Introduction
Starting in January 2020, the SARS-CoV-2 pandemic caused enormous changes in the dynamics of the nation’s health systems.1 Public and private hospitals were reorganized to receive patients with COVID-19 disease during the lock-down period from March to May 2020. This reorganization led to a near-total stop of non-urgent, elective surgeries across all specialties, including hip and knee arthroplasty; impacting a huge economic loss on budgets, especially for private hospitals.1,2 However the aim of most European governments was to slow down the infected SARS-CoV-2 patient’s curve and prevent a collapse of nationals health systems.3 Only in May 2020, a gradual elective surgery restarting was possible with some limitations.1,3 After a short summer break, the infections rate is rising again, due to poor adherence to the social distancing rules in holiday resorts. Sardinia is an example, which seems to be one of the new Italian epicentres of the disease. Currently, on April 12, 2021, 3,77 million cases of COVID-19 disease were confirmed in Italy, among these 49109 in Sardinia. The deaths count increased to 114000.4 Total knee arthroplasty (TKA) represents one of the most performed elective procedures,5 however, the SARS-CoV-2 pandemic resulted in a not negligible reduction in this surgery.6 When knee arthroplasty in patients suffering from severe osteoarthritis (OA) was delayed for a long time, the final outcome could be affected.3. Knee osteoarthritic pain could lead to increased use of opioids, NAIDS drugs, and nutraceuticals with increased side effects and related complications.7–9 Patients often need to prolong their absence from work or request temporary unemployment benefits, therefore the direct and indirect costs for health care and social welfare could be significant.3 The aim of this study is to describe the surgical activity of a Sardinian reference centre for prosthetic surgery and the measures implemented to safeguard the health of patients and healthcare workers during the SARS-CoV-2 pandemic.
Materials and methods
The present study is a retrospective one-centre analysis regarding all patients who underwent primary knee arthroplasty at our Orthopaedic and Traumatology unit between March 1st and October 1st, 2020. Using the institutional database were extracted for each patient: age, sex, comorbidities, American Society of Anaesthesiologists (ASA) Physical Status Classification System, perioperative complication, hospital stay, need of blood transfusion, need of postoperative intensive care.
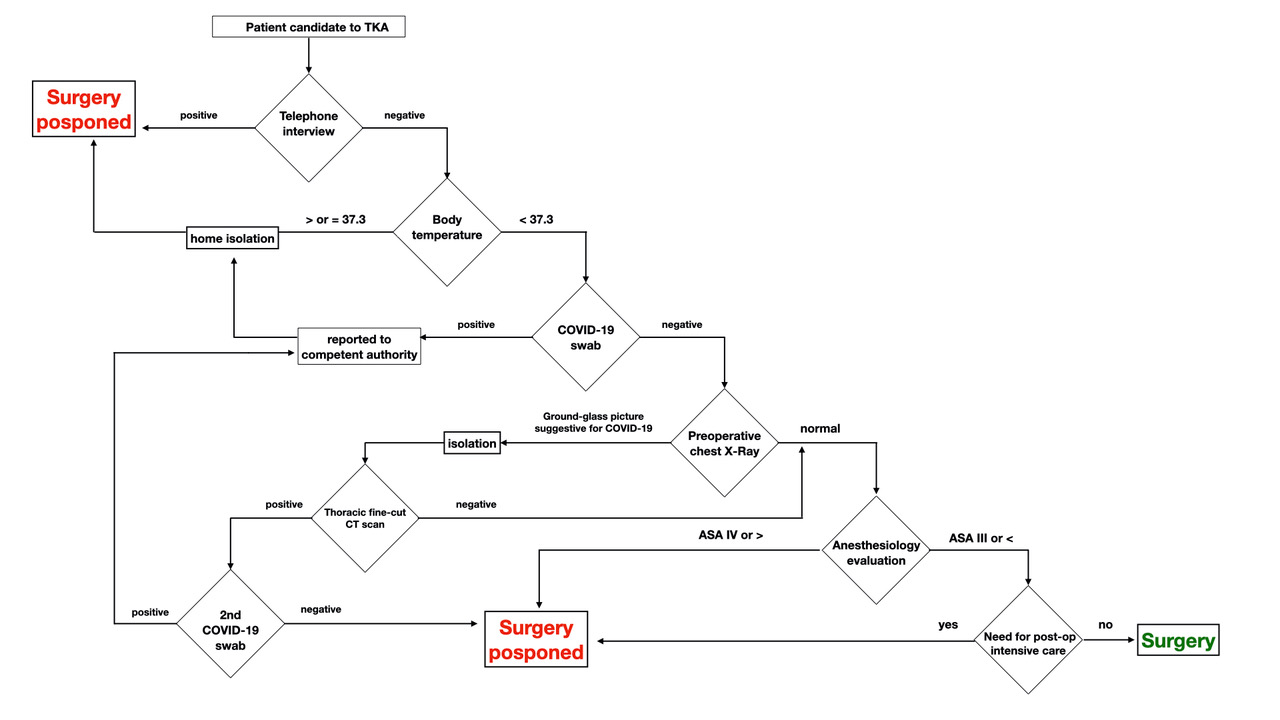
During the study period, a total of 147 TKA were performed. Principal patient data were reported in Table 1. The study time was divided into 2 periods: Pandemic (from March 2020 to May 2020), Post Pandemic (from June 2020 to October 2020). As a standard of care, to safeguard the health of patients and healthcare workers, a preoperative Ad hoc protocol was implemented (Figure 1). Before scheduling the operations (knee arthroplasty) for each patient an accurate COVID-19 anamnesis was performed by telephone interview. The patients were questioned about the typical symptoms of patients with COVID-19 infection: fever (as the first symptom), cough, fatigue, ageusia, anosmia palpitations, headache, and diarrhea.10

Considering the incubation period for SARS-CoV-2 we also asked about recent contact (last 15 days) with patients affected of or suspicion for COVID-19 diseases, recent (last 15 days) stay in endemic areas for COVID-19 disease. All patients treated were invited to the hospital the day before the surgery.
Upon arrival at the hospital, all patients were measured their body temperature using a thermo-scanner; patients with a temperature > 37.3 ° C were not hospitalized and were entrusted to the competent authorities, while other patients underwent to a preoperative SarsCov2 screening through nasal and oropharyngeal swabs. The obtained sample was analyzed was with polymerase chain reaction (PCR). Patients were isolated from each other until the results of the swabs. Positive patients were reported to the competent authorities, while negative patients were hospitalized and subjected to routine pre-operative examinations (chest X-ray, electrocardiogram, routine blood tests, and blood coagulation tests). If a suspicion of ground-glass opacities, bilateral and peripheral, coexisting with consolidations or cord-like opacities was made on chest x-ray a chest computed tomography (CT) scan was performed. If chest CT scan was negative the patient was a candidate for surgery, otherwise, if chest CT scan was positive or suspicion for COVID-19 the patient was isolated and another nasal and oropharyngeal swab was performed. All patients have been asked to wear a surgical face mask during all hospital stay, in case of spinal anesthesia in the operating room too. After surgery, patients underwent post-operative (hip or knee) X-rays, serial blood checks and were transferred to the rehabilitation department within 72 hours of surgery. All healthcare workers involved during hospitalization used adequate personal protective equipment PPE (FFP2 or FFP3 masks and disposable gloves). The presence of relatives or carers was forbidden during hospitalization except in exceptional cases that followed the same protocol performed for patients. All procedures performed were in accordance with the 1964 Helsinki declaration. This research has been approved by the IRB of the authors’ affiliated institutions. Written informed consent for scientific purposes and clinical data collection and publication was obtained for each patient according to institutional protocol.
Results
A total of 147 patients underwent total knee replacement surgery in the analyzed period. Overall, 31 patients (21%) were treated during the pandemic period, while 116 (79%) in the post-pandemic period, with a mean increment of surgical activity of 374%.
Concerning ASA score, 29 (93.5%) patients treated during the pandemic period had an ASA II score while 2 (6.5%) had an ASA III score. Among the patients treated during the post-pandemic period, 98 had an ASA II score, while 18 (15.5%) had an ASA III score.
All patients received an intravenous antibiotics prophylaxis with Cephazolin 2g according to our institutional protocols.11 All patients treated during the pandemic period were operated on with selective spinal anesthesia, while during the post-pandemic period 101 patients were operated on with selective spinal anesthesia and 15 with general anesthesia.
The mean surgical time was 77.6 (+/-18.9). The intraoperative mean blood loss was 54 (+/-28) ml (a division for the two groups is reported in Table 1). No surgical drains were placed during surgery according to the Literature evidence.12
The mean hospital stay was 3-4 days (a division for the two groups is reported in Table 1). Eleven patients needed a blood transfusion in the postoperative period. Three patients, treated during the post-pandemic period needed postoperative intensive care, for a duration of fewer than 48 hours. One patient treated during the post-pandemic period had a periprosthetic tibial fracture during rehabilitation caused by an accidental fall, therefore underwent revision surgery. Two superficial wound infection was observed during the rehabilitation period and treated with antibiotic therapy.
Among the treated patients no case of COVID-19 infection was observed. During the study period, five cases of COVID-19 infection among medical or paramedical teams non directly involved in surgical and medical treatment of the enrolled patients were observed; all positive workers were promptly subjected to home isolation until recovery. All hospital staff was screened with nasal swabs at regular intervals (approximately every 15 days) to reduce the risk of patient infection.
Discussion
Most of the reports on the reorganization of health resources to cope with the COVID-19 emergency and on the protocols concerning the management of non-COVID hospital patients were conceived in the initial phase of the global pandemic.1,13 Despite the rationalization of resources representing a crucial point in emergency management, the restart of elective surgical activity is necessary for the health economic balance; in fact without the financial income provided by the elective procedures, the financial burden for hospital organizations will only increase.6,14
The development and application of a standardized protocol for the treatment of elective patients during a new pandemic wave remain a topic of debate.15 In fact, the European Hip Society and European Knee Associates in a recent paper suggest the need to implement specific protocols in the patient pathway for primary arthroplasty, without prejudice to the common national and local guidance rules, for a safe return to orthopedic elective surgery.3 However, despite the use of these protocols, the limited availability of beds in the intensive care units represents a strong limit to the restart of elective surgery. In this context, the patient choice could play an important role so much so that, ESSKA guidelines recommended reserving the priority of treatment to the younger patients, who need fewer days of hospitalization and are subject to fewer perioperative complications.16 The AAHKS Research Committee advised postponing elective surgery for elderly patients (>75 years), especially if they had more of one comorbidity (e.g. cardiovascular, immunosuppression, active neoplastic disease, etc.).17 According to this recommendation, in our clinical practice, we try to limit surgical interventions in high-risk (ASA III or higher), multimorbid, or very elderly patients. This would reduce the risk of patient contagion and the need for intensive postoperative care, optimizing the use of hospital resources. In fact, analyzing our data, during the pandemic period only 7.5% of patients reported an ASA III score, and 15.5% in the post-pandemic period, with an average need for postoperative intensive care in 2% of patients.
A multidisciplinary team that involves anesthesiologists, orthopedists, and physiatrists in the workflow of the elective orthopedic patient is fundamental in reducing the average hospital stay, the number of perioperative complications, and also has a positive impact on the final outcome.17 These figures should cooperate in the therapeutic project planning of each patient undergoing TKA surgery.
According to our data, in fact, the presence of anesthesiologists dedicated to orthopedic surgery allowed almost 90% of surgery were performed under selective spinal anesthesia with considerable advantages in the clinical and peri-operative improved pain control, reduced opioid use and postoperative pulmonary complications, less postoperative nausea and vomiting, and probable reduction in postoperative cognitive impairment and delirium, especially in the elderly population; moreover is possible to reduce the risk of transmitting respiratory infection as the absence of manipulation of the airways and the use of mechanical ventilation allow to avoid the phenomenon of aerosolization by reducing the spread of pathogens in the environment, both in atomized form and deposited on all surfaces. The use of regional anesthesia offers additional benefits. Compared to general anesthesia, the reduced consumption of opiates and the absence of curarization decrease the risk of serious respiratory complications, the need for hospitalization in ICU, and the length of hospitalization. Compatibly with the type and duration of surgery and the patient’s clinical risk, a regional anesthesia technique should be favored whenever possible.18,19
With the aim of reducing the mean hospital stay, a correct implementation of a rehabilitation process (pre and post-operative) must be considered.20–23 Ideally, during this pandemic and post-pandemic period, the efforts of physiatrists should be aimed at achieving patient-specific home-based rehabilitation protocol.22,23 During the hospital stay in the rehabilitation ward physiatrists and physiotherapists should also: educate the treated patients on the possible red flags related to arthroplasty management and the use of appropriate devices (e.g. crutches, walkers, toilet seat, toilet chair). Finally, remote rehabilitation medicine systems, defined as telerehabilitation, it could represent an effective method for continuing rehabilitation at home, minimizing the risk of contagion for patients and healthcare workers.24 In our experience, the presence of an internal rehabilitation ward, ready to receive patients a few days after the surgery, allowed us to optimize rehabilitation protocols and reduce the total days of hospitalization, reducing healthcare costs and positively affecting the final clinical results. Furthermore, early referral of patients to rehabilitation wards does not appear to be a risk factor for contracting Covid-19 infection.
Conclusion
Despite the risk of a new epidemic wave, it remains our duty to ensure high standards of care for elective patients. The use of our protocol, developed ad hoc for the management of elective orthopedic patients, allowed the restart of elective orthopedic surgery in a safe and reproducible way with an average increase of 374% on surgical activity between the pandemic and post-pandemic periods without record cases of contagion among the treated patients. However, to date, it is difficult to predict the evolution of the COVID-19 pandemic, and the threat of a new lockdown, given the inexorable increase in daily infections, seems ever closer.