
Abstract
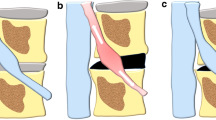
Background: Large lumbar or lumbosacral (LS) disc herniations usually expand from the paramedian space to the neuroforamen and compress both the transversing (lower) and the exiting (upper) nerve roots, thus leading to bi-radicular symptoms. Bi-radicular involvement is a statistically significant risk factor for poor outcome in patients presenting with far lateral or foraminal disc herniation after facet preserving microdecompression. There is evidence showing that patients suffering from large lumbar disc herniations treated with interbody fusion have significant superior results in comparison with those who received a simple discectomy We report our experiences on managing large LS disc herniation with bi-radicular symptoms by transforaminal lumbar interbody fusion (TLIF) using one diagonal fusion cage with unilateral pedicle screw/rod fixation.
Materials and Methods: Twenty-three patients who suffered from single level lumbar or LS disc herniation with bi-radicular symptoms treated with unilateral decompression and TLIF using one diagonal fusion cage with ipsilateral pedicle screw/rod fixation operated between January 2005 and December 2009, were included in this study. Operation time and blood loss were recorded. The pain and disability status were pre- and postoperatively evaluated by the visual analog score (VAS) and Oswestry Disability Index (ODI). Interbody bony fusion was detected by routine radiographs and computed tomography scan. Adjacent segment degeneration was detected by routine radiographs and magnetic resonance imaging examination. Overall outcomes were categorized according to modified Macnab classification.
Results: The patients were followed up for an average of 44.7 months. Pain relief in the VAS and improvement of the ODI were significant after surgery and at final followup. No severe complications occurred during hospital stay. Interbody bony fusion was achieved in every case. No cage retropulsion was observed, while 3 cases experienced cage subsidence. Adjacent segment degeneration occurred at 3 discs cephalic to the fusion segment at followup. No patients underwent revised surgery. Overall outcome was excellent in 5 patients (21.7%), good in 13 (56.5%), fine in 4 (17.5%), and poor in 1 (4.3%).
Conclusions: TLIF using one cage with ipsilateral pedicle screw/rod fixation is an effective treatment option for massive lumbar or LS disc herniation with bi-radicular involvement.
Similar content being viewed by others


References
Abdullah AF, Wolber PG, Warfield JR, Gunadi IK. Surgical management of extreme lateral lumbar disc herniations: Review of 138 cases. Neurosurgery 1988;22:648–53.
Chang SB, Lee SH, Ahn Y, Kim JM. Risk factor for unsatisfactory outcome after lumbar foraminal and far lateral microdecompression. Spine (Phila Pa 1976) 2006;31:1163–7.
O’Hara LJ, Marshall RW. Far lateral lumbar disc herniation. The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943–7.
Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976) 1988;13:696–706.
Kutlay M, Topuz K, Colak A, Simsek H, Cetinkal A, Demircan MN. Management of disc herniations with bi-radicular symptoms via combined lateral and interlaminar approach. Neurosurg Rev 2010;33:97–105.
Paolini S, Ciappetta P, Raco A, Missori P, Delfini R. Combined intra-extracanal approach to lumbosacral disc herniations with bi-radicular involvement. Technical considerations from a surgical series of 15 cases. Eur Spine J 2006;15:554–8.
Satoh I, Yonenobu K, Hosono N, Ohwada T, Fuji T, Yoshikawa H. Indication of posterior lumbar interbody fusion for lumbar disc herniation. J Spinal Disord Tech 2006;19:104–8.
Turner JA, Ersek M, Herron L, Deyo R. Surgery for lumbar spinal stenosis. Attempted meta-analysis of the literature. Spine (Phila Pa 1976) 1992;17:1–8.
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2001;26:1873–8.
Bambakidis NC, Feiz-Erfan I, Klopfenstein JD, Sonntag VK. Indications for surgical fusion of the cervical and lumbar motion segment. Spine (Phila Pa 1976) 2005;30 (16 Supp):S2–6.
Esses SI, Huler RJ. Indications for lumbar spine fusion in the adult. Clin Orthop Relat Res 1992;279:87–100.
Luk KD, Chow DH, Holmes A. Vertical instability in spondylolisthesis: A traction radiographic assessment technique and the principle of management. Spine (Phila Pa 1976) 2003;28:819–27.
Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976) 2001;26:567–71.
Zhao J, Hou T, Wang X, Ma S. Posterior lumbar interbody fusion using one diagonal fusion cage with transpedicular screw/rod fixation. Eur Spine J 2003;12:173–7.
Chitnavis B, Barbagallo G, Selway R, Dardis R, Hussain A, Gullan R. Posterior lumbar interbody fusion for revision disc surgery: Review of 50 cases in which carbon fiber cages were implanted. J Neurosurg 2001;95 2 Suppl: 190–5.
Kabins MB, Weinstein JN, Spratt KF, Found EM, Goei VK, Woody J, et al. Isolated L4-L5 fusions using the variable screw placement system: Unilateral versus bilateral. J Spinal Disord 1992;5:39–49.
Anandjiwala J, Seo JY, Ha KY, Oh IS, Shin DC. Adjacent segment degeneration after instrumented posterolateral lumbar fusion: A prospective cohort study with a minimum five-year followup. Eur SpineJ 2011;20:1951–60.
Cheh G, Bridwell KH, Lenke LG, Buchowski JM, Daubs MD, Kim Y, et al. Adjacent segment disease followinglumbar/ thoracolumbar fusion with pedicle screw instrumentation: A minimum 5-year followup. Spine (Phila Pa 1976) 2007;32:2253–7.
Okuda S, Iwasaki M, Miyauchi A, Aono H, Morita M, Yamamoto T. Risk factors for adjacent segment degeneration after PLIF. Spine (Phila Pa 1976) 2004;29:1535–40.
Wai EK, Santos ER, Morcom RA, Fraser RD. Magnetic resonance imaging 20 years after anterior lumbar interbody fusion. Spine (Phila Pa 1976) 2006;31:1952–6.
Lai PL, Chen LH, Niu CC, Fu TS, Chen WJ. Relation between laminectomy and development of adjacent segment instability after lumbar fusion with pedicle fixation. Spine (Phila Pa 1976) 2004;29:2527–32.
Najarian S, Dargahi J, Heidari B. Biomechanical effect of posterior elements and ligamentous tissues of lumbar spine on load sharing. Biomed Mater Eng 2005;15:145–58.
Chen Z, Zhao J, Xu H, Liu A, Yuan J, Wang C. Technical factors related to the incidence of adjacent superior segment facet joint violation after transpedicular instrumentation in the lumbar spine. Eur Spine J 2008;17:1476–80.
Kumar MN, Baklanov A, Chopin D. Correlation between sagittal plane changes and adjacent segment degeneration following lumbar spine fusion. Eur SpineJ 2001;10:314–9.
Lazennec JY, Ramaré S, Arafati N, Laudet CG, Gorin M, Roger B, et al. Sagittal alignment in lumbosacral fusion: Relations between radiological parameters and pain. Eur Spine J 2000;9:47–55.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Rights and permissions
About this article

Cite this article
Zhao, CQ., Ding, W., Zhang, K. et al. Transforaminal lumbar interbody fusion using one diagonal fusion cage with unilateral pedicle screw fixation for treatment of massive lumbar disc herniation. IJOO 50, 473–478 (2016). https://doi.org/10.4103/0019-5413.189595
Published:
Issue Date:
DOI: https://doi.org/10.4103/0019-5413.189595
Key words
- Bi-radicular involvement
- large disc herniation
- unilateral pedicle screw fixation
- lumbar disc
- transforaminal interbody fusion