

Introduction
First discovered in a 50-year-old woman by Alois Alzheimer in 1906, Alzheimer’s disease (AD) is the progression of cognitive and functional decline caused by the death of neurons. AD primarily targets the brain during the initial stages of the disease including the inability to encode and store new memories. Changes in the patient’s cognition and behavior signify that the disease progressed into the later stages. Alterations in amyloid precursor protein (APP) cleavage and production of APP fragment beta-amyloid along with hyperphosphorylated tau protein production, and risk genes (e.g. ApoE) cause a reduction in synaptic strength, synaptic loss, and overall neurodegeneration.1,2 Alzheimer’s Disease International began an evidence-based Delphi consensus on the prevalence of dementia globally in 2005. The Delphi study estimated that about 42.3 million patients are diagnosed with AD with 4.6 million new cases of dementia every year. They also concluded that the countries that have the most cases of dementia are China, the western Pacific, western Europe, and the USA.3 Niu et al. conducted a meta-analysis of the prevalence of AD in Europe and concluded that the incidence of AD was approximately 7.02 per 1000 people per year for men and 13.25 per 1000 people annually for women with the rates increasing with age.4 Among patients with AD, the Alzheimer’s Association concluded in 2016 that about 81% are ≥75 years old, 15% are 65-74 years old, and 4% are ≤65 years old.5 As it is the most common form of dementia, AD has grown into a global health concern. Effective treatment for AD has become necessary to control the prevalence of AD among both US and global communities.
Currently, there are only two categories of pharmacologic therapy available for patients with AD. Patients with mild, moderate, and severe AD are recommended cholinesterase inhibitors donepezil, rivastigmine, and galantamine. Alternative therapies include following the Mediterranean diet (e.g. fresh produce, whole grains, olive oil, seafood), regular aerobic exercise, and nutraceutical huperzine A, all of which have the capacity to improve both the patient’s memory functions and common activities in their daily life.6 While these therapies can curb the effects of AD, they can only delay the progression of AD; there is yet a solid and effective treatment for AD.
Due to the great prevalence of AD globally every year, afflicted patients gradually lose the ability to store new memories and conduct their daily activities. As a result, family members and close friends must become the patient’s caregivers and maintain the patient’s mental stability and lifestyle. The sudden change in the caregivers’ daily lifestyle, the amount of time they must dedicate to the patient, the excessive costs, and other circumstances caused caregivers to face unique circumstances, which can negatively impact their own mental health and stress levels. According to a study conducted by Barbara Grabher, caregivers are afflicted with work-related stress in addition to taking care of a patient with AD. For example, 57% of caregivers must go to work late, leave early, or take time off, 16% must take a leave of absence, and 18% had to change their job from full-time to part-time. Along with work-related stress, caregivers are afflicted with stress for finding time to take care of the patient and a decline in their own physical and mental health.7
A study of 309 caregivers from China discovered that depression, anxiety, and sleeping problems are their most common challenges. In addition, caregivers dedicate most of their time to taking care of the patient with AD, not leaving any time for themselves. The authors of this study found out that the lower the functional status of the patient, the higher the burden for the caregiver.8 A study conducted by Truglio-Londrigan et al. used the Kreuger and Casey systematic focus group interview method. Data was collected through transcriptions of 90-minute recorded sessions among participants. The study discovered that caregivers offer themselves up for taking care of the patient and realized that they all needed some sort of support to endure all the challenges.9
Several other variables can contribute to the increase of stress among caregivers, including their relationship with the patient, their motivations, and financial factors. The authors of this study sought to investigate the emotional, physical, and social impact AD has on caregivers.
Methods
Recruitment and Data Collection
Two hundred (N = 200) caregivers of patients with AD within the US were surveyed through a survey research platform that utilizes organic sampling built on Random Device Engagement (RDE). Using artificial intelligence (AI) to track unique respondent identification, RDE contacts users in their natural environments. Participants can answer the survey through any device while also performing their daily activities. The survey platform has numerous partnerships with approximately 120,000 other applications and more than 700 million global users. As a result, the survey platform stimulates the randomization of participants and their eligibility for the survey through incentives specific to the user’s daily activities on their device. The advanced AI algorithm and technology prevent fraud from single users from several accounts and suspicious or illogical responses to survey questions. The survey platform uses weighting to give certain respondents more weight so that the overall survey demographics match correctly for age and gender. All results are reported with this weighting.10
The Survey
One screening question was used to determine participant eligibility for the study. The question asked whether or not the participants are currently a caregiver for a patient with AD. The subsequent thirteen questions focus on the motivations behind taking care of the patient with AD, how their duty as caregivers impacts their physical, mental, and social health, and other factors that may contribute to their stress. For some of the questions, multiple selections among the multiple choices were allowed. The final question was open-ended and designed to capture the participants’ feelings not discussed in the survey.
Statistical Analysis
Data were analyzed using JMP 16 for Mac. Participants with a household income of less than $25,000 annually were considered “low-income”. For comparing 2 x 2 contingency tables, Fisher’s two-tailed exact test was used. Ninety-five percent confidence intervals (CI) for odd ratios are Wald-based. All results were weighted to match the univariate distributions of age and gender.
Ethical considerations
HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE) issued study exemption #2022-475.
Results
Due to the screening question, all participants were caregivers of a patient with AD. There were 200 participants total with 104 (52%) females and 96 (48%) males. The median age of participating caregivers was 37 years, with an interquartile range of 32-47, a maximum of 75 years, and a minimum of 16 years. 10.5% of participants were divorced, 36% married, 33.5% single, 8.5% live with their partners, and the remaining 11.5% are separated or widowed. White, black, and Hispanic caregivers make up approximately 91% of the participants. 43% are considered low-income participants (less than $50,000 annually); 34% are considered middle-income participants; and, the remaining 23% are high-income participants. Participants also reported other demographic variables such as their education, number of children, employment status, and their occupations. Each question is explored in detail in the following.
As a caregiver, what is your relationship to the patient with Alzheimer’s?
30.5% of participating caregivers reported that they are the parents of patients with AD. 5.5% of participants are the spouses of patients with AD. 16.5% are the children of patients with AD. 11.5% reported that they are close friends of the patient. 25.5% reported that they are relatives of the patient. 10.5% reported others (Fig. 1).

How has Alzheimer’s disease impacted your relationship with the patient?
47.5% of participants noted a more strained relationship with the patient. 19.5% of the participants said that they have improved their relationship with the patient. 33% noted that AD has no impact on their relationship with the patient.
On a scale of 1-5, please rate your stress from being a caregiver (1 = least stress, 5 = extremely stressed)
1.5% of the participants rated their stress as 1, implying that they aren’t as stressed compared to others while being a caregiver. 8% of the participants rated their stress as a 2. And 32% of the participants gave a rating of 3. And 36% of the participants gave a rating of 4. And 22% of the participants gave a rating of 5, implying that they are the most stressed compared to other participants.
How difficult would you say is it to take care of an Alzheimer’s patient?
3.5% of participants reported that taking care of a patient with AD is very easy. 2.5% of participating caregivers said that taking care of a patient with AD is easy. 28.5% of participants noted that taking care of a patient with AD is medium (moderately difficult). 38% of participants reported that taking care of a patient is hard, and 27% thought that taking care of a patient is extremely hard. These results demonstrate that more than half of the participating caregivers thought that taking care of a patient with AD is difficult.
How has being a caregiver impacted your sleep?
47% of participants report that they became sleep deprived after becoming caregivers. 3% of participants note that they sleep more after becoming caregivers. 50% of participants report that they sleep approximately the same amount, implying that becoming a caregiver doesn’t affect their sleep as much.
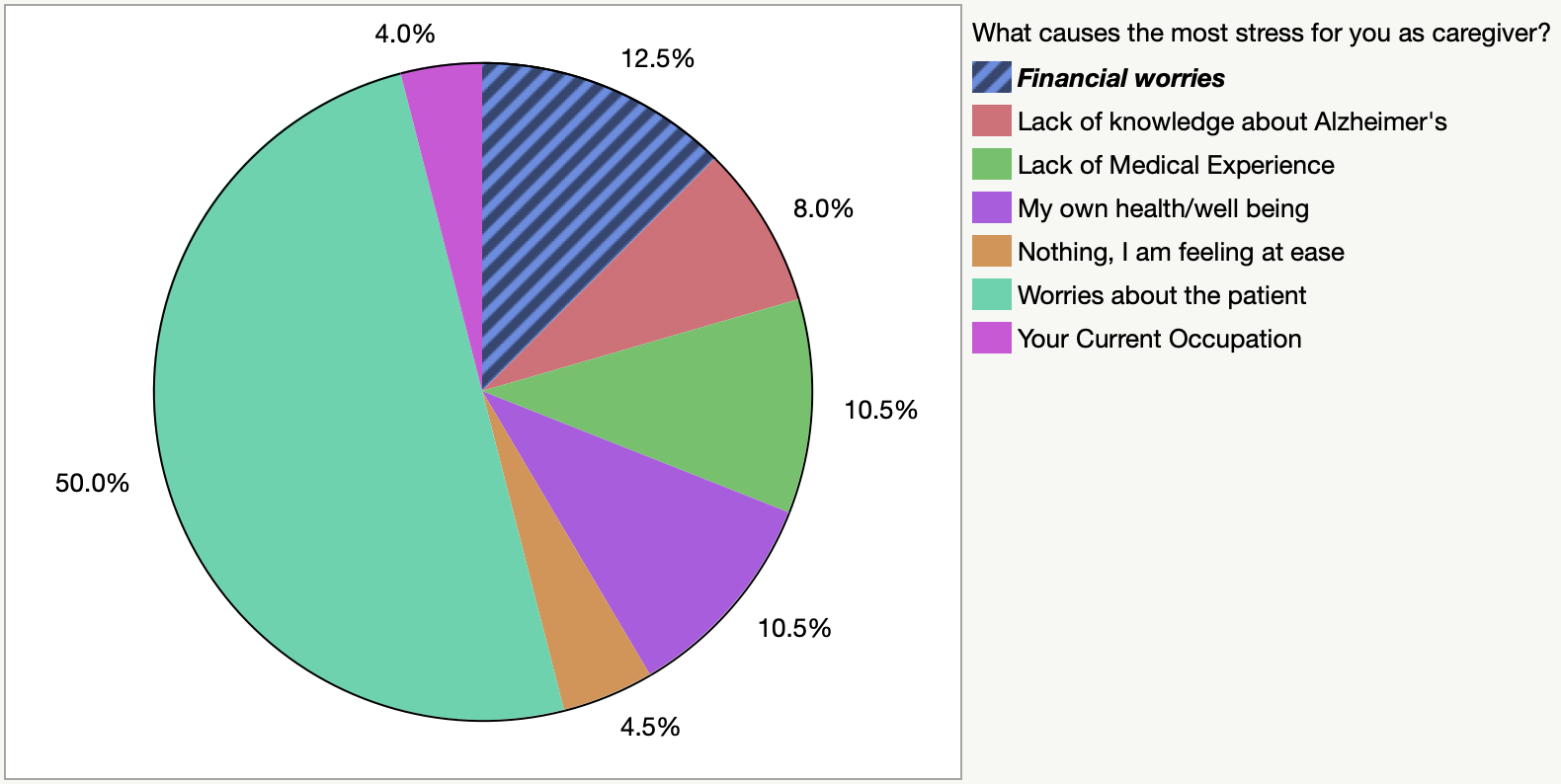
What causes the most stress for you as a caregiver?
56.5% of participants are stressed because they are worried about the patient with AD. 11.5% of participants are worried about their own health and well-being. 10.5% of participants are afflicted with financial worries, which contributes to most of their stress as a caregiver. Approximately 15% of participating caregivers said that most of their stress comes from their lack of medical experience and Alzheimer’s. 3% of participants note that most of their stress comes from their current occupation. 3% commented that they aren’t stressed as a caregiver (Fig. 2).

As a caregiver, approximately how many hours per week do you take care of the patient?
27.5% of participating caregivers dedicate about 10-20 hours per week to taking care of a patient. 22.5% of participants dedicate 24/7 (all their time) hours per week to taking care of a patient. 18% of participants dedicate 6-10 hours per week to taking care of a patient. This data demonstrates that more than half of the sample size dedicates at least six hours per week to taking care of a patient with AD. This would result in the caretaker having less time for themselves, which would potentially increase their stress. 20.5% of participants dedicate 4-6 hours per week to taking care of a patient. 11.5% of participants dedicate less than four hours per week to taking care of a patient.
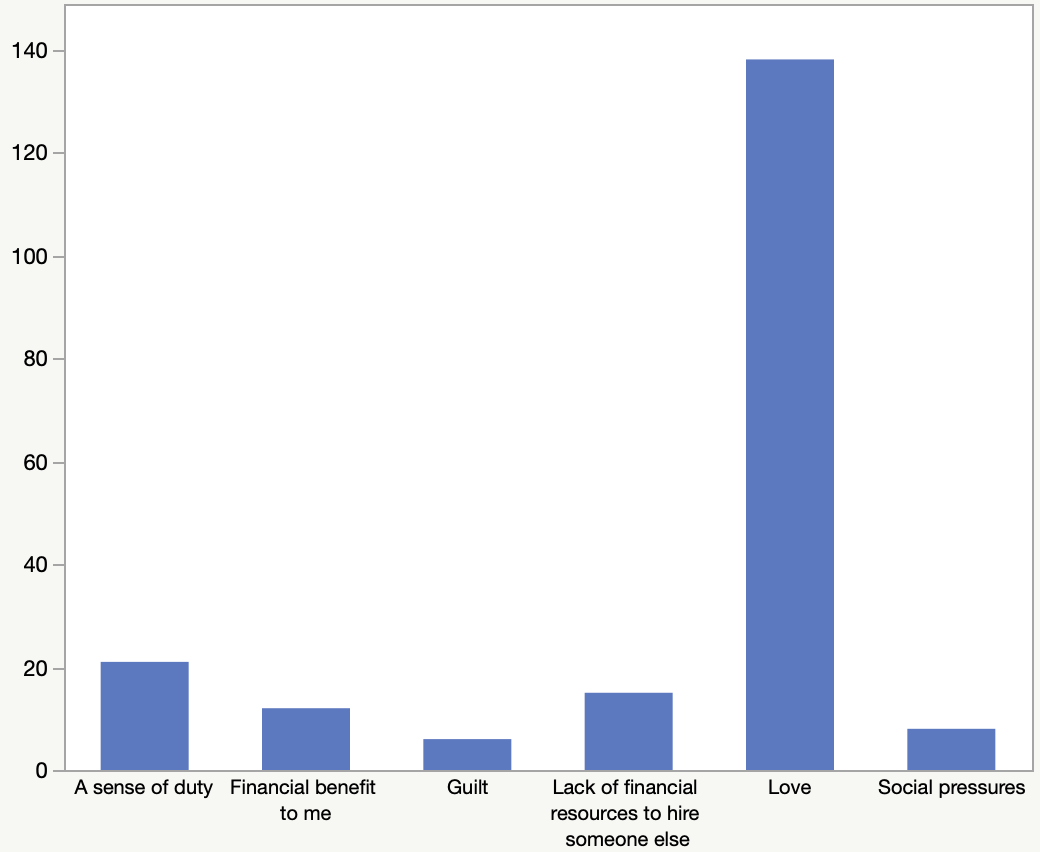
What motivates you to care for the patient?
A majority of 75.5% of participants noted that their main motivation for taking care of a patient with AD is love. 10.5% of participating caregivers felt a sense of duty that propels them to take care of a patient. 6% of participants note that they must take care of a patient because of the lack of financial resources to hire someone else. 4.5% of participants said that there’s a financial benefit to them for taking care of a patient. 2.5% of participants are pressured by social factors to take care of the patient. 1.5% of participants said that guilt was their primary motivation (Fig. 3).

After becoming a caregiver, would you say you became more socially isolated from your friends and family?
As a majority of participating caregivers dedicate most of their time to taking care of a patient, they would have less time to dedicate to themselves, family, and friends. Interestingly, a majority of 57% of participants stated that they aren’t socially isolated from their friends and family after becoming a caregiver. Only 43% of participants said that they feel more socially isolated from their friends and family. Using Fisher’s exact test, the authors didn’t find any significant differences in the prevalence of social isolation among participating caregivers across gender, the number of children, race or income. A majority of social isolation seems to occur in the middle-aged groups, such as 25-34 and 35-44 years old (Fig. 4), and this was statistically significant when compared to the younger age group of 18-24 (p = 0.0274). On univariate analysis, education was also statistically significant for the responses (p = 0.0008).

Have you done anything to alleviate your stress?
For this question, multiple responses were allowed. Increased participation in mindfulness activities (e.g. yoga), physical activity and exercise, professional help, drug use (e.g. alcohol and marijuana), getting a new hobby, and getting into unhealthy habits were found in 22.5%, 54.5%, 13.5%, 35.5%, 26.5%, and 10% and of the weighted population, respectively. About 20% of participants had not done anything to relieve their stress.
Did you ever try to get help from others?
About 64.5% of participating caregivers attempted to get help from others. On the other hand, 35.5% of participants didn’t receive help from others. A contingency table analysis was used. Having a postgraduate graduate was statistically significant (p = 0.0072, 95% CI = 1.564-17.37) for getting outside help. Postgraduate compared to university education yielded an odds ratio of 3.326, p = 0.0204, 95% CI 1.231-11.89. Participants were 233% more likely to ask for help if they have a postgraduate versus university degree and 421% higher if they have a postgraduate degree compared to a high school degree.
Are there any other factors/circumstances you would like to share about the stress as a caregiver has on you? (e.g. specific examples of how your daily life changed after becoming a caregiver, how you initially felt when you heard the patient was first diagnosed with Alzheimer’s, etc.)
For the final question, the authors created an open-ended question designed to capture any remaining feelings from the participants. As such, there wasn’t information for numerical patterns to emerge. Below are a few verbatim responses that capture the range of sentiments experienced by participating caregivers.
-
“Finding time for myself.”
-
“I wish our medical and elderly support system were much better than it is. We need better government support in this department.”
-
“My mom doesn’t understand what is wrong with her. She will say she doesn’t feel like herself and that’s hard to relate to.”
-
“Trying to keep them safe is hard.”
-
“I have a soft spot for patients with Alzheimer’s, due to more and more being left alone with no family involved.”
-
“I vowed to always be here for her and will not turn my back.”
-
“Afraid to take care of them.”
-
“It’s extremely hard to watch my loved one change and forget his family.”
Discussion
AD has brought severe physical, mental, and social repercussions among caregivers, such as becoming more isolated from their friends and family as well as losing sleep, and resorting to drug usage. As the number of AD cases rises every year, more patients lose the ability to store new memories and perform daily functions. Caregivers must dedicate more time to taking care of the patient, leaving no time for themselves. As reported by our survey, AD adversely impacts wellness and increases the stress of US caregivers, which is measured by self-reported increased social isolation, and sleep deprivation. Consistent with these results, Yu et. al indicates that the decreasing level of cognitive function in patients, high hours, and lack of support for caregiving are directly related to a caregiver’s burden.11 Because of these challenges, caregivers are likely to experience increased anxiety and depression and a decreased quality of life.12 This accounts for the increasing levels of stress among participating caregivers who are within the class of 25 to 44 year-olds compared to younger caregivers. This is likely because middle-aged caregivers have time-consuming occupations, as well as take care of other circumstances (e.g. raising a family, financial woes).
Based on our survey’s results, the majority of caregivers are the parents, relatives, or children of their patients. This demonstrates that a majority of caregivers are family to the patient with AD. Of the relatives, it seems the caregivers who are the most stressed are 25-44 years old. When the survey asked participating caregivers to rate their stress on a scale of one to five (1 = least stress, 5 = extremely stressed), more than 58% of participants noted that they are incredibly stressed. In addition, when asked how difficult it is to take care of a patient with AD, more than half of the cohort noted that it is indeed difficult to take care of a patient. Caregivers must spend a fair amount of time taking care of the patient, such as making the patient eat and sleep at regular intervals and spending a lot of financial resources to maintain the patient’s daily lifestyle. For example, the survey asked participants approximately how many hours per week they take care of a patient. Approximately more than half of the participants dedicate at least six hours per week to take care of a patient with AD. This means that the caregivers barely have any time for themselves or for their family, adversely adding on to their stress. In addition, being close to the patient makes it more difficult for their caregivers because it’s emotionally wounding to see the patients slowly forget them. In addition to taking care of the patient with AD, middle-aged caregivers must balance other challenges, such as limited time, energy, financial resources, while also taking care of their own children. In addition, according to Liu et al, older females and spouses play an important role in providing family care for patients with AD.8 Due to these unique challenges, participating middle-aged caregivers may experience increased stress, anxiety, and even depression.
AD also has repercussions on the social health of participating US caregivers (Fig. 5).

For example, it has the capacity to impact the relationship between caregivers and the patient. When the survey asked participants how AD impacts their relationship with the patient, nearly half of the participants (47.5%) noted a more strained relationship with the patient. As AD gradually degrades the connections between neuron cells and eventually the neuron cells themselves, the patient would gradually lose their memories, especially the memories regarding their identities and relationships with their close friends and family. Because of this, caregivers’ relationships with patients (especially if they’re relatives of the patient) can become more strained. Surprisingly, about one-third of the sample size said that AD doesn’t impact their relationship with the patient. Perhaps these specific participants are hospital caregivers who are assigned to the patient, so they wouldn’t have any emotional attachments to the patient. Other possibilities could be that the caregivers are motivated by monetary factors so that they won’t feel any attachments toward the patient. Relations with the patient seemed to improve for 19.5% of the participating caregivers. This could result from the increasing involvement of the caretaker with the patient’s lifestyle. In addition, they could feel closer to the patient when they comfort the patient from anxiety and depression. In addition, when the survey asked whether participants felt more socially isolated from their friends and family. Interestingly, a majority of participating caregivers said that they don’t feel isolated from their friends and family. This is probably because they realize the numerous challenges that come with taking care of a patient with AD. Therefore, they likely rely on a variety of support systems (e.g. friends and family) to help them endure the challenges. As a result, they would feel more connected with their family instead of becoming more isolated. On the other hand, 43% of the participants become more socially isolated from their friends and family. These participants probably wouldn’t have as many support systems. Because taking care of a patient takes a tremendous amount of time, the caregivers would have less time for themselves and their families. As a result, they would feel more isolated from their friends and family. In addition, when the survey inquired whether caregivers received more help from others, a majority (64.5%) tried to find help. Because of the numerous challenges, the stress levels of caregivers would increase. Therefore, they would rely on the people around them, their friends and family, to help them get through the process. while 35.5% didn’t attempt to find help. A minority probably didn’t find help probably because they didn’t have the financial resources to get help. These results are aligned with other existing reports. The greater cognitive, psychological, behavior, and motor impairment of patients with AD, the higher the levels of burden and distress in their caregivers, who, as a result, adopt coping strategies and seek familial and social support.13
AD also has the potential to impact the physical health of US caregivers. Interestingly, the survey reports that half of the participants sleep a regular amount while 47 lose more sleep after becoming caregivers. If caregivers are sleeping the normal amount, it implies that they have a great support system that allows them to receive more hours to sleep. On the other hand, caregivers are dedicated a lot of time to patients and maintaining their lifestyle (e.g. making the patient sleep and eat), along with their own family, occupations, and other circumstances that would increase their stress levels. In addition to sleeping issues, the eating habits of caregivers are also negatively impacted by AD. For example, Rivière et. al discovered that there’s a direct relationship between the decline of cognition and motor functions in patients with AD and the decline of healthy eating habits in caregivers.14
Caregivers have a variety of motivations to take care of patients along with factors that contribute the most to their stress and methods to alleviate their own stress. A majority of participants (75.5%) noted that their main motivation for taking care of patients with AD is their love for the patient (possibly as their close friend or family). A fair amount of participants mentioned a sense of duty as being their main drive to take care of the patient. This demonstrates the variety of motives that drive caregivers to take care of patients with AD. In addition, several factors contribute to the high-stress level of caregivers. In line with the results of Grabher et. al, worries for their loved ones and financial strains seem to be the top stressors for US caregivers. As a result of the numerous difficulties they faced, several caregivers came up with coping strategies. According to our survey, a majority of people seemed to use healthy coping strategies (e.g. yoga, physical exercise, or getting professional help). On the other hand, because low-income participants seemed to be the major demographic in this sample size, a noted increase in drug usage (e.g. alcohol and marijuana) seemed to be the less-expensive method of relieving their stress. In addition, another study discovered that emotion-focused coping, associated with religion and spirituality, was used most commonly among caregivers and can reduce the symptoms of depression and anxiety.15
In summary, several motivations and incentives drive caregivers to take care of patients with AD, with love and financial woes being the primary ones. Because of the vast amount of resources it takes to care for a patient, caregivers are expected to become more involved in the patient’s daily lives, thus leaving them with less time for themselves, their family, and their occupations. As a result, the stress can increase, which will adversely impact their physical, mental, and social health. Caretakers must rely on a support system (e.g. their friends and family) and coping strategies in order to mediate their increasing level of stress. Coping strategies can include healthy ones, such as physical exercise or seeking professional help, but it can also include cheaper, unhealthy ones, such as resorting to drinking and smoking. Because AD doesn’t yet have a cure, caregivers are the primary workforce to take care of patients and are expected to be increasingly involved in maintaining a patient’s life.
Limitations
These results, while representative of the US geographic population, are limited to caregivers who are registered to complete surveys with the survey platform. Possibly because of monetary and other incentives given by the research survey platform, the majority of participants seem to come from low-income participants. In this survey, approximately 43% of participants are of low-income status while the national average is 11.4%.16 Possibly due to personal reasons, a handful of participants preferred not to disclose their income or occupation. Our slightly disproportionate sample indicates that our findings may not fully represent all US caregivers. In addition, the survey questions may not have been completely eliminated in biases despite the authors’ best efforts. Participants may be biased to give optimistic or conversely, exaggerated answers to the questions, so there’s a chance that the results aren’t completely accurate. For example, 30.5% of caregivers reported being the parents of patients with AD. This result seems unlikely since AD commonly occurs in the elderly population. Finally, this study’s small sample size (N = 200) makes the results more restricted in representing the overall population of US caregivers in comparison to having a larger sample size.
Future investigative measures should include looking into the specific experiences of caregivers as well as other factors, such as whether caregivers are officially diagnosed with mental disorders (e.g. clinical depression, anxiety), the stress of caregivers who care for patients with other neurodegenerative diseases such as dementia and Parkinson disease, and areas of improvement for specific support systems and healthier coping strategies for caregivers.
Conclusion
AD degrades the cognitive, behavioral, psychological, and motor functions of thousands of patients in the US every year. The gradual progression of the disease causes an increase in stress and grief in caregivers, negatively impacting their physical, mental, and social health (e.g. becoming more isolated from their friends, and losing sleep). Because of this, caregivers have been leaning on recent support systems and coping mechanisms to deal with stress. This study demonstrates that compassion, comfort, and greater support for caregivers is needed to alleviate their burden.
Disclaimer
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.