



This scoping review explores the current research on PTSD interventions for Natural Disaster survivors. It includes fourteen randomized control trials (RCTs). The included interventions were, pharmaceuticals, nutraceuticals, herbal supplements, CBT, yoga, narrative exposure therapy, acupuncture stimulation, web-based interventions, and a multimodal art and meditation program. CBT is considered the standard of care for general PTSD treatment and was also found to be effective for the treatment of natural disaster-related PTSD symptoms. However, higher-level clinical evidence is needed. There are inconsistencies with the use of pharmaceuticals, nutraceuticals, and herbal supplements, while there is insufficient clinical evidence to effectively determine the efficacy of yoga, acupuncture, art, and narrative exposure therapies. Factors like the availability of resources, cultural sensitivity, and values and preferences impact the effectiveness of interventions used to treat PTSD in natural disaster survivors. Clinical studies in this field need to be further expanded regardless of the study type.
Introduction
Natural disasters have a profound impact on today’s society. They are extreme events generally caused by abrupt climate change and other environmental factors such as earthquakes, landslides, volcanic eruptions, floods, hurricanes, tornadoes, blizzards, tsunamis, cyclones, and wildfires.1 Over the past decade, approximately 45,000 people globally died from natural disasters each year.2 As such, it is important to study and understand the impacts of natural disasters on the world, and thus how its effects can be overcome. Of particular importance is the mental afflictions and trauma brought upon by natural disasters. Natural disasters such as hurricanes, earthquakes, and floods can impose great stress and emotional distress on an individual, which can lead to the development of PTSD.3 PTSD, or post-traumatic stress disorder, is a syndrome that can result from natural disasters, resulting in symptoms of re-experiencing the traumatic event, intrusive thoughts, nightmares, flashbacks, dissociation (detachment from oneself or reality), and intense negative emotions (sadness, guilt) and physiological reaction on being exposed to the traumatic reminder.4 Overall, studies report a prevalence of 5% to 60% prevalence of PTSD in populations in the first 1-2 years after a natural disaster.5,6 The development of PTSD impairs natural disaster survivors’ ability to continue to engage in normal life. Because the areas where these natural disasters occur are devastated and in a state of economic distress, the loss of human capital caused by trauma from natural disasters is particularly important to address.
While systematic reviews examining the effects of interventions for PTSD in natural disasters related to specific disasters such as named tsunamis or earthquakes in particular regions, exist to date, there is currently no comprehensive scoping review available that encompasses all types of natural disasters. Considering this, further research is required to collate and vet existing literature.
Evidence shows that a scoping review is more appropriate than a systematic review when the purpose of the review is to identify knowledge gaps, scope a body of literature, clarify concepts, or investigate research conduct.7 This scoping review aimed to identify the current research outcomes that have been conducted regarding the treatment of PTSD of natural disaster survivors, the gaps presented in this field of research, and recommendations for further literature development in this field.
Methodology
The methodology employed in this scoping review aimed to adhere to the PRISMA-IPD checklist to the best extent possible. However, certain limitations should be noted, such as the non-registration of the study protocol and the absence of extensive statistical analysis. It is important to recognize that this review is designed as a scoping review rather than a systematic review and meta-analysis.
Step 1: Identifying the Research Question
During stage 1 of the scoping review, the researchers searched articles to identify research questions. After several rounds of review, the following questions were posed: [1] What is the reported effectiveness of each individual intervention studied for PTSD and Natural Disasters? [2] Which populations were targeted in RCT of natural disaster survivors with PTSD? [3] What adverse events were reported in the treatment of PTSD for Natural Disaster survivors? [4] To what extent do the interventions for PTSD in natural disasters demonstrate ease of implementation? [5] Which areas of research exhibit potential for further investigation for the treatment of PTSD in natural disaster survivors?
Step 2: Identifying Relevant Studies
Information Source: To identify the relevant studies for this scoping review, a comprehensive literature search was conducted on 3 databases including Medline and APA PsychInfo via EBSCO, and PTSDpubs on ProQuest utilizing PICOS methodology. We used Boolean search which allowed us to combine keywords.
The search terms included keywords of PTSD (ptsd or post traumatic stress disorder or posttraumatic stress disorder or post-traumatic stress disorder), natural disasters (tsunamis or floods or drought or wildfire or earthquake or tornado or hurricane or snowstorm or environmental disasters or humanitarian crisis), and treatment (intervention or therapy or management).
Eligibility Criteria: (1) Study Design: The study designs of the publications included in this scoping review were restricted solely to randomized control trials written in English, irrespective of publication date. (2) Participant Type: This review included natural disaster event survivors of all ages with PTSD and related symptoms. Studies related to war, terrorism, infectious diseases, and other man-made disasters were excluded. Studies were strictly limited to primary victims and did not include the caretakers of the victims or close family. (3) Intervention Type: All types of interventions were included in this scoping study, from pharmaceuticals to yoga to CBT. However, all studies regarding preventative measures for PTSD symptom development after a natural disaster were excluded. (4) Control Group Intervention: Any type of intervention was allowed for the control group. (5) Outcome: The outcome measures included all changes in the level of PTSD symptoms measured or if no effect was observed. Studies that mentioned anxiety or depression post-natural disaster but did not refer to ‘PTSD’ were eliminated.
Step 3: Selecting Studies to Be Included in the Review
In the third stage of the scoping review, publications were manually screened for duplicates and were assessed using the inclusion and exclusion criteria by two independent reviewers. In instances where discrepancies were identified, the reviewers took the initiative to revisit the search process, refine their strategies and conduct additional searches. This was done to ensure comprehensive coverage of the literature and facilitate collaboration to reach a consensus. The full texts of the articles were then screened for eligibility. The detailed process is shown below table.

Step 4: Charting the Data
A data extraction sheet was developed by the research team consisting of several items, including (1) general information (e.g. author’s name, year of publication, country); (2) number of participants; (3) type of disaster (e.g. hurricane, earthquake, tsunami); (4) intervention (e.g. CBT, acupuncture, yoga); (5) control; (6) median age; (7) duration of study; (8) outcome variables including effects and findings.
Step 5: Collating, Summarizing, and Reporting the Results
The data extracted from the included studies were synthesized and summarized using the scoping review analytical framework. The effectiveness of the intervention was then judged based on factors including the outcome, sample size, study duration, and more. Any disagreements between the researchers regarding the evaluation of an intervention were discussed until a conclusion was reached.
Statistical Method
Microsoft Excel 2019 software was used to process data. Quantitative data was summarized using statistical mean. The outcome was displayed in a combo bar-chart-scatter plot format and bar charts. In the combo bar-chart-scatter plot chart, the bar-charts represent intervention outcomes of the intervention group before and after administration of intervention. The scatter plots represent the control/placebo outcomes before and after observation or administration of placebo.
Results
Literature Search and study selection
In the initial search, 177 records were obtained, excluding duplicate documents. In the first screening process, 31 potentially relevant records were screened, among which 30 underwent full-text reviews, except for one record whose full text was unavailable. In the second screening process, 1 duplicate, 1 non-English paper, 6 non-randomized trials, 7 articles whose participants were not all survivors of the natural disaster, and 1 study without any intervention were excluded. Ultimately, a total of 14 randomized clinical trials were included in this scoping review.
General characteristics of included studies
Among the included studies, there were a total of 14 randomized controlled trials (RCTs) published from 2009 to 2023.
Population: The scope of the randomized control trials included wildfires, tornadoes, tsunamis, floods, and earthquakes. Earthquakes were the most prominent event, possessing 9 RCTs, 2 related to the 2010/2011 Canterbury and Christchurch Earthquakes in New Zealand,8,9 4 related to the 2008 Sichuan Earthquake in China,10–13 2 related to the Great East Japan Earthquake,14,15 and 1 related to the 1999 Gölcük Earthquake in Turkey.16 Other than earthquakes, 2 of the RCTs were related to the 2004 Indian Ocean Tsunami in Thailand and Sri Lanka,17,18 and 1 RCT each for the 2008 Bihar Flood in India,19 the Spring 2011 Tornadoes in the United States,20 and the 2016 Fort McMurray Wildfires in Canada.21 The geographical frequency of disasters survey in this scoping review was more concentrated around South and East Asia compared to the rest of the world.
Intervention: 4 RCTs used CBT,10,16,18,21 including one with a group-administered CBT intervention,18 one with a therapist-assisted online intervention,21 and another single-session modified behavioral treatment.16 5 other RCTs used pharmacotherapies, nutritional supplements or herbs,15 including the administration of hydrocortisone,8 micronutrients (Berocca Performance, CNE4, and CNE8),9 traditional Japanese herbal medicine saikokeishikankyoto (SKK),15 Chinese herbal formula Xiao-Tan-Jie-Yu-Fang (XTJYF) [10], and fish oil as supplementation to psychoeducation.14 Also included was a yoga intervention,19 narrative exposure therapy,12 acupuncture with a CBT control group,13 a web-based intervention named BBN (Bounce Back Now) consisting of behavioral treatment, coping strategies, and anxiety management,20 and a school-based intervention termed ERASE Stress Sri-Lanka targeted towards children using psychoeducational material, cognitive-behavioral skills, meditative practices, and bio-energetic exercises as well as processing traumatic experiences by utilizing art therapy and narrative techniques.17
Control: Most interventions in the control group were placebos for pharmacotherapies and waitlisting for therapies or other interventions. One study testing fish oil as a supplement to psychoeducation used psychoeducation as a control group.14 Another trial testing the effectiveness of acupoint stimulation and CBT used CBT as a control group.13
Outcome: Most studies utilized DSM IV criteria to determine eligibility for PTSD diagnosis.
This scoping review included fourteen randomized control trials (RCTs). The included interventions were pharmacotherapies (n=5), CBT and its variations (n=4), yoga (n=1), narrative exposure therapy (n=1), acupuncture stimulation (n=1), Bounce Back Now (a web-based intervention; n=1), and ERASE Stress Sri Lanka (a school-based therapy targeted towards adolescent; n=1). Generally, pharmaceuticals, nutraceuticals, and herbal supplements exhibited inconsistencies in results. CBT interventions were standard of care and effective. High-level clinical evidence (RCTs) is lacking to effectively determine the efficacy of interventions related to yoga, acupuncture, narrative exposure therapy, and more. Clinical studies in this field need to be further expanded regardless of the study type.
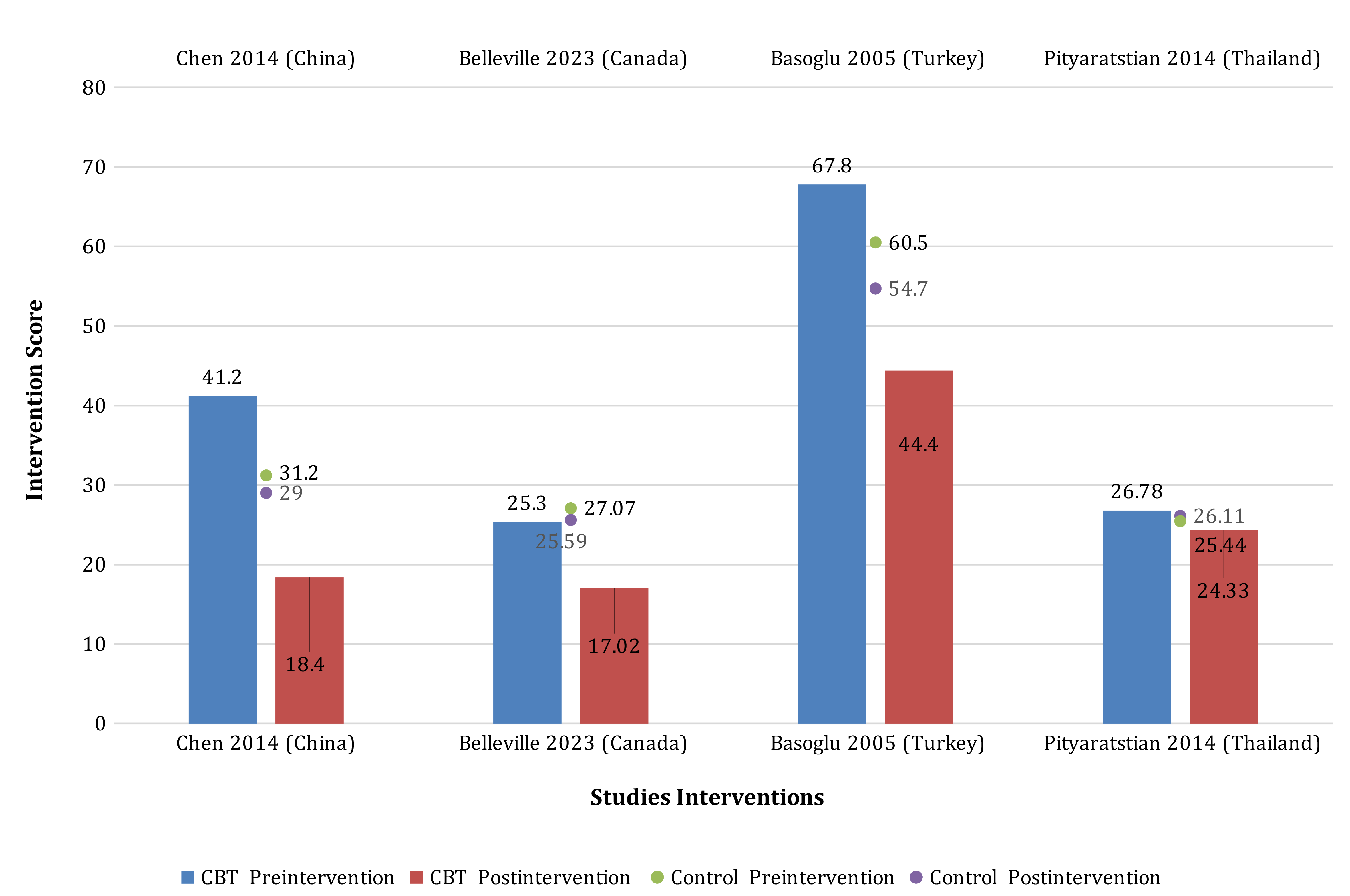
Figure 2 and table 3 show the effectiveness of CBT in the 4 studies included in this review. It is to be noted that the scales of all four studies are not uniform, as the graphs shows change in the pre and post intervention of the scales used in the respective studies. In the study conducted in China and Thailand,10,18 the Children’s Revised Impact of Events Scale (CRIES-13) psychological instrument was used to diagnose the presence PTSD in study participants. The study conducted in Canada regarding wildfires21 used the PCL-5 psychological instruments to diagnose the Prescence PTSD while the study conducted in Turkey16 used CAPS (Clinician-Administered PTSD Scale) to assess the presence of PTSD in study participants. All these instruments provide standardized ways to diagnose PTSD in patients exposed to natural disasters.

At baseline, the mean scores for the CBT intervention group were high across all four studies, indicating the PTSD symptoms experienced by participants before receiving the intervention. However, at the post-treatment stage, the mean scores for the CBT intervention group decreased, illustrating the effectiveness of CBT in reducing PTSD symptoms. This reduction in mean scores suggests that the CBT interventions had a positive impact on the psychological well-being of natural disaster survivors. Also, these scores reflect the outcomes of CBT interventions compared to control conditions in each study. Generally, lower scores indicate reduced symptom severity or improved outcomes.

Figure 3 and table 4 display the effectiveness of the interventions of five studies including 1 pharmaceutical,8 2 herbal supplements,11,15 and 2 nutraceuticals.9,14 Two studies in Japan testing fish oil and SKK herbal supplement as interventions14,15 and a study conducted in New Zealand testing micronutrients9 utilized the Impact of Event Scale (IES-R). The herbal supplement XTJYF in the China study11 used the Symptom Check-List-90-Revised (SCL-90-R) score while atypical use of pharmaceutical hydrocortisone in the New Zealand8 study used the Subjective Units of Distress Scale (SUDS).
At this time there are not many studies examining each of the pharmaceutical, nutraceutical, and herbal supplements for PTSD treatment in the context of natural disasters to make definitive conclusions. Pharmaceuticals, nutraceuticals, and herbal supplements may have a role in addressing PTSD symptoms, but further research is needed. This review identifies a gap in this aspect.

Figure 4 shows the variability of study duration among the 14 studies examined in this scoping review. The duration of the trials varied: CBT studies ranged from 4-24 weeks and pharmaceutical, herbal supplement and nutraceutical studies ranged from 1-48 weeks. Other interventions also collectively ranged from 1-48 weeks.
Discussion
The current scoping review aimed to identify the current status of research regarding interventions for PTSD of natural disaster survivors. The literature surveyed reveals insight into both the current data collection and research gaps to investigate.
Question 1: What is the reported effectiveness of each individual intervention studied for PTSD and Natural Disasters?
CBT (n=4)
4 studies in this scoping review used CBT or a modified form of it.10,16,18,21 All 4 studies displayed a clinically significant decrease in PTSD symptoms after follow-up compared to the control group. The CBT studies focused on adolescents and youth displayed significant decreases in CRIES (Children Revised Impact of Events Scale) scores after the disaster.10,18 Specifically, a group CBT intervention in a post-disaster setting with limited resources like many third-world countries proved to be effective.18 Furthermore, one study showed that CBT proved to be a better intervention than general support, affirming its superiority.10 Another study after the 2016 Fort McMurray Wildfires showed that an online-based CBT intervention led to clinically significant decreases in PTSD symptoms and related markers, affirming CBT’s viability as a virtual intervention.21 A study utilizing a modified form of CBT, SSBT (single-session modified behavioral treatment), found a 49% improvement rate, rising to 85% after 24 weeks.16 This shows that CBT can be delivered at shorter lengths being more cost-effective, and further research is needed to verify SSBT’s effectiveness.
Pharmaceuticals, nutraceuticals, and herbal supplements (n=5)
5 studies in the scoping review used pharmaceuticals, nutraceuticals, and herbal supplements as interventions.8,9,11,14,15 The RCT administering hydrocortisone in combination with script-driven imagery found non-significant trends of increasing subjective distress (the opposite effect), proving ineffective.8 The RCT administering fish oil supplementation to psychoeducation also found non-significant trends for the superiority of fish oil supplementation plus psychoeducation over psychoeducation alone for attenuating PTSD symptoms.14 Three RCTs displayed results in favor of specific micronutrients and herbal formulations for PTSD.9,11,15 Traditional Japanese herbal medicine SKK showed significantly improved IES-R scores (Impact of Event Scale or level of subjective distress) among patients after administration, however, the study spanned only 2 weeks in length, so the herbal medicine’s long-term efficacy is unknown. The modified traditional Chinese medicine XTJYF displayed positive results in the measured SCL-90-R score (The Symptom Checklist-90) in comparison to a placebo over a study duration of 8 weeks and a sample size of 245.11 The SCL-90-R scale used was less specific than other scales in evaluating PTSD symptoms. The RCT evaluating the effectiveness of micronutrients showed better outcomes when taken during the acute phase after an earthquake.9 Pharmaceuticals, nutraceuticals, and herbal supplements provide mixed results of effectiveness. Current evidence regarding pharmaceuticals (hydrocortisone), herbal medicines, supplements like fish oil, and micronutrients requires further investigation for conclusions to be drawn.
Yoga (n=1)
1 study in this scoping review used yoga as an intervention.19 The RCT found that a week of yoga practice for one hour a day, consisting of loosening exercises (sithilikarana vyayama) for ten minutes, physical postures (asanas) for twenty minutes, and breathing techniques (pranayamas) for twenty-five minutes, resulted in a significant decrease in sadness compared to an increase in anxiety in the control group. There was a non-significant decrease in fear, anxiety, and disturbed sleep in the intervention group.19 This study, conducted over a time span of one week and with a participant number of 22 individuals, shows that yoga could be used as a cost-effective intervention for natural disaster victims, but requires further research.
Narrative Exposure Therapy (n=1)
1 study in this scoping review used narrative exposure therapy (NET) and a revised version shortened to one week in intervals of 1-2 days (NET-R).12 Results showed that both interventions showed significant reductions in PTSD and related symptoms compared to the waitlist control group. More research is required both on narrative exposure therapy’s effectiveness after a disaster and how shortened versions of therapies such as NET-R and SSBT compared to their originals with their cost-effectiveness.
Acupuncture (n=1)
1 study in this scoping review used acupoint stimulation with a CBT control group as an intervention.13 The study showed a significant reduction in subjective distress (IES-R score) compared to the solely CBT control group. The study did not account for the placebo effect and thus further research into acupuncture therapy as a sole means of intervention is needed.
Bounce Back Now (n=1)
1 study in this scoping review utilized a web-based intervention addressing PTSD symptoms targeted toward adolescents.20 The intervention showed that adolescents in the intervention group had fewer PTSD symptoms after 12 months compared to the control web-based assessment group. Along with the therapist-assisted online version of CBT, more research is required to correctly conclude the effectiveness of web-based interventions like BBN.
ERASE Stress Sri-Lanka (n=1)
1 study in this scoping review used a synthesized program covering a wide range of therapies tailored toward children in schools.17 Results showed a significant reduction in all outcome variables and improvements in PTSD severity, functional problems, somatic complaints, depression, and hope scores in the intervention group. This study shows insight into how interventions tailored toward kids can be done in a school with art and narrative therapies. More research is required to accurately determine the consistent feasibility of such interventions.
Question 2: Which populations were targeted in interventions for natural disaster survivors with PTSD?
The populations targeted in interventions for natural disaster survivors were mainly adults, with population mean ages between 30 and 55 years of age.8,9,11–16,19,21 A few trials targeted children and adolescents for their studies, with mean ages ranging from 12.25 - 14.5.10,17,18,20 The studies concerning adolescents and children were especially accommodating for children. For example, the study implementing the program ERASE Stress Sri Lanka utilized art and drawing as means of therapy tailored towards children that are accomplishable in schools.17
In general, the ethnicity and racial group of the majority of the participants of this study were Asian due to the high frequency of disasters in the region. This included four occurrences in China,10–13 two in Japan,14,15 and one each in Thailand,18 India,19 and Sri Lanka.17 In contrast, two studies were conducted in New Zealand,9 and one each for Turkey,16 The United States,20 and Canada.21 The high frequency of Asian studies could account for the occurrence of traditional herbal medicines used as interventions11,14,15 as well as the testing of acupuncture therapy.13 As research shows that Asians, such as the Chinese, cope differently than other ethnic groups because of cultural differences,22 this imbalance in the geographic concentration of high-level clinical evidence such as RCTs regarding the treatment of PTSD for natural disaster survivors posits a need for further studies to be conducted in more diverse locations around the world such as Europe, Africa, or South America.
Question 3: What adverse events were reported in the treatment of PTSD for natural disaster survivors?
In the literature reviewed, there were a few adverse events reported which brings up the need for further investigation for safety protocols to be taken. The study administering Chinese herbal medicine XTJYF found that both the control and intervention groups reported nausea, diarrhea, and malaise, which were eventually found to be minor and unrelated to the herbal medicine’s intolerance.11 It is important to note that pharmaceuticals, nutraceuticals, and herbal supplements in general can have adverse effects. Acupoint stimulation was also a point of concern in regard to safety practices. The study testing acupoint stimulation compounded with CBT showed that there were no adverse events reported except for a slight numbness sensation.13 This means that acupuncture therapy can be carried out safely with the correct procedures in place.
Questions 4 & 5: To what extent do the interventions for PTSD in natural disasters demonstrate ease of implementation? Which areas of research exhibit potential for further investigation for the treatment of PTSD in natural disaster survivors?
The various interventions discussed in this scoping review all pose challenges to their implementations. For example, traditional CBT has been proven to be extremely effective in numerous studies but is limited by factors such as cost and the shortage of trained therapists in rural settings23 and major parts of the world. However, alternative forms of CBT in this review such as SSBT,16 Group CBT,18 and online CBT21 combat this deficit though it is unclear if they are as effective as traditional CBT. The traditional herbal medicines in this review also face problems, as SKK and XTJYF are not widely accessible due to their regional availability.11,15 Evidence for nutraceuticals and pharmaceuticals also have deficits in the fact that there is not enough rigorous scientific research to show their benefits and the safety issues that they pose.8,9,14 Further research investigating the impact of medications, anti-depressants, and other types of pharmaceuticals, nutraceuticals and herbal supplements is needed.
Like CBT, NET also faces the same issues in terms of cost-effectiveness and availability of professionals but has been proven by previous studies as effective.12,24 If further research on modified forms of NET is explored, it is possible that the most cost-effective versions can be produced. On the other hand, web-based interventions such as BBN and therapist-assisted online CBT are more accessible to groups of people in more developed countries and recently impacted third-world countries may not possess the infrastructure to use the internet on a large scale.20,21 Furthermore, issues such as language adaptation, education level of the treatment group, and coordination are barriers to web-based interventions’ implementation. If these issues are combated on a large scale and more research is done to affirm that therapies conducted over the Internet do not lose effectiveness, web-based interventions can be promoted further. Acupuncture therapies also possess barriers to acquisition. This includes issues like the availability of resources, strictness of local regulations, access to trained professionals, and individual preferences.25 More research regarding acupuncture’s effects is required. Mind-body therapies, such as yoga, have a large ease of implementation due to the popularity and large number of trained professionals and versatility in both online and in-person settings.26 Yoga practices, including mindfulness meditation and breathwork, can enhance emotional regulation skills, potentially leading to improved mental well-being and resilience.27 Although there is evidence pointing towards the benefits of yoga, high-level clinical evidence such as RCTs for PTSD survivors after a natural disaster are not many in number, and further research should be done comparing Yoga to current standard care treatments like CBT.

In this scoping review, 60% of the studies reviewed were testing on populations of earthquake survivors. The prevalence of PTSD is presumed to be higher among earthquake survivors due to the significant loss of life associated with earthquakes when compared to other natural disasters, however, reliable data supporting this claim is currently unavailable.28 Floods are the most common type of disaster globally, responsible for almost 53,000 deaths in the last decade alone, yet only 27% of studies surveilled included flood survivors.29 Furthermore, the US Environmental Protection Agency (EPA) claims that flooding is becoming increasingly common throughout the American shoreline 30. Given these circumstances, there is a pressing need for more in-depth research on the mental health implications, including PTSD, among flood victims in the United States
Limitations of this review
This scoping review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to the best possible extent. However, it should be noted that certain aspects were not fully implemented in this scoping review. Firstly, the current absence of biomarkers for diagnosing PTSD in clinical practice, despite research exploring potential associations was a limitation in our study. Secondly, several studies in this review relied on self-reported adherence to the protocol for assessment which could interfere with the credibility of the results. The third limitation of this review is that the methodological quality of the studies reviewed was not checked using rigorous criteria such as Cochrane’s risk of bias tool. Additionally, obtaining protocol registration and conducting detailed statistical analysis such as exploration of variation in effects, risk of bias assessment, confidence intervals, and measures of statistical heterogeneity were not within the scope of this study. This means that the review of literature may have not accounted for specific faults in the study’s methodology, which could jeopardize the implications of this review.
Conclusion
Current literature in the form of high-level clinical evidence (RCTs) testing the effects of interventions for the PTSD of natural disaster survivors is limited. This scoping review shows that among evidence-based practices, pharmaceuticals, nutraceuticals, and herbal supplements exhibited inconsistencies in results. Of special note is the limited availability of studies pertaining to the use of pharmacotherapies, nutraceuticals, and herbal supplements in the treatment of PTSD for natural disaster survivors highlights a potential research gap that warrants further investigation. CBT interventions are considered standard of care for general PTSD treatment and were also found to be effective for the treatment of natural disaster-related PTSD symptoms in this review. However, more RCTs are needed. There is insufficient clinical evidence to effectively determine the efficacy of yoga, acupuncture, art, and narrative exposure therapies. Post-disaster relief efforts should not only support interventions according to the level of scientific evidence of their efficacy but also consider factors like the availability of resources including public education on how to best prevent PTSD, trained professionals to diagnose and treat PTSD, cultural sensitivity of the intervention used, values and preferences of relevant stakeholders. Clinical studies in this field need to be further expanded regardless of the study type.
Recommendations
-
Given the limited number of high-quality studies and the gaps in the current literature, it is important to conduct additional research to expand the evidence base for the PTSD interventions in natural disaster survivors. This could include more randomized controlled trials (RCTs) with larger sample sizes, longer follow-up periods, and rigorous methodology to assess the effectiveness of different interventions.
-
The majority of studies in the reviewed literature focused on Asian populations, reflecting the frequency of natural disasters in that region. However. It is important to explore the effectiveness of interventions across diverse populations, including different ethnic and cultural groups. Conducting studies in other regions of the world, such as Europe, Africa, or South America, would provide a more comprehensive understanding of the effectiveness of interventions in various cultural contexts.