
Repetitive Negative Thinking and Eating Disorders: A Meta-Analysis of the Role of Worry and Rumination

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.1.1. Eligible Studies Included
2.1.2. Information Sources and Search
2.1.3. Study Selection, Data Collection Process and Data Items
2.1.4. Assessment of Risk of Bias in Individual Studies
2.2. Quality Assessment
2.3. Data Analyses
3. Results
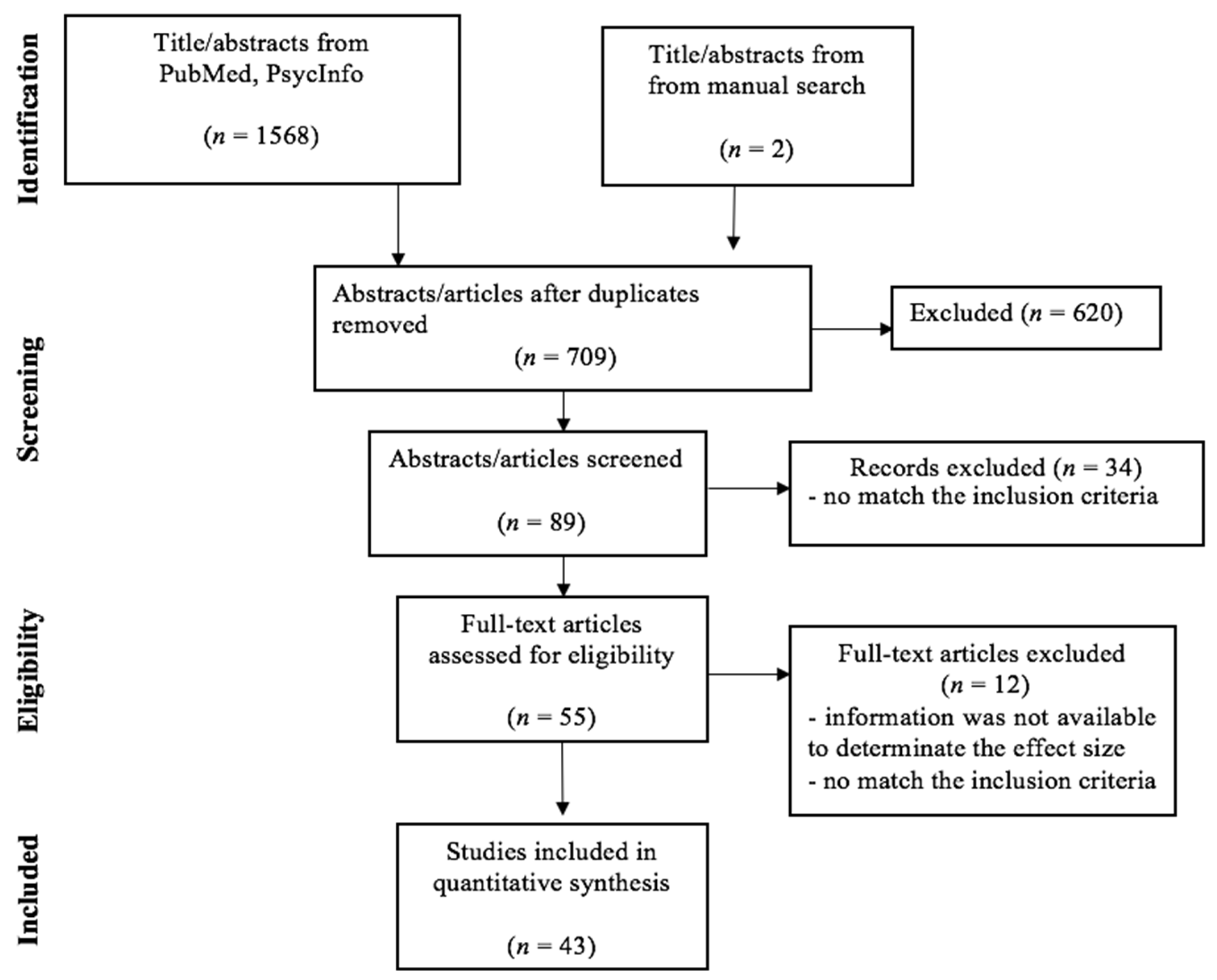
3.1. Study Selection
3.2. Study Quality
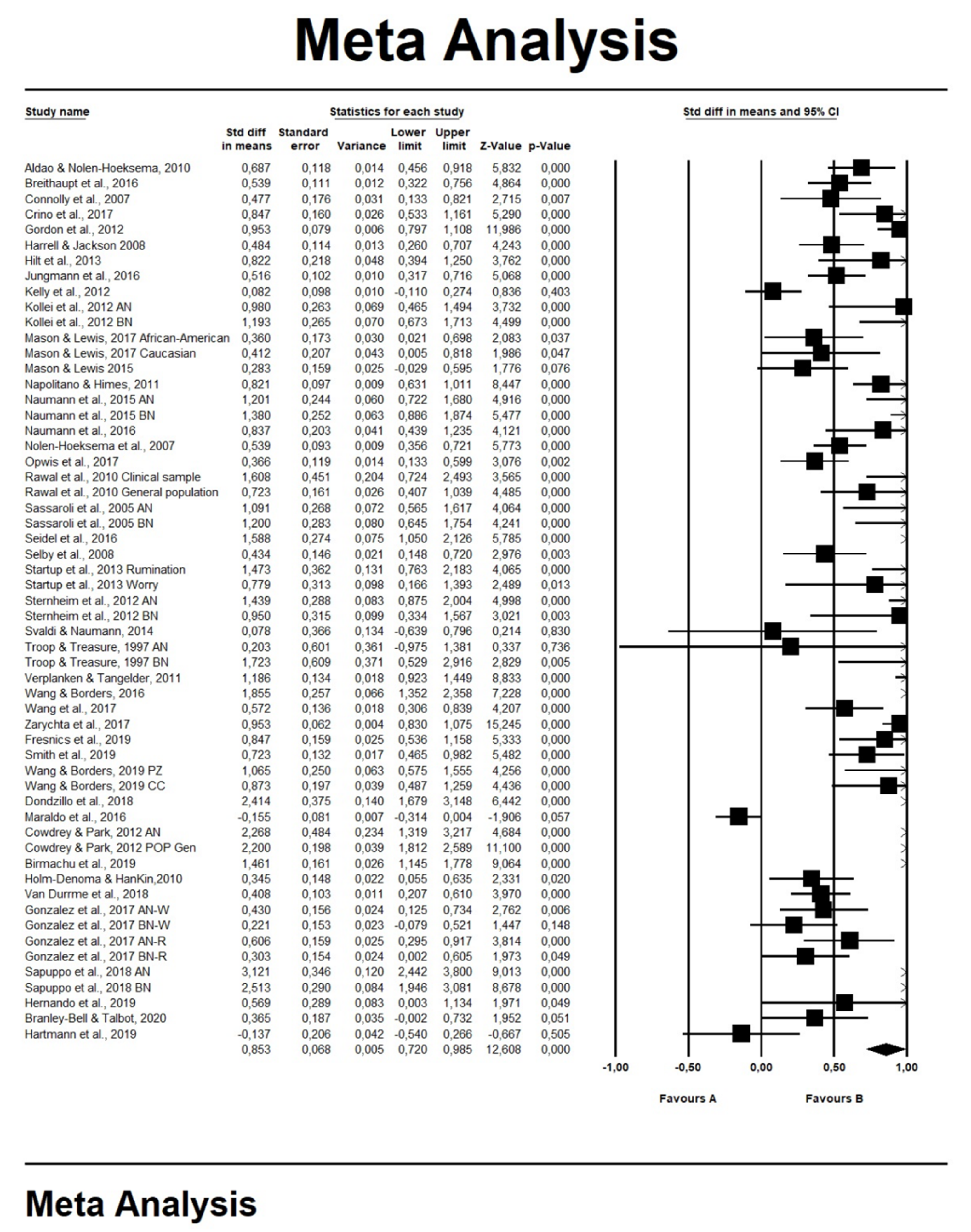
3.3. RT and Eating Problems
Moderator Analyses: Subtypes of ED Symptoms, Presence vs. Absence of Diagnosis of EDs, Worry–Rumination and Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Segerstrom, S.C.; Stanton, A.L.; Alden, L.E.; Shortridge, B.E. A Multidimensional Structure for Repetitive Thought: What’s on Your Mind, and How, and How Much? J. Pers. Soc. Psychol. 2003, 85, 909. [Google Scholar] [CrossRef]
- Ehring, T.; Watkins, E.R. Repetitive Negative Thinking as a Transdiagnostic Process. Int. J. Cogn. Ther. 2008, 1, 192–205. [Google Scholar] [CrossRef]
- Watkins, E.R. Constructive and unconstructive repetitive thought. Psychol. Bull. 2008, 134, 163–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borkovec, T.; Robinson, E.; Pruzinsky, T.; DePree, J.A. Preliminary exploration of worry: Some characteristics and processes. Behav. Res. Ther. 1983, 21, 9–16. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Morrow, J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The Lorma Prieta earthquake. J. Pers. Soc. Psychol. 1991, 65, 115–121. [Google Scholar] [CrossRef]
- Papageorgiou, C. Worry and rumination: Styles of persistent negative thinking in anxiety and depression. In Worry and Its Psychological Disorder; Davey, G.C.L., Wells, A., Eds.; John Wiley: Chichester, UK, 2006; pp. 21–40. [Google Scholar]
- Watkins, E. Appraisals and strategies associated with rumination and worry. Pers. Individ. Differ. 2004, 37, 679–694. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Naragon-Gainey, K.; Wolitzky-Taylor, K.B. Specificity of Rumination in Anxiety and Depression: A Multimodal Meta-Analysis. Clin. Psychol. 2013, 20, 225–257. [Google Scholar] [CrossRef]
- Chorpita, B.F.; Tracey, S.A.; Brown, T.A.; Collica, T.J.; Barlow, D.H. Assessment of worry in children and adolescents: An adaptation of the Penn State Worry Questionnaire. Behav. Res. Ther. 1997, 35, 569–581. [Google Scholar] [CrossRef]
- Muris, P.; Meesters, C.; Merckelbach, H.; Sermon, A.; Zwakhalen, S. Worry in Normal Children. J. Am. Acad. Child Psychiatry 1998, 37, 703–710. [Google Scholar] [CrossRef]
- Perrin, S.; Last, C.G. Worrisome thoughts in children referred for anxiety disorder. J. Clin. Child Adolesc. Psychol. 1997, 26, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Wells, A. Metacognitive Therapy for Anxiety and Depression; The Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Andrews, V.H.; Borkovec, T. The differential effects of inductions of worry, somatic anxiety, and depression on emotional experience. J. Behav. Ther. Exp. Psychiatry 1988, 19, 21–26. [Google Scholar] [CrossRef]
- Chelminski, I.; Zimmerman, M. Pathological worry in depressed and anxious patients. J. Anxiety Disord. 2003, 17, 533–546. [Google Scholar] [CrossRef]
- Starcevic, V. Pathological worry in major depression: A preliminary report. Behav. Res. Ther. 1995, 33, 55–56. [Google Scholar] [CrossRef]
- Calmes, C.A.; Roberts, J.E. Repetitive Thought and Emotional Distress: Rumination and Worry as Prospective Predictors of Depressive and Anxious Symptomatology. Cogn. Ther. Res. 2007, 31, 343–356. [Google Scholar] [CrossRef]
- Clark, D.M.; Wells, A. A cognitive model of social phobia. In Social Phobia: Diagnosis, Assessment and Treatment; Heimberg, R., Liebowitz, M., Hope, D.A., Schneier, F.R., Eds.; Guilford Press: New York, NY, USA, 1995. [Google Scholar]
- Fresco, D.M.; Frankel, A.N.; Mennin, D.S.; Turk, C.L.; Heimberg, R.G. Distinct and Overlapping Features of Rumination and Worry: The Relationship of Cognitive Production to Negative Affective States. Cogn. Ther. Res. 2002, 26, 179–188. [Google Scholar] [CrossRef]
- Harrington, J.A.; Blankenship, V. Ruminative Thoughts and Their Relation to Depression and Anxiety. J. Appl. Soc. Psychol. 2002, 32, 465–485. [Google Scholar] [CrossRef]
- Kashdan, T.B.; Roberts, J.E. Social anxiety, depressive symptoms, and post-event rumination: Affective consequences and social contextual influences. J. Anxiety Disord. 2007, 21, 284–301. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; Nolen-Hoeksema, S. Rumination as a transdiagnostic factor in depression and anxiety. Behav. Res. Ther. 2011, 49, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Mellings, T.M.; Alden, L.E. Cognitive processes in social anxiety: The effects of self-focus, rumination and anticipatory processing. Behav. Res. Ther. 2000, 38, 243–257. [Google Scholar] [CrossRef]
- de Silveira, M.É., Jr.; Kauer-Sant’Anna, M. Rumination in bipolar disorder: A systematic review. Rev. Bras. Psiquiatr. 2015, 37, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Vassilopoulos, S.P. Social anxiety and ruminative self-focus. J. Anxiety Disord. 2008, 22, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Caselli, G.; Ferretti, C.; Leoni, M.; Rebecchi, D.; Rovetto, F.; Spada, M.M. Rumination as a predictor of drinking behaviour in alcohol abusers: A prospective study. Addiction 2010, 105, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Devynck, F.; Kornacka, M.; Sgard, F.; Douilliez, C. Repetitive Thinking in Alcohol-Dependent Patients. Subst. Use Misuse 2017, 52, 108–118. [Google Scholar] [CrossRef]
- Halari, R.; Premkumar, P.; Farquharson, L.; Fannon, D.; Kuipers, E.; Kumari, V. Rumination and Negative Symptoms in Schizophrenia. J. Nerv. Ment. Dis. 2009, 197, 703–706. [Google Scholar] [CrossRef]
- Cooper, Z.; Fairburn, C. The eating disorder examination: A semi-structured interview for the assessment of the specific psychopathology of eating disorders. Int. J. Eat. Disord. 1987, 6, 1–8. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Smith, K.E.; Mason, T.B.; Lavender, J.M. Rumination and eating disorder psychopathology: A meta-analysis. Clin. Psychol. Rev. 2018, 61, 9–23. [Google Scholar] [CrossRef]
- Napolitano, M.A.; Himes, S. Race, weight, and correlates of binge eating in female college students. Eat. Behav. 2011, 12, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Sassaroli, S.; Bertelli, S.; DeCoppi, M.; Crosina, M.; Milos, G.; Ruggiero, G. Worry and eating disorders: A psychopathological association. Eat. Behav. 2005, 6, 301–307. [Google Scholar] [CrossRef]
- Sternheim, L.; Startup, H.; Saeidi, S.; Morgan, J.; Hugo, P.; Russell, A.; Schmidt, U. Understanding catastrophic worry in eating disorders: Process and content characteristics. J. Behav. Ther. Exp. Psychiatry 2012, 43, 1095–1103. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; American Psychiatric Association: Washington, DC, USA, 1980. [Google Scholar]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; American Psychiatric Association: Washington, DC, USA, 1987. [Google Scholar]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Spitzer, R.L.; Endicott, J.; Robins, E. Research Diagnostic Criteria: Rationale and reliability. Arch. Gen. Psychiatry 1978, 35, 773. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Manual of the 28. International Statistical Classification of Diseases, Injuries, and Causes of Death; Sixth Revision of the International Lists of Diseases and Causes of Death, Adopted 1948; World Health Organization: Geneva, Switzerland, 1948. [Google Scholar]
- World Health Organization. Manual of the 30. International Statistical Classification of Diseases, Injuries, and Causes of Death; Based on the Recommendations of the Seventh Revision Conference, 1955, and Adopted by the Ninth World Health Assembly under the WHO Nomenclature Regulations; World Health Organization: Geneva, Switzerland, 1957. [Google Scholar]
- World Health Organization. Manual of the 32. International Statistical Classification of Diseases, Injuries, and Causes of Death; Based on Recommendations of the Eighth Revision Conference, 1965, and Adopted by the Nineteenth World Health Assembly; World Health Organization: Geneva, Switzerland, 1967. [Google Scholar]
- World Health Organization. Manual of the 34. International Classification of Diseases, Injuries, and Causes of Death; Based on the Recommendations of the Ninth Revision Conference, 1975, and Adopted by the Twenty-Ninth World Health Assembly; World Health Organization: Geneva, Switzerland, 1977. [Google Scholar]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Mansueto, G.; Caselli, G.; Ruggiero, G.M.; Sassaroli, S. Metacognitive beliefs and childhood adversities: An overview of the literature. Psychol. Health Med. 2018, 24, 542–550. [Google Scholar] [CrossRef]
- Zhu, C.; Sun, X.; So, S.H.-W. Associations between belief inflexibility and dimensions of delusions: A meta-analytic review of two approaches to assessing belief flexibility. Br. J. Clin. Psychol. 2018, 57, 59–81. [Google Scholar] [CrossRef]
- Palmieri, S.; Mansueto, G.; Ruggiero, G.M.; Caselli, G.; Sassaroli, S.; Spada, M.M. Metacognitive beliefs across eating disorders and eating behaviours: A systematic review. Clin. Psychol. Psychother. 2021. [Google Scholar] [CrossRef]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.E.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2010; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 March 2021). [CrossRef]
- Hakamata, Y.; Lissek, S.; Bar-Haim, Y.; Britton, J.C.; Fox, N.A.; Leibenluft, E.; Ernst, M.; Pine, D.S. Attention Bias Modification Treatment: A Meta-Analysis Toward the Establishment of Novel Treatment for Anxiety. Biol. Psychiatry 2010, 68, 982–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaini, S.; Belotti, R.; Ogliari, A.; Battaglia, M. A comprehensive meta-analysis of cognitive-behavioral interventions for social anxiety disorder in children and adolescents. J. Anxiety Disord. 2016, 42, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R. The file drawer problem and tolerance for null results. Psychol. Bull. 1979, 86, 638. [Google Scholar] [CrossRef]
- Juffer, F.; Van Ijzendoorn, M.H. Adoptees do not lack self-esteem: A meta-analysis of studies on self-esteem of transracial, international, and domestic adoptees. Psychol. Bull. 2007, 133, 1067. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.; Rothstein, H.R. References; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2009; pp. 409–414. [Google Scholar]
- González, M.; Ibáñez, I.; Barrera, A. Rumination, worry and negative problem orientation: Transdiagnostic processes of anxiety, eating behavior and mood disorders. Acta Colomb. Psicol. 2017, 20, 42–52. [Google Scholar]
- Kollei, I.; Brunhoeber, S.; Rauh, E.; De Zwaan, M.; Martin, A. Body image, emotions and thought control strategies in body dysmorphic disorder compared to eating disorders and healthy controls. J. Psychosom. Res. 2012, 72, 321–327. [Google Scholar] [CrossRef]
- Naumann, E.; Tuschen-Caffier, B.; Voderholzer, U.; Caffier, D.; Svaldi, J. Rumination but not distraction increases eating-related symptoms in anorexia and bulimia nervosa. J. Abnorm. Psychol. 2015, 124, 412. [Google Scholar] [CrossRef] [PubMed]
- Sapuppo, W.; Ruggiero, G.M.; Caselli, G.; Sassaroli, S. The Body of Cognitive and Metacognitive Variables in Eating Disorders: Need of Control, Negative Beliefs about Worry Uncontrollability and Danger, Perfectionism, Self-esteem and Worry. Isr. J. Psychiatry Relat. Sci. 2018, 55, 55–63. [Google Scholar]
- Troop, N.A.; Treasure, J.L. Psychosocial factors in the onset of eating disorders: Responses to life-events and difficulties. Br. J. Med. Psychol. 1997, 70, 373–385. [Google Scholar] [CrossRef]
- Cowdrey, F.A.; Park, R.J. The role of experiential avoidance, rumination and mindfulness in eating disorders. Eat. Behav. 2012, 13, 100–105. [Google Scholar] [CrossRef]
- Rawal, A.; Park, R.J.; Williams, J.M.G. Rumination, experiential avoidance, and dysfunctional thinking in eating disorders. Behav. Res. Ther. 2010, 48, 851–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.B.; Borders, A. The unique effects of angry and depressive rumination on eating-disorder psychopathology and the mediating role of impulsivity. Eat. Behav. 2018, 29, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Mason, T.B.; Lewis, R.J. Examining social support, rumination, and optimism in relation to binge eating among Caucasian and African–American college women. Eat. Weight. Disord. 2017, 22, 693–698. [Google Scholar] [CrossRef]
- Startup, H.; Lavender, A.; Oldershaw, A.; Stott, R.; Tchanturia, K.; Treasure, J.; Schmidt, U. Worry and Rumination in Anorexia Nervosa. Behav. Cogn. Psychother. 2013, 41, 301–316. [Google Scholar] [CrossRef]
- Zarychta, K.; Mullan, B.; Kruk, M.; Luszczynska, A. A vicious cycle among cognitions and behaviors enhancing risk for eating disorders. BMC Psychiatry 2017, 17, 154. [Google Scholar] [CrossRef]
- Crino, N.; Touyz, S.; Rieger, E. How eating disordered and non-eating disordered women differ in their use (and effectiveness) of cognitive self-regulation strategies for managing negative experiences. Eat. Weight. Disord. 2019, 24, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.S.; Cordes, M.; Hirschfeld, G.; Vocks, S. Affect and worry during a checking episode: A comparison of individuals with symptoms of obsessive-compulsive disorder, anorexia nervosa, bulimia nervosa, body dysmorphic disorder, illness anxiety disorder, and panic disorder. Psychiatry Res. 2019, 272, 349–358. [Google Scholar] [CrossRef]
- Connolly, A.M.; Rieger, E.; Caterson, I. Binge eating tendencies and anger coping: Investigating the confound of trait neuroticism in a non-clinical sample. Eur. Eat. Disord. Rev. 2007, 15, 479–486. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Stice, E.; Wade, E.; Bohon, C. Reciprocal relations between rumination and bulimic, substance abuse, and depressive symptoms in female adolescents. J. Abnorm. Psychol. 2007, 116, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Harrell, Z.A.T.; Jackson, B. Thinking Fat and Feeling Blue: Eating Behaviors, Ruminative Coping, and Depressive Symptoms in College Women. Sex Roles 2008, 58, 658–665. [Google Scholar] [CrossRef]
- Selby, E.A.; Anestis, M.D.; Joiner, T.E. Understanding the relationship between emotional and behavioral dysregulation: Emotional cascades. Behav. Res. Ther. 2008, 46, 593–611. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S. Specificity of cognitive emotion regulation strategies: A transdiagnostic examination. Behav. Res. Ther. 2010, 48, 974–983. [Google Scholar] [CrossRef]
- Holm-Denoma, J.M.; Hankin, B.L. Perceived Physical Appearance Mediates the Rumination and Bulimic Symptom Link in Adolescent Girls. J. Clin. Child Adolesc. Psychol. 2010, 39, 537–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verplanken, B.; Tangelder, Y. No body is perfect: The significance of habitual negative thinking about appearance for body dissatisfaction, eating disorder propensity, self-esteem and snacking. Psychol. Health 2011, 26, 685–701. [Google Scholar] [CrossRef] [PubMed]
- Gordon, K.H.; Holm-Denoma, J.M.; Troop-Gordon, W.; Sand, E. Rumination and body dissatisfaction interact to predict concurrent binge eating. Body Image 2012, 9, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Kelly, N.R.; Lydecker, J.; Mazzeo, S.E. Positive cognitive coping strategies and binge eating in college women. Eat. Behav. 2012, 13, 289–292. [Google Scholar] [CrossRef]
- Hilt, L.M.; Roberto, C.A.; Nolen-Hoeksema, S. Rumination mediates the relationship between peer alienation and eating pathology in young adolescent girls. Eat. Weight. Disord. 2013, 18, 263–267. [Google Scholar] [CrossRef]
- Svaldi, J.; Naumann, E. Effects of Rumination and Acceptance on Body Dissatisfaction in Binge Eating Disorder. Eur. Eat. Disord. Rev. 2014, 22, 338–345. [Google Scholar] [CrossRef]
- Mason, T.B.; Lewis, R.J. Minority Stress and Binge Eating Among Lesbian and Bisexual Women. J. Homosex. 2015, 62, 971–992. [Google Scholar] [CrossRef]
- Breithaupt, L.; Rallis, B.; Mehlenbeck, R.; Kleiman, E. Rumination and self-control interact to predict bulimic symptomatology in college students. Eat. Behav. 2016, 22, 1–4. [Google Scholar] [CrossRef]
- Jungmann, S.M.; Vollmer, N.; Selby, E.A.; Witthöft, M. Understanding Dysregulated Behaviors and Compulsions: An Extension of the Emotional Cascade Model and the Mediating Role of Intrusive Thoughts. Front. Psychol. 2016, 7, 994. [Google Scholar] [CrossRef] [Green Version]
- Maraldo, T.M.; Zhou, W.; Dowling, J.; Wal, J.S.V. Replication and extension of the dual pathway model of disordered eating: The role of fear of negative evaluation, suggestibility, rumination, and self-compassion. Eat. Behav. 2016, 23, 187–194. [Google Scholar] [CrossRef]
- Naumann, E.; Tuschen-Caffier, B.; Voderholzer, U.; Svaldi, J. Spontaneous Emotion Regulation in Anorexia and Bulimia Nervosa. Cogn. Ther. Res. 2016, 40, 304–313. [Google Scholar] [CrossRef]
- Seidel, M.; Petermann, J.; Diestel, S.; Ritschel, F.; Boehm, I.; King, J.A.; Geisler, D.; Bernardoni, F.; Roessner, V.; Goschke, T.; et al. A naturalistic examination of negative affect and disorder-related rumination in anorexia nervosa. Eur. Child Adolesc. Psychiatry 2016, 25, 1207–1216. [Google Scholar] [CrossRef]
- Opwis, M.; Salewski, C.; Schmidt, J.; Martin, A. Gender differences in eating behavior and eating pathology: The mediating role of rumination. Appetite 2017, 110, 103–107. [Google Scholar] [CrossRef]
- Wang, S.B.; Borders, A. Rumination mediates the associations between sexual minority stressors and disordered eating, particularly for men. Eat. Weight. Disord. 2017, 22, 699–706. [Google Scholar] [CrossRef]
- Wang, S.B.; Lydecker, J.A.; Grilo, C.M. Rumination in Patients with Binge-Eating Disorder and Obesity: Associations with Eating-Disorder Psychopathology and Weight-bias Internalization. Eur. Eat. Disord. Rev. 2017, 25, 98–103. [Google Scholar] [CrossRef]
- Dondzilo, L.; Rieger, E.; Palermo, R.; Byrne, S.; Bell, J. Correction: The mediating role of rumination in the relation between attentional bias towards thin female bodies and eating disorder symptomatology. PLoS ONE 2018, 13, e0196143. [Google Scholar] [CrossRef] [Green Version]
- Van Durme, K.; Goossens, L.; Bosmans, G.; Braet, C. The Role of Attachment and Maladaptive Emotion Regulation Strategies in the Development of Bulimic Symptoms in Adolescents. J. Abnorm. Child Psychol. 2017, 46, 881–893. [Google Scholar] [CrossRef]
- Birmachu, A.M.; Heidelberger, L.; Klem, J. Rumination and perceived social support from significant others interact to predict eating disorder attitudes and behaviors in university students. J. Am. Coll. Health 2019. [Google Scholar] [CrossRef]
- Fresnics, A.A.; Wang, S.B.; Borders, A. The unique associations between self-compassion and eating disorder psychopathology and the mediating role of rumination. Psychiatry Res. 2019, 274, 91–97. [Google Scholar] [CrossRef]
- Hernando, A.; Pallás, R.; Cebolla, A.; García-Campayo, J.; Hoogendoorn, C.J.; Roy, J.F. Mindfulness, rumination, and coping skills in young women with Eating Disorders: A comparative study with healthy controls. PLoS ONE 2019, 14, e0213985. [Google Scholar] [CrossRef]
- Smith, K.E.; Mason, T.B.; Anderson, N.L.; Lavender, J.M. Unpacking cognitive emotion regulation in eating disorder psychopathology: The differential relationships between rumination, thought suppression, and eating disorder symptoms among men and women. Eat. Behav. 2019, 32, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Branley-Bell, D.; Talbot, C.V. Exploring the impact of the COVID-19 pandemic and UK lockdown on individuals with expe-rience of eating disorders. J. Eat. Disord. 2020, 8, 1–12. [Google Scholar] [CrossRef]
- Martino, F.; Caselli, G.; Berardi, D.; Fiore, F.; Marino, E.; Menchetti, M.; Prunetti, E.; Ruggiero, G.M.; Sasdelli, A.; Selby, E.; et al. Anger rumination and aggressive behaviour in borderline personality disorder. Pers. Ment. Health 2015, 9, 277–287. [Google Scholar] [CrossRef]
- Salters-Pedneault, K.; Roemer, L.; Tull, M.; Rucker, L.; Mennin, D.S. Evidence of Broad Deficits in Emotion Regulation Associated with Chronic Worry and Generalized Anxiety Disorder. Cogn. Ther. Res. 2006, 30, 469–480. [Google Scholar] [CrossRef]
- Vann, A.; Strodl, E.; Anderson, E. Thinking about internal states, a qualitative investigation into metacognitions in women with eating disorders. J. Eat. Disord. 2013, 1, 22. [Google Scholar] [CrossRef] [Green Version]
- Vinai, P.; Da Ros, A.; Cardetti, S.; Casey, H.; Studt, S.; Gentile, N.; Tagliabue, A.; Vinai, L.; Vinai, P.; Bruno, C.; et al. The DSM-5 effect: Psychological characteristics of new patients affected by Binge Eating Disorder following the criteria of the DSM-5 in a sample of severe obese patients. Eat. Weight Disord. 2016, 21, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.; Matthews, G. Modelling cognition in emotional disorder: The S-REF model. Behav. Res. Ther. 1996, 34, 881–888. [Google Scholar] [CrossRef]
- Wells, A. Emotional Disorders and Metacognition: Innovative Cognitive Therapy; Wiley: Chichester, UK, 2000. [Google Scholar]
- Spada, M.M.; Caselli, G.; Nikčević, A.V.; Wells, A. Metacognition in addictive behaviors. Addict. Behav. 2015, 44, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Spada, M.M.; Caselli, G.; Fernie, B.A.; Manfredi, C.; Boccaletti, F.; Dallari, G.; Gandini, F.; Pinna, E.; Ruggiero, G.M.; Sassaroli, S. Desire thinking: A risk factor for binge eating? Eat. Behav. 2015, 18, 48–53. [Google Scholar] [CrossRef]
- Mansueto, G.; Martino, F.; Palmieri, S.; Scaini, S.; Ruggiero, G.M.; Sassaroli, S.; Caselli, G. Desire Thinking across addictive behaviours: A systematic review and meta-analysis. Addict. Behav. 2019, 98, 106018. [Google Scholar] [CrossRef]
- Hong, R.Y. Worry and rumination: Differential associations with anxious and depressive symptoms and coping behavior. Behav. Res. Ther. 2007, 45, 277–290. [Google Scholar] [CrossRef]
- Hoyer, J.; Gloster, A.T.; Herzberg, P.Y. Is worry different from rumination? Yes, it is more predictive of psychopathology! GMS Psycho Soc. Med. 2009, 6. [Google Scholar] [CrossRef]
- Kaplan, D.M.; Palitsky, R.; Carey, A.L.; Crane, T.E.; Havens, C.M.; Medrano, M.R.; Reznik, S.J.; Sbarra, D.A.; O’Connor, M.-F. Maladaptive repetitive thought as a transdiagnostic phenomenon and treatment target: An integrative review. J. Clin. Psychol. 2018, 74, 1126–1136. [Google Scholar] [CrossRef] [PubMed]
- Watkins, E.R. Rumination-Focused Cognitive-Behavioral Therapy for Depression; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Fava, G.A. Meta-Analyses and Conflict of Interest. CNS Drugs 2012, 26, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Cowdrey, F.A.; Park, R.J. Assessing rumination in eating disorders: Principal component analysis of a minimally modified ruminative response scale. Eat. Behav. 2011, 12, 321–324. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Source | Study Design | Sample-Size | Age (Years) Mean ± SD | Sex % (n) | Diagnostic Tool Eating Measure | Sub-Types of ED Symptoms | Worry Measure |
|---|---|---|---|---|---|---|---|
| Napolitano and Himes 2011 [31] | case–control | cases: 46 binge eating group without BED: 186 | - | F: 100% (232) | DSM-IV-TR EDDS | BED | FOBES |
| Sassaroli et al. 2005 [32] | case–control | cases: 63 controls: 30 | 23.06 ± 4.54 vs. 26.32 ± 4.27 | F: 100% (93) | SCID-I | AN BN | PSWQ |
| Sternheim et al. 2012 [33] | case–control | cases: 45 controls: 37 | 25.8 ± 8.5 vs. 27.8 ± 10.2 | not reported | DSM-IV EDE | AN BN | PSWQ Catastrophizing Interview |
| González et al. 2017 [57] | cross-sectional | general population: 176 | 31.2 ± 13.3 | F: 67% (118) | EAT | AN BN | PSWQ |
| Kollei, et al. 2012 [58] | case–control | cases: 66 control: 33 | AN: 26.94 ± 9.15 BN: 25.94 ± 8.25 CG: 26.91 ± 8.48 | F: 95.45% (63) vs. 69.7% (23) | DSM-IV | AN BN | CITQ |
| Sapuppo et al. 2018 [60] | case–control | cases: 84 controls: 38 | 23.39 ± 4.75 vs. 25.31 ± 5.4 | F: 100% (122) | SCID-I | AN BN | PSWQ |
| Startup et al. 2013 [66] | cross-sectional | cases: 62 | 26.6 ± 7.8 | F: 93.5% (58) | DSM-IV EDE | AN | PSWQ |
| Zarychta et al. 2017 [67] | cross-sectional | general population: 1260 | 16.38 ± 0.80 | F: 41.7% (525) | MBSRQ | - | MBSRQ |
| Crino et al. 2019 [68] | case–control | cases: 90 controls: 97 | 25.23 ± 8.33 vs. 20.63 ± 6.37 | F: 100% (187) | DSM-5 | AN BN BED No-ED | TCQ |
| Hartmann et al. 2019 [69] | cross-sectional | cases: 95 | AN: 23.64 ± 0.62 BN: 26.09 ± 1.17 | F: 98%(49) F: 97.78%(44) | EDE-Q | AN BN | Self-constructed worry item |
| Source | Study Design | Sample-Size | Age (Years) Mean ± SD | Sex % (n) | Diagnostic Tool Eating Measure | Sub-Types of ED Symptoms | Rumination Measure |
|---|---|---|---|---|---|---|---|
| González et al. 2017 [57] | cross-sectional | general population: 176 | 31.2 ± 13.3 | F: 67% (118) | EAT-26 | AN BN | RRS |
| Naumann et al. 2015 [59] | experiment case-control | cases: 36 controls: 19 | AN: 24.94 ± 8.92 BN: 23.28 ± 6.37 CG: 23.32 ± 8.02 | F: 100% (111) | DSM-IV-TR EDE | AN BN | Rumination experimentally induced by Nolen-Hoeksema and Morrow’s task (1993) RSQ |
| Troop and Treasure 1997 [61] | case–control | cases: 21 controls: 15 | AN: 23.3 ± 5 BN: 25.4 ± 10.8 CG: 29.5 ± 9 | F: 100% (36) | ICD-10 | AN BN | Coping Strategies Interview |
| Cowdrey and Park 2012 [62] | cross-sectional | general population: 228 | 24.03 ± 7.62 | F:100% vs. 100% | EDE-Q | AN and Eating pathology | RRS-ED |
| AN: 42 | 24 ± 8.31 | ||||||
| Rawal et al. 2010 [63] | Study 1 cross-sectional | students: 177 | 22.39 ± 5.13 | F: 68.92% (122) | DSM-IV EDE-Q | AN | Study 1 & 2: RRS |
| Study 2 case–control | cases: 13 controls: 13 | 26.38 ± 8.77 vs. 25.77 ± 4.85 | F:100% vs. 100% | MINI EDE | |||
| Wang and Borders 2018 [64] | Study 1 cross-sectional | undergraduate students: 126 | 19.7 ± 1.10 | F: 84% (106) | EDE-Q | Eating pathology | RRS |
| Study 2 cross-sectional | cases: 85 | 24.57 ± 9.95 | F: 87.1% (74) | ||||
| Mason and Lewis 2017 [65] | cross-sectional | general population Caucasian: 100 | 20.14 ± 1.82 | F = 100% | DSM-5 (binge eating episode) | - | RSQ |
| African-America: 84 | 19.75 ± 1.86 | ||||||
| Startup et al. 2013 [66] | cross-sectional | cases: 62 | 26.6 ± 7.8 | F: 93.5% (58) | DSM-IV EDE | AN | CERTS |
| Connolly et al. 2007 [70] | cross-sectional | general population: 140 | 19.5 ± 2.57 | F 100% (140) | BES EDE-Q | BED | BARQ |
| Nolen-Hoeksema et al. 2007 [71] | cross-sectional | general population: 496 | 13.5 ± 0.67 | F = 100% | DSM-IV EDE | BN | RSQ |
| Harrell et al. 2008 [72] | cross-sectional | general population: 329 | 19.31 | F = 100% | Dieting and Bingeing Severity Scale | - | AFCI |
| Selby et al. 2008 [73] | cross-sectional | general population: 200 | 18.6 ± 2.36 | F: 68.5% (137) | EDI | BN | CERQ |
| Aldao and Nolen-Hoeksema 2010 [74] | cross-sectional | undergraduate students: 252 | 18.44 ± 0.66 | F: 55.6% (140) | EDE-Q | - | RRS |
| Holm-Denoma and Hankin 2010 [75] | cross-sectional | general population: 191 | 14.5 ± 1.4 | F = 100% | EDDS | BN | CRSQ |
| Verplanken and Tangelder 2011 [76] | cross-sectional | students: 303 | 24 ± 4 | F: 50.16% (152) | EDS-5 | - | Negative Body Image Thinking |
| Gordon et al. 2012 [77] | cross-sectional | general population: 780 | 19.27 ± 2.12 | F: 65.7% (512) | BES | BED | RRS |
| Kelly et al. 2012 [78] | cross-sectional | general population: 419 | 18.95 ± 1.33 | F = 100% | EDE-Q | BED | CERQ |
| Hilt et al. 2013 [79] | cross-sectional | general population: 101 | 12.7 ± 1.14 | F = 100% | Children’s Eating Attitudes Test ChEAT | Eating pathology | CRSQ |
| Svaldi and Naumann 2014 [80] | cross-sectional | cases: 30 | 46.33 | F = 100% | DSM-IV-TR EDE | BED | PTQ |
| Mason and Lewis 2015 [81] | cross-sectional | general population: 164 | - | F = 100% | BES | BED | CERQ |
| Breithaupt et al. 2016 [82] | cross-sectional | general population: 353 | 21.93 ± 5.78 | F = 85% (300) | EAT-26 | BN | RRS |
| Jungmann et al. 2016 [83] | cross-sectional | general population: 414 | 47.2 ± 16.7 | F: 54% (223) | EDI-2 | BN | RSQ |
| Maraldo et al. 2016 [84] | cross-sectional | community participants: 313 students: 296 | 34.74 ± 11.36 vs. 19.44 ± 1.75 | F = 100% | EDE-Q | Eating pathology | RRS |
| Naumann et al. 2016 [85] | case-control | cases: AN: 42 BN: 40 controls: 41 | AN: 25.71 ± 10.65 BN: 25.78 ± 8.49 CG: 25.61 ± 10.30 | F = 100% | DSM-IV EDE | AN BN | Self-constructed Visual Analog Scales |
| Seidel et al. 2016 [86] | case-control | cases: 37 controls: 33 | AN: 16.40 ± 2.33 CG: 16.51 ± 3.79 | F = 100% | DSM-IV EDI-2 | AN | PTQ |
| Opwis et al. 2017 [87] | cross-sectional | general population: 295 | F: 30.23 ± 8.94 M: 30.76 ± 9.14 | F: 69% (205) | EDE-Q | Eating pathology | RS-8 |
| Wang and Borders 2017 [88] | cross-sectional | general population: 116 | 24.8 ± 5.35 | M: 59.5% (69) | EAT-26 | Eating pathology | Items modified from the Rumination About Interpersonal Offences Scale |
| Wang et al. 2017 [89] | cross-sectional | cases: 237 | 47.9 ± 10 | F: 70% (167) | DSM-IV-TR EDE | BED | RRS |
| Dondzillo et al. 2018 [90] | cross-sectional | general population: 73 | 18.59 ± 1.28 | F = 100% | DEBQ | AN | RRS-ED |
| Van Durme et al. 2018 [91] | cross-sectional | general population: 397 | 14.02 | F: 62.7% (249) | EDI-II | BN | FEEL-KJ |
| Birmachu et al. 2019 [92] | cross-sectional | general population: 300 | 22.99 ± 6.91 | F: 63.6% (190) | EDE-Q | Eating pathology | RRQ |
| Fresnics et al. 2019 [93] | cross-sectional | general population: 190 | 19.3 ± 1.10 | F: 84% (160) | EDE-Q | Eating pathology | RRS |
| Hernando et al. 2019 [94] | case-control | cases: 25 controls: 25 | 16.6 ± 2.24 vs. 19.08 ± 0.64 | F = 100% | - | AN, BN, OSFED | RSQ |
| Smith et al. 2019 [95] | cross-sectional | undergraduate students: 263 | 20.3 ± 3.68 | F: 74.9% (197) | EDDS | Eating pathology | RRS |
| Branley-Bell and Talbot 2020 [96] | cross-sectional | general population: 129 | 9.27 ± 8.99 | F: 93.8% (121) | Self-reported ED | Eating pathology | RRS-ED |
| ES | β Point Estimate | SE | CI | p | |
|---|---|---|---|---|---|
| Subtypes of ED symptoms | 0.003 | ||||
| AN | 1.35 | 0.20 | 0.96–1.74 | <0.001 | |
| BN | 0.75 | 0.11 | 0.54–0.97 | <0.001 | |
| BED | 0.50 | 0.15 | 0.20–0.80 | 0.001 | |
| Presence vs. absence of diagnosis of EDs | 0.004 | ||||
| Clinical samples | 1.14 | 0.13 | 0.87–1.40 | <0.001 | |
| Healthy controls from the general population | 0.69 | 0.08 | 0.54–0.85 | <0.001 | |
| Repetitive Negative Thinking | 0.118 | ||||
| Worry | 1.04 | 0.14 | 0.76–1.32 | <0.001 | |
| Rumination | 0.79 | 0.08 | 0.64–0.94 | <0.001 | |
| Age | −0.0108 | 0.009 | −0.03–0.01 | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmieri, S.; Mansueto, G.; Scaini, S.; Caselli, G.; Sapuppo, W.; Spada, M.M.; Sassaroli, S.; Ruggiero, G.M. Repetitive Negative Thinking and Eating Disorders: A Meta-Analysis of the Role of Worry and Rumination. J. Clin. Med. 2021, 10, 2448. https://doi.org/10.3390/jcm10112448
Palmieri S, Mansueto G, Scaini S, Caselli G, Sapuppo W, Spada MM, Sassaroli S, Ruggiero GM. Repetitive Negative Thinking and Eating Disorders: A Meta-Analysis of the Role of Worry and Rumination. Journal of Clinical Medicine. 2021; 10(11):2448. https://doi.org/10.3390/jcm10112448
Chicago/Turabian StylePalmieri, Sara, Giovanni Mansueto, Simona Scaini, Gabriele Caselli, Walter Sapuppo, Marcantonio M. Spada, Sandra Sassaroli, and Giovanni Maria Ruggiero. 2021. "Repetitive Negative Thinking and Eating Disorders: A Meta-Analysis of the Role of Worry and Rumination" Journal of Clinical Medicine 10, no. 11: 2448. https://doi.org/10.3390/jcm10112448