

Cartilaginous tumors exist in benign or malignant forms. Chondrosarcoma, the malignant form, is a heterogenous tumor class that includes conventional, clear cell, mesenchymal, or dedifferentiated types.1 Dedifferentiated chondrosarcoma (DCS), which accounts for approximately 10% of all chondrosarcomas, is a rare and exceedingly aggressive subtype associated with high rates of metastasis and poor survival.2
The histologic findings of DCS include a low-grade cartilage tumor juxtaposed with a non-chondroid, high-grade sarcoma.3 On radiography, DCS appears as a destructive lesion often with an associated soft tissue mass. Despite its well-described radiographic and histologic profile, however, clinical data to inform the management of patients with DCS are sparse. Notably, the disease course is aggressive, with five-year survival ranging from 7% to 24% according to the literature.4–9 Furthermore, DCS tends to metastasize and locally recur despite wide margin surgery and modern adjuvant treatment strategies.
Given the lack of clinical outcome data and the poor prognosis of DCS, there is a need for studies that describe the natural disease course. Here we describe our institution’s experience in management and outcomes for 16 patients with dedifferentiated chondrosarcoma and review the current literature. We demonstrate poor survival rates that are in line with the current, existing literature.
Material and Methods
Selection
Following Institutional Review Board approval, a musculoskeletal pathologist used natural language search to identify cases of dedifferentiated chondrosarcoma within our pathology reports. A total of 23 patients from 2000 to 2018 with DCS over 18 years of age were identified. The following patients were excluded: duplicate record (4.3%, n=1), equivocal histopathological evidence of DCS (10%, n=4), index surgical treatment at an outside facility (4.7%, n=1), and loss to follow-up before one year without death occurrence (4.7%, n=1). Electronic medical records of the remaining 16 cases were reviewed.
Characteristics
Pooled characteristics of the included cases are summarized in Table 1. The median age of all patients was 62 years (interquartile range [IQR], 52;69) at diagnosis. At the initial encounter, 12.5% (n=2) had pathological fracture and 18.8% (n=3) had metastases to the spine (n=1) or lungs (n=2). The majority of patients were biopsied (core needle: 56%, n=9; incisional: 14.3%, n=2; excisional: 14.3%, n=2; core needle plus fine-needle aspiration: 6.3%, n=1). Biopsy was omitted in one patient with aggressive bony destruction of the humerus due to DCS diagnosed radiographically, and in one case of pelvic DCS where resection was indicated outright. DCS was suspected in 43.7% (n=7) of biopsies, though was misdiagnosed as undifferentiated pleomorphic sarcoma (UPS) in 12.5% (n=2) of cases, and low-grade chondrosarcoma in 31.2% (n=5) of cases.
The most common locations of DCS were the femur (50%, n=8) and pelvis (25%, n=4), followed by one case each in the ribs, tibia, humerus, and near the scapula. Five cases were associated with known enchondromas. The high-grade sarcoma component was most frequently UPS (37.5%, n=6), followed by osteosarcoma (31.3%, n=5), rhabdomyosarcoma (6.3%, n=1), and mixed (features of UPS, fibrosarcoma, and osteosarcoma; 6.3%, n=1) Figure 1. The high-grade sarcoma component was unspecified in two cases, and furthermore, the case of periscapular DCS was noted to have initial “low-grade” dedifferentiation. However, this tumor eventually recurred as a low-grade chondrosarcoma, and when reoperated on appeared to be adjacent to the scapula rather than arising from the bone itself.

Statistical Analyses
Demographic and clinicopathologic data were analyzed using descriptive statistics. Continuous variables of interest were represented as the mean or median with range, interquartile range (IQR), or standard deviation (SD). Categorical variables were compared with Chi-square test of independence or Fischer’s Exact test. Continuous variables were compared using a two-tailed t-test and represented with p-values. OS and RFS probabilities were estimated using Kaplan and Meier (e.g., log rank) methods. OS was recorded from the time of biopsy until date of death (event) or last known follow-up without death having occurred. RFS was calculated from the time of surgical intervention until date of local or systemic relapse (event). Due to the small size of our cohort, we were unable to perform a meaningful statistically powered analysis.
Results
Management
Of the 16 total cases, 81.3% (n=13) underwent limb salvage or wide margin resection Figure 2. An intralesional procedure was performed in one patient with pelvic DCS, and surgery was not pursued in two patients, both with initial metastases. The third case of initial metastasis had a palliative proximal femoral replacement to prevent pathological fracture. In total, 25% (n=4) had surgery alone, 43% (n=6) had surgery plus chemotherapy (neoadjuvant or adjuvant), and of the six cases with surgery and chemotherapy, four received radiation.

Neoadjuvant chemotherapy and neoadjuvant radiation were used in two patients (one with pelvic DCS and initial metastasis, and one with localized lower extremity DCS). In each of the aforementioned cases with neoadjuvant chemotherapy, the regimen consisted of cisplatin and doxorubicin (AP), given over two days in a 21-day cycle for a total of six cycles. One case with neoadjuvant chemotherapy had minimal tumor necrosis after AP, and the other did not undergo surgical resection. The general adjuvant regimen varied by case, and included AP alone (n=2), methotrexate and AP (MAP, n=1) and pazopanib plus proton radiation therapy (n=2). A regimen of AP and ifosfamide/etoposide (IE) was used in a patient with initial metastasis (and no surgery) but was changed to gemcitabine/docetaxel (GD) after disease progression.
The pelvic DCS patient who underwent an intralesional procedure was given palliative radiation and observed, though underwent subsequent radical resection with sacral corpectomy and laminectomy for disease progression after two years. Among the index surgical cases, 43% (n=6) had a reoperation, and the local recurrence rate following surgery was 29% (n=4) at a median interval of 12.5 months. Among the recurrences, 50% (n=2) recurred as conventional chondrosarcoma and one recurred as DCS. The third case of local recurrence was diagnosed radiographically. Reoperation was performed for local disease progression (n=4), failure of an intercalary allograft (n=1), and periprosthetic infection of an allograft prosthetic composite after resection of pelvic DCS (n=1). On histopathological evaluation of surgical resection specimens, 86% (n=12) recorded negative margins. Positive margins were recorded in an intralesional procedure for pelvic DCS, as well as in a case of DCS within the ribs in a patient who underwent an extended posterolateral thoracotomy with en bloc rib removal.
Outcomes
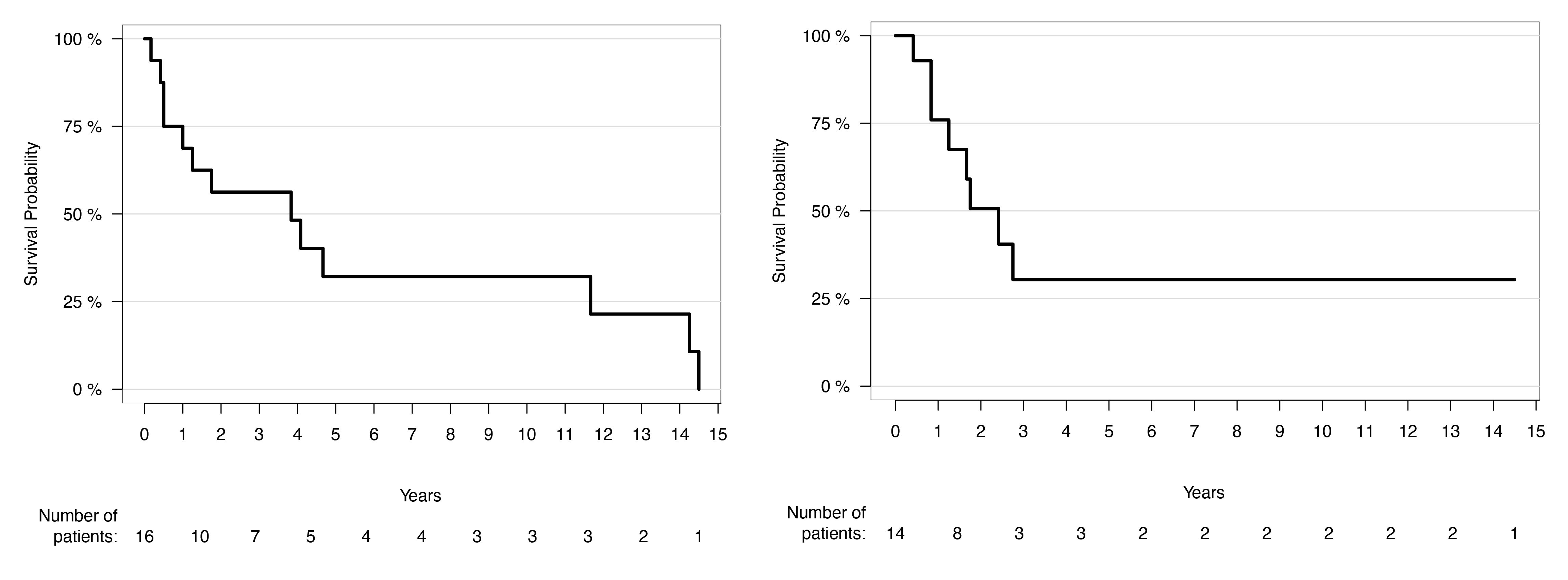
The median follow-up was 18.5 months (range, 1-140 months). By study conclusion, 81% (n=13) were deceased, 12.5% (n=2) were alive with relapsed disease, and one patient who was treated with a modular distal femoral endoprosthetic for DCS was alive and disease-free at 25 months follow-up. Among those without initial metastasis (n=13), 38% (n=5) progressed to systemic disease at a median 20 months. For all included patients, the median (IQR) OS was 46 months (12;140) with a five and ten-year OS probability of 32.1% (95% confidence interval [CI], 7.3% to 57.0%). One-year OS was 68.8% (95% CI, 46.0% to 91.5%) Figure 3-A. Similarly, the median (IQR) RFS was 29 months (15;42), with a five and ten-year estimated RFS probability of 30.4% (95% CI, 2.8% to 58.0%) Figure 3-B. Individual treatment characteristics and outcomes can be seen in Table 2.

Discussion
Among the previous literature that describe the outcomes of patients with DCS, five-year survival ranges from 7% to 24%.4–9 Our data confirm the prognosis of patients with DCS is poor, with a five-year probability of 32%. Similar to the majority of other data, these findings suggest the probability of long-term survival with DCS is low, despite advancements in surgical technique and modern aggressive multimodal management Table 3.
Very little is known about how treatment modalities affect the outcomes of patients with DCS, though the demographic patterns appear to be consistent throughout the literature. In the current study, the most common locations of DCS were the femur and pelvis, followed by the scapula (soft tissue), ribs, humerus, and tibia. Interestingly, larger studies note DCS tends to occur more commonly in the femur, pelvis, ribs, and scapula.4,5,10 Aside from location, DCS is also more common older patients and typically affects those around 50 to 60 years of age.6 Furthermore, DCS appear to have an equal predilection for sex, though some studies demonstrate a slight male predominance.4–6,11–13 In the current study, the distribution of sex and age is consistent with previous reports, with a near equal proportion of males and females and a median age of 62 years at diagnosis.
Few studies with sufficient sample sizes have identified prognostic factors associated with worse survival in patients with DCS. Staals et al. were among the first to suggest metastatic disease at diagnosis, along with the type of high-grade dedifferentiated component and percentage of high-grade dedifferentiated features, are poor prognostic factors.4 Conceptually, advanced disease at diagnosis would lead to worse outcomes, and this finding has been reliably confirmed in subsequent reports.6,7,9,13 With respect to the association of the dedifferentiated component and survival, the consensus is unclear. Johnson et al. suggest the dedifferentiated cell type was unrelated to development of metastasis and survival, except when it resembled low-grade fibrosarcoma.14 However, it also appears rhabdomyosarcomatous dedifferentiation has an association with worse survival, though the current evidence is limited to case reports.15 More recently, Dhinsa et al. observed a slight increase in survival with chemotherapy in DCS with dedifferentiated osteosarcoma subtype, though the benefit was small and may be related to the chemosensitivity of osteosarcoma.16 In contrast, Maio et al. showed evidence of worse survival in the UPS subtype, and thus it remains unclear whether the high-grade component of DCS affects survival.13 The current study was limited by low numbers; however, no appreciable difference in survival was observed between UPS and osteosarcoma subgroups with respect to the dedifferentiated components. Larger studies are likely needed to definitively confirm any association of subtype with outcomes.
The location of DCS has also been suggested to have an association with survival, though this evidence is also controversial. In one of the largest studies of DCS (n=59, SEER database) Strotman et al. found patients with axial and chest wall DCS have a lower risk of mortality than extremity DCS.6 This suggests chest wall DCS may be more amenable to resection, which would explain the lower risk of mortality in these patients. In contrast, Liu et al. demonstrated evidence of significantly worse survival among patients with axial versus appendicular DCS, though this sample had disproportionately higher number of axial DCS.9 In the current study, tumor location did not appear to affect survival. Although we did observe an aggressive disease course of DCS in the ribs, the evidence is limited, and this may have been related to a positive margin resection. The general lack of association of location and survival has also been further suggested by other studies.11,17,18 Given the paucity of data and the rarity of DCS, it is unlikely that a definitive association with anatomical location has been established.
The majority of the current literature describe a discernable benefit with surgery for the treatment of DCS. In studies of DCS with large samples, a clear survival benefit is seen after amputation or limb-salvage surgery.4,6,13 Furthermore, the importance of margin status was suggested by Grimer et al., who in their study showed more adequate local control with wide margin resection.5 In the current study, survival remained poor despite surgical intervention. However, in our clinical practice we continue to perform surgery with curative intent when possible. This is particularly true in non-metastatic cases, whereas in cases of known distant disease, palliative procedures may be more reasonable. Although there was no survival benefit observed in the current series, it is a small cohort, and resection for localized disease can be clinically beneficial.
Aside from surgery, there is no consensus regarding the role of adjuvant therapy for DCS. With respect to radiation, Strotman et al. found no survival benefit, and thus the use of any adjuvant therapy is also likely palliative in nature.6 According to the majority of the literature, there is also no benefit with chemotherapy.4,5,9,12,18–20 However, some studies have demonstrated a limited benefit, such as Kawaguchi et al. and Mitchell et al. who found surgical resection with adjuvant chemotherapy offered a survival advantage.11,21 With respect to the regimen used, AP therapy may have benefit in select patients for treatment of DCS with osteosarcomatous differentiation, though no regimen has been widely recognized as the optimal treatment.13,16 In the current study, survival did not appear to differ with chemotherapy and surgery versus surgery alone, nor with radiation in addition to surgery and chemotherapy.
There are significant limitations to this study. First, the study is retrospective in nature. Additionally, the small sample size precludes a powered statistical analysis of survival estimates with respect to surgical management and adjuvant therapies, which may be elucidated with analysis of a larger cohort. While surgery appears to portend better outcomes in the literature, there are mixed reports regarding the efficacy of adjuvant therapy Future, larger or multi-centered trials are needed to resolve these discrepant findings.
Conclusion
In summary, our data confirm the poor prognosis of patients with DCS despite advancements in adjuvant therapy. We record a five-year survival probability of 32% which aligns with the current literature. We hope that our data may add to the existing literature and provide an updated review of DCS. DCS remains an unsolved clinical challenge and future strategic recommendations for the optimal management for DCS are needed.
Funding
No funding sources were required for this study.
Availability of data
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
Rush University Medical Center obtained individual Institutional Review Board approval with an approved waiver of consent prior to beginning any research efforts.
Disclosures
ATB: (BMJ Case Reports: Editorial or governing board; Clinical Orthopaedics and Related Research: Editorial or governing board; exparel/pacira: Stock or stock Options; Journal of Oncology Practice: Editorial or governing board; Journal of Surgical Oncology: ad hoc reviewer; Lancet - Oncology: Editorial or governing board; Musculoskeletal Tumor Society: Board or committee member; Onkos Surgical: Paid consultant; Pediatric Blood and Cancer: Editorial or governing board; Rare Tumors: Editorial or governing board; Rush Orthopedic Journal: Editorial or governing board; Swim Across America Cancer Research Grant: Research support); SG: (Onkos Surgical: Paid consultant; Stock or stock Options; USMI: Stock or Stock Options). MWC: (Alphatec Spine: IP royalties; Paid consultant; AO Spine North America: Board or committee member; Research support; Cervical Spine Research Society: Board or committee member; CSRS: Research support; DePuy, A Johnson & Johnson Company: Paid presenter or speaker; K2M: Paid presenter or speaker; Musculoskeletal Tumor Society: Board or committee member; North American Spine Society: Board or committee member; Orthofix, Inc.: Paid presenter or speaker; Spinal Elements: Paid consultant. All other authors have no pertinent financial disclosures or pertinent conflicts of interest.
Acknowledgements
None.
Author Contributions
Study concept and design: S.G., A.T.B.; analysis and interpretation of data: C.A.G.; drafting of the manuscript: C.A.G., L.L., A.G.Z. Z.S.; critical revision of the manuscript for important intellectual content: C.A.G., L.L., A.G.Z., Z.S, S.G., I.M., M.C., A.T.B.; statistical analysis: C.A.G.