SVT Therapy – Yesterday, Today and Tomorrow?
This essay is a brief review of advances in treatment of patients with supraventricular tachycardia (SVT) over the past 55 years. We review the knowledge base available in terms of arrhythmia diagnosis and the limited availability of drug therapy. Significant advances resulted in the introduction of direct-current defibrillators as well as introduction of ambulatory ECG recordings. We also witnessed a tremendous increase in an understanding of the mechanisms of SVT which in turn led to the development of first surgical and subsequently catheter based techniques for localization and ablation of foci or pathways responsible for arrhythmias. More recently, surgical and catheter techniques have been introduced in an attempt to cure atrial fibrillation. These techniques have proven especially effective for those with paroxysmal atrial fibrillation and less effective for those with long standing persistent fibrillation. The future brings hope for more extensive use of non-invasive techniques both to diagnose arrhythmia mechanisms together with techniques to ablate cardiac foci without patient instrumentation and finally in the use of gene therapy for patients with cardiac arrhythmia.
Correspondence to:
Treatment of Supraventricular tachycardia (SVT) – then and now
For this essay, I decided to restrict myself from the time I entered medical school (1956) to the present. It must be said at the onset that in this short essay one could not possibly list all the individuals who have made major contributions, therefore, I offer apologies for any omissions.
Our characterization of supraventricular arrhythmias was actually fairly well developed by the 1950s ([Fig1]). Uses of the electrocardiogram to diagnose rhythm disorders were well established and clinicians interested in cardiology routinely used an ECG machine. The anatomy of the specialized conduction system pioneered by the work of Tawara and His [1] were widely appreciated. Furthermore, due to the efforts of the past masters (i.e. Sir Thomas Lewis, Wenkebach, Scherf, Mines, Pck, and Langerdoff), we were taught to recognize the ECG pattern of atrial fibrillation, atrial flutter as well as, paroxysmal supraventricular tachycardia.
Figure 1.
The Wolff-Parkinson-White (WPW) Syndrome
In 1930, Drs. Wolff, Parkinson, and White described a clinical syndrome characterized by a short PR interval and SVT. [2] Prior to this report, isolated case reports were described by others [3],[4] but the report by Drs. Wolff, Parkinson, and White was the largest and most complete description of the syndrome which is now recognized as an important cause of SVT.
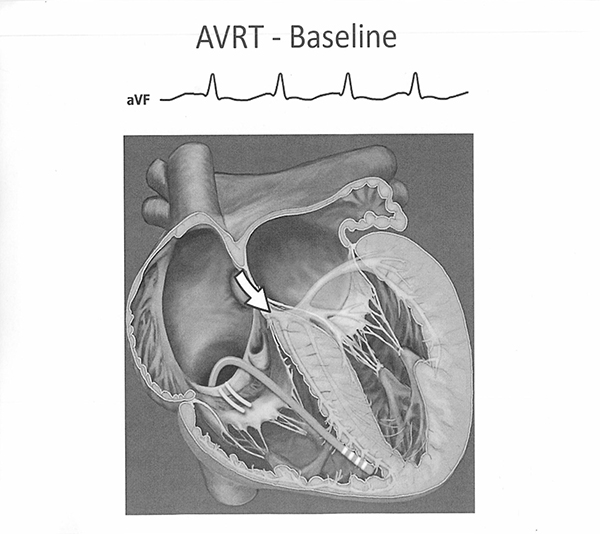
The mechanism of the tachycardia is now well established and is due to differences in the conduction and refractoriness between the AV node – His axis and the accessory pathway. The WPW pattern is recognized as a fusion complex due to simultaneous activation of the AV node – His axis and ventricular myocardium via the accessory pathway ([Fig2])
Figure 2.
Special attention is focused on the masterful work of Pick and Langendorf [5],[6] where by painstaking analyses, discovered so many of the concepts that underlie our present understanding of supraventricular tachycardia. For example, their contribution to our understanding of the genesis of SVT as it relates the Wolf Parkinson’s White syndrome is illustrated in [Fig3]. They also recognized the relationship of atrial fibrillation to the WPW syndrome.
Figure 3.
While diagnostic criteria separating SVT from other arrhythmias, as well as, the various types of SVT were well appreciated, available treatment options were rather limited [Fig4]. For example, digitalis preparations were the prime drugs used for either acute or chronic management of SVT. We used very rapid acting preparations (i.e. acetyl strophanthidin) for acute rhythm control of SVT or Atrial fibrillation and oral digoxin for chronic treatment. We were taught to administer these drugs to the onset of side effects and then to back off for chronic administration. It is a small wonder that we have so many instances of arrhythmias attributed to digitalis toxicity, an entity which is seldom seen in contemporary cardiology practice. Oral Quinidine was used for attempted conversion of atrial fibrillation to sinus rhythm as well as for attempted rhythm control in those with paroxysmal or permanent atrial fibrillation. As with the digitalis medications, untoward side effects (especially diarrhea) were fairly common with chronic Quinidine use. The rest of the therapeutic arsenal contained intra venous procainamide for ventricular tachycardia as well as atropine or isoproterenol for bradycardia.
The early 1960s were especially noteworthy with the introduction of the direct-current defibrillation [7]. This device had a truly remarkable effect in terms of prompt reversion of SVT or VT to sinus rhythm and truly revolutionized care of seriously ill cardiac patients. This innovation rivaled the introduction of permanent pacemakers for treatment of bradycardia. Another revolutionary contribution in the early 1960s was the introduction of ambulatory ECG monitoring by Holter which led to the concept of prolonged monitoring in specialized units championed by Dr. Lown. The late 60s were noteworthy for the introduction of electrical stimulation of the heart first introduced by Wellens and Durrer [8],[9] whose work actually laid the foundation for our current understanding of the mechanisms of SVT. This was well established even before our potential ability to record the His bundle electrogram [10].
Figure 4.
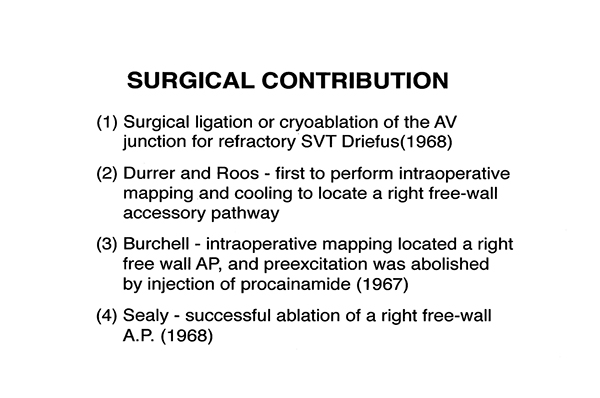
In addition, we must give homage to the impressive contributions of our surgical colleagues [fig5]. In the 1960s, patients with SVT refractory to drug therapy were treated with cardiotomy and direct ligation or cryoablation of the AV junction which, of course, required permanent pacing. Durrer and Roos were the first to perform intraoperative mapping and cooling to locate a free wall accessory pathway at the time of cardiotomy [11] subsequently Burchell used intra-operative mapping to locate a right-sided accessory pathway whose function was temporarily abolished by local injection of procainamide. It was left for Dr. Sealy to be accorded the honor of being the first surgeon to successfully and permanently ablate an accessory pathway [12].
Figure 5.
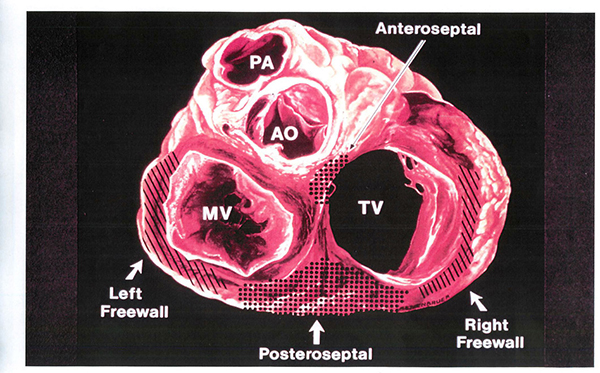
The surgeons in the ensuing decade showed that accessory pathways in any location were amendable to ablation. They defined the anatomic regions in which pathways were located [fig 7] and served as the bases for the development of catheter ablative techniques.
Figure 7.
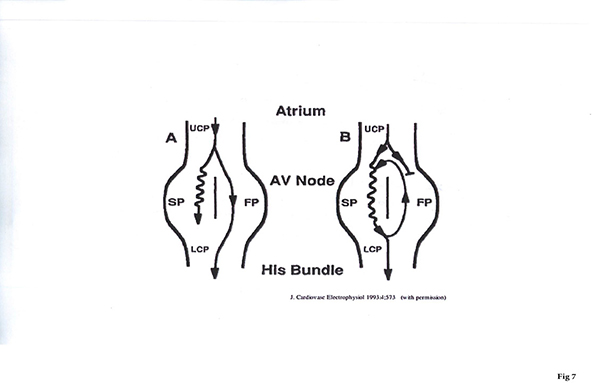
AV nodal reentry is the most common mechanism of SVT. Evidence for duality of nodal conduction was initially described by Mendez and Moe in 1966. [13] A schema often used to describe this mechanism is shown in [fig6]. In the typical form an atrial premature beat is blocked in the normal (or fast pathway) and conducts slowly over the slow pathway and returns to the fast pathway when it is no longer refractory and give rise to an echo beat or to sustained tachycardia.
The earliest description of a non-pharmalogic approach for cure of AVNRT was described by Ross et al in 1985 [14]. Catheter techniques targeting the fast pathway was introduced in 1989 [15] and the current approach targeting the slow pathway was introduced by Jackman et al in 1993 [16]. This technique was associated with a very high incidence of arrhythmia cure and a low incidence of AV block. This technique is still the preferred method for ablative cure of AVNRT.
Figure 6.
The early 80s witnessed the birth of catheter techniques for ablation of either the AV junction or accessory pathways [fig6]. The initial catheter technique involved use of high energy direct-current discharges in the region of the compact node [17]. Subsequently, a similar technique was used for successful ablation of posteroseptal accessory pathways [18]. In the late 1980s, high energy direct-current discharge was replaced by radio frequency energy which proved to be much safer and more applicable to ablation of a wide variety of SVTs. Use of radiofrequency energy was introduced by Borgreffe and Breithardt in Europe [19] and by Huang and Marcus in the United States. This technique avoided the intense barotrauma associated with high energy direct current shocks and served as a vital catalyst to external ablative procedures to a wide variety of SVTs. These included ablation of the slow pathway for AV nodal reentry [16] as well as ablative procedures for atrial tachycardia as well as atrial flutter.
In the 1990s, we witnessed the introduction of mapping techniques [fig8] which allowed for better elucidation of tachycardia pathways and allowed for expansion of ablative techniques to complex atrial (or ventricular) tachycardia circuits. Prior to the three-dimensional mapping, even the clinician was obliged to remember the sequence of activation points which was quite cumbersome for complicated tachycardia circuits.
Figure 8.

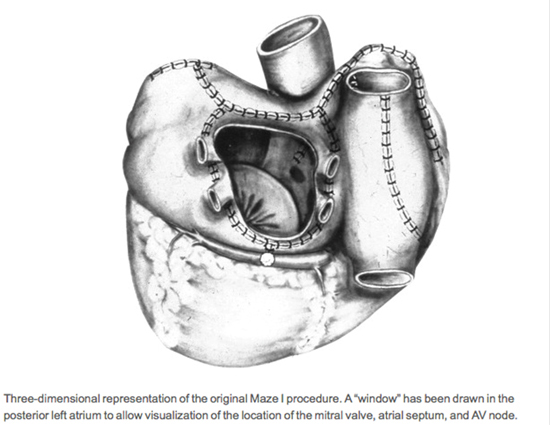
The 1990s also witnessed the introduction of the Cox maze procedure for cure of atrial fibrillation [20]. The original maze procedure involved a cut and sew approach for isolation of wide areas of the posterior left atrium, removal of the left atrial appendage as well as construction of a variety of surgical lines connecting the left atrial room as well as the mitral isthmus [Fig9]. The original procedure also involved creation of surgical lines in the right atrium (i.e. intercaval and CTI lines). This procedure was associated with an astonishingly high success rate but had to be modified because of the high incidence of sinus node dysfunction and because of the length of the procedure. The original Cox procedure has been modified and is still in use today primarily for these patients with atrial fibrillation who require cardiac surgical procedures for other reasons (i.e. valvular or coronary artery disease).
Figure 9.
The 21st century has witnessed a veritable explosion of newer techniques for ablative cure of atrial fibrillation. We now appreciate the importance of rapid electrical discharge from the left atrial muscles that coat the pulmonary veins [21]. Initial attempts involved localization of the vein(s) that harbored the discharging impulses but we have subsequently learned the importance of total isolation of both the pulmonary veins as well as the surrounding left atrium [22]. A number of ancillary techniques have been introduced to improve the results of catheter ablation for cure atrial fibrillation. These include construction of ablation lesions to connect the left atrial roof as well as the mitral isthmus as adjunctive therapy in difficult cases [23] The incremental effectiveness of these lines are still a matter of debate.
In addition, we have learned a great deal about the pathophysiology of atrial fibrillation. There, however, is still debate about the importance of rotor activity as well as techniques introduced to identify and ablate rotor activity [24]. In addition, the value of ablation of complex fractionated potentials [25] has not been established. A host of other factors appear to play important roles in the genesis and maintenance of atrial fibrillation including the role of the intrinsic cardiac anatomic ganglionic plexi (Scherleg, Jackman) as well as the role of inflammation. In some families, genetic mutations involving the cardiac sodium or potassium channels appear to play an important role in the geneses of atrial fibrillation.
As opposed to the rapid development of catheter ablative techniques for treatment of Atrial Fibrillation, development of newer drug therapy has been disappointing. For example, attempts to develop drugs that specifically target K+ channels that are seen in atrial tissue alone (i.e. iKur) have not proved helpful. Early in vitro and animal studies show that specific blockers of the late sodium current may prove of value in controlling Atrial Fibrillation.
A Glimpse into the Future
As pointed out, the last six decades have brought incredible advances in the management of patients with complex cardiac rhythm disturbances. Looking into the crystal ball, I think the future portends a greater emphasis on non-invasive techniques for better diagnosis and treatment of rhythm disturbances. Among these advances are the development of external recordings from the chest wall to accurately map complex tachycardia circuits such as the ECGI technique developed by Dr. Ruddy [26]. This technique promises to give clinicians important insights into tachycardia mechanisms prior to taking the patient to the catheter laboratory. Moreover, we are witnessing the development external beam radiation to target specific areas involved in maintain or initiation of tachycardia. Early uses of these procedures clinically have already been reported [27]. Finally, a variety of techniques have been used in animal models to introduce genes that modify channel or protein functions to cure disease. Some of the outstanding developments include the work of Kevin Donohue involving the introduction of a mutation responsible for prolongation of the atrial action potential and showing that treated animals become resistant to pacing induced atrial fibrillation. [28] In addition, Priori has developed a mutation that results in gain of function of the CASQ2 gene which both prevents development of CPVT as well is effective in reversal of signs of CPVT (i.e. bidirectional VT) in mice. [29].
It is clear that brilliant pioneers as well as technological developments have achieved a great deal. In addition, the future including more use of non-invasive techniques as well as development of gene therapy adds great potential to our goal of curing cardiac rhythm disturbances.






