

Abstract
Objective. To evaluate the clinical significance of the 2016 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR)/Pediatric Rheumatology International Trials Organization (PRINTO) classification criteria for macrophage activation syndrome (MAS) in patients with adult-onset Still disease (AOSD).
Methods. We performed a retrospective analysis of patients with AOSD with fever who were admitted to Severance Hospital between 2005 and 2016. The patients with AOSD were evaluated for MAS using the 2016 classification criteria for MAS. Clinical features, laboratory findings, and overall survival were analyzed. Logistic regression analysis was used to evaluate the factors associated with in-hospital mortality.
Results. Among 64 patients with AOSD, 36 (56.3%) were classified as having MAS. The overall survival rate was significantly lower in patients with MAS than in those without (67% vs 100%, p < 0.001). Multivariate analysis showed that a low erythrocyte sedimentation rate, a low albumin level, an increase in ferritin of over 2 folds, and the development of MAS on admission were significantly associated with mortality in patients with AOSD.
Conclusion. The 2016 EULAR/ACR/PRINTO classification criteria for MAS are potentially useful for the identification of patients with AOSD at high risk for a poor outcome. Febrile patients with AOSD should be monitored with the 2016 classification criteria for MAS in the early diagnosis and proper treatment of MAS.
- MACROPHAGE ACTIVATION SYNDROME
- ADULT-ONSET STILL DISEASE
- SYSTEMIC JUVENILE IDIOPATHIC ARTHRITIS
- FERRITIN
Adult-onset Still disease (AOSD) is a rare systemic inflammatory disease with the characteristic features of quotidian fever, arthritis, evanescent rash, and leukocytosis. Other common clinical features include sore throat, lymphadenopathy, hepatosplenomegaly, and abnormal liver function test results. Nonsteroidal antiinflammatory drugs (NSAID) are the initial drugs of choice in mild cases1, while steroids are the first-line treatments in patients with systemic manifestations2. In steroid-refractory cases, potent immunosuppressive treatment is required3,4. Although the overall prognosis of the disease is known to be favorable, the natural course of the disease is often dismal, especially in steroid-refractory cases. However, it is difficult to predict the outcome owing to the wide range of responses to steroid treatment.
Macrophage activation syndrome (MAS) involves acute systemic inflammation arising in the context of various autoimmune and autoinflammatory conditions, and is seen most commonly in cases of systemic juvenile idiopathic arthritis (sJIA)5. It is potentially life-threatening, and it requires early diagnosis and aggressive treatment. Although MAS has not been reported to be common in patients with AOSD, it is known to be a fatal complication of AOSD6,7,8. The early diagnosis of MAS is considered difficult because there are no pathognomonic findings or disease-specific laboratory markers. Although hemophagocytic histiocytes are frequently seen in the bone marrow or liver of patients with MAS, their occurrence in these organs is not specific to MAS and may not be apparent in the early stage of MAS9. Recently, the European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR)/Pediatric Rheumatology International Trials Organization (PRINTO) Collaborative Initiative group developed new criteria for the classification of MAS in patients with sJIA10,11. Validation of the 2016 classification criteria for MAS showed that MAS was identifiable in cases of sJIA, with a sensitivity of 0.73 and a specificity of 0.99. AOSD is considered an adult counterpart of sJIA because both these conditions share clinical features, including high fever, rash, joint pain, and lymphadenopathy. Therefore, we evaluated the clinical significance of the 2016 EULAR/ACR/PRINTO classification criteria for MAS in patients with AOSD.
MATERIALS AND METHODS
Patient selection
We retrospectively reviewed the electronic medical records of patients admitted to Severance Hospital and collected the clinical and laboratory data of patients who were hospitalized owing to fever and AOSD between December 1, 2005, and May 31, 2016. Patients with documented fever, defined as a body temperature of over 37.8°C during the admission period12, were included. Patients with fever that was not considered attributable to the activity of AOSD and those who did not undergo testing for the serum ferritin level were excluded. Finally, 64 patients were analyzed, and all patients fulfilled the Yamaguchi criteria for AOSD13. As part of the diagnostic procedure, cancer and infectious diseases were evaluated during hospitalization with microbial cultures (blood, urine, and sputum), echocardiography, imaging tests of chest and abdomen (radiograph, ultrasound, and/or computed tomography), and tests for human immunodeficiency virus and tuberculosis. This study was approved by the Institutional Review Board (IRB) of Severance Hospital and was performed in accordance with the principles set forth in the Declaration of Helsinki (IRB protocol number 4-2016-0280).
Definition of MAS and classification of patients
The 2016 EULAR/ACR/PRINTO classification criteria for MAS are based on clinical data of patients with sJIA, and they are highly specific for detecting the development of MAS in sJIA. Although these criteria have not been validated in patients with AOSD, we applied the criteria to our patients with AOSD because AOSD is considered an adult counterpart of sJIA. In our study, patients were classified as having MAS if they had fever and a ferritin level ≥ 684 ng/ml, and fulfilled more than 2 of the following 4 criteria: platelet count ≤ 181,000/µl, aspartate aminotransferase (AST) level > 48 units/l, triglyceride level > 156 mg/dl, and fibrinogen level ≤ 360 mg/dl. Patients with MAS were further divided into the following 2 groups: those who already had MAS at admission and those who developed MAS after admission.
Clinical and laboratory data collection and definition of ferritin fold increase
Clinical data were collected: age, sex, body temperature, and presence of arthritis, rash, leukocytosis, sore throat, lymphadenopathy, and hepatosplenomegaly. Glucocorticoid dosage per day was calculated by dividing the total steroid dosage used during hospitalization by the number of days of steroid use, and was expressed in prednisolone-equivalent dosage. Baseline laboratory data were white blood cell (WBC) and platelet counts, erythrocyte sedimentation rate (ESR), and levels of hemoglobin, C-reactive protein (CRP), blood urea nitrogen, creatinine, AST, alanine aminotransferase (ALT), total bilirubin, total protein, albumin, ferritin, lactate dehydrogenase (LDH), fibrinogen, and triglycerides. Because the fibrinogen and triglyceride levels were not measured regularly, both the levels were included for analysis when the results were obtained within 3 days of the date of laboratory data selection. Ferritin fold increase was calculated by dividing the maximum level of ferritin during admission by the baseline ferritin level.
Evaluation of the hemophagocytic syndrome score (HScore) in patients with AOSD with and without MAS
The HScore was developed to estimate an individual’s risk of having reactive hemophagocytic syndrome14. We further evaluated the HScore in our study population and compared the probability of having hemophagocytic syndrome between patients classified as having MAS and not having MAS according to the 2016 EULAR/ACR/PRINTO classification criteria. As previously described, the HScore and probability of having hemophagocytic syndrome were calculated by using the calculator available online (saintantoine.aphp.fr/score). In addition, the in-hospital mortality rates between patients with the probability of having hemophagocytic syndrome ≥ 80% and < 80%, without MAS, were also calculated.
Statistical analysis
For normally distributed data, continuous variables are presented as means with SD, while non-normally distributed data are presented as medians with interquartile ranges (IQR). Categorical variables are expressed as frequencies and percentages. For continuous variables, comparisons of different groups were performed using the Student t test or the Mann-Whitney U test as appropriate, and for categorical variables, comparisons were performed using the chi-square test or Fisher’s exact test. The probability of survival in patients with MAS and those without was calculated using the Kaplan-Meier method and the log-rank test. Risk factors for in-hospital mortality in patients with AOSD were determined by performing univariate and multivariate analyses with a forward stepwise logistic regression. The multivariate forward stepwise logistic regression included only factors that were statistically significant in the univariate analysis model. OR and 95% CI were calculated, and a 2-tailed p value < 0.05 was considered statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences software version 21 (SPSS Inc.) and the MedCalc statistical software version 16.2.0 (MedCalc Software bvba).
RESULTS
Baseline characteristics of the AOSD patients with and without MAS
There were 71 patients with AOSD who were hospitalized because of fever during the study period. Among those patients, 3 were excluded because their fever was due to infection, and an additional 4 patients were excluded because ferritin level was not measured on admission. Among the remaining 64 patients with AOSD, 36 (56.3%) were found to be classified as having MAS during the admission period (Table 1). Of these 36 patients, 22 (61.1%) had MAS at admission and 14 (38.9%) developed MAS after admission. On comparing the baseline characteristics between patients with and without MAS, we noted that the proportion of female patients was higher in patients with MAS than in those without MAS. Regarding laboratory variables, the platelet count, ESR, total protein level, and fibrinogen level were lower, and the AST, ALT, LDH, ferritin, and triglyceride levels were higher in patients with MAS than in those without. No differences in sex were noted between patients with MAS at admission and those who developed MAS after admission. However, the platelet count and ESR were lower and the LDH and triglyceride levels were higher in patients with MAS at admission than in those who developed MAS after admission. There was no difference between groups in clinical manifestations (Supplementary Table 1, available with the online version of this article). Among 64 patients, 26 had undergone a bone marrow study; 18 belonged to the MAS during admission group, and 8 belonged to the group without MAS. Among 18 patients with MAS, hemophagocytosis was observed in 9 patients, whereas none of the patients without MAS had hemophagocytosis in a bone marrow study.
Baseline characteristics of the patients with AOSD. Values are median (interquartile range) unless otherwise specified.
Comparison of overall survival according to MAS and ferritin
We analyzed the prognosis of patients according to the presence of MAS and ferritin fold increase (Figure 1). Among the 64 patients included in our study, in-hospital mortality was noted in 12 patients. In-hospital mortality was not noted in patients without MAS. Overall survival was significantly lower in patients with MAS than in those without MAS (66.6% vs 100.0%, p < 0.001; Figure 1A). Additionally, overall survival was lower in patients with ferritin fold increase ≥ 2.0 than in those with ferritin fold increase < 2.0 (65.2% vs 90.2%, p = 0.014; Figure 1B).
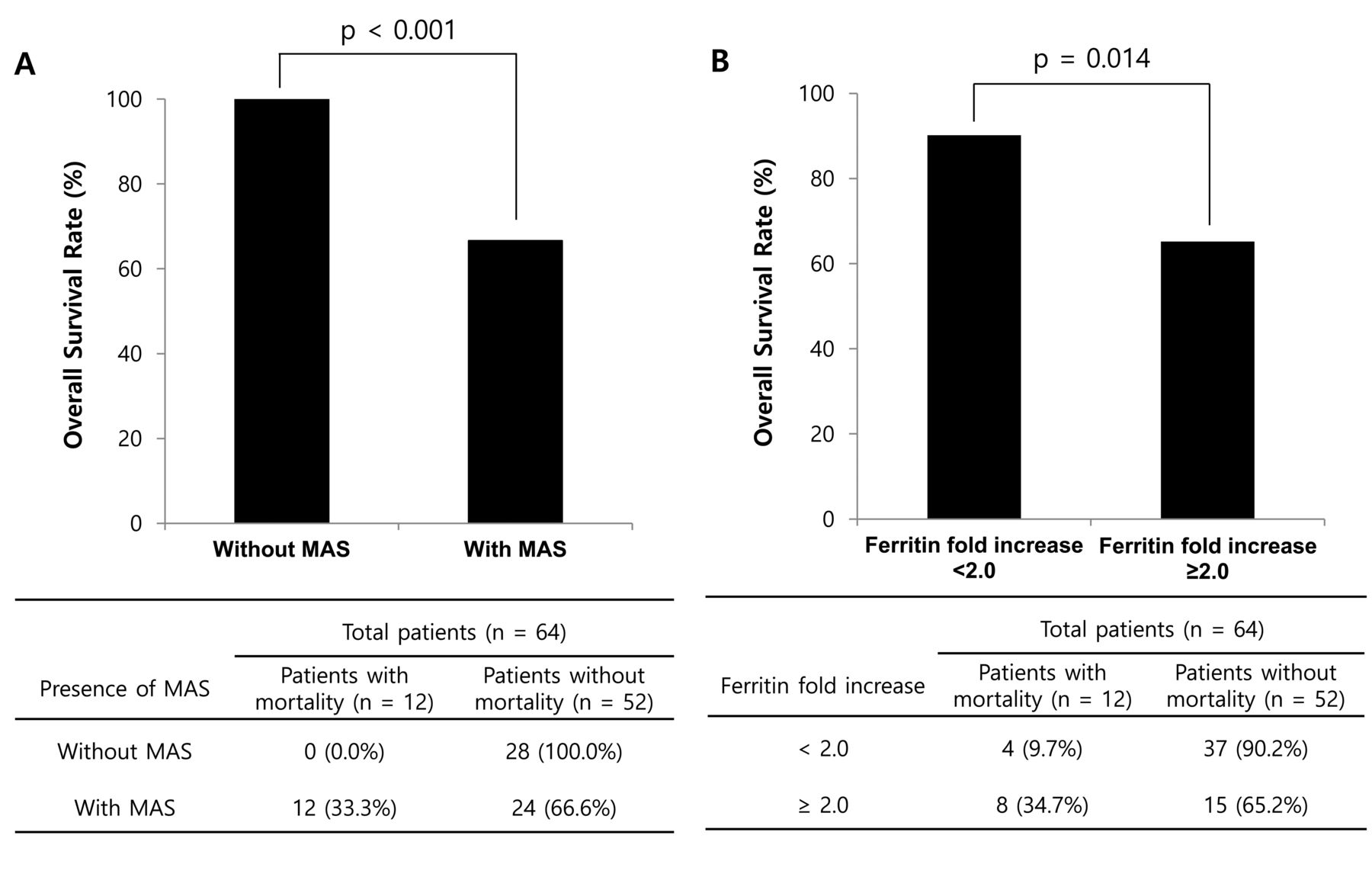
Comparison of the overall survival rate in patients with AOSD. (A) Survival rate comparison between patients with and those without MAS. (B) Survival rate comparison according to changes in the ferritin level. Ferritin fold increase was calculated by dividing the maximum level of ferritin during admission by the ferritin level at admission. AOSD: adult-onset Still disease; MAS: macrophage activation syndrome.
Evaluation of the HScore in AOSD patients with and without MAS
The absolute HScore and probability of having hemophagocytic syndrome was compared between patients who were classified as having and not having MAS according to the 2016 EULAR/ACR/PRINTO classification criteria. A comparison of the HScore between both groups showed that patients with MAS had a higher HScore and probability of having hemophagocytic syndrome than those without MAS (p < 0.001; Figure 2A and Figure 2B). Further, patients with MAS with the probability of having hemophagocytic syndrome ≥ 80% had a higher in-hospital mortality rate than those with MAS with a probability of having hemophagocytic syndrome < 80% and patients without MAS during the admission period (Figure 2C).

Evaluation of the HScore and probability of having hemophagocytic syndrome in AOSD patients with MAS. The HScore was compared between patients with and without MAS. In-hospital mortality between patients with the probability of having hemophagocytic syndrome ≥ 80% and < 80%, without MAS, was also compared. (A) Comparison of the absolute HScore between the groups. (B) Comparison of the probability of having hemophagocytic syndrome between the groups. (C) Comparison of the in-hospital mortality rate in patients with probability of having hemophagocytic syndrome ≥ 80% and < 80%, without MAS. Data are expressed as the means and 95% CI. * p < 0.05. ** p < 0.01. *** p < 0.001. HScore: hemophagocytic syndrome score; AOSD: adult-onset Still disease; MAS: macrophage activation syndrome.
Comparison of the use of glucocorticoids and other immunosuppressive agents in patients with AOSD
A comparison of the use of glucocorticoids and immunosuppressive agents in patients with and without MAS showed that patients with MAS were treated more aggressively, including a higher glucocorticoid dosage and more frequent cyclosporine, etoposide, and intravenous (IV) immunoglobulin use, than those without MAS (Supplementary Table 2, available with the online version of this article). In addition, to evaluate the effect of treatment on patients’ outcome, the medication usage was compared between patients with MAS with in-hospital mortality and those without in-hospital mortality. Compared to patients without in-hospital mortality, the treatment option used in patients with in-hospital mortality differed only regarding IV immunoglobulin usage (Supplementary Table 2, available with the online version of this article).
Risk factors for in-hospital mortality in patients with AOSD
To analyze the risk factors for in-hospital mortality in patients with AOSD during admission, we performed logistic regression analysis with a forward stepwise method. In univariate logistic regression analysis, these variables were associated with in-hospital mortality: ESR (OR 0.972, p = 0.009), total protein level (OR 0.184, p = 0.005), albumin level (OR 0.202, p = 0.018), LDH level (OR 1.001, p = 0.022), ferritin level (OR 1.000, p = 0.020), ferritin fold increase of ≥ 2 (OR 4.933, p = 0.019), and MAS at admission (OR 9.000, p = 0.003). Multivariate logistic regression analysis showed that these were significant risk factors for in-hospital mortality in patients with AOSD (Table 2): ferritin fold increase of ≥ 2 (OR 18.276, 95% CI 1.749–190.966, p = 0.015), MAS at admission (OR 10.321, 95% CI 1.094–97.308, p = 0.041), ESR (OR 0.965, 95% CI 0.934–0.997, p = 0.033), and albumin level (OR 0.138, 95% CI 0.019–0.976, p = 0.047).
Univariate and multivariate logistic regression analyses of in-hospital mortality among patients with adult-onset Still disease.
Kaplan-Meier survival analysis of patients with AOSD according to MAS development
There were 9 deaths among patients with MAS at admission and 3 deaths among patients who developed MAS after admission. Kaplan-Meier analysis with the log-rank test showed that the in-hospital mortality rate was higher in patients with MAS at admission and patients who developed MAS after admission than in those without MAS (MAS at admission vs without MAS, p < 0.001; MAS after admission vs without MAS, p = 0.013; Figure 3). However, there was no difference in the in-hospital mortality rate between patients with MAS at admission and those who developed MAS after admission (p = 0.208). Of the 12 cases of in-hospital mortality, 8 (66.6%) resulted from multisystem organ failure and 4 (33.3%) from secondary infections during admission. The median number of days from the diagnosis to death was 17.0 (IQR 9.0–34.0).
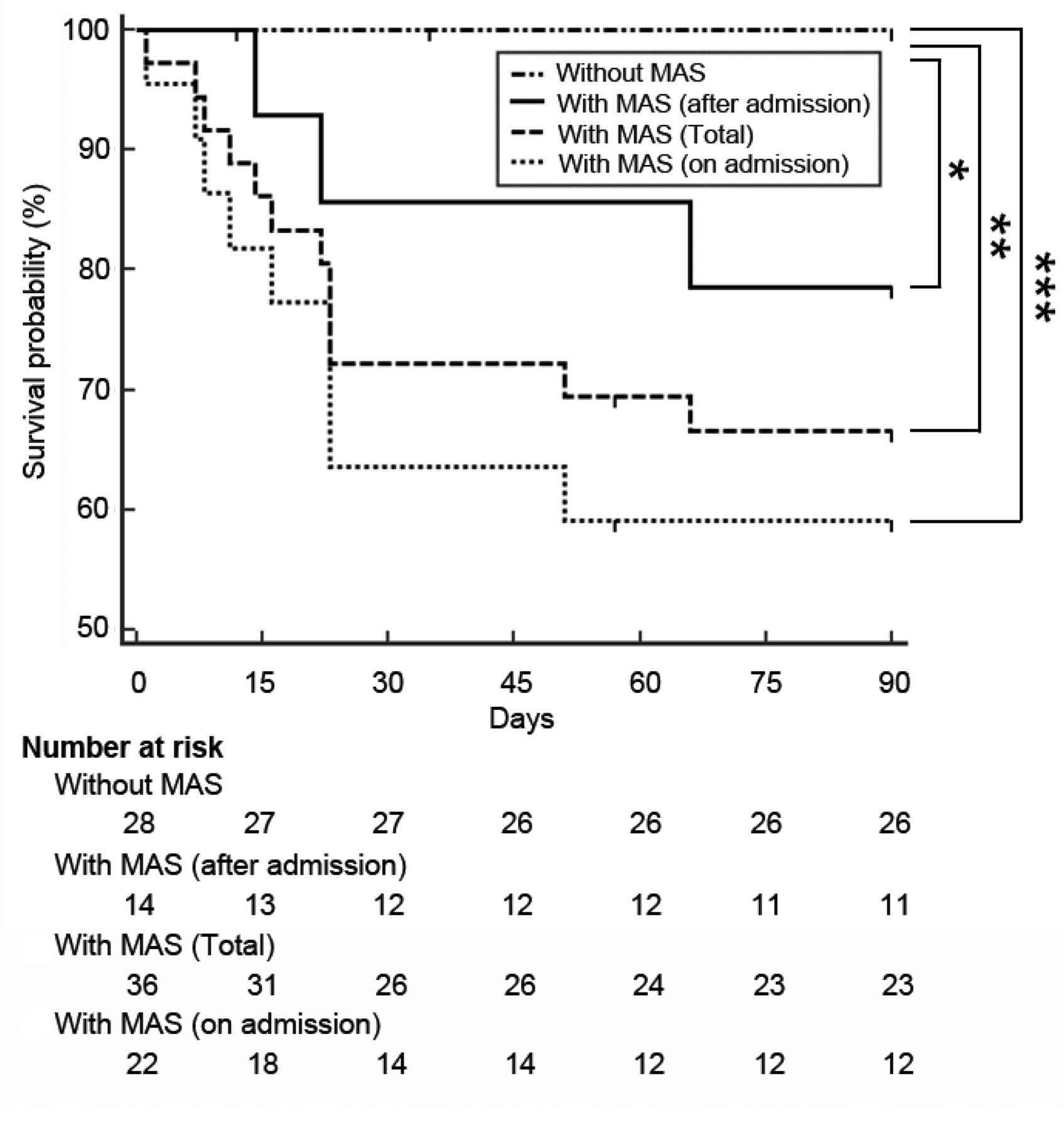
Results of the Kaplan-Meier analysis of the cumulative survival rate in patients with adult-onset Still disease with and without MAS. * p < 0.05. ** p < 0.01. *** p < 0.001. MAS: macrophage activation syndrome.
DISCUSSION
MAS refers to acute overwhelming inflammation caused by a “cytokine storm,” and a clinician’s suspicion is critical for early detection and proper management9. Several autoimmune diseases, such as sJIA, Kawasaki disease, systemic lupus erythematosus (SLE), and AOSD, have been reported to be associated with the development of MAS15. However, even with a clinical suspicion, the diagnosis of MAS is difficult because it might be hard to distinguish the clinical features of MAS from those of conditions that may have overlapping manifestations, such as flares of underlying rheumatic diseases and systemic infection5. Multiple cytokines, such as interleukin (IL)-18, IL-10, and interferon-γ, have been found to be associated with MAS; however, clinical validation for the diagnosis of MAS has not been performed5. To date, several classification criteria for MAS have been suggested, which include the hemophagocytic lymphohistiocytosis (HLH)-1991 and HLH-2004 criteria, and the 2014 criteria for reactive hemophagocytosis14,16,17. Application of the HLH-1991 and HLH-2004 in patients included in our study showed that only 1 patient fulfilled the HLH-1991 criteria and 7 patients fulfilled the HLH-2004 criteria. The low percentage of patients fulfilling both criteria occurred because the bone marrow study was not performed or failed to demonstrate hemophagocytosis, and several laboratory tests (natural killer cell activity and soluble CD25) were not performed in most patients. In contrast, application of the 2014 criteria showed that AOSD patients with MAS had a higher HScore and probability of having hemophagocytic syndrome than those without MAS. In addition, patients with the probability of having hemophagocytic syndrome ≥ 80% had a higher in-hospital mortality than those with the probability of having hemophagocytic syndrome < 80% and without MAS. Although these criteria are not diagnostic but rather the classification type, our study suggests that the 2016 classification criteria can be used as a reliable and simple measure for recognizing MAS in patients with AOSD, which is associated with an increased risk of early mortality.
In our study, we investigated the clinical significance of the 2016 EULAR/ACR/PRINTO classification criteria for MAS in patients with AOSD, and we demonstrated that 56% of patients with AOSD who were hospitalized for fever were considered to have MAS. Our study population was in the inpatient setting, and therefore could be skewed toward having MAS. In comparison, we found only 1 patient who fulfilled the 2016 classification criteria among 35 patients with AOSD in our outpatient clinic during the study period. In addition, the clinical features of AOSD patients with MAS were distinct when compared with the features of patients without MAS. First, the baseline clinical features were much worse in patients with MAS than in those without MAS. Second, the required therapeutic dosage of steroids and immunosuppressive agents used was higher in patients with MAS than in those without MAS. Third, the in-hospital mortality rate was higher in patients with MAS than in those without MAS. These findings support the clinical use of the 2016 classification criteria for MAS in patients with AOSD, and patients at high risk for a poor prognosis can be identified. In the survival analysis, most patients with MAS died within the first month, and in-hospital mortality was noted only in patients with MAS. Detection of MAS is important for early immunosuppressive treatment, while patients with AOSD without MAS can be treated with NSAID or low-dose steroids.
The 2016 EULAR/ACR/PRINTO classification criteria for MAS include fever and 5 common laboratory variables (ferritin, AST, platelets, triglycerides, and fibrinogen). These laboratory results can be obtained as part of routine laboratory tests, and the tests can be easily repeated for followup. However, unlike pediatric patients, in whom hyperferritinemia is useful in the diagnosis of MAS18, various diseases are reported to be associated with hyperferritinemia in adults19. Therefore, the absolute value of the ferritin level itself is not sufficient for diagnosing MAS. Further, although the new classification criteria set was validated in patients with sJIA, these criteria may not be comprehensively applicable to other autoinflammatory/autoimmune diseases in adults. The reason for this is that the clinical manifestation of MAS can differ according to the underlying rheumatic disease. A study has shown that MAS arising in the context of SLE and AOSD differs in several clinical and laboratory features. In detail, patients with MAS associated with AOSD had higher WBC, CRP, ferritin, and ALT levels compared with patients with MAS associated with SLE20. Therefore, the development of uniform MAS classification criteria for autoinflammatory/autoimmune diseases might be challenging.
Ferritin is an intracellular protein related to iron storage, and is usually used for the differential diagnosis of anemia21. Although the ferritin level serves as a marker of iron storage, it can also be elevated in the case of acute inflammation. A wide range of medical conditions is characterized by high levels of ferritin, such as systemic inflammatory disease, infection, and cancer22. Among those conditions of hyperferritinemia, a differential diagnosis of AOSD, MAS, catastrophic antiphospholipid syndrome (CAPS), and septic shock23 has special interest because of nonspecific systemic manifestations and high mortality. Diagnosing CAPS is often difficult in clinical practice because other forms of thrombotic microangiopathies must be excluded, and the presence of antiphospholipid antibodies and vascular thrombosis must be confirmed24. Similarly, although the diagnosis of sepsis is made with a suspected or confirmed source of infection, there is difficulty in diagnosing sepsis because only a fraction of cases of sepsis can be microbiologically documented25. Though several serum markers including soluble IL-2 receptor-α receptors and soluble CD163 have been recognized as important biomarkers in the diagnosis of MAS26,27, the diagnosis of MAS is clinically challenging, especially in patients with AOSD.
A high ferritin level has been shown to be associated with AOSD28,29. Various studies have evaluated the prognostic value of the ferritin level in AOSD; however, the results have been inconsistent6,7,30,31, probably because of the paucity of the disease and the diversity of patients in the studies. In addition, a recent study suggested that the change in laboratory values over time is more relevant than the achievement of the absolute threshold for MAS32. In line with this suggestion, our data showed that ferritin fold increase of ≥ 2 is significantly associated with in-hospital mortality in patients with AOSD. The dynamics of the ferritin level during the course of AOSD may be useful to predict patients at high risk for a poor outcome.
Because of the poor prognosis of HLH, various studies have endeavored to discover its prognostic factors. In a publication by Kaito, et al, these were associated with mortality: age over 30 years, the presence of disseminated intravascular coagulation, an increased ferritin and β2-microglobulin, anemia accompanied by thrombocytopenia, and jaundice33. In addition, in a study by Takahashi, et al, the presence of lymphoma was associated with a poor prognosis in patients with hemophagocytic syndrome34, and Arca, et al linked a poor prognosis to increasing age, decreasing platelet count, underlying lymphoma, and no etoposide in disease management35. Further, a recent study by Ruscitti, et al, which evaluated the prognostic factor in MAS, old age and increased ferritin levels were associated with mortality36. However, because of wide heterogeneity of the patient inclusion criteria and difference in study design, the prognostic factor of patients with AOSD with MAS requires further investigation.
Our study has several limitations. First, it was a retrospective study with a relatively small number of patients, and the data were collected by reviewing the hospital’s medical records. Second, data on fibrinogen and triglycerides were missing in some patients, and this might have influenced the classification of MAS. Third, the 2016 classification criteria for MAS have not been validated in patients with AOSD, especially for differentiation with systemic infection. Fourth, the effect of treatment in the outcome of patients could not be evaluated, probably because of the small sample size and retrospective study design. Prospective studies with a larger number of patients, serial testing of laboratory variables, and a proper control group are necessary.
The 2016 EULAR/ACR/PRINTO classification criteria for MAS are potentially useful to identify patients with AOSD at high risk for a poor outcome. Although the 2016 classification criteria for MAS have been validated in patients with sJIA, febrile patients with AOSD should be monitored with the 2016 classification criteria for MAS for the early diagnosis and proper treatment of MAS.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
Supported by the Basic Science Research Program (2015R1C1A1A01053140) through the National Research Foundation of Korea, funded by the Ministry of Education, Science, and Technology.
- Accepted for publication February 17, 2017.








{kind=link}
{kind=link}
{kind=link}