Abstract
Many non-invasive methods, such as imaging tests, have been developed aiming to add a contribution to existing studies in estimating patients’ prognosis after myocardial injury. This prognosis is proportional to myocardial viability, which is evaluated in coronary artery disease and left ventricular dysfunction patients only.
While myocardial viability represents the likelihood of a dysfunctional muscle (resulting from decreased oxygen supply for coronary artery obstruction), hibernation represents post-interventional functional recovery itself.
This article proposes a review of pathophysiological basis of viability, diagnostic methods, prognosis and future perspectives of myocardial viability. An electronic bibliographic search for articles was performed in PubMed, Lilacs, Cochrane and Scielo databases, according to pre-established criteria.
The studies showed the ability of many imaging techniques in detecting viable tissues in dysfunctional areas of left ventricle resulting from coronary artery injuries. These techniques can identify patients who may benefit from myocardial revascularization and indicate the most appropriate treatment.
Keywords
Tissue Survival; Diagnostic Imaging; Myocardial Revascularization / surgery; Myocardium Stunning / physiopathology
Resumo
Diversos métodos não invasivos, como novos exames de imagem, vem sendo aprimorados, a fim de somar esforços com os atuais em estimar o prognóstico de pacientes pós-injúria miocárdica. Este prognóstico é proporcional à viabilidade miocárdica, a qual tem sua avaliação reservada para pacientes portadores de doença arterial coronariana e insuficiência ventricular esquerda. Enquanto a viabilidade miocárdica se mostra como a capacidade de recuperação funcional do músculo com disfunção por redução de oxigênio fornecido por artérias coronárias obstruídas, a hibernação consiste na própria recuperação funcional após intervenções.
Este artigo propõe uma revisão sobre as bases fisiopatológicas do processo de viabilidade, métodos diagnósticos disponíveis, prognóstico e perspectivas para o futuro acerca dessa condição. Realizou-se pesquisa de busca bibliográfica informatizada em bases eletrônicas de dados, como PubMed, Lilacs, Cochrane e Scielo, onde foram selecionados os estudos de acordo com critérios pré-determinados.
Os estudos demonstram a capacidade de várias técnicas de imagem de identificar tecido viável em regiões disfuncionais do ventrículo esquerdo em decorrência de lesões em artérias coronárias. Estas técnicas podem identificar pacientes com potencial benefício da revascularização miocárdica e orientar o tratamento mais adequado.
Palavras-chave
Sobrevivência de Tecidos; Diagnóstico por Imagem; Revascularização Miocárdica / cirurgia; Miocárdio Atordoado / fisiopatologia
Introduction
Assessment of myocardial viability using non-invasive imaging techniques has motivated several studies in search of the most promising and sensitive tests. These tests highlight the importance of a correct evaluation of this condition for an appropriate risk stratification and selection of patients considered eligible for myocardial revascularization. Since cardiac function is not a dichotomous variable, some of its aspects measured by imaging techniques may not be measurable by another method. Useful parameters to guide therapeutic strategies include ejection fraction, scar size, ischemia and remodeling extension, as well as duration of cardiac dysfunction.11 Anavekar NS, Chareonthaitawee P, Narula J, Gersh BJ. Revascularization in patients with severe left ventricular dysfunction. is the assessment of viability still viable? J Am Coll Cardiol. 2016;67(24):2874-87.,22 Ling LF, Marwick TH, Flores DR, Jaber WA, Brunken RC, Cerqueira MD, et al. Identification of therapeutic benefit from revascularization in patients with left ventricular systolic dysfunction: Inducible ischemia versus hibernating myocardium. Circ Cardiovasc Imaging 2013;6(3):363-72.
Using a multimodal approach of viability, a pilot study33 Narula J, Dawson MS, Singh BK, Amanullah A, Acio ER, Chaudhry FA, et al. Noninvasive characterization of stunned, hibernating, remodeled and nonviable myocardium in ischemic cardiomyopathy. J Am Coll Cardiol. 2000;36(6):1913-9. showed higher values for these variables, which were analyzed in combination, providing a more reliable characterization of myocardial function. However, due to the lack of larger studies, imaging tests based on multimodal approach are not recommended yet. It is worth pointing out that even though the presence of a viable myocardium in a large heart area is important for revascularization, the decision for this procedure should be based on patient’s clinical status, evidence of ischemia, coronary anatomy and left ventricular global and regional function.44 Zaret BL, Beller GA. Clinical Nuclear Cardiology: state of the heart and future directions. 4th ed. Amsterdam: Elsevier; 2006 p. 31-4, 495-555.
Determination of myocardial viability is a common and clinically relevant challenge, that may be necessary in post-infarction patients receiving thrombolytic therapy. Also, it may be helpful for surgeons and cardiologists in choosing the best therapy from interventionist strategy, angioplasty and myocardial revascularization.55 Ragosta M, Beller GA. The noninvasive assessment of myocardial viability. Clin Cardiol. 1993;16(7):531-8. This is particularly important in cases when myocardial revascularization is considered, due to high mortality rate and perioperative morbidity in these patients.66 Solar M, Zizka J, Klzo L, Tintera J, Vizda J, Ceral J. Contrast-enhanced magnetic resonance and thallium scintigraphy in the detection of myocardial viability:a prospective comparative study. Int Heart J. 2006;47(4):521-32.
In viability studies, while nuclear medicine techniques have high sensitivity, the techniques used to evaluate contractile reserve have higher specificity. Imaging methods, such as computed tomography (CT), positron-emission tomography (PET), myocardial scintigraphy, echocardiography with dobutamine and cardiac magnetic resonance (CMR) have been exhaustively investigated in attempt to establish the best method for myocardial study.77 Fernandes H, Sousa A, Campos J, Patrício J, Oliveira A, Vieira T, et al. [Myocardial viability assessment]. Acta Med Port. 2011 Dec;24 Suppl 4:989-94.
Pathophysiology
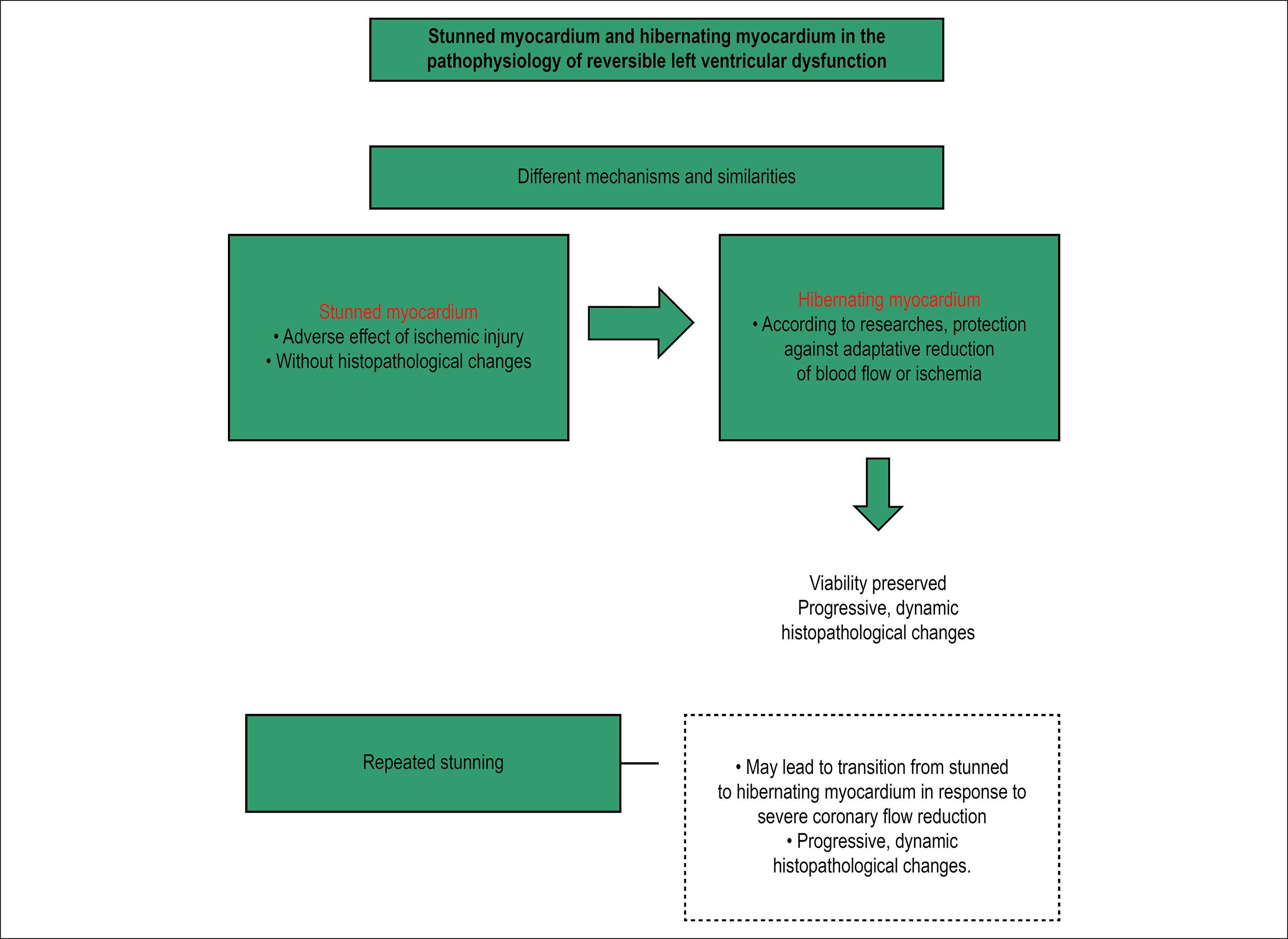
Myocardial viability refers to myocardial cells that are alive after myocardial injury, according to cellular, metabolic and contractile functions. It describes ventricular dysfunction without tissue necrosis, which enables functional recovery after restoration of blood supply. In this context, although the definitions “stunned myocardium” and “hibernating” myocardium have distinct characteristics, the latter may represent the adaptation of repeated episodes of the former, as described by Chareonthaitawee et al.88 Chareonthaitawee P, Gersh BJ, Araoz PA, Gibbons RJ. Revascularization in severe left ventricular dysfunction: the role of viability testing; J Am Coll Cardiol. 2005;46(4):567-74. (Figure 1).
Main feature of the physiopathology of stunned myocardium and hibernating myocardium [adapted from Chareonthaitawee et al.88 Chareonthaitawee P, Gersh BJ, Araoz PA, Gibbons RJ. Revascularization in severe left ventricular dysfunction: the role of viability testing; J Am Coll Cardiol. 2005;46(4):567-74.]
“Stunned myocardium” results from a rapid, severe episode of coronary occlusion followed by recovery of coronary flow. An abrupt decrease in coronary flow causes contractile dysfunction, which persists even after its restoration. Despite minimal necrosis, ventricular dysfunction may be prolonged, from hours or even weeks. A group of researchers,99 Barnes E, Dutka DP, Khan M, Camici PG, Hall RJ. Effect of repeated episodes of reversible myocardial ischemia on myocardial blood flow and function in humans. Am J Physiol Heart Circ Physiol. 2002;282(5):H1603-8. investigating ventricular function in patients with coronary heart disease, demonstrated that repeated episodes of ischemia may lead to cumulative stunning, which contributes to the development of chronic, post-ischemic, left ventricular dysfunction. Interestingly, similar degrees of left ventricular dysfunction in distinct patients may be associated with significant differences in the degree of myocardial viability. Besides, viability is not correlated with myocardial wall thickness, since ventricular wall thinning does not necessarily mean absence of myocardial viability.1010 Camici PG, Prasad SK, Rimoldi OE. Stunning, hibernation, and assessment of myocardial viability. Circulation. 2008;117(1):103-14.
“Hibernating myocardium” has been defined as the presence of severe systolic dysfunction with evidence of hypoperfusion at rest;33 Narula J, Dawson MS, Singh BK, Amanullah A, Acio ER, Chaudhry FA, et al. Noninvasive characterization of stunned, hibernating, remodeled and nonviable myocardium in ischemic cardiomyopathy. J Am Coll Cardiol. 2000;36(6):1913-9. it refers to a myocardium with preserved cellularity, but reduced blood flow, leading to depressed ventricular function, even at rest.1111 Demirkol MO. Myocardial viability testing in patients with severe left ventricular dysfunction by SPECT and PET. Anadolu Kardiyol Derg. 2008 Nov;8 Suppl 2:60-70. The first theory of hibernating myocardium characterized it as an adaptation to chronic hypoperfusion whose intensity was not sufficiently significant to cause infarction.1212 Lim SP, Mc Ardle BA, Beanlands RS, Hessian RC. Myocardial viability: it is still alive. Semin Nucl Med. 2014;44(5):358-74. This was supported by CMR and PET studies on dysfunctional myocardial areas with reduced blood flow.1313 Selvanayagam JB, Jerosch-Herold M, Porto I, Sheridan D, Cheng AS, Petersen SE, et al. Resting myocardial blood flow is impaired in hibernating myocardium: a magnetic resonance study of quantitative perfusion assessment. Circulation. 2005;112(21):3289-96.,1414 Conversano A, Walsh JF, Geltman EM, Perez JE, Bergmann SR, Gropler RJ. Delineation of myocardial stunning and hibernation by positron emission tomography in advanced coronary artery disease. Am Heart J. 1996;131(3):440-50. However, pathogenesis of hibernating myocardium is still subject of studies and has not been elucidated yet,; it is believed, however, to be conditioned to a functional dysregulation related to mitochondrial impairment, in attempt to protect cardiac muscle cells from ischemia.1111 Demirkol MO. Myocardial viability testing in patients with severe left ventricular dysfunction by SPECT and PET. Anadolu Kardiyol Derg. 2008 Nov;8 Suppl 2:60-70.,1515 Canty JM Jr, Fallavollita JA. Hibernating myocardium. J Nucl Med. 2005;12(1):104-19. Hibernating is also known to have intrinsic cellular and extracellular changes, that may be associated with the time required for reversibility of the process,1212 Lim SP, Mc Ardle BA, Beanlands RS, Hessian RC. Myocardial viability: it is still alive. Semin Nucl Med. 2014;44(5):358-74. which may vary from days to 14 months.1616 Vanoverschelde JL, Wijns W, Borgers M, Heyndrickx G, Depré C, Flameng W, et al. Chronic myocardial hibernation in humans: from bedside to bench. Circulation. 1997;95(7):1961-71.,1717 Bax JJ, Visser FC, Poldermans D, Elhendy A, Cornel JH, Boersma E, et al. Time course of functional recovery of stunned and hibernating segments after surgical revascularization. Circulation. 2001;104(12 Suppl 1):I314-8.
Clinical implications
Assessment of viability may significantly contribute to the identification of patients who would benefit from revascularization, particularly by the improvement in ventricular function and survival. To demonstrate the clinical usefulness of viability, a meta-analysis was performed with 24 studies on different techniques on viability detection in patients with chronic coronary artery disease (CAD) and myocardial dysfunction. Annual mortality rate in the group of patients with myocardial viability and in drug treatment was 16%, in contrast with 3.2% in the group that underwent revascularization.1818 Arai AE. Myocardial infarction and viability with an emphasis on imaging delayed enhancement. In: Kwong RY. (ed.). Cardiovascular magnetic resonance imaging. Totowa (NJ): Humana Press Inc; 2008. p. 351-75.,1919 Allman KC, Shaw LJ, Hachamovitch R, Udelson JE. Myocardial viability testing and impact of revascularization on prognosis in patients with coronary artery disease and left ventricular dysfunction: a meta-analysis. J Nucl Cardiol. 2002;39(7):1151-8.
In CAD patients, left ventricular dysfunction may be caused by areas of viable myocardium and fibrotic areas combined. Assessment of cardiac muscle using imaging methods enables the localization, quantification of viability in dysfunctional myocardium and possibility of anatomical revascularization, which is essential for treatment planning of these patients.1111 Demirkol MO. Myocardial viability testing in patients with severe left ventricular dysfunction by SPECT and PET. Anadolu Kardiyol Derg. 2008 Nov;8 Suppl 2:60-70.
This article proposes a review of pathophysiological bases of myocardial viability, diagnostic methods available, prognosis and risk for this condition. A bibliographic search was performed on the electronic databases PubMed, Lilacs, Cochrane and Scielo, based on pre-established criteria.
Methods
To achieve the objectives and results proposed, a descriptive review of scientific literature was conducted of studies on diagnostic accuracy of imaging tests used for the measurement of myocardial viability. We included both studies showing the superiority of certain method and those comparing the efficacy of the methods from the perspective of other authors.
Inclusion criteria:
Types of study: as “review articles”, we included studies aimed to demonstrate the efficacy of imaging tests in measuring myocardial viability after ischemia.
Population: heart disease patients with history of myocardial infarction.
Exclusion criteria:
Studies that did not provide a detailed description of the protocols of the diagnostic methods or of data statistical analysis, and studies that did not meet the inclusion criteria were excluded.
Search on the databases
The following databases were searched:
• PubMed/MEDLINE: North-American database, one of the largest in health, with no limits of date.
The following descriptors were used for the search on Pubmed: Myocardial viability; PET; CT; SPECT; Resonance Magnetic myocardial; Echocardiography.
• LILACS: database that integrates the BIREME system and includes several scientific journals, dissertations and books.
The following terms were used: Myocardial Viability ANS viability studies.
• COCHRANE: database focused on systemic reviews. The terms used in this database were: Myocardial viability.
Diagnostic methods
Assessment of myocardial viability by dobutamine stress echocardiography
The use of dobutamine stress echocardiography for detection of myocardial viability is an efficient and safe method in both acute and chronic phases of CAD,2020 Pierard LA, De Landsheere CM, Berthe C, Rigo P, Kulbertus HE. Identification of viable myocardium by echocardiography during dobutamine infusion in patients with myocardial infarction after thrombolytic therapy: comparison with positron emission tomography. J Am Coll Cardiol. 1990;15(5):1021-3. with low incidence of significant events2121 Picano E, Mathias W Jr, Pingitore A, Bigi R, Previtali M. Safety and tolerability of dobutamine-atropine stress echocardiography: a prospective, multicenter study. Lancet. 1994;344(8931):1190-2. (around 0,5%).2121 Picano E, Mathias W Jr, Pingitore A, Bigi R, Previtali M. Safety and tolerability of dobutamine-atropine stress echocardiography: a prospective, multicenter study. Lancet. 1994;344(8931):1190-2.,2222 Cortigiani L, Bigi R, Gigli G, Coletta C, Mariotti E, Dodi C, et al. Prognostic implications of intraventricular conduction defects in patients undergoing stress echocardiography for suspected coronary artery disease. Am J Med. 2003;115(1):12-8. This method has favorable sensitivity (77-89%) and specificity (68-93%) not only in the post-infarction phase,2323 Salustri A, Elhendy A, Garyfallidis P, Ciavatti M, Cornel JH, ten Cate FJ, et al. Prediction of improvement of ventricular function after acute myocardial infarction using low-dose dobutamine stress echocardiography. Am J Cardiol. 1994;74(9):853-6.,2424 Elhendy A, Trocino G, Salustri A, Cornel JH, Roelandt JR, Boersma E, et al. Low-dose dobutamine echocardiography and rest-redistribution thallium-201 tomography in the assessment of spontaneous recovery of left ventricular function after recent myocardial infarction. Am Heart J. 1996;131(6):1088-96. but also in the chronic phase (82% and 92%, respectively), as shown by Marzullo et al.2525 Marzullo P, Parodi O, Reisenhofer B, Sambuceti G, Picano E, Distante A, et al. Value of rest - thallium-201/technetium-99 sestamibi and dobutamine echocardiography for detecting myocardial viability. Am J Cardiol. 1993;71(2):166-72.
Assessment of myocardial viability using baseline-nitrate (99m)Tc-Sestamibi scintigraphy
Myocardial perfusion scintigraphy using nitrate-augmented (99m)Tc-Sestamibi is a widely available method for assessment of myocardial viability. The use of nitrates enables the improvement of blood flow in narrowed and collateral vessels, responsible for irrigation of hypoperfused areas, which potentiates the ability of the method to detect viable tissues, especially when combined with (99m)Tc-Sestamibi.1111 Demirkol MO. Myocardial viability testing in patients with severe left ventricular dysfunction by SPECT and PET. Anadolu Kardiyol Derg. 2008 Nov;8 Suppl 2:60-70. This is assured by the fact that both absorption and retention of sestamibi depend on perfusion, cell membrane integrity and membrane potential (mitochondrial function), which hence constitute the markers of viable tissue.2525 Marzullo P, Parodi O, Reisenhofer B, Sambuceti G, Picano E, Distante A, et al. Value of rest - thallium-201/technetium-99 sestamibi and dobutamine echocardiography for detecting myocardial viability. Am J Cardiol. 1993;71(2):166-72.
26 Schinkel AF, Poldermans D, Elhendy A, Bax JJ. Assessment of myocardial viability in patients with heart failure. J Nucl Med. 2007;48(7):1135-46.-2727 Giogetti A, Marzullo P, Sambuceti G, Di Quirico S, Kusch A, Landi P, et al; Baseline/postnitrate Tc-99m tetrofosmin mismatch for the assessment of myocardial viability in patients with severe left ventricular dysfunction: comparison with baseline Tc-99m tetrofosmin scintigraphy/FDG PET imaging. J Nucl Cardiol. 2004;11(12):142-51. Schinkel AF et al.2828 Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32(7):375-410. reported a 81% sensitivity and 69% specificity of nitrate-enhanced (99m)Tc-Sestamibi scintigraphy to detect viability, which is lower than those reported with the use of PET-1818 Arai AE. Myocardial infarction and viability with an emphasis on imaging delayed enhancement. In: Kwong RY. (ed.). Cardiovascular magnetic resonance imaging. Totowa (NJ): Humana Press Inc; 2008. p. 351-75.F-FDG.2828 Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32(7):375-410. In Figure 1, we illustrate a case where rest perfusion defect, initially attributed to the infarction area, normalized after treatment of the coronary obstruction in the anterior descending artery, demonstrating a viable myocardium. These findings illustrate a practical limitation of imaging techniques using (99m)Tc-Sestamibi in the detection of myocardial fibrosis and viability.
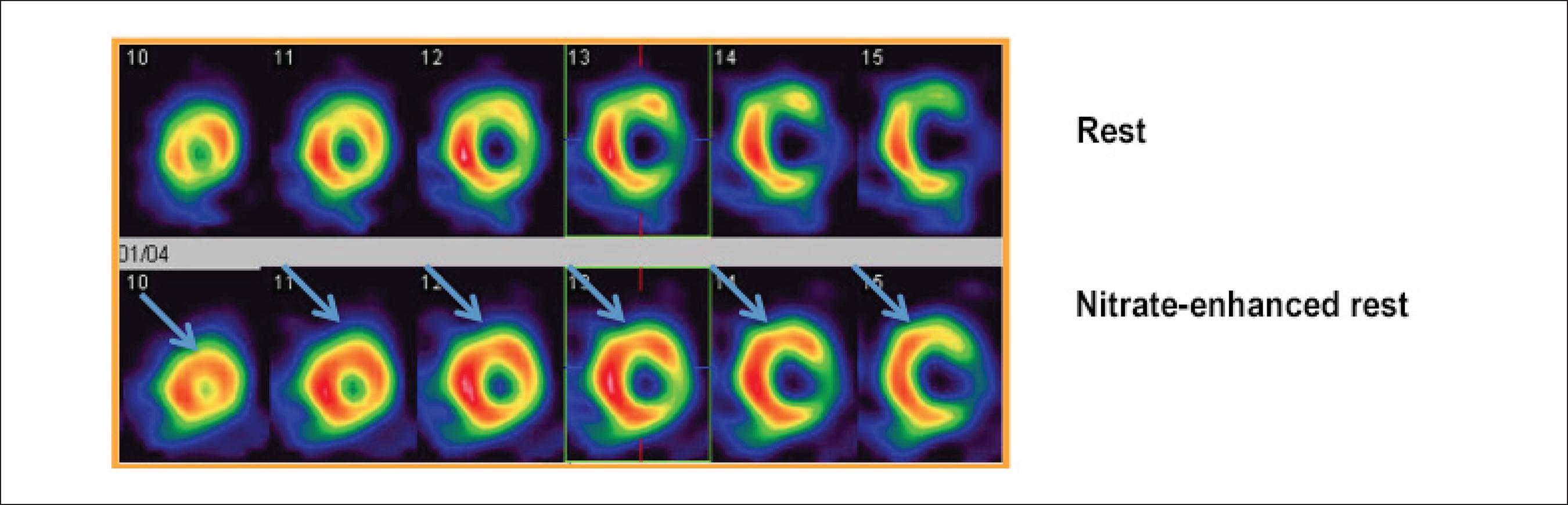
In most studies on baseline-nitrate (99m)Tc-Sestamibi scintigraphy, two patterns of images are commonly obtained: rest images and nitrate-enhanced images. Reversibility of the lesion (by filling) is indicative of viability. Sciagra et al.2929 Sciagra R, Pellegri M, Pupi A, Bolognese L, Bisi G, Carnovale V, et al. Prognostic implications of Tc-99m sestamibi viability imaging and subsequent therapeutic strategy in patients with chronic coronary artery disease and left ventricular dysfunction. J Am Coll Cardiol. 2000;36(3):739-45. studied 105 patients with chronic CAD and left ventricular dysfunction who underwent baseline-nitrate sestamibi perfusion imaging and showed that the most powerful prognostic predictors of events were the number of nonrevascularized dysfunctional areas with viability in sestamibi imaging2828 Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32(7):375-410.,2929 Sciagra R, Pellegri M, Pupi A, Bolognese L, Bisi G, Carnovale V, et al. Prognostic implications of Tc-99m sestamibi viability imaging and subsequent therapeutic strategy in patients with chronic coronary artery disease and left ventricular dysfunction. J Am Coll Cardiol. 2000;36(3):739-45. (Figure 2).
Images of rest (upper line) and nitrate-enhanced rest (lower line) myocardial perfusion scintigraphy, showing improvement of perfusion in anterior (apical, medial and basal) and anterolateral (medial and basal) segments.
Assessment of myocardial viability with 201Tálio
201Tálio has some limitations for routine use, due to its longer physical half-life, and relatively low photon energy and flow. This may yield images with low count-rates and possible attenuation artifacts and, consequently, suboptimal images.44 Zaret BL, Beller GA. Clinical Nuclear Cardiology: state of the heart and future directions. 4th ed. Amsterdam: Elsevier; 2006 p. 31-4, 495-555.
However, 201Tálio has the advantage of entering myocardial cells by active transportation, which increases its accuracy for detecting viable myocardium. For this purpose, two protocols are usually used - stress-redistribution-reinjection and rest-redistribution imaging. While the first is focused on data about stress-induced ischemia and viability, the second focuses only on viability2626 Schinkel AF, Poldermans D, Elhendy A, Bax JJ. Assessment of myocardial viability in patients with heart failure. J Nucl Med. 2007;48(7):1135-46. (Figure 3).
Myocardial perfusion scintigraphy with 201Tálio for assessment of myocardial viability; stress imaging (upper line) and 24-hour redistribution imaging after injection of the radiotracer 201Tálio (lower line), showing improvement of perfusion in anterior (apical, medial and basal) and anterolateral (medial and basal) segments.
201Tálio perfusion scintigraphy may show different perfusion defects that vary within a range from totally reversible to irreversible, according to the degree of improvement in the activity of late images.77 Fernandes H, Sousa A, Campos J, Patrício J, Oliveira A, Vieira T, et al. [Myocardial viability assessment]. Acta Med Port. 2011 Dec;24 Suppl 4:989-94.
In a meta-analysis, Schinkel et al. reported an 87% sensitivity and 54% specificity in predicting post-revascularization recovery.2828 Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32(7):375-410. Some studies have suggested that improvement in systolic function is not a sine qua non for clinical benefits, with a better prognosis but no improvement in the ejection fraction of some patients.44 Zaret BL, Beller GA. Clinical Nuclear Cardiology: state of the heart and future directions. 4th ed. Amsterdam: Elsevier; 2006 p. 31-4, 495-555.,1111 Demirkol MO. Myocardial viability testing in patients with severe left ventricular dysfunction by SPECT and PET. Anadolu Kardiyol Derg. 2008 Nov;8 Suppl 2:60-70.,2626 Schinkel AF, Poldermans D, Elhendy A, Bax JJ. Assessment of myocardial viability in patients with heart failure. J Nucl Med. 2007;48(7):1135-46.,2828 Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32(7):375-410.
Assessment of myocardial viability using positron emission tomography with fluorine-18-deoxyglucose (18F-FDG PET)
Among the methods available for assessment of myocardial viability, 18F-FDG PET is considered the gold standard method.3030 Tillisch J, Brunken R, Marshall R, Schwaiger M, Mandelkern M, Phelps M, et al. Reversibility of cardial wall-motion abnormalities predicted by positron tomography. N Engl J Med. 1986;314(14):884-8.,3131 Maddahi J, Schelbert H, Brunken R, Di Carli M. Role of thallium-201 and PET imaging in evaluation of myocardial viability and management of patients with coronary artery disease and left ventricular dysfunction. J Nucl Med. 1994;35(4):707-15. Because 18F-FDG is a glucose analog, it is used to evaluate the metabolism of cardiac glucose, and thereby the uptake of this marker is similar to glucose utilization by myocytes.44 Zaret BL, Beller GA. Clinical Nuclear Cardiology: state of the heart and future directions. 4th ed. Amsterdam: Elsevier; 2006 p. 31-4, 495-555.
In fasting conditions, myocardium uses preferentially free fatty acids as energy source, whereas in post-prandial phase, its metabolism is shifted to glucose (with increased levels of circulating insulin).55 Ragosta M, Beller GA. The noninvasive assessment of myocardial viability. Clin Cardiol. 1993;16(7):531-8. As the metabolism of free fatty acids depends on oxygen, during myocardial ischemia, glucose is the preferred substrate (glycolytic pathway), which is the hallmark of myocardial viability.3535 Goldstein RA. Rubidium-82 kinetics after coronary occlusion: temporal relation net myocardial accumulation and viability in open-chested dogs. J Nucl Med. 1986;27(9):1456-61.,3232 Marshall RC, Tillisch JH, Phelps ME, Huang SC, Carson R, Henze E, et al. Identification and differentiation of resting myocardial ischemia in man with positron computed tomography, 18F-labeled fluorodeoxyglucose, and N-13 ammonia. Circulation. 1983;67(4):766-78.
33 Goldstein R, Mullani N, Wong W, Hartz RK, Hicks CH, Fuentes F, et al. Positron imaging of myocardial infarction with rubidium-82. J Nucl Med. 1986;27(12):1824-9.
34 Gould K, Goldstein R, Mullani N, Kirkeeide RL, Wong WH, Tewson TJ, et al. Noninvasive assessment of coronary stenoses by myocardial perfusion imaging during pharmacologic coronary vasodilation. VIII. Clinical feasibility of positron cardiac imaging without a cyclotron using generator-produced rubidium-82.; J Am Cardiol. 1986;7(4):775-89.-3535 Goldstein RA. Rubidium-82 kinetics after coronary occlusion: temporal relation net myocardial accumulation and viability in open-chested dogs. J Nucl Med. 1986;27(9):1456-61.
PET with 1818 Arai AE. Myocardial infarction and viability with an emphasis on imaging delayed enhancement. In: Kwong RY. (ed.). Cardiovascular magnetic resonance imaging. Totowa (NJ): Humana Press Inc; 2008. p. 351-75.F-FDG has mean sensitivity of 92% and specificity of 63% in assessing the likelihood of functional improvement of the muscle in the after revascularization. Many studies have used comparative data of perfusion and 18F-FDG uptake, defining myocardial viability as hypoperfused areas with preserved glucose metabolism.2626 Schinkel AF, Poldermans D, Elhendy A, Bax JJ. Assessment of myocardial viability in patients with heart failure. J Nucl Med. 2007;48(7):1135-46.,2828 Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32(7):375-410.,3232 Marshall RC, Tillisch JH, Phelps ME, Huang SC, Carson R, Henze E, et al. Identification and differentiation of resting myocardial ischemia in man with positron computed tomography, 18F-labeled fluorodeoxyglucose, and N-13 ammonia. Circulation. 1983;67(4):766-78.
33 Goldstein R, Mullani N, Wong W, Hartz RK, Hicks CH, Fuentes F, et al. Positron imaging of myocardial infarction with rubidium-82. J Nucl Med. 1986;27(12):1824-9.-3434 Gould K, Goldstein R, Mullani N, Kirkeeide RL, Wong WH, Tewson TJ, et al. Noninvasive assessment of coronary stenoses by myocardial perfusion imaging during pharmacologic coronary vasodilation. VIII. Clinical feasibility of positron cardiac imaging without a cyclotron using generator-produced rubidium-82.; J Am Cardiol. 1986;7(4):775-89. (Figure 4).
Myocardial perfusion scintigraphy with 99mTc-Sestamibi (upper line) and 18F-FDG PET (lower line) for assessment of myocardial viability, showing improvement in perfusion/metabolism in anterior (apical, medial and basal), apical septal, anteroseptal (medial and basal) and inferoseptal (medial and basal) segments; “mismatch” pattern.
Overall improvement of left ventricle may also be evaluated by 18F-FDG. Left ventricular ejection fraction (LVEF) improves from 37% to 47% (mean values) in patients with myocardial viability detected by 18F-FDG PET after revascularization. In patients without viable myocardium, LVEF remained almost unchanged (39% x 40%).3131 Maddahi J, Schelbert H, Brunken R, Di Carli M. Role of thallium-201 and PET imaging in evaluation of myocardial viability and management of patients with coronary artery disease and left ventricular dysfunction. J Nucl Med. 1994;35(4):707-15.,3434 Gould K, Goldstein R, Mullani N, Kirkeeide RL, Wong WH, Tewson TJ, et al. Noninvasive assessment of coronary stenoses by myocardial perfusion imaging during pharmacologic coronary vasodilation. VIII. Clinical feasibility of positron cardiac imaging without a cyclotron using generator-produced rubidium-82.; J Am Cardiol. 1986;7(4):775-89.
35 Goldstein RA. Rubidium-82 kinetics after coronary occlusion: temporal relation net myocardial accumulation and viability in open-chested dogs. J Nucl Med. 1986;27(9):1456-61.
36 Stankewicz MA, Mansour CS, Eisner RL, Churchwell KB, Williams BR, Sigman SR, et al. Myocardial viability assessment by PET: 82Rb defect washout does not predict the results of metabolic-perfusion mismatch. J Nucl Med. 2005;46(10):1602-9.
37 Sampson UK, Dorbala S, Limaye A, Di Carli MF. Diagnostic accuracy of rubidium-82 myocardial perfusion imaging with hybrid positron emission tomography/computed tomography in the detection of coronary artery disease. J Am Coll Cardiol. 2007;49(10):1052-8.
38 Knesaurek K, Machac J, Krynyckyi BR, Almeida OD. Comparison of 2- dimensional and 3-dimensional 82Rb myocardial perfusion PET imaging. J Nucl Med. 2003;44(8):1350-6.-3939 Krivokapich J, Smith GT, Huang SC, Hoffman EJ, Ratib O, Phelps ME, et al. 13N ammonia myocardial imaging at rest and with exercise in normal volunteers: quantification of absolute myocardial perfusion with dynamic positron emission tomography. Circulation. 1989;80(5):1328-37.
Assessment of myocardial viability with computed tomography (CT)
CT is the most recent and widely used method for coronary angiography. Three techniques are currently used for cardiac CT - coronary angiography, CT with iodinated and non-contrast CT - and all of them can provide information on myocardial viability.4040 Van den Hoff J, Burchert W, Borner AR, Fricke H, Kuhnel G, Meyer GJ, et al. [1-(11)C] acetate as a quantitative perfusion tracer in myocardial PET. J Nucl Med. 2001;42(8):1174-82.
41 Partington SL, Kwong RY, Dorbala S. Multimodality imaging in the assessment of myocardial viability. Heart Fail Rev. 2011;16(4):381-95.-4242 Achenbach S. Cardiac CT: state of the art for the detection of coronary arterial stenosis. J Cardiovasc Comput Tomogr. 2007;1(1):3-20.
CT coronary angiography has high negative predictive value (> 95%) in excluding epicardial CAD, with increasing role in the assessment of chest pain. It may also provide valuable information in the evaluation of patients with left ventricular systolic dysfunction, with suspected congenital heart disease or coronary anomaly.4242 Achenbach S. Cardiac CT: state of the art for the detection of coronary arterial stenosis. J Cardiovasc Comput Tomogr. 2007;1(1):3-20.
Delayed enhancement CT uses a similar principle to gadolinium-based magnetic resonance (MR) imaging for imaging studies of myocardial scarring. In CT, the use of iodinated contrast causes an increase in Hounsfield units in contrasted tissues, due to attenuation of X-rays, allowing the visualization of cardiac muscle in the early arterial phase, and discrimination of macro and microvascular obstruction. When evaluated 5-10 minutes after injection of iodinated contrast and increased enhancement, the obstruction is suggestive of infarction, due to extracellular contrast accumulation.4141 Partington SL, Kwong RY, Dorbala S. Multimodality imaging in the assessment of myocardial viability. Heart Fail Rev. 2011;16(4):381-95.,4242 Achenbach S. Cardiac CT: state of the art for the detection of coronary arterial stenosis. J Cardiovasc Comput Tomogr. 2007;1(1):3-20.
Finally, non-contrast CT can reveal calcified aneurysms in the left ventricle, for showing similar images to those obtained during attenuation correction scans or calcium scoring.4141 Partington SL, Kwong RY, Dorbala S. Multimodality imaging in the assessment of myocardial viability. Heart Fail Rev. 2011;16(4):381-95.,4242 Achenbach S. Cardiac CT: state of the art for the detection of coronary arterial stenosis. J Cardiovasc Comput Tomogr. 2007;1(1):3-20.
Some advantages of cardiac CT include the possibility of being performed in combination with coronary CT, requiring only the addition of some minutes to the angiography protocol; its high spatial resolution, being of great importance in evaluation of small infarctions; near-isotropic resolution and reliable 3D data reconstruction for the small slide thickness; possibility of inclusion of patients with pacemakers and other metallic devices. As disadvantages, we can mention the necessity of higher radioactive emission for acquisition of additional images following coronary images, and poorer localization ability and transmurality as compared with CMR.4343 Brodoefel H, Klumpp B, Reimann A, Fenchel M, Heuschmid M, Miller S, et al. Sixty-four-MSCT in the characterization of porcine acute and subacute myocardial infarction: determination of transmurality in comparison to magnetic resonance imaging and histopathology. Eur J Radiol. 2007;62(2):235-46.
Assessment of myocardial viability with MR imaging
MR is a highly efficient method for myocardial viability study2626 Schinkel AF, Poldermans D, Elhendy A, Bax JJ. Assessment of myocardial viability in patients with heart failure. J Nucl Med. 2007;48(7):1135-46. and has played an important role in the clinical practice. It has also been considered a gold standard method in the assessment of left ventricular function. MR allows assessment of left ventricular dysfunction associated with chronic ischemic disease by evaluation of contractile reserve using dobutamine at low dose and, most importantly, evaluation of fibrosis by late gadolinium enhancement. In a metanalysis, Romero et al.4444 Romero J, Xue X, Gonzalez W, Garcia MJ. CMR imaging assessing viability in patients with chronic ventricular dysfunction due to coronary artery disease: a meta-analysis of prospective trials. JACC Cardiovasc Imaging. 2012;5(5):494-508. concluded that MR with low-dose dobutamine has high sensitivity and specificity (81% and 91%, respectively), whereas late gadolinium enhancement MR has 95% sensitivity and 51% specificity, and high accuracy in determining some parameters, including ejection fraction, left ventricular volume, regional wall motion, and myocardial thickness.4545 Hammermeister KE, DeRouen TA, Dodge HT. Variables predictive of survival in patients with coronary disease: selection by univariate and multivariate analyses from the clinical, electrocardiographic, exercise, arteriographic, and quantitative angiographic evaluations. Circulation. 1979;59(3):421-30.,4646 Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343(20):1445-53. Left ventricular wall thickness at end diastole is important to exclude viability.
The most notable characteristic of MR is its high spatial resolution, and, for this reason, the method stands out for its high imaging quality and capacity to diagnose ischemic areas that would not be detectable by other methods. MR may also be particularly useful in the assessment of myocardial blood flow at rest in hibernating areas of narrowed coronary artery and improvement of local myocardial contractility after coronary revascularization.1313 Selvanayagam JB, Jerosch-Herold M, Porto I, Sheridan D, Cheng AS, Petersen SE, et al. Resting myocardial blood flow is impaired in hibernating myocardium: a magnetic resonance study of quantitative perfusion assessment. Circulation. 2005;112(21):3289-96.,4747 Selvanayagam JB, Kardos A, Francis JM, Wiesmann F, Petersen SE, Taggart DP, et al. Value of delayed-enhancement cardiovascular magnetic resonance imaging in predicting myocardial viability after surgical revascularization. Circulation. 2004;110(12):1535-41.
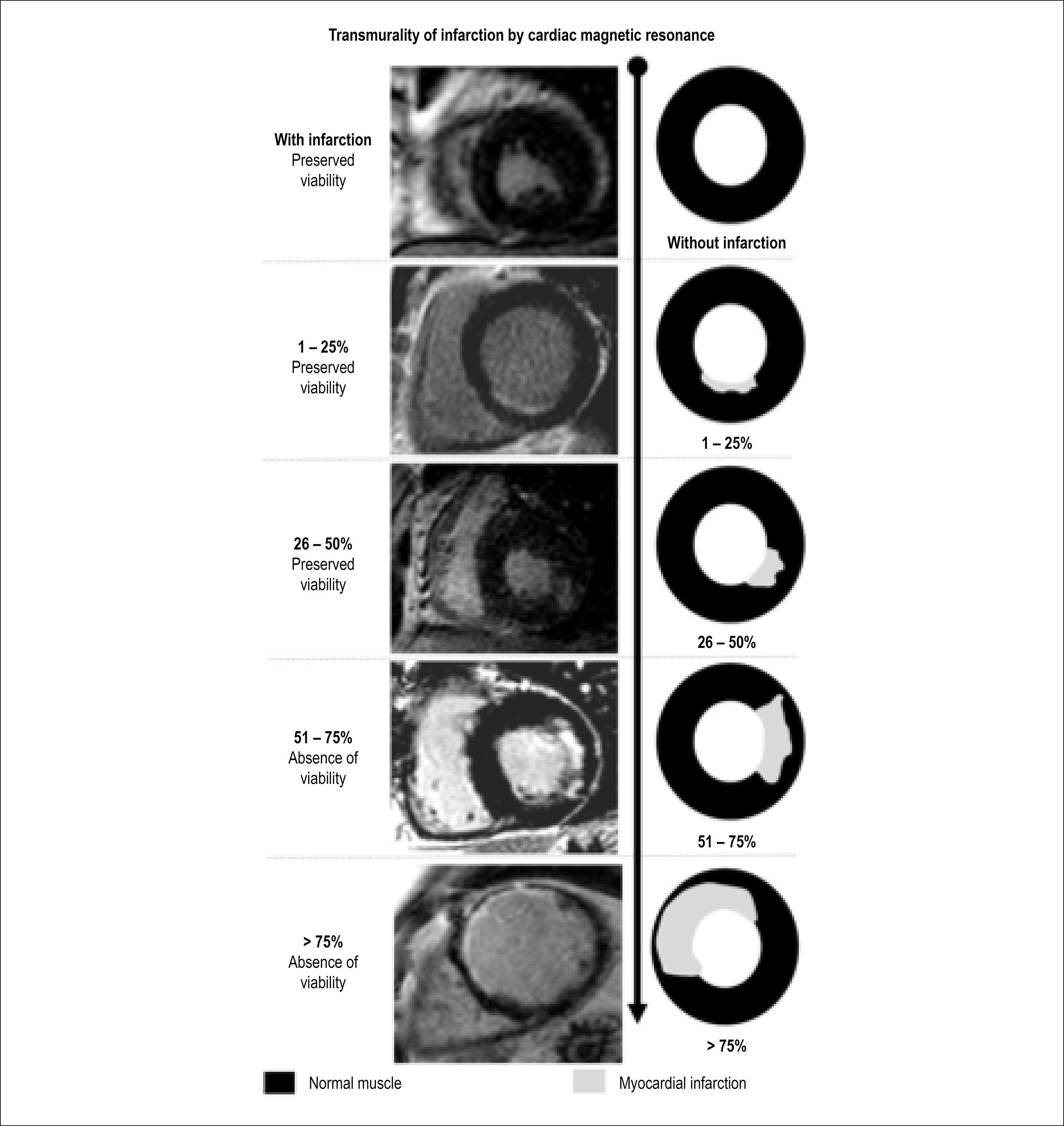
The use of gadolinium as a contrast medium in MR allows the detection of the effects of perfusion, microvascular obstruction and differentiation between transmural and subendocardial necrosis.4848 Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, et al. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218(1):215-23. Gadolinium has a low risk of nephrotoxicity, except for patients with end-stage renal disease, in which the risk of systemic toxicity is real. Although chelated-gadolinium compounds are distributed in the extracellular space, and do not penetrate in intact cells, they may accumulate in myocytes with ruptured cell membrane (e.g. acute myocardial infarction) and fibrotic areas1010 Camici PG, Prasad SK, Rimoldi OE. Stunning, hibernation, and assessment of myocardial viability. Circulation. 2008;117(1):103-14. (Figure 5).
Patterns of transmurality of infarction in the presence and absence of viability by cardiac magnetic resonance
The likelihood of functional recovery after revascularization is proportional to the transmurality of acute myocardial infarction. A very important marker of improvement of myocardial function is the amount of delayed enhancement by MR imaging since there is a progressive improvement in myocardial function with the increase of transmurality of scar tissue. Kim et al.4646 Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343(20):1445-53. evaluated the ability of contrast-enhanced MR imaging to predict functional recovery after revascularization. Approximately 80% of segments with less than 25% of transmural fibrosis had functional recovery after revascularization, whereas only 10% of the segments with transmurality higher than 50% recovered after revascularization. Selvanayagam et al.4747 Selvanayagam JB, Kardos A, Francis JM, Wiesmann F, Petersen SE, Taggart DP, et al. Value of delayed-enhancement cardiovascular magnetic resonance imaging in predicting myocardial viability after surgical revascularization. Circulation. 2004;110(12):1535-41. showed that delayed-enhancement cardiovascular MR imaging is a strong predictor of myocardial viability after surgical revascularization.
Left ventricular wall thickness may reveal valuable information about viability. Schinkel et al.2626 Schinkel AF, Poldermans D, Elhendy A, Bax JJ. Assessment of myocardial viability in patients with heart failure. J Nucl Med. 2007;48(7):1135-46. showed that segments with an end-diastolic wall thickness of less than 5 mm was associated with higher likelihood of recovery after revascularization.
Taken together, these findings suggest that segments with an end-diastolic wall thickness of less than 5.5 mm never show recovery of function after revascularization, which may be related to the presence of nontransmural infarction. These segments contain subendocardial scar tissue, with residual viability in the epicardium. Therefore, significant wall thinning indicates scar tissue, with low likelihood of recovery after revascularization; nevertheless, evidence suggests that recovery of function may occur, but only when contrast-enhanced MR excludes scar tissue.1010 Camici PG, Prasad SK, Rimoldi OE. Stunning, hibernation, and assessment of myocardial viability. Circulation. 2008;117(1):103-14.
Geber et al.4949 Gerber BL, Rousseau MF, Ahn SA, le Polain de Waroux JB, Pouleur AC, Phlips T, et al. Prognostic value of myocardial viability by delayed-enhanced magnetic resonance in patients with coronary artery disease and low ejection fraction: impact of revascularization therapy. J Am Coll Cardiol. 2012;59(9):825-35 demonstrated that cardiac MR was important in identifying patients with ischemic cardiomyopathy and severe left ventricular dysfunction who would benefit from myocardial revascularization. CMR can be performed in ischemic cardiomyopathy with left ventricular dysfunction to characterize myocardial viability.5050 Sara L, Szarf G, Tachibana A, Shiozaki AA, Villa AV, de Oliveira AC, et al; Sociedade Brasileira de Cardiologia, Colegio Brasileiro de Radiologia. [II Guidelines on Cardiovascular Magnetic Resonance and Computed Tomography of the Brazilian Society of Cardiology and the Brazilian College of Radiology]. Arq Bras Cardiol. 2014;103(6 Suppl 3):1-86. Limitations of this technique, however, include its high cost, difficulty of performing scans in patients with implanted devices, and limited availability.1010 Camici PG, Prasad SK, Rimoldi OE. Stunning, hibernation, and assessment of myocardial viability. Circulation. 2008;117(1):103-14.
PET-RM
A new technique - PET-MR started to be studied, but still has limited availability. The method has the advantage of combining the high spatial resolution of MR with the sensitivity of PET, without excessive ionizing radiation. In contrast to PET-CT, however, the synergism between PET and MR still need to be evaluated.
Comparison of left ventricular end-diastolic wall thickness on MRI with glucose use on 1818 Arai AE. Myocardial infarction and viability with an emphasis on imaging delayed enhancement. In: Kwong RY. (ed.). Cardiovascular magnetic resonance imaging. Totowa (NJ): Humana Press Inc; 2008. p. 351-75.F-FDG PET demonstrated that regions with an end-diastolic wall thickness of less than 5.5 mm had reduced glucose use, whereas regions with a wall thickness of 5.5 mm did not use this carbohydrate.5151 Klein C, Nekolla SG, Bengel FM, Momose M, Sammer A, Haas F, et al. Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: comparison with positron emission tomography. Circulation. 2002;105(2):162-7. Studies on usefulness of PET-MR in cardiology are still ongoing, but it includes specific localization of lesions, contributing to therapeutic intervention.5252 Pohle K, Notni J, Bussemer J, Kessler H, Schwaiger M, Beer AJ. 68Ga-NODAGA-RGD is a suitable substitute for 18FGalacto-RGD and can be produced with high specific activity in a cGMP/GRP compliant automated process. Nucl Med Biol. 2012;39(6):777-84. Preliminary data indicate the possibility of PET-MR to measure inflammatory response to myocardial infarction and neoangiogenesis.5252 Pohle K, Notni J, Bussemer J, Kessler H, Schwaiger M, Beer AJ. 68Ga-NODAGA-RGD is a suitable substitute for 18FGalacto-RGD and can be produced with high specific activity in a cGMP/GRP compliant automated process. Nucl Med Biol. 2012;39(6):777-84.,5353 Higuchi T, Nekolla SG, Jankaukas A, Weber AW, Huisman MC, Reder S, et al. Characterization of normal and infarcted rat myocardium using a combination of small-animal PET and clinical MRI. J Nucl Med. 2007;48(2):288-94. While MR is helpful in the analysis of scar extension, PET provides characteristics of the subepicardium and likelihood of functional recovery of areas free of scars.5151 Klein C, Nekolla SG, Bengel FM, Momose M, Sammer A, Haas F, et al. Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: comparison with positron emission tomography. Circulation. 2002;105(2):162-7.
Comparison between the techniques:
For practical purposes, the most appropriate methods for viability assessment are those in which the clinician or the institution have the highest experience. Echocardiography with dobutamine has, in general, high positive predictive value, and thus, is relatively more specific whereas nuclear medicine techniques are more sensitive to diagnosis, with a significative negative predictive value, as can be seen in the study by Panza et al.,5454 Panza JA, Dilsizian V, Laurienzo JM, Curiel RV, Katsiyiannis PT. Relation between thallium uptake and contractile response to dobutamine: implications regarding myocardial viability in patients with chronic coronary artery disease and left ventricular dysfunction. Circulation. 1995;91(4):990-8. who compared the echocardiography and 201Tálio myocardial scintigraphy methods. Hakimeh et al.5555 Sadeghian H, Majd-Ardakani J, Lotfi-Tokaldany M, Jahangiri C, Fathollahi MS. Comparison between dobutamine stress echocardiography and myocardial perfusion scan to detect viable myocardium in patients with coronary artery disease and low ejection fraction. Hellenic J Cardiol. 2009;50(1):45-51. evaluated viable kinetic segments by resting (99m)Tc-Sestamibi, and observed that the number of these segments was significantly greater than those showing a contractile response to dobutamine. Hence, due to its greater accessibility, echocardiography may be the method of choice in the screening for the presence of viability, and in a second line of investigation, a nuclear method could be used.5656 Pagano D, Bonser RS, Townend JN, Ordoubadi F, Lorenzoni R, Camici PG. Predictive value of dobutamine echocardiography and positron emission tomography in identifying hibernating myocardium in patients with postischaemic heart failure. Heart. 1998;79(3):281-8.
(99m)Tc-Sestamibi has been used as an alternative to 201Tálio for its higher quality combined with lower exposure to radiation. In cases when (99m)Tc-Sestamibi imaging are not conclusive, or when greater viability is still clinically possible, the use of 201Tálio is indicated for its higher detection rate, especially in severe hypoperfusion areas.2525 Marzullo P, Parodi O, Reisenhofer B, Sambuceti G, Picano E, Distante A, et al. Value of rest - thallium-201/technetium-99 sestamibi and dobutamine echocardiography for detecting myocardial viability. Am J Cardiol. 1993;71(2):166-72.
An excellent method for assessment of hibernating myocardium is 18F-FDG PET, for its higher sensitivity in detecting dysfunctional, but viable, myocardium. Although a sensitivity of 93% was shown for this technique in a metanalysis,3535 Goldstein RA. Rubidium-82 kinetics after coronary occlusion: temporal relation net myocardial accumulation and viability in open-chested dogs. J Nucl Med. 1986;27(9):1456-61. other authors reported a lower specificity (58%).5757 Barrington SF, Chambers J, Hallett WA, O’Doherty MJ, Roxburgh JC, Nunan TO. Comparison of sestamibi, thallium, echocardiography and PET for the detection of hibernating myocardium. Eur J Nucl Med Mol Imaging. 2004;31(3):355-61.
58 Rahimtoola SH. Concept and evaluation of hibernating myocardium. Annu Rev Med. 1999;50:75-86.-5959 Beller GA, Ragosta M. Extent of myocardial viability in regions of left ventricular dysfunction by rest-redistribution thallium-201 imaging: a powerful predictor of outcome.; J Nucl Cardiol. 1998;5(4):445-8.
With respect to MR and nuclear medicine techniques, comparison of contrast MR imaging, with dobutamine echocardiography and 201Tálio rest-redistribution showed an agreement of 83% and 75%, respectively.6060 Ramani K, Judd RM, Holly TA, Parrish TB, Rigolin VH, Parker MA, et al. Contrast magnetic resonance imaging in the assessment of myocardial viability in patients with stable coronary artery disease and left ventricular dysfunction.; Circulation. 1998;98(24):2687-94. Klein et al.5151 Klein C, Nekolla SG, Bengel FM, Momose M, Sammer A, Haas F, et al. Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: comparison with positron emission tomography. Circulation. 2002;105(2):162-7. showed a good agreement between contrast MR and 1818 Arai AE. Myocardial infarction and viability with an emphasis on imaging delayed enhancement. In: Kwong RY. (ed.). Cardiovascular magnetic resonance imaging. Totowa (NJ): Humana Press Inc; 2008. p. 351-75.F-FDG PET; in patients with CAD and severely reduced LVEF, MR imaging can identify fibrotic areas with results similar to those obtained by PET measurements, provided by comparison of flow and glucose metabolism. MR also provides other parameters of tissue viability, such as wall thickness, contractile reserve and delayed enhancement.5959 Beller GA, Ragosta M. Extent of myocardial viability in regions of left ventricular dysfunction by rest-redistribution thallium-201 imaging: a powerful predictor of outcome.; J Nucl Cardiol. 1998;5(4):445-8.
60 Ramani K, Judd RM, Holly TA, Parrish TB, Rigolin VH, Parker MA, et al. Contrast magnetic resonance imaging in the assessment of myocardial viability in patients with stable coronary artery disease and left ventricular dysfunction.; Circulation. 1998;98(24):2687-94.
61 Lee VS, Resnick D, Tiu SS, Sanger JJ, Nazzaro CA, Israel GM, et al. MR imaging evaluation of myocardial viability in the set of equivocal SPECT results with 99m Tc-sestamibi. Radiology. 2004;230(1):191-7.-6262 Alderman EL, Fisher LD, Litwin P, Kaiser GC, Myers WO, Maynard C, et al. Results of coronary artery surgery in patients with poor left ventricular function (CASS). Circulation. 1983;68(4):785-95.
In addition, in comparison with CT, MR has higher contrast resolution for soft tissues, without requiring radiation exposure. CT and PET4141 Partington SL, Kwong RY, Dorbala S. Multimodality imaging in the assessment of myocardial viability. Heart Fail Rev. 2011;16(4):381-95. may be an alternative test to MR for patients with pacemakers, implantable cardioverter defibrillator or mechanical cardiac valve. Table 1 summarizes the comparison between these methods of assessment of myocardial viability.
Prognosis:
Observational studies have suggested that the presence of viable myocardium is directly associated with favorable progress of left ventricular function and good prognosis after revascularization. Patients who seem to benefit more from surgical revascularization are those with ischemic symptoms and severe left ventricular dysfunction. A significant perioperative risk should be considered in relation to long-term benefits on mortality.6262 Alderman EL, Fisher LD, Litwin P, Kaiser GC, Myers WO, Maynard C, et al. Results of coronary artery surgery in patients with poor left ventricular function (CASS). Circulation. 1983;68(4):785-95.
63 Velazquez EJ, Lee KL, Jones RH, Al-Khalidi HR, Hill JA, Panza JA, et al; STICHES Investigators. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy.; N Engl J Med. 2016;374(16):1511-20.
64 Shah B.N.; Khattar R.S.; Senior R.; The hibernating myocardium: current concepts, diagnostic dilemmas, and clinical challenges in the post-STICH era.; Eur Heart J 2013;34:1323-36
65 Desideri A.; Cortigiani L.; Christen A.I.; et al.; The extent of perfusion-F18-fluorodeoxyglucose positron emission tomography mismatch determines mortality in medically treated patients with chronic ischemic left ventricular dysfunction.; J Am Coll Cardiol 2005;46:1264-9.-6666 Van Loon, R.B.; Veen G.; Baur L. HB; Kamp O.; Bronzwaer J. GF.; Twisk J. W. R.; Verheugt F. WA; Van Rossum, A. C.; Improved clinical outcome after invasive management of patients with recent myocardial infarction and proven myocardial viability: primary results of a randomized controlled trial (VIAMI-trial); Trials 2012, 13:1
Comparison of randomized studies of miocardial viability
Today, there is little evidence of randomized studies on this theme, with conflicting results.
Stich trial
Randomized, multicenter study involving 1,212 patients, 601 assessed for myocardial viability by dobutamine echocardiography (130 patients), SPECT (321 patients) or both (150 patients).6767 Peter Carson P.; Wertheimer J.; Alan Miller A.; O’Connor C. M.; Ileana L. Pina I. L.; Selzman C.; Sueta C.; She L.; Greene D.; Lee K. L.; Jones R. H.; Velazquez E. J.; for the STICH Investigators; The STICH Trial (Surgical Treatment for Ischemic Heart Failure); JACC: Heart Failure, Vol.1, No. 5, 2013. In the myocardial viability study, 298 patients were randomly allocated to receive conservative treatment plus surgical revascularization, and 303 patients to receive pharmacological therapy alone. Median follow-up period was 56 months (12 months - 100 months).6767 Peter Carson P.; Wertheimer J.; Alan Miller A.; O’Connor C. M.; Ileana L. Pina I. L.; Selzman C.; Sueta C.; She L.; Greene D.; Lee K. L.; Jones R. H.; Velazquez E. J.; for the STICH Investigators; The STICH Trial (Surgical Treatment for Ischemic Heart Failure); JACC: Heart Failure, Vol.1, No. 5, 2013. No statistically significant benefit of surgical intervention on mortality, or of assessment of myocardial viability on surgical intervention, suggesting that investigation of a viable myocardium do not differentiate patients who would benefit from revascularization from those who would benefit from medical therapy alone.6767 Peter Carson P.; Wertheimer J.; Alan Miller A.; O’Connor C. M.; Ileana L. Pina I. L.; Selzman C.; Sueta C.; She L.; Greene D.; Lee K. L.; Jones R. H.; Velazquez E. J.; for the STICH Investigators; The STICH Trial (Surgical Treatment for Ischemic Heart Failure); JACC: Heart Failure, Vol.1, No. 5, 2013.
Despite its limitations and biases, the STICH trial is, so far, the largest study on the influence of myocardial viability on clinical outcomes in patients with ischemic heart disease. Also, it is the first study to evaluate differential results of revascularization and pharmacological therapy.6767 Peter Carson P.; Wertheimer J.; Alan Miller A.; O’Connor C. M.; Ileana L. Pina I. L.; Selzman C.; Sueta C.; She L.; Greene D.; Lee K. L.; Jones R. H.; Velazquez E. J.; for the STICH Investigators; The STICH Trial (Surgical Treatment for Ischemic Heart Failure); JACC: Heart Failure, Vol.1, No. 5, 2013.
PARR-2 Trial
Study designed to evaluate the efficacy of 18F-FDG PET in patients with left ventricular dysfunction, by risk stratification and identification of those who would benefit from myocardial revascularization. A total of 430 patients with LVEF < 35% and CAD were allocated into two groups - standard care (n = 212) and treatment assisted by 18F-FDG PET (n = 218).6868 Beanlands R.S.B.; Nichol G.; Huszti E.; et al.; PARR-2 Investigators. F-18-fluorodeoxyglucose positron emission tomography imaging-assisted management of patients with severe left ventricular dysfunction and suspected coronary disease: a randomized, controlled trial (PARR-2).; J Am Coll Cardiol 2007;50:2002-12.
At one year, the PARR-2 trial did not show a significant difference between the groups in the primary outcomes that included death for cardiac causes, acute myocardial infarction or hospital stays for cardiac cause (30% vs. 36% p = 0.15). In PET group, however, there was a significant decrease in primary outcome over the follow-up period (relative risk 0.62; 95% CI 0.42 - 0.93; p = 0.019).6868 Beanlands R.S.B.; Nichol G.; Huszti E.; et al.; PARR-2 Investigators. F-18-fluorodeoxyglucose positron emission tomography imaging-assisted management of patients with severe left ventricular dysfunction and suspected coronary disease: a randomized, controlled trial (PARR-2).; J Am Coll Cardiol 2007;50:2002-12.
Perspectives
Myocardial viability is still a subject of clinical importance and a focus of clinical trials and translational science. Pathophysiological basis of left ventricular ischemic dysfunction seems to be correlated with myocardial stunning, hibernation or myocardial necrosis. Imaging methods used for assessment of viable muscular tissue have their own operational characteristics and should be appropriate to the patient’s individual characteristics. The detection of myocardial viability may be a valuable predictor of the response to revascularization and long-term prognostic and, thereby, contribute to the decision-making in the medical practice.
18F-FDG PET and CMR are considered first-choice methods for detection of viability due to their high sensitivity and specificity rates, whereas both echocardiography and myocardial scintigraphy considered acceptable methods for their wide availability and accessibility. With respect to the impact on medical practice, there are no definite studies showing the benefits of myocardial viability assessment on patients’ prognosis, which reinforce the necessity of larger studies, considering the great relevance of the theme.
-
Sources of FundingThere were no external funding sources for this study.
-
Study AssociationThis article is part of the thesis of master submitted by Wilter dos Santos Ker, from Universidade Federal Fluminense.
-
Ethics approval and consent to participateThis article does not contain any studies with human participants or animals performed by any of the authors.
References
-
1Anavekar NS, Chareonthaitawee P, Narula J, Gersh BJ. Revascularization in patients with severe left ventricular dysfunction. is the assessment of viability still viable? J Am Coll Cardiol. 2016;67(24):2874-87.
-
2Ling LF, Marwick TH, Flores DR, Jaber WA, Brunken RC, Cerqueira MD, et al. Identification of therapeutic benefit from revascularization in patients with left ventricular systolic dysfunction: Inducible ischemia versus hibernating myocardium. Circ Cardiovasc Imaging 2013;6(3):363-72.
-
3Narula J, Dawson MS, Singh BK, Amanullah A, Acio ER, Chaudhry FA, et al. Noninvasive characterization of stunned, hibernating, remodeled and nonviable myocardium in ischemic cardiomyopathy. J Am Coll Cardiol. 2000;36(6):1913-9.
-
4Zaret BL, Beller GA. Clinical Nuclear Cardiology: state of the heart and future directions. 4th ed. Amsterdam: Elsevier; 2006 p. 31-4, 495-555.
-
5Ragosta M, Beller GA. The noninvasive assessment of myocardial viability. Clin Cardiol. 1993;16(7):531-8.
-
6Solar M, Zizka J, Klzo L, Tintera J, Vizda J, Ceral J. Contrast-enhanced magnetic resonance and thallium scintigraphy in the detection of myocardial viability:a prospective comparative study. Int Heart J. 2006;47(4):521-32.
-
7Fernandes H, Sousa A, Campos J, Patrício J, Oliveira A, Vieira T, et al. [Myocardial viability assessment]. Acta Med Port. 2011 Dec;24 Suppl 4:989-94.
-
8Chareonthaitawee P, Gersh BJ, Araoz PA, Gibbons RJ. Revascularization in severe left ventricular dysfunction: the role of viability testing; J Am Coll Cardiol. 2005;46(4):567-74.
-
9Barnes E, Dutka DP, Khan M, Camici PG, Hall RJ. Effect of repeated episodes of reversible myocardial ischemia on myocardial blood flow and function in humans. Am J Physiol Heart Circ Physiol. 2002;282(5):H1603-8.
-
10Camici PG, Prasad SK, Rimoldi OE. Stunning, hibernation, and assessment of myocardial viability. Circulation. 2008;117(1):103-14.
-
11Demirkol MO. Myocardial viability testing in patients with severe left ventricular dysfunction by SPECT and PET. Anadolu Kardiyol Derg. 2008 Nov;8 Suppl 2:60-70.
-
12Lim SP, Mc Ardle BA, Beanlands RS, Hessian RC. Myocardial viability: it is still alive. Semin Nucl Med. 2014;44(5):358-74.
-
13Selvanayagam JB, Jerosch-Herold M, Porto I, Sheridan D, Cheng AS, Petersen SE, et al. Resting myocardial blood flow is impaired in hibernating myocardium: a magnetic resonance study of quantitative perfusion assessment. Circulation. 2005;112(21):3289-96.
-
14Conversano A, Walsh JF, Geltman EM, Perez JE, Bergmann SR, Gropler RJ. Delineation of myocardial stunning and hibernation by positron emission tomography in advanced coronary artery disease. Am Heart J. 1996;131(3):440-50.
-
15Canty JM Jr, Fallavollita JA. Hibernating myocardium. J Nucl Med. 2005;12(1):104-19.
-
16Vanoverschelde JL, Wijns W, Borgers M, Heyndrickx G, Depré C, Flameng W, et al. Chronic myocardial hibernation in humans: from bedside to bench. Circulation. 1997;95(7):1961-71.
-
17Bax JJ, Visser FC, Poldermans D, Elhendy A, Cornel JH, Boersma E, et al. Time course of functional recovery of stunned and hibernating segments after surgical revascularization. Circulation. 2001;104(12 Suppl 1):I314-8.
-
18Arai AE. Myocardial infarction and viability with an emphasis on imaging delayed enhancement. In: Kwong RY. (ed.). Cardiovascular magnetic resonance imaging. Totowa (NJ): Humana Press Inc; 2008. p. 351-75.
-
19Allman KC, Shaw LJ, Hachamovitch R, Udelson JE. Myocardial viability testing and impact of revascularization on prognosis in patients with coronary artery disease and left ventricular dysfunction: a meta-analysis. J Nucl Cardiol. 2002;39(7):1151-8.
-
20Pierard LA, De Landsheere CM, Berthe C, Rigo P, Kulbertus HE. Identification of viable myocardium by echocardiography during dobutamine infusion in patients with myocardial infarction after thrombolytic therapy: comparison with positron emission tomography. J Am Coll Cardiol. 1990;15(5):1021-3.
-
21Picano E, Mathias W Jr, Pingitore A, Bigi R, Previtali M. Safety and tolerability of dobutamine-atropine stress echocardiography: a prospective, multicenter study. Lancet. 1994;344(8931):1190-2.
-
22Cortigiani L, Bigi R, Gigli G, Coletta C, Mariotti E, Dodi C, et al. Prognostic implications of intraventricular conduction defects in patients undergoing stress echocardiography for suspected coronary artery disease. Am J Med. 2003;115(1):12-8.
-
23Salustri A, Elhendy A, Garyfallidis P, Ciavatti M, Cornel JH, ten Cate FJ, et al. Prediction of improvement of ventricular function after acute myocardial infarction using low-dose dobutamine stress echocardiography. Am J Cardiol. 1994;74(9):853-6.
-
24Elhendy A, Trocino G, Salustri A, Cornel JH, Roelandt JR, Boersma E, et al. Low-dose dobutamine echocardiography and rest-redistribution thallium-201 tomography in the assessment of spontaneous recovery of left ventricular function after recent myocardial infarction. Am Heart J. 1996;131(6):1088-96.
-
25Marzullo P, Parodi O, Reisenhofer B, Sambuceti G, Picano E, Distante A, et al. Value of rest - thallium-201/technetium-99 sestamibi and dobutamine echocardiography for detecting myocardial viability. Am J Cardiol. 1993;71(2):166-72.
-
26Schinkel AF, Poldermans D, Elhendy A, Bax JJ. Assessment of myocardial viability in patients with heart failure. J Nucl Med. 2007;48(7):1135-46.
-
27Giogetti A, Marzullo P, Sambuceti G, Di Quirico S, Kusch A, Landi P, et al; Baseline/postnitrate Tc-99m tetrofosmin mismatch for the assessment of myocardial viability in patients with severe left ventricular dysfunction: comparison with baseline Tc-99m tetrofosmin scintigraphy/FDG PET imaging. J Nucl Cardiol. 2004;11(12):142-51.
-
28Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis and patient outcomes. Curr Probl Cardiol. 2007;32(7):375-410.
-
29Sciagra R, Pellegri M, Pupi A, Bolognese L, Bisi G, Carnovale V, et al. Prognostic implications of Tc-99m sestamibi viability imaging and subsequent therapeutic strategy in patients with chronic coronary artery disease and left ventricular dysfunction. J Am Coll Cardiol. 2000;36(3):739-45.
-
30Tillisch J, Brunken R, Marshall R, Schwaiger M, Mandelkern M, Phelps M, et al. Reversibility of cardial wall-motion abnormalities predicted by positron tomography. N Engl J Med. 1986;314(14):884-8.
-
31Maddahi J, Schelbert H, Brunken R, Di Carli M. Role of thallium-201 and PET imaging in evaluation of myocardial viability and management of patients with coronary artery disease and left ventricular dysfunction. J Nucl Med. 1994;35(4):707-15.
-
32Marshall RC, Tillisch JH, Phelps ME, Huang SC, Carson R, Henze E, et al. Identification and differentiation of resting myocardial ischemia in man with positron computed tomography, 18F-labeled fluorodeoxyglucose, and N-13 ammonia. Circulation. 1983;67(4):766-78.
-
33Goldstein R, Mullani N, Wong W, Hartz RK, Hicks CH, Fuentes F, et al. Positron imaging of myocardial infarction with rubidium-82. J Nucl Med. 1986;27(12):1824-9.
-
34Gould K, Goldstein R, Mullani N, Kirkeeide RL, Wong WH, Tewson TJ, et al. Noninvasive assessment of coronary stenoses by myocardial perfusion imaging during pharmacologic coronary vasodilation. VIII. Clinical feasibility of positron cardiac imaging without a cyclotron using generator-produced rubidium-82.; J Am Cardiol. 1986;7(4):775-89.
-
35Goldstein RA. Rubidium-82 kinetics after coronary occlusion: temporal relation net myocardial accumulation and viability in open-chested dogs. J Nucl Med. 1986;27(9):1456-61.
-
36Stankewicz MA, Mansour CS, Eisner RL, Churchwell KB, Williams BR, Sigman SR, et al. Myocardial viability assessment by PET: 82Rb defect washout does not predict the results of metabolic-perfusion mismatch. J Nucl Med. 2005;46(10):1602-9.
-
37Sampson UK, Dorbala S, Limaye A, Di Carli MF. Diagnostic accuracy of rubidium-82 myocardial perfusion imaging with hybrid positron emission tomography/computed tomography in the detection of coronary artery disease. J Am Coll Cardiol. 2007;49(10):1052-8.
-
38Knesaurek K, Machac J, Krynyckyi BR, Almeida OD. Comparison of 2- dimensional and 3-dimensional 82Rb myocardial perfusion PET imaging. J Nucl Med. 2003;44(8):1350-6.
-
39Krivokapich J, Smith GT, Huang SC, Hoffman EJ, Ratib O, Phelps ME, et al. 13N ammonia myocardial imaging at rest and with exercise in normal volunteers: quantification of absolute myocardial perfusion with dynamic positron emission tomography. Circulation. 1989;80(5):1328-37.
-
40Van den Hoff J, Burchert W, Borner AR, Fricke H, Kuhnel G, Meyer GJ, et al. [1-(11)C] acetate as a quantitative perfusion tracer in myocardial PET. J Nucl Med. 2001;42(8):1174-82.
-
41Partington SL, Kwong RY, Dorbala S. Multimodality imaging in the assessment of myocardial viability. Heart Fail Rev. 2011;16(4):381-95.
-
42Achenbach S. Cardiac CT: state of the art for the detection of coronary arterial stenosis. J Cardiovasc Comput Tomogr. 2007;1(1):3-20.
-
43Brodoefel H, Klumpp B, Reimann A, Fenchel M, Heuschmid M, Miller S, et al. Sixty-four-MSCT in the characterization of porcine acute and subacute myocardial infarction: determination of transmurality in comparison to magnetic resonance imaging and histopathology. Eur J Radiol. 2007;62(2):235-46.
-
44Romero J, Xue X, Gonzalez W, Garcia MJ. CMR imaging assessing viability in patients with chronic ventricular dysfunction due to coronary artery disease: a meta-analysis of prospective trials. JACC Cardiovasc Imaging. 2012;5(5):494-508.
-
45Hammermeister KE, DeRouen TA, Dodge HT. Variables predictive of survival in patients with coronary disease: selection by univariate and multivariate analyses from the clinical, electrocardiographic, exercise, arteriographic, and quantitative angiographic evaluations. Circulation. 1979;59(3):421-30.
-
46Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343(20):1445-53.
-
47Selvanayagam JB, Kardos A, Francis JM, Wiesmann F, Petersen SE, Taggart DP, et al. Value of delayed-enhancement cardiovascular magnetic resonance imaging in predicting myocardial viability after surgical revascularization. Circulation. 2004;110(12):1535-41.
-
48Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, et al. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218(1):215-23.
-
49Gerber BL, Rousseau MF, Ahn SA, le Polain de Waroux JB, Pouleur AC, Phlips T, et al. Prognostic value of myocardial viability by delayed-enhanced magnetic resonance in patients with coronary artery disease and low ejection fraction: impact of revascularization therapy. J Am Coll Cardiol. 2012;59(9):825-35
-
50Sara L, Szarf G, Tachibana A, Shiozaki AA, Villa AV, de Oliveira AC, et al; Sociedade Brasileira de Cardiologia, Colegio Brasileiro de Radiologia. [II Guidelines on Cardiovascular Magnetic Resonance and Computed Tomography of the Brazilian Society of Cardiology and the Brazilian College of Radiology]. Arq Bras Cardiol. 2014;103(6 Suppl 3):1-86.
-
51Klein C, Nekolla SG, Bengel FM, Momose M, Sammer A, Haas F, et al. Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: comparison with positron emission tomography. Circulation. 2002;105(2):162-7.
-
52Pohle K, Notni J, Bussemer J, Kessler H, Schwaiger M, Beer AJ. 68Ga-NODAGA-RGD is a suitable substitute for 18FGalacto-RGD and can be produced with high specific activity in a cGMP/GRP compliant automated process. Nucl Med Biol. 2012;39(6):777-84.
-
53Higuchi T, Nekolla SG, Jankaukas A, Weber AW, Huisman MC, Reder S, et al. Characterization of normal and infarcted rat myocardium using a combination of small-animal PET and clinical MRI. J Nucl Med. 2007;48(2):288-94.
-
54Panza JA, Dilsizian V, Laurienzo JM, Curiel RV, Katsiyiannis PT. Relation between thallium uptake and contractile response to dobutamine: implications regarding myocardial viability in patients with chronic coronary artery disease and left ventricular dysfunction. Circulation. 1995;91(4):990-8.
-
55Sadeghian H, Majd-Ardakani J, Lotfi-Tokaldany M, Jahangiri C, Fathollahi MS. Comparison between dobutamine stress echocardiography and myocardial perfusion scan to detect viable myocardium in patients with coronary artery disease and low ejection fraction. Hellenic J Cardiol. 2009;50(1):45-51.
-
56Pagano D, Bonser RS, Townend JN, Ordoubadi F, Lorenzoni R, Camici PG. Predictive value of dobutamine echocardiography and positron emission tomography in identifying hibernating myocardium in patients with postischaemic heart failure. Heart. 1998;79(3):281-8.
-
57Barrington SF, Chambers J, Hallett WA, O’Doherty MJ, Roxburgh JC, Nunan TO. Comparison of sestamibi, thallium, echocardiography and PET for the detection of hibernating myocardium. Eur J Nucl Med Mol Imaging. 2004;31(3):355-61.
-
58Rahimtoola SH. Concept and evaluation of hibernating myocardium. Annu Rev Med. 1999;50:75-86.
-
59Beller GA, Ragosta M. Extent of myocardial viability in regions of left ventricular dysfunction by rest-redistribution thallium-201 imaging: a powerful predictor of outcome.; J Nucl Cardiol. 1998;5(4):445-8.
-
60Ramani K, Judd RM, Holly TA, Parrish TB, Rigolin VH, Parker MA, et al. Contrast magnetic resonance imaging in the assessment of myocardial viability in patients with stable coronary artery disease and left ventricular dysfunction.; Circulation. 1998;98(24):2687-94.
-
61Lee VS, Resnick D, Tiu SS, Sanger JJ, Nazzaro CA, Israel GM, et al. MR imaging evaluation of myocardial viability in the set of equivocal SPECT results with 99m Tc-sestamibi. Radiology. 2004;230(1):191-7.
-
62Alderman EL, Fisher LD, Litwin P, Kaiser GC, Myers WO, Maynard C, et al. Results of coronary artery surgery in patients with poor left ventricular function (CASS). Circulation. 1983;68(4):785-95.
-
63Velazquez EJ, Lee KL, Jones RH, Al-Khalidi HR, Hill JA, Panza JA, et al; STICHES Investigators. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy.; N Engl J Med. 2016;374(16):1511-20.
-
64Shah B.N.; Khattar R.S.; Senior R.; The hibernating myocardium: current concepts, diagnostic dilemmas, and clinical challenges in the post-STICH era.; Eur Heart J 2013;34:1323-36
-
65Desideri A.; Cortigiani L.; Christen A.I.; et al.; The extent of perfusion-F18-fluorodeoxyglucose positron emission tomography mismatch determines mortality in medically treated patients with chronic ischemic left ventricular dysfunction.; J Am Coll Cardiol 2005;46:1264-9.
-
66Van Loon, R.B.; Veen G.; Baur L. HB; Kamp O.; Bronzwaer J. GF.; Twisk J. W. R.; Verheugt F. WA; Van Rossum, A. C.; Improved clinical outcome after invasive management of patients with recent myocardial infarction and proven myocardial viability: primary results of a randomized controlled trial (VIAMI-trial); Trials 2012, 13:1
-
67Peter Carson P.; Wertheimer J.; Alan Miller A.; O’Connor C. M.; Ileana L. Pina I. L.; Selzman C.; Sueta C.; She L.; Greene D.; Lee K. L.; Jones R. H.; Velazquez E. J.; for the STICH Investigators; The STICH Trial (Surgical Treatment for Ischemic Heart Failure); JACC: Heart Failure, Vol.1, No. 5, 2013.
-
68Beanlands R.S.B.; Nichol G.; Huszti E.; et al.; PARR-2 Investigators. F-18-fluorodeoxyglucose positron emission tomography imaging-assisted management of patients with severe left ventricular dysfunction and suspected coronary disease: a randomized, controlled trial (PARR-2).; J Am Coll Cardiol 2007;50:2002-12.
Publication Dates
-
Publication in this collection
Mar 2018
History
-
Received
22 Aug 2017 -
Reviewed
16 Nov 2017 -
Accepted
12 Dec 2017