
Abstract
Background
Mini-subvastus approach for Total Knee Arthropalsty allows a faster recovery. It is traditionally not utilized for obese patients because of difficulty in exposure of the knee and eversion of the patella. We hypothesized that obesity should not really cause a problem for patients undergoing a TKA with the mini-subvastus approach as the anatomy of the quadriceps in the obese and the nonobese patient population is the same. We present an analysis of the use of mini-subvastus approach in obese patients.
Materials and Methods
97 obese patients (109 knees) 81 females + 16 males with mean age 64 years underwent total knee arthroplasty (TKA) by mini-subvastus approach between January 2006 to July 2007.16 patients (18 kness)were morbidly obese. All patients were prospectively evaluated by pre- and postoperative Knee Society and function score. The average follow-up was 18 months (range from 1 to 3 years) with minimum 1 year follow-up.
Results
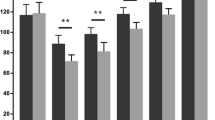
The approach provided adequate exposure in all knees, with an average surgical time of 90 minutes. The patella could be everted easily after the tibial and femoral cuts. The average Knee Society score improved from 42 to 89 and the function score from 48 to 65. The complications included medial collateral ligament injury (one case) and patellar tendon avulsion (one case).
Conclusion
Our results compare favorably with other reported series in obese patients. The mini-subvastus approach can be considered in obese patients.
Similar content being viewed by others


References
Leach RE, Baumgard S, Broom J. Obesity: its relationship to osteoarthritis of the knee. Clin Orthop Relat Res 1973;93:271–3.
Felson DT, Anderson JJ, Naimark A, Walker AM, Meenan RF. Obesity and knee osteoarthritis. The Framingham Study. Ann Intern Med 1988;109:18–24.
Amin AK, Clayton RA, Patton JT, Gaston M, Cook RE, Brenkel IJ. Total knee replacement in morbidly obese patients. Results of a prospective, matched study. J Bone Joint Surg Br 2006;88:1321–6.
Foran JR, Mont MA, Etienne G, Jones LC, Hungerford DS. The outcome of total knee arthroplasty in obese patients. J Bone Joint Surg Am 2004;86:1609–15.
Winiarsky R, Barth P, Lotke P. Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am 1998;80:1770–4.
Hofmann AA, Plaster RL, Murdock LE. Subvastus (Southern) approach for primary total knee arthroplasty. Clin Orthop Relat Res 1991;269:70–7.
Matsueda M, Gustilo RB. Subvastus and medial parapatellar approaches in total knee arthroplasty. Clin Orthop Relat Res 2000;371:161–8.
Scuderi GR, Tenholder M, Capeci C. Surgical approaches in mini-incision total knee arthroplasty. Clin Orthop Relat Res 2004;428:61–7.
Boerger TO, Aglietti P, Mondanelli N, Sensi L. Mini-subvastus versus medial parapatellar approach in total knee arthroplasty. Clin Orthop Relat Res 2005;440:82–7.
Scuderi RG, Tria JA. Insall and scott’s textbook of knee surgery. 4th ed. page 1634. 2006
Engh GA. Midvastsus approach. In: Scuderi GR, Tria AJ Jr, editors. Surgical Techniques in Total Knee Arthroplasty. New York: Springer-Verlag; 2002. p. 127–30.
Kim JM, Choi NY, Kim SJ. Large thigh girth is a relative contraindication for the subvastus approach in primary total knee arthroplasty. J Arthroplast 2007;22:4.
Bonutti PM, Mont MA, Kester MA. Minimally invasive total knee arthroplasty: A 10-feature evolutionary approach. Orthop Clin N Am 2004;35:217–26.
Benoni G, Fredin H. Fibrinolytic inhibition with tranexamic acid reduces blood loss and blood transfusion after knee arthroplasty: A prospective, randomised, double-blind study of 86 patients. J Bone Joint Surg Br 1996;78:434–40.
Ewald FC. The Knee Society total knee arthroplasty roentgenographic valuation and scoring system. Clin Orthop Relat Res 1989;284:9–12.
Leopold S, McStay C, Klafeta K, Jacobs JJ, Berger RA, Rosenberg AG. Primary repair of intraoperative disruption of the medial collateral ligament during total knee arthroplasty. J Bone Joint Surg Am 2001;86:86.
Dalury DF, Dennis DA. Mini-incision total knee arthroplasty can increase risk of component malalignment. Clin Orthop Relat Res 2005;440:77–81.
Hass SB, Cook S, Beksac B: Minimally invasive total knee replacement through a mini midvastus approach: A comparative study. Clin Orthop Relat Res 2004;428:68–73.
Laskin RS. Minimally invasive total knee arthroplasty: the results justify its use. Clin Orthop Relat Res 2005;440:54–9.
Parentis MA, Rumi MN, Deol GS, Kothari M, Parrish WM, Pellegrini VD Jr. A comparison of the vastus splitting and the median parapatellar approaches in total knee arthroplasty. Clin Orthop Relat Res 1999;367:107–16.
Stern SH, Insall JN. Total knee arthroplasty in obese patients. J Bone Joint Surg Am 1990;72:1400–4.
Rand JA, Morrey BF, Bryan RS. Patellar tendon rupture after total knee arthroplasty. Clin Orthop Relat Res 1989;244:233.
Lynch AF, Rorabeck CH, Bourne RB. Extensor mechanism complication following Total Knee Arthroplasty. J Arthropalst 1987;2:135–40.
Argenson JN, Vinel H, Aubaniac JM. Total knee arthroplasty for the stiff knee. Osteoarthritis of the Knee. Paris: Springer; 2008. p. 315–21.
Tarabichi S, Tarabichi Y. Can an anterior quadriceps release improve range of motion in the stiff arthritic knee? J Arthroplast 2010;25:571–5.
Tenholder M, Clarke HD, Scuderi GR. Minimal-incision total knee arthroplasty: The early clinical experience. Clin Orthop Relat Res 2005;440:67–76.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shah, N., G, N. & Patel, N. Mini-subvastus approach for total knee arthroplasty in obese patients. IJOO 44, 292–299 (2010). https://doi.org/10.4103/0019-5413.65157
Published:
Issue Date:
DOI: https://doi.org/10.4103/0019-5413.65157