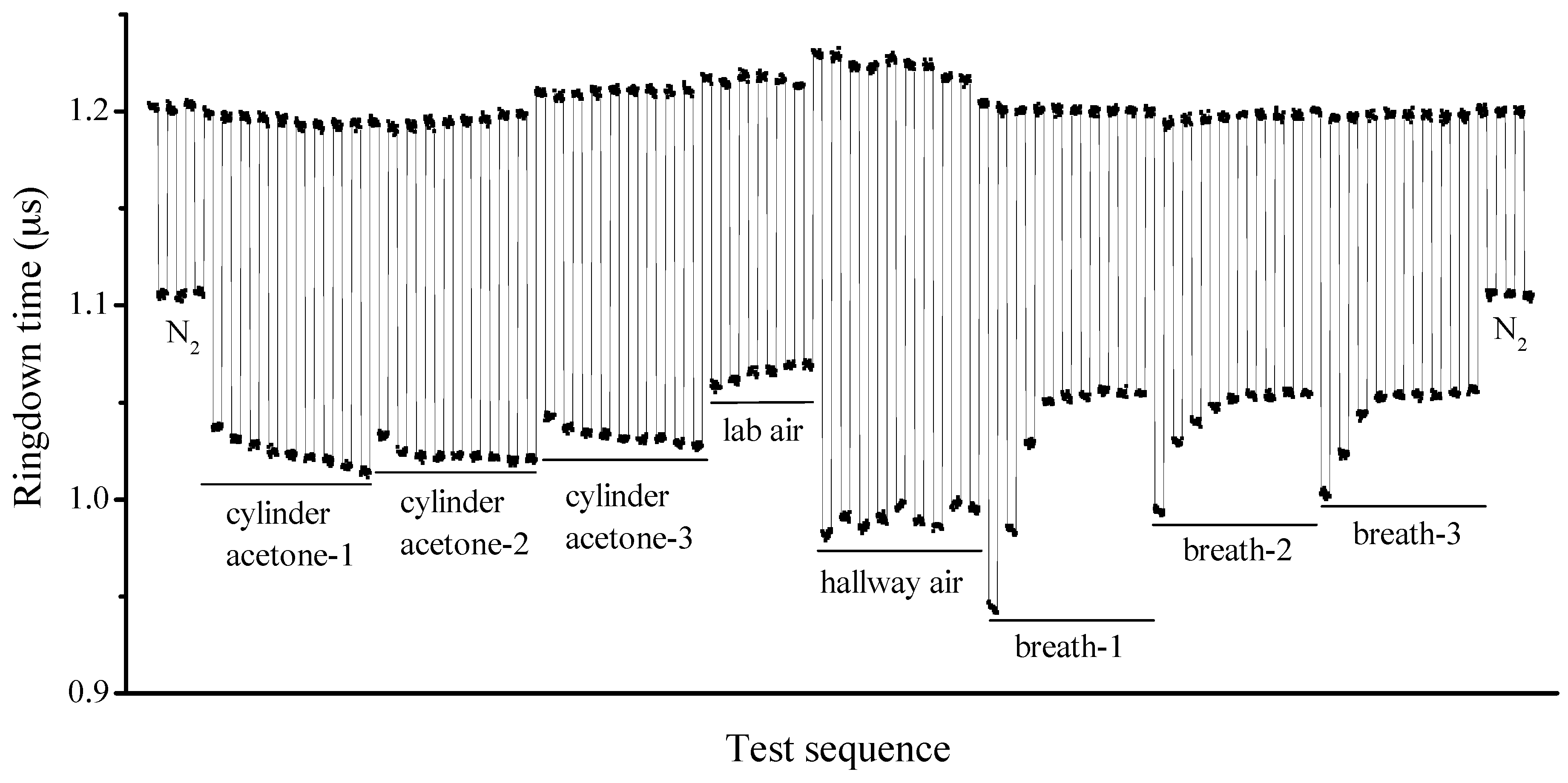
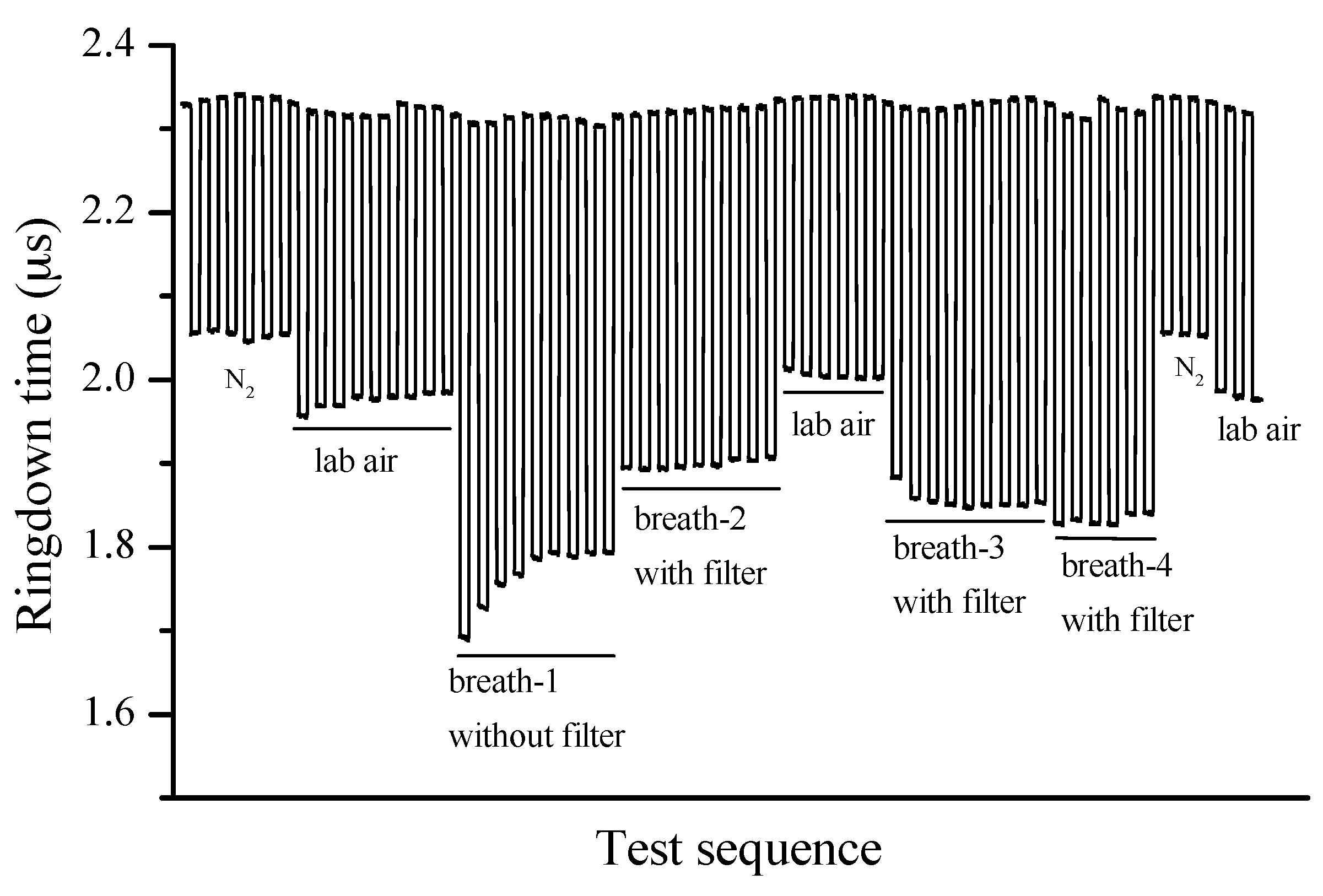
3.1. Performance of the Instrument
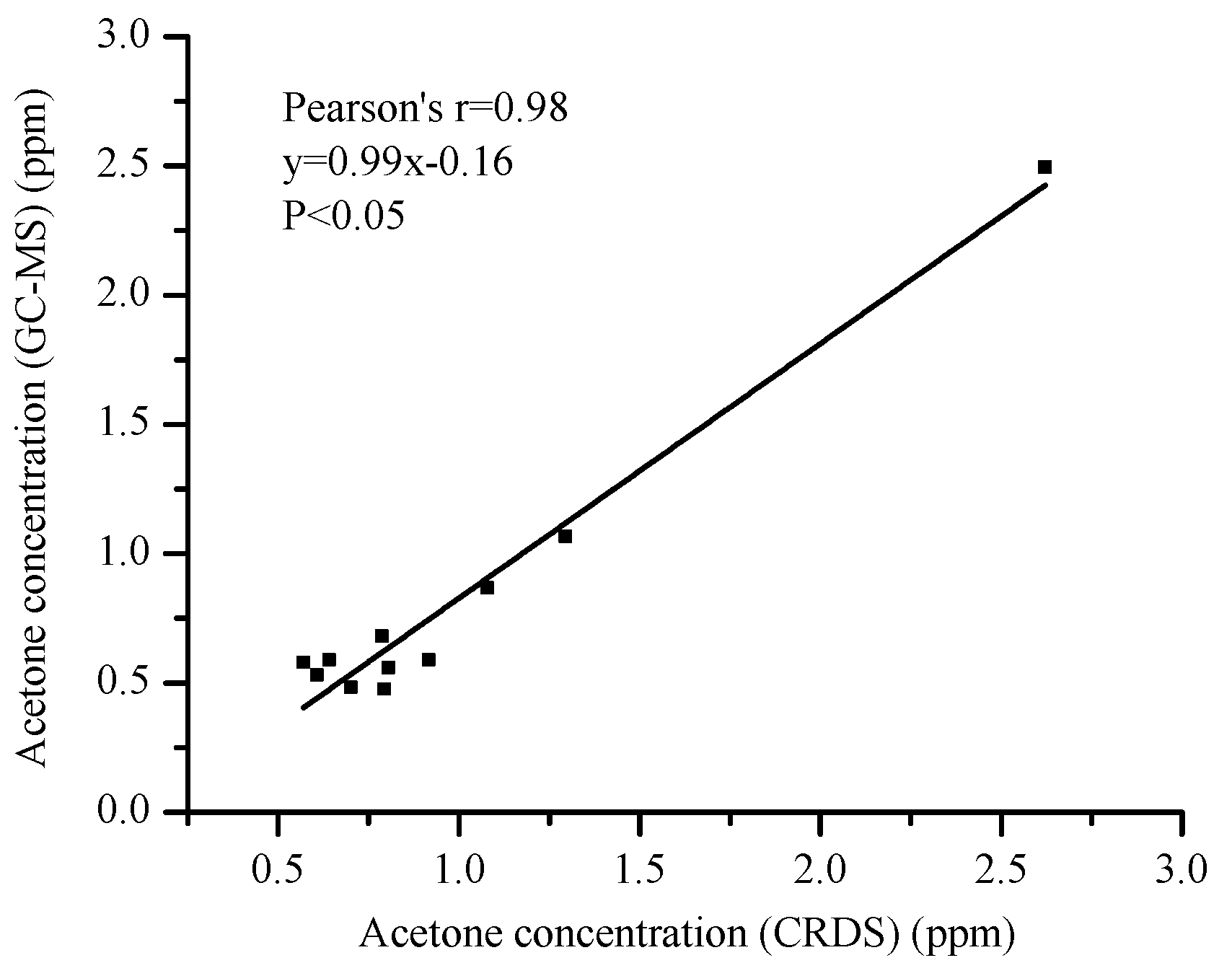
3.2. Comparison of Acetone Values from CRDS to GC-MS Values
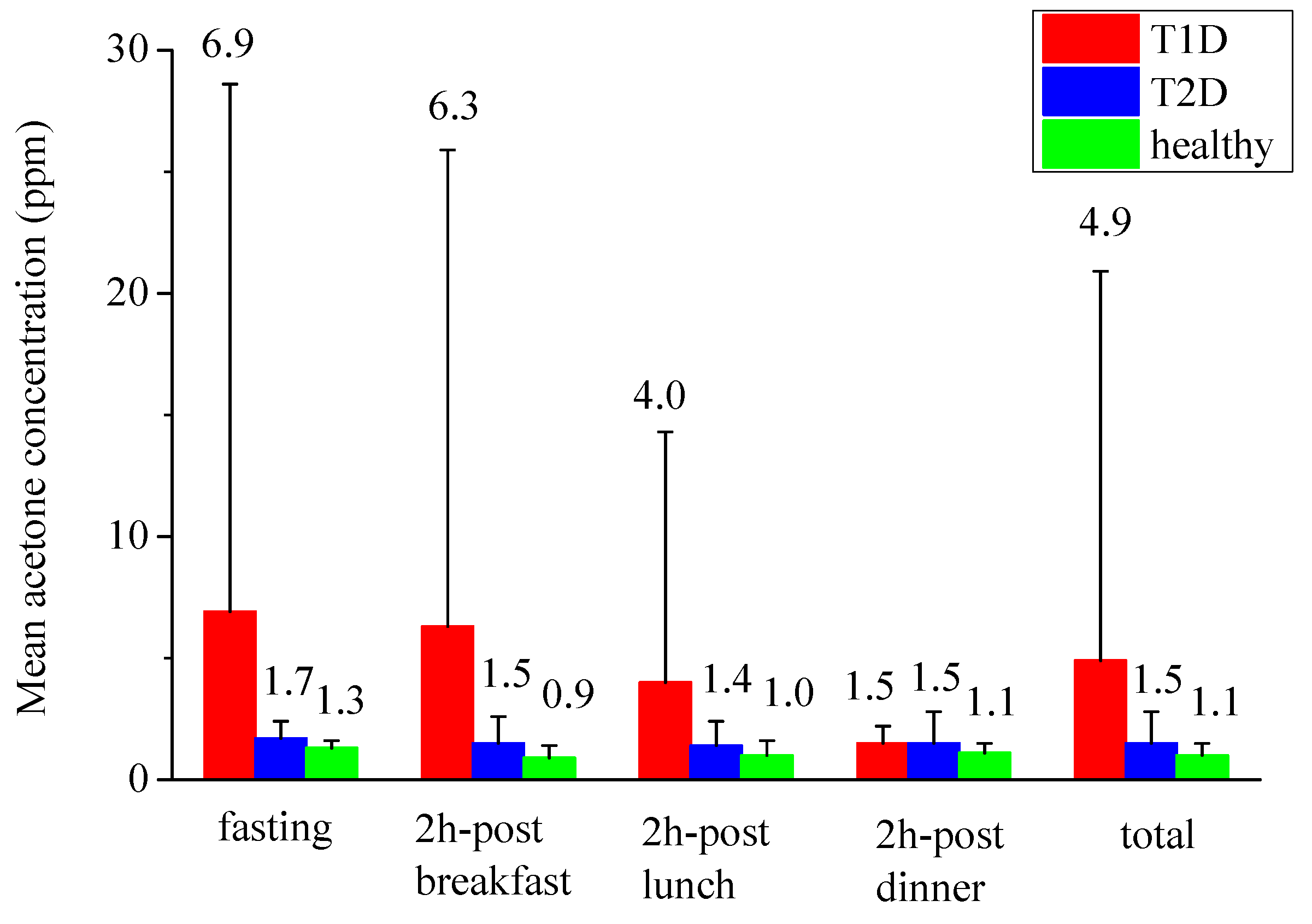
3.3. Breath Tests in Human Subjects Using the Validated Breath Acetone Analyzer
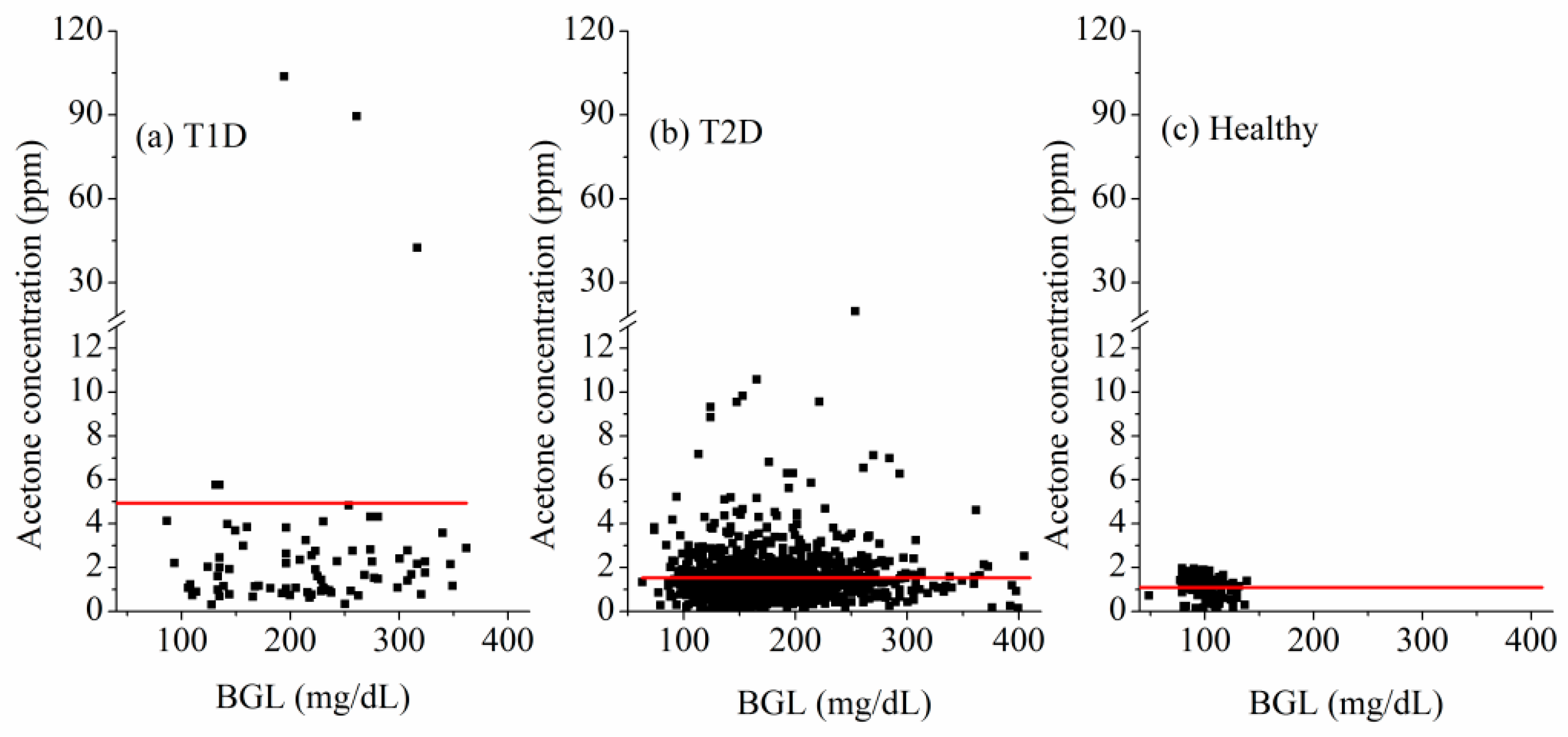
3.4. Toward Diabetes Screening and Management
4. Summary
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jansson, B.O.; Larsson, B.T.J. Analysis of organic compounds in human breath by gas chromatography-mass spectrometry lab. Clin. Med. 1969, 74, 961–966. [Google Scholar]
- Pauling, L.; Robinson, A.B.; Cary, P. Quantitative analysis of urine vapor and breath by gas-liquid partition chromatography. Proc. Natl. Acad. Sci. USA 1971, 68, 2374–2376. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.M.; Szidon, J.P.; Krotoszynski, B.K.; Gibbons, R.D.; O’Neill, H.J. Volatile organic compounds in exhaled air from patients with lung cancer. Clin. Chem. 1985, 31, 1278–1282. [Google Scholar] [PubMed]
- Risby, T.H.; Solga, S.F. Current status of clinicalbreath analysis. Appl. Phys. B 2006, 85, 421–426. [Google Scholar] [CrossRef]
- Mürtz, M. Breath diagnostics using laser spectroscopy. Opt. Photonics News 2005, 16, 30–35. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, C. Is breath acetone a biomarker of diabetes—A historical review on breath acetone measurements. J. Breath Res. 2013, 7. [Google Scholar] [CrossRef] [PubMed]
- Rooth, G.; Ostenson, S. Acetone in alveolar air, and the control of diabetes. Lancet 1966, 288, 1102–1105. [Google Scholar] [CrossRef]
- Nelson, N.; Lagesson, V.; Nosratabadi, A.; Ludvigsson, J.; Tagesson, C. Exhaled isoprene and acetone in newborn infants and in children with diabetes mellitus. Pediatr. Res. 1998, 44, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Diskin, A.M.; Španěl, P.; Smith, D. Time variation of ammonia, acetone, isoprene and ethanol in breath: A quantitative SIFT-MS study over 30 days. Physiol. Meas. 2003, 24, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Spaněl, P.; Fryer, A.A.; Hanna, F.; Ferns, G.A. Can volatile compounds in exhaled breathbe used to monitor control in diabetes mellitus? J. Breath Res. 2011, 5. [Google Scholar] [CrossRef] [PubMed]
- Turner, C.; Španěl, P.; Smith, D. A longitudinal study of ammonia, acetone and propanol in the exhaled breath of 30 subjects using selected ion flow tube mass spectrometry, SIFT-MS. Physiol. Meas. 2006, 27, 321–337. [Google Scholar] [CrossRef] [PubMed]
- Teshima, N.; Li, J.; Toda, K.; Dasgupta, P.K. Determination of acetone in breath. Anal. Chim. Acta 2005, 535, 189–229. [Google Scholar] [CrossRef]
- Anderson, J.C.; Lamm, W.J.; Hlastala, M.P. Measuring airway exchange of endogenous acetone using a single-exhalation breathing maneuver. J. Appl. Physiol. 2006, 100, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Natale, C.D.; Paolesse, R.; Martinelli, E.; Capuano, R. Solid-state gas sensors for breath analysis: A review. Anal. Chim. Acta 2014, 824, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Reyes, A.; Horsten, R.C.; Urbach, H.P.; Bhattacharya, N. Study of the exhaled acetone in type 1 diabetes using quantum cascade laser spectroscopy. Anal. Chem. 2015, 87, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.C. Measuing breath acetone for minitoring fat loss: Review. Obesity 2015, 23, 2327–2334. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liu, Y.; Lu, X.; Huang, Y.; Liu, Y.; Cheng, S.; Duan, Y. A cross-sectional study of breath acetone based on diabetic metabolic disorders. J. Breath Res. 2015, 9. [Google Scholar] [CrossRef] [PubMed]
- Nording, M.L.; Yang, J.; Hegedus, C.M.; Bhushan, A.; Kenyon, N.J.; Davis, C.E.; Hammock, B.D. Endogenouslevels of five fatty acid metabolites in exhaled breath condensate to monitor asthma by high-performance liquid chromatography: Electrospray tandem mass spectrometry. IEEE Sens. J. 2010, 10, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Ulanowska, A.; Trawinska, E.; Sawrycki, P.; Buszewski, B. Chemotherapy control by breath profile with application of SPME-GC/MS method. J. Sep. Sci. 2012, 35, 2908–2913. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Mester, Z.; Lord, H.; Pawliszyn, J. Automated in-tube solid phase micro extraction coupled with liquid chromatography-electrospray ionization mass spectrometry for the determination of selected benzodiazepines. J. Anal. Toxicol. 2000, 24, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Wang, T.; Španěl, P. On-line, simultaneous quantification of ethanol, some metabolites and water vapour in breath following the ingestion of alcohol. Physiol. Meas. 2002, 23, 477–479. [Google Scholar] [CrossRef] [PubMed]
- Harrison, G.R.; Critchley, A.D.; Mayhew, C.A.; Thompson, J.M. Real-time breath monitoring of propane and its volatile metabolites during surgery using a novel mass spectrometric technique: A feasibility study. Br. J. Anaesth. 2003, 91, 797–799. [Google Scholar] [CrossRef] [PubMed]
- Moser, B.; Bodrogi, F.; Eibl, G.; Lechner, M.; Rieder, J.; Lirk, P. Mass spectrometric profile of exhaled breath-field study by PTR-MS. Respir. Physiol. Neurobiol. 2005, 145, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Ruzsanyi, V.; Baumbach, J.; Litterst, P.; Westhoff, M.; Freitag, L. Detection of human metabolites using multi-capillary columns coupled to ion mobility spectrometers. J. Chromatogr. A 2005, 1084, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Allafchian, A.R.; Majidian, Z.; Lelbeigi, V.; Tabrizchi, M. A novel method for the determination of three volatile organic compounds in exhaled breath by solid-phase microextraction-ion mobility spectrometry. Anal. Bioanal. Chem. 2016, 408, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Španěl, P. Selected ion flow tube mass spectrometry (SIFT-MS) for on-line trace gas analysis. Mass Spectrom. Rev. 2005, 24, 661–700. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Hou, C.; Huo, D.; Luo, X.; Bao, M.; Li, X.; Yang, M.; Fa, H. A novel device based on a fluorescent cross-responsive sensor array for detecting lung cancer related volatile organic compounds. Rev. Sci. Instrum. 2015, 86. [Google Scholar] [CrossRef] [PubMed]
- Tisch, U.; Haick, H. Chemical sensors for breath gas analysis: The latest developments at the breath analysis summit 2013. J. Breath Res. 2014, 8. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Sahay, P. Breath analysis using laser spectroscopy techniques: Breath biomarkers, spectral fingerprints, and detection limits. Sensors 2009, 9, 8230–8262. [Google Scholar] [CrossRef] [PubMed]
- Wang, C. Biomedical applications of cavity ringdown spectroscopy: Present and perspective. In Proceedings of the 57th Southeast/61st Southwest Joint Regional Meeting of the American Chemical Society, Memphis, TN, USA, 1–4 November 2005.
- O’keefe, A.; Deacon, D.A. Cavity ring-down optical spectrometer for absorption measurements using pulsed laser sources. Rev. Sci. Instrum. 1988, 59, 2544–2551. [Google Scholar] [CrossRef]
- Berden, G.; Peeters, R.; Meijer, G. Cavity ring-down spectroscopy: Experimental schemes and applications. Int. Rev. Phys. Chem. 2000, 22, 565–607. [Google Scholar] [CrossRef]
- Wang, C.; Srivastava, N.; Jones, B.A.; Reese, R.B. A novel multiple species ringdown spectrometer for in situ measurements of methane, carbon dioxide, and carbon isotope. Appl. Phys. B 2008, 92, 259–270. [Google Scholar] [CrossRef]
- Berden, G.; Engeln, R. Cavity Ring-Down Spectroscopy: Techniques and Applications; Wiley-Blackwell: Chichester, UK, 2009. [Google Scholar]
- Wang, C.; Mbi, A.; Shepherd, M. A study on breath acetone in diabetic patients using a cavity ringdown breath analyzer: Exploring correlations of breath acetone with blood glucose and glycohemoglobin A1C. IEEE Sens. J. 2010, 10, 54–63. [Google Scholar] [CrossRef]
- Ciaffoni, L.; Hancock, G.; Harrison, J.J.; van Helden, J.-P.H.; Langley, C.E.; Peverall, R.; Ritchie, G.A.D.; Wood, S. Demonstration of a mid-infrared cavity enhanced absorption spectrometer for breath acetone detection. Anal. Chem. 2013, 85, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Surampudi, A.B. An acetone breath analyzer using cavity ringdown spectroscopy: An initial test with human subjects under various situations. Meas. Sci. Technol. 2008, 22. [Google Scholar] [CrossRef]
- Wang, C.; Mbi, A. A new acetone detection device using cavity ringdown spectroscopy at 266 nm: Evaluation of the instrument performance using acetone sample solutions. Meas. Sci. Technol. 2007, 18, 2731–2741. [Google Scholar] [CrossRef]
- Sun, M.; Chen, Z.; Gong, Z.; Zhao, X.; Jiang, C.; Yuan, Y.; Wang, Z.; Li, Y.; Wang, C. Determination of breath acetone in 149 type 2 diabetic patients using a ringdown breath-acetone analyzer. Anal. Bioanal. Chem. 2015, 407, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, C.; Lathan, P. Breath acetone analysis of diabetic dogs using a cavity ringdown breath analyzer. IEEE Sens. J. 2013, 14, 1117–1123. [Google Scholar] [CrossRef]
- Sun, M.; Zhao, X.; Yin, H.; Wang, Z.; Jiang, C.; Liu, W.; Chen, Z.; Yuan, Y.; Li, Y.; Wang, C. Study of breath acetone and its correlations with blood glucose and blood beta-hydroxybutyrate using an animal model with lab-developed type 1 diabetic rat. RSC Adv. 2015, 5, 71002–71010. [Google Scholar] [CrossRef]
- Sahay, P.; Scherrer, S.; Wang, C. Measurements of the weak UV absorptions of isoprene and acetone at 261–275 nm using cavity ringdown spectroscopy for evaluation of a potential portable ringdown breath analyzer. Sensors 2013, 13, 8170–8187. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Sun, M.; Jiang, C.; Wang, Z.; Kang, M.; Li, Y.; Wang, C. A ringdown breath acetone analyzer: Performance and validation using gas chromatography-mass spectrometry. J. Anal. Bioanal. Tech. 2014, S7. [Google Scholar] [CrossRef]
- Yeaw, J.; Lee, W.C.; Aagren, M.M.; Christensen, T. Cost of self-monitoring of blood glucose in the United States among patients on an insulin regimen for diabetes. J. Manag. Care Pharm. 2012, 18, 21–32. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject Number | T1D (n = 22) | T2D (n = 312) | Healthy (n = 52) | |
|---|---|---|---|---|
| Sample Number Per Subject | ||||
| 1 | 2 | 57 | 9 | |
| 2 | 2 | 4 | 4 | |
| 3 | 2 | 56 | 5 | |
| 4 | 16 | 195 | 34 | |
| Total number of samples | 76 | 1013 | 168 | |
| Factor | T1D (n = 22) | T2D (n = 312) | Healthy (n = 52) | p Value | |
|---|---|---|---|---|---|
| Age | 28.1 ± 13.4 (13.0~61.0) | 57.0 ± 12.9 (14.0~83.0) | 27.0 ± 4.8 (20.0~48.0) | <0.0001 | |
| Gender | male | 8 (34.8%) | 178 (57.1%) | 22 (42.3%) | 0.931 |
| female | 14 (65.2%) | 134 (42.9%) | 30 (57.7%) | ||
| Years (year) | 5.5 ± 7.4 (0.1~23.0) | 11.7 ± 8.0 (0.0~36.0) | — | — | |
| Weight (kg) | 54.8 ± 6.3 (46.0~69.0) | 72.8 ± 14.0 (44.0~117.0) | 62.2 ± 11.4 (46.0~91.0) | <0.0001 | |
| Height (cm) | 163.1 ± 5.4 (156.0~171.0) | 165.3 ± 8.6 (144.0~186.0) | 167.5 ± 8.0 (153.0~183.0) | 0.1 | |
| BMI (kg/m2) | 20.6 ± 2.5 (18.4~27.2) | 26.5 ± 3.8 (17.9~38.2) | 22.1 ± 3.1 (17.1~33.9) | <0.0001 | |
| Acetone (ppm) | Fasting (n1 = 22, n2 = 312, n3 = 52) | 6.9 ± 21.7 (0.7~103.7) | 1.7 ± 0.7 (0.1~19.8) | 1.3 ± 0.3 (0.3~1.9) | 0.3 |
| 2h post-breakfast (n1 = 20, n2 = 255, n3 = 40) | 6.3 ± 19.6 (0.7~89.5) | 1.5 ± 1.1 (0.1~7.1) | 0.9 ± 0.5 (0.1~2.0) | <0.05 | |
| 2h post-lunch (n1 = 16, n2 = 195, n3 = 41) | 4.0 ± 10.3 (0.3~42.5) | 1.4 ± 1.0 (0.1~7.2) | 1.0 ± 0.6 (0.1~2.0) | 0.4 | |
| 2h post-dinner (n1 = 18, n2 = 251, n3 = 35) | 1.5 ± 0.7 (0.6~2.9) | 1.5 ± 1.3 (0.1~10.6) | 1.1 ± 0.4 (0.3~1.4) | 0.2 | |
| Total (n1 = 76, n2 = 1013, n3 = 168) | 4.9 ± 16 (0.3~103.7) | 1.5 ± 1.3 (0.1~19.8) | 1.1 ± 0.5 (0.1~2.0) | <0.01 | |
| BGL (mg/dL) | Fasting (n1 = 22, n2 = 312, n3 = 38) | 203.3 ± 53.9 (86.4~324.0) | 152.1 ± 41.0 (63.0~304.2) | 91.8 ± 7.3 (79.2~108.0) | <0.0001 |
| 2h post-breakfast (n1 = 20, n2 = 255, n3 = 35) | 252.9 ± 70.4 (124.2~433.8) | 206.5 ± 59.8 (73.8~392.4) | 96.8 ± 13.6 (48.6~124.2) | <0.0001 | |
| 2h post-lunch (n1 = 16, n2 = 195, n3 = 32) | 207.9 ± 70.4 (106.2~324.0) | 189.0 ± 57.2 (73.8~405.0) | 105.3 ± 14.0 (79.2~131.4) | <0.0001 | |
| 2h post-dinner (n1 = 18, n2 = 251, n3 = 34) | 235.6 ± 93.3 (93.6~394.2) | 181.4 ± 52.3 (90.0~397.8) | 118.3 ± 12.4 (100.8~138.6) | <0.0001 | |
| Total (n1 = 76, n2 = 1013, n3 = 168) | 224.6 ± 74.7 (86.4~433.8) | 180.6 ± 56.2 (63.0~405.0) | 100.0 ± 14.5 (48.6~138.6) | <0.0001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, C.; Sun, M.; Wang, Z.; Chen, Z.; Zhao, X.; Yuan, Y.; Li, Y.; Wang, C. A Portable Real-Time Ringdown Breath Acetone Analyzer: Toward Potential Diabetic Screening and Management. Sensors 2016, 16, 1199. https://doi.org/10.3390/s16081199
Jiang C, Sun M, Wang Z, Chen Z, Zhao X, Yuan Y, Li Y, Wang C. A Portable Real-Time Ringdown Breath Acetone Analyzer: Toward Potential Diabetic Screening and Management. Sensors. 2016; 16(8):1199. https://doi.org/10.3390/s16081199
Chicago/Turabian StyleJiang, Chenyu, Meixiu Sun, Zhennan Wang, Zhuying Chen, Xiaomeng Zhao, Yuan Yuan, Yingxin Li, and Chuji Wang. 2016. "A Portable Real-Time Ringdown Breath Acetone Analyzer: Toward Potential Diabetic Screening and Management" Sensors 16, no. 8: 1199. https://doi.org/10.3390/s16081199