

Abstract
Objective. C-reactive protein (CRP), S100A8/A9, and procalcitonin have been suggested as markers of infection in patients with systemic lupus erythematosus (SLE). We investigated the clinical significance of these factors for indication of infection in SLE.
Methods. Blood samples were prospectively collected from 34 patients with SLE who had bacterial infections and 39 patients with SLE who had disease flares and no evidence of infection. A second set of serum samples was collected after the infections or flares were resolved.
Results. CRP levels of SLE patients with infections were higher than those with flares [5.9 mg/dl (IQR 2.42, 10.53) vs 0.06 mg/dl (IQR 0.03, 0.15), p < 0.001] and decreased after the infection was resolved. S100A8/A9 and procalcitonin levels of SLE patients with infection were also higher [4.69 μg/ml (IQR 2.25, 12.07) vs 1.07 (IQR 0.49, 3.05) (p < 0.001) and 0 ng/ml (IQR 0–0.38) vs 0 (0–0) (p < 0.001), respectively]; these levels were also reduced once the infection disappeared. In the receiver-operating characteristics analysis of CRP, S100A8/A9, and procalcitonin, the area under the curve was 0.966 (95% CI 0.925–1.007), 0.732 (95% CI 0.61–0.854), and 0.667 (95% CI 0.534–0.799), respectively. CRP indicated the presence of an infection with a sensitivity of 100% and a specificity of 90%, with a cutoff value of 1.35 mg/dl.
Conclusion. Our data suggest that CRP is the most sensitive and specific marker for diagnosing bacterial infections in SLE.
Infection is common in systemic lupus erythematosus (SLE), and is also a main cause of mortality. Increased susceptibility to infection can be explained by several intrinsic and acquired defects of the immune system related to the disease itself or the immunosuppressive therapies. Therefore, it is important to diagnose infection early in these individuals. However, a major obstacle for recognizing the presence of infection is that clinical manifestations of infection are similar to those of disease flare1,2. Therefore, a simple marker that could be used to diagnose bacterial infection at an early stage and rule out disease flare would be very useful.
Common laboratory tests such as white blood cell counts with increased neutrophils or increased acute-phase reactants are helpful, but are not always diagnostic because some markers of infection can be elevated when patients have disease flares. It is known that C-reactive protein (CRP) levels are not elevated during SLE flares, making the factor unsuitable for monitoring disease activity3,4. Elevated levels of CRP are found in the sera of patients with SLE who present concurrent infections5,6. However, moderately increased CRP levels are also found in cases of SLE-associated serositis and arthritis3,6. The range of CRP levels in SLE patients with infection sometimes overlaps considerably with those of SLE patients with flares7. Therefore, investigators have tried to find a new biomarker that can distinguish infection from flare in patients with SLE.
S100A8 and S100A9 are 2 calcium-binding proteins belonging to the S100 family8. Under inflammatory conditions, S100A8 and S100A9 are expressed by infiltrating monocytes and neutrophils, but not in quiescent resident macrophages and lymphocytes9,10. S100A8/A9 can be detected in high levels in serum and body fluids in patients with different types of infectious, inflammatory, and malignant disorders11,12.
Procalcitonin is a protein with a molecular weight of 13 kDa that is produced by thyroid gland C cells as a precursor of calcitonin13. Serum procalcitonin levels are elevated in patients with bacterial infections, but are below the detection limit in healthy individuals and patients with viral infections. This indicates that procalcitonin is useful for diagnosing systemic bacterial infections14.
Previous studies have reported that S100A8/A9 and procalcitonin serum levels are elevated under infection and may be used as markers of infection in patients with SLE15,16,17,18. However, the results of these investigations were variable and the sample sizes were small. Therefore, we investigated the clinical use of S100A8/A9 and procalcitonin as biomarkers of infection in Korean patients with SLE and compared them to CRP.
MATERIALS AND METHODS
Subjects
Patients with SLE who were admitted due to disease flares or infections were prospectively recruited from December 2009 through January 2011. All patients satisfied the American College of Rheumatology (ACR) 1982 revised criteria for the classification of SLE. Thirty-four patients with SLE had a concurrent bacterial infection (SLE with infection). The presence of an infection was confirmed by the presence of a positive pathogen test from various specimens (blood, sputum, pus, stool, and urine) or clear evidence of infection, such as an abscess on computed tomography. Also, sepsis was confirmed clinically (at least 2 systemic inflammatory response syndrome criteria) and/or by positive blood culture. Table 1 shows the types of bacterial infections of patients with SLE in our study. Thirty-nine patients had flares without any evidence of infection (SLE with flare). The flare was defined as any clinical event directly attributable to disease activity leading to a Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score ≥ 6 that would require an escalation of treatment without evidence of infection.
Types of bacterial infections found in 34 patients with systemic lupus erythematosus.
Serum samples were collected immediately after admission for infection or flare. The duration from the development of symptom to blood sampling was 4 ± 3.58 days in SLE with infection. Followup serum samples were collected from 30 SLE patients with infection and from all SLE patients with flares after the infections or flares were resolved (SLEDAI ≤ 4). All blood samples were stored at −20°C immediately after collection.
Information on the medical history, clinical symptoms, and physical examinations was entered into a database when serum sampling was done. Each patient also underwent blood cell count, routine chemistry, urinalysis, complement, and anti-dsDNA antibody analyses. SLE activity was evaluated according to the SLEDAI scores. Our study was approved by the Institutional Review Board of our hospital, and informed consent was received from all subjects.
S100A8/A9 and procalcitonin assay
Serum S100A8/A9 levels were measured using commercial ELISA kits (Buhlmann Laboratories, Schonenbuch, Switzerland) according to the manufacturer’s instructions. Procalcitonin levels were determined using an enzyme-linked fluorescent assay (Vidas Brahms Procalcitonin, bioMérieux, Lyon, France) according to the manufacturer’s instructions. The detection limits for S100A8/A9 and procalcitonin were 0.3 μg/ml and 0.05 ng/ml, respectively. Procalcitonin levels below 0.05 ng/ml were considered to be negligible.
CRP determination
Serum CRP levels were measured by immunoturbidimetry using a TBA-200FR chemistry autoanalyzer (Toshiba, Tokyo, Japan). The limit of CRP detection was 0.02 mg/dl. CRP levels < 0.02 mg/dl were considered negligible. The reference normal range was < 0.8 mg/dl according to this assay.
Statistical analysis
The statistical analysis was performed using SPSS, version 12.0 (SPSS, Chicago, IL, USA). A p value < 0.05 was regarded as statistically significant. The sample size of enrolled patients was calculated from the previous study3. To achieve a power of 80%, type 1 error of 0.025, and a significance level of 0.05, the required sample size was calculated as 36 patients per group. Due to asymmetrical distribution of the serum CRP, S100A8/A9, and procalcitonin levels, summary statistics are given as median and interquartile range (IQR). Other data were shown as mean ± SD. Differences in CRP, S100A8/A9, and procalcitonin levels were determined by a Mann-Whitney U test. The ability of CRP, S100A8/A9, and procalcitonin to accurately diagnose infection in patients with SLE was evaluated by a receiver-operating characteristic (ROC) analysis. We constructed an ROC curve for CRP, S100A8/A9, and procalcitonin to identify the optimal thresholds by maximizing the sum of sensitivity and specificity. We calculated the sensitivity and specificity of CRP, S100A8/A9, and procalcitonin cutoff values determined by the ROC curves. Statistical significance of differences between the areas under 2 or more ROC curves for different test groups was determined using MedCalc software (version 10.2; MedCalc Software, MariaKerke, Belgium) based on the method described by Hanley and McNeil19.
RESULTS
Clinical characteristics of the patients
The mean age of the SLE patients with infection was 32.76 ± 12.41 years and that of the SLE patients with flare, 32.77 ± 10.43 years (Table 2). There were no significant differences in age, sex, or disease duration between SLE with infection and SLE with flare. The main clinical symptoms in SLE with infection included malar rash (26.5%), arthritis (26.5%), renal disease (32.4%), and neurologic disorders (8.8%). The frequencies of clinical features were not statistically different between SLE with infection and SLE with flare except arthritis, which was more frequently observed in SLE with flare. The level of anti-dsDNA antibody was lower in SLE with infection than SLE with flare (p = 0.045). However, leukocyte counts, C3 levels, and erythrocyte sedimentation rate (ESR) were higher in SLE with infection (p = 0.015, 0.005, and 0.014, respectively).
Clinical characteristics of 34 systemic lupus erythematosus (SLE) patients with infection and 39 SLE patients with flare.
CRP, S100A8/A9, and procalcitonin levels
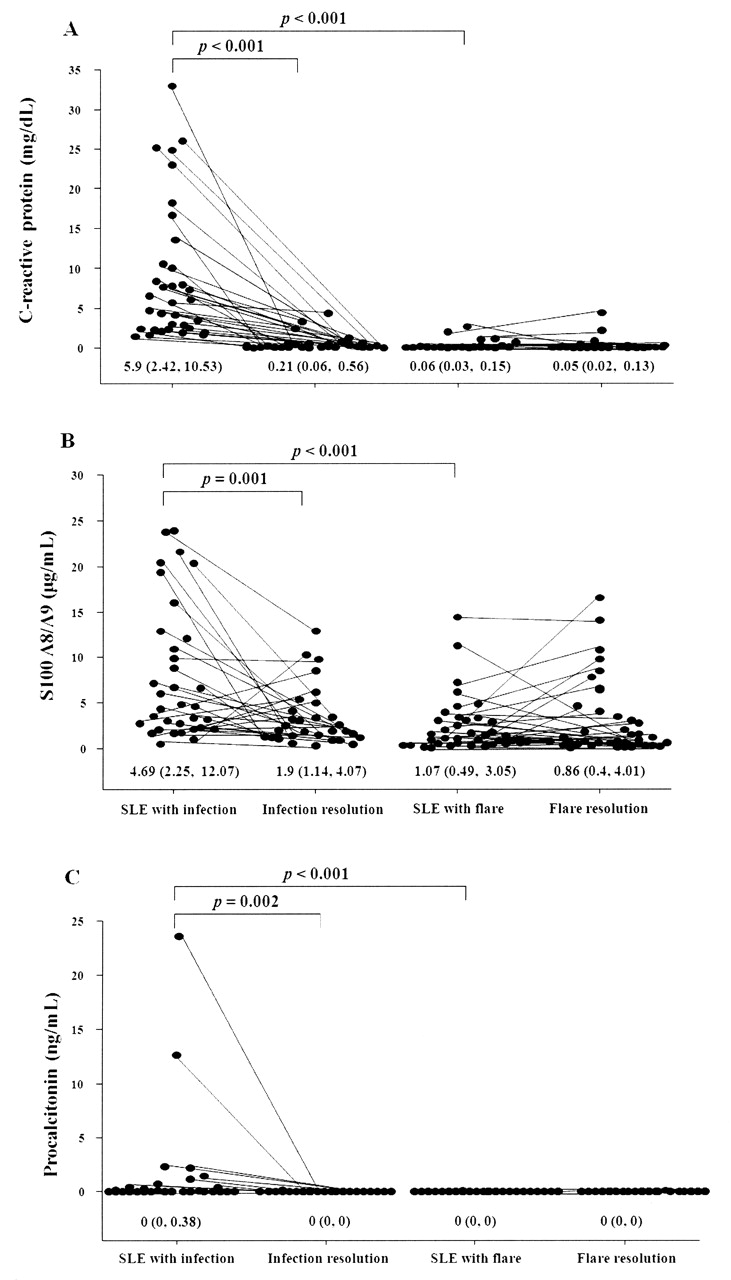
Figure 1 shows CRP, S100A8/A9, and procalcitonin levels in SLE with infection or flare. The CRP levels of SLE with infection [5.9 mg/dl (IQR 2.42, 10.53)] were higher than those of SLE with flare [0.06 mg/dl (IQR 0.03, 0.15); p < 0.001]. Additionally, the S100A8/A9 and procalcitonin levels of SLE with infection were higher than SLE with flare [4.69 μg/ml (IQR 2.25, 12.07) vs 1.07 μg/ml (IQR 0.49, 3.05) (p < 0.001), and 0 ng/ml (IQR 0, 0.38) vs 0 ng/ml (IQR 0, 0) (p < 0.001), respectively]. Further, the levels of all 3 markers were decreased after the infections were resolved. In SLE with infection, CRP levels were positively correlated with those of S100A8/A9 and procalcitonin (r = 0.443, p < 0.001, and r = 0.558, p < 0.001, respectively). In SLE patients with sepsis, procalcitonin levels [0.75 ng/ml (IQR 0, 2.19)] were higher than in SLE patients with other types of infections [0 ng/ml (IQR 0, 0.08); p = 0.028], but CRP and S100A8/A9 levels were not.

The levels of C-reactive protein (A), S100 A8/A9 (B), and procalcitonin (C) in 34 systemic lupus erythematosus (SLE) patients with infections and 39 SLE patients with flares. Data are expressed as the median and interquartile range. A Mann-Whitney test was used to perform the statistical analysis.
Sensitivity and specificity of CRP, S100A8/A9, and procalcitonin for diagnosing infections in patients with SLE
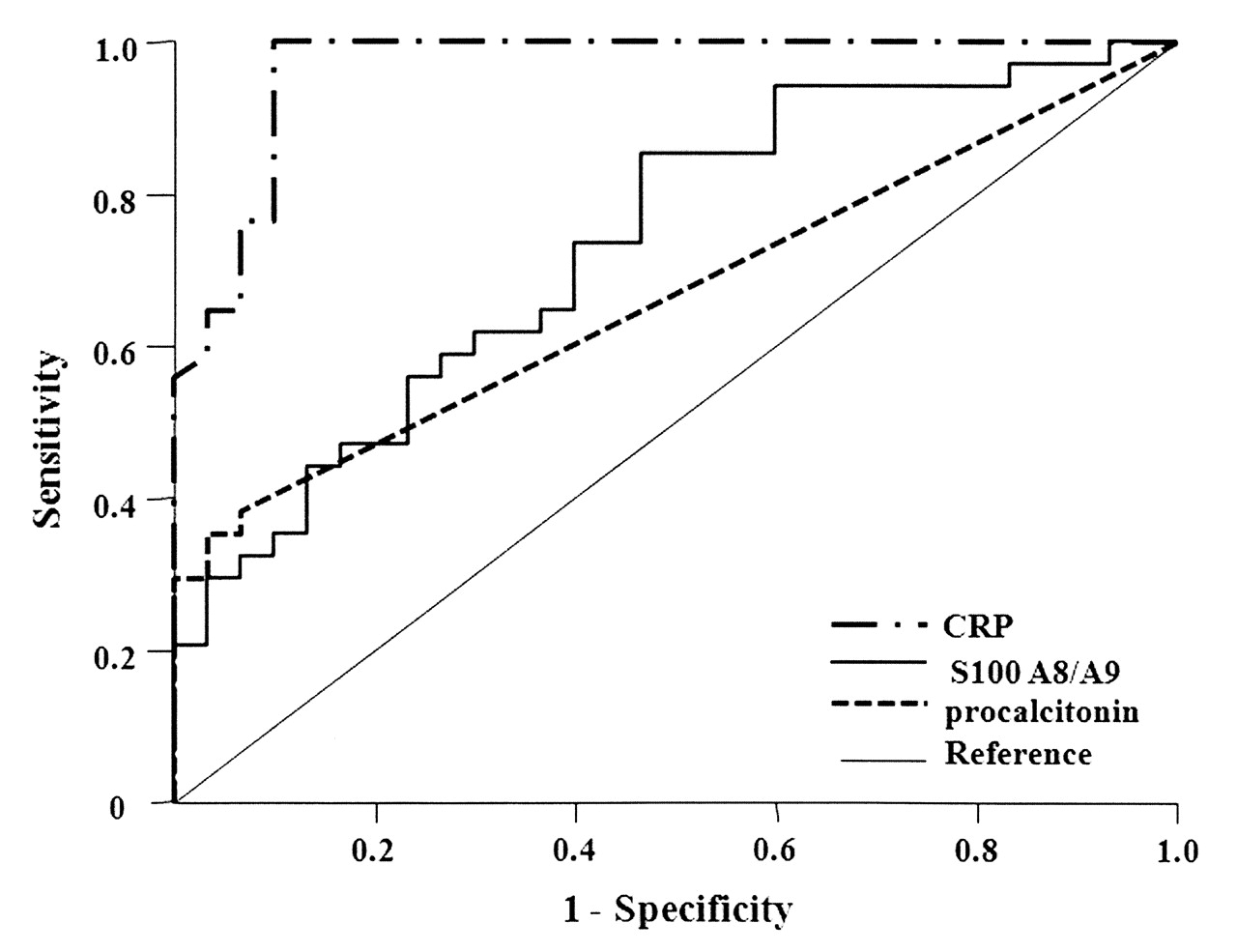
In the ROC analysis of CRP, S100A8/A9, and procalcitonin, the area under the curve (AUC) was 0.966 (95% CI 0.925–1.007), 0.732 (95% CI 0.61–0.854), and 0.667 (95% CI 0.534–0.799), respectively (Figure 2). With a cutoff value of 1.35 mg/dl, the sensitivity and specificity of CRP for detecting infection in patients with SLE was 100% and 90%, respectively. However, the sensitivity and specificity of S100A8/A9 were 85.2% and 53.3%, respectively (cutoff value, 1.975 μg/ml), and those of procalcitonin were 38.2% and 93.3% (cutoff value, 0.025 ng/ml). The combined use of both CRP and S100A8/A9 showed a sensitivity 85.3% and specificity 93.3% for diagnosing infection in patients with SLE (Table 3). Pairwise comparison of the AUC showed that the area of CRP was significantly greater than those of S100A8/A9 and procalcitonin (p < 0.001 and p < 0.001, respectively).
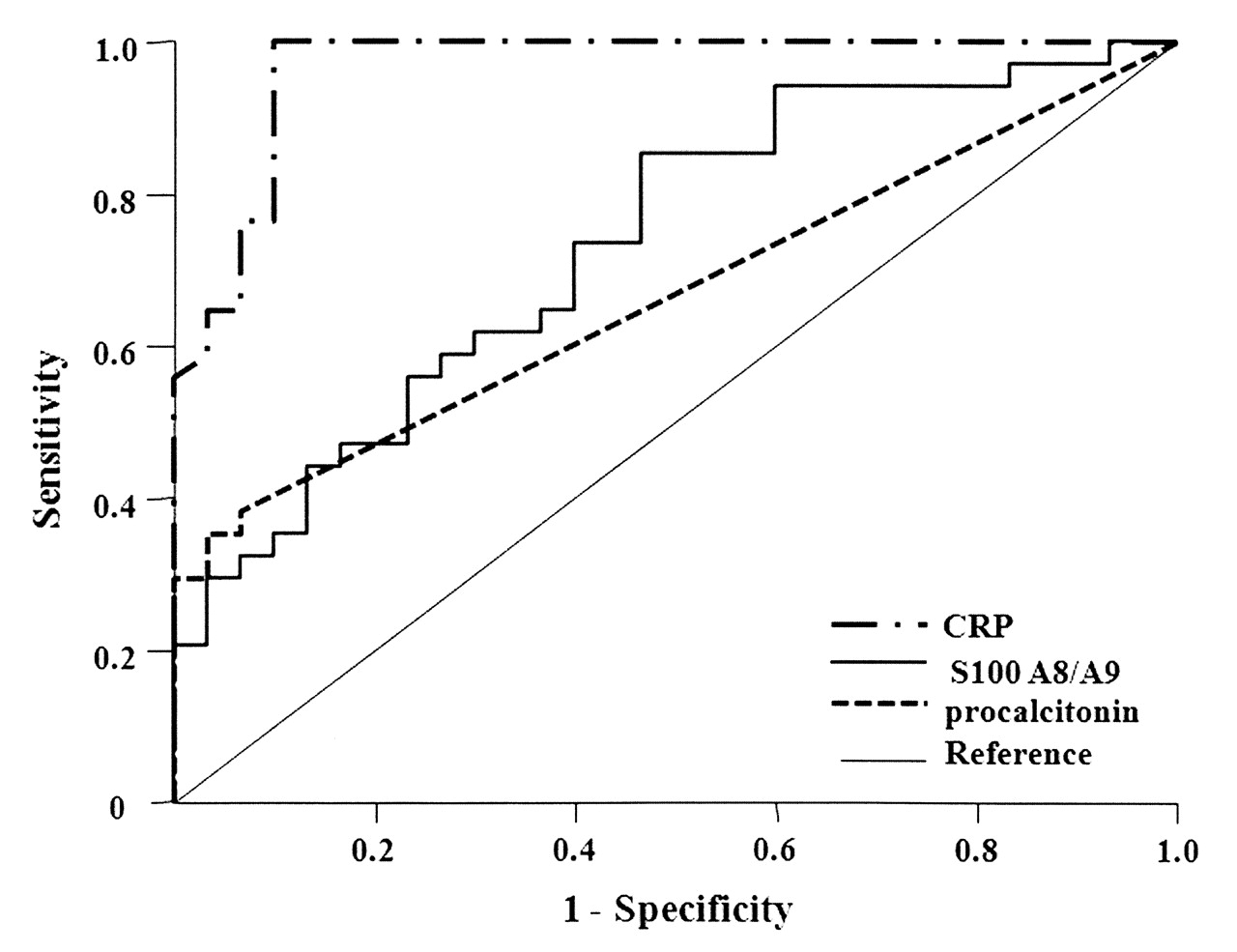
The receiver-operating characteristic (ROC) curves for C-reactive protein (CRP), S100 A8/A9, and procalcitonin levels in SLE patients with infections. The ROC curve values were 0.966 for CRP (95% CI 0.925–1.007; p < 0.001), 0.732 for S100 A8/A9 (95% CI 0.61–0.854; p = 0.001), and 0.667 for procalcitonin (95% CI 0.534–0.799; p = 0.022).
The sensitivity and specificity of 3 markers in systemic lupus erythematosus (SLE) patients with bacterial infections. Positive cutoff values were determined by receiver-operating characteristics curves. Cutoff values of procalcitonin, S100 A8/A9, and CRP are 0.025 ng/ml, 1.975 μg/ml, and 1.35 mg/dl, respectively.
Serum S100A8/A9 levels and disease activity in SLE with flare
There was a report that showed higher S100A8/A9 levels in SLE with flare than SLE with remission (SLEDAI ≤ 4)15. In our study, although ESR, anti-dsDNA, C3, and SLEDAI were decreased after resolution of flare, the S100A8/A9 levels of SLE with flare [1.07 μg/ml (IQR 0.49, 3.05)] were not decreased during remission [0.86 μg/ml (IQR 0.4, 4.01); Table 4]. Further, the comparisons of serum S100A8/A9 levels according to clinical manifestations of SLE revealed no significant differences. No correlation was found between S100A8/A9 and other disease activity markers such as anti-dsDNA antibody and SLEDAI scores (data not shown).
Clinical characteristics of 39 systemic lupus erythematosus (SLE) patients with flare and after resolution of flare. Data are median ± SD unless otherwise indicated.
DISCUSSION
The distinction between infection and disease flare in patients with SLE is often difficult to make. In our study there was no significant SLEDAI difference between SLE with flare and SLE with infection. It is well known that patients with flare are immunocompromised by the disease itself or by concomitant immunosuppressive therapy, and therefore are at high risk of developing systemic infections. However, the distinction between infection and disease flare is clearly of great importance for the management of SLE. Therefore, a reliable marker that can be measured easily and without delay would be valuable for promptly distinguishing infection from disease flare.
To examine the clinical usefulness of CRP, S100A8/A9, and procalcitonin, a relatively large number of patients with SLE were prospectively examined, and serial sampling was performed after the infections and flares had been resolved. Serum CRP, S100A8/A9, and procalcitonin levels of SLE patients with bacterial infections were significantly higher than those of SLE patients with flares. Further, those levels of SLE patients with bacterial infections decreased when the infections were resolved. When sensitivity and specificity of CRP, S100A8/A9, and procalcitonin were evaluated for diagnosing infection using ROC curves, CRP was found to have the highest sensitivity and specificity, with a cutoff value of 1.35 mg/dl.
S100 proteins, which mediate inflammatory responses and are involved in the recruitment of inflammatory cells to sites of injury, have been suspected of forming damage-associated molecular patterns20,21. S100 proteins form a family with more than 20 members, including 3 that are linked to innate immune functions by their expression by myeloid cells: S100A8, S100A9, and S100A12. S100A8 and S100A9 form heterodimers that are the biologically relevant forms22,23. S100A8/A9 is released during inflammation, and there is a strong correlation between systemic S100A8/A9 levels and the presence of inflammation24. Recently, S100A8/A9 has been shown to be the endogenous ligand of Toll-like receptor-4, to play an important role in innate immunity, and to be associated with human sepsis and endotoxemia12,23. Only 1 study has examined S100A8/A9 for detecting infection in SLE15. SLE patients with infections had higher levels of S100A8/A9 than SLE patients with flares. Additionally, S100A8/A9 is a better marker at a cutoff concentration of 8100 ng/ml than CRP at a cutoff concentration of 1 mg/dl for detecting infections. However, a very small number of SLE patients with infections (n = 6) were examined, and the cutoff values for S100A8/A9 and CRP used to compare sensitivity were based on the lowest values found in SLE patients with infections15.
In our study, we determined the S100A8/A9 levels of 34 SLE patients with bacterial infections through serial sampling. Serum S100A8/A9 levels of SLE patients with infections were significantly higher than those of SLE patients with flares (p < 0.001). After resolving the infections, most patients had significantly decreased S100A8/A9 levels (p = 0.001). In the ROC analysis, however, the AUC of S100A8/A9 (0.732) was lower than that of CRP (0.966; p < 0.001). Further, the sensitivity and specificity of S100A8/A9 (cutoff value, 1.975 μg/ml) were 85.2% and 53.3%, respectively, which were less sensitive and specific than CRP. Using both CRP and S100A8/A9 to diagnose infection resulted in higher specificity but lower sensitivity than when CRP was used alone. These results suggest that CRP is a better marker than S100A8/A9 for detecting bacterial infections in SLE.
Procalcitonin is the precursor of calcitonin, a calcium-regulating peptide with a role in calcium homeostasis. It has been shown that there is increased procalcitonin release in the presence of severe inflammation after thyroidectomy, suggesting that the site of procalcitonin synthesis in response to inflammation must be outside the thyroid gland14,25. Serum procalcitonin level has been used as a marker of bacterial, parasitic, and fungal infections because it is not elevated in healthy individuals, and is induced only slightly in cases of viral or localized bacterial infections26,27. However, the usefulness of procalcitonin to identify systemic bacterial infections in patients with SLE remains controversial. Although several studies have examined procalcitonin in SLE patients with infections, those studies have been limited by small numbers of patients with infection, analysis of multiple serum samples, variability of patient characteristics, or with the inclusion of patients with other systemic autoimmune disease16,17,25,28,29,30. One study demonstrated that SLE patients with bacterial or fungal infections (n = 9) had significantly higher procalcitonin levels than those with viral infections (n = 3) or lupus flares (n = 7) and a normal control group (n = 11)16. Nevertheless, that study examined only a small number of subjects, and it is unclear whether any patients had systemic infections. Another study recently reported that severe infections were not associated with elevated procalcitonin levels in patients with SLE28. However, that study enrolled a small number of SLE patients with systemic infections (n = 5).
In our study, although only some SLE patients with bacterial infections had elevated procalcitonin levels, these were significantly decreased after resolution of infection (p = 0.002). Further, the serum procalcitonin levels of SLE patients with infections were significantly higher than those of SLE patients with flares (p < 0.001). The procalcitonin levels of SLE patients with sepsis were higher than those of SLE patients without sepsis (p = 0.028); however, there were no differences in CRP or S100A8/A9 levels. In the ROC analysis, the AUC of procalcitonin (0.667) was lower than that of CRP (0.966; p < 0.001), and procalcitonin had a low sensitivity (38.2%) for detecting bacterial infections. These results are probably due to the inclusion of patients with localized infections. Our study suggests that CRP is a more sensitive marker than procalcitonin for identifying bacterial infections in SLE and that procalcitonin can be used for determining the presence of sepsis.
S100A8/A9 expression is highly upregulated in cases of several inflammatory diseases such as rheumatoid arthritis, glomerulonephritis, and vasculitis31. Recently, patients with cutaneous lupus erythematosus were found to have substantial numbers of epidermal cells expressing S100A8 and A930. Both proteins are also substantially upregulated during inflammation in tissues, such as in the kidneys, of patients with SLE. One study found significantly increased levels of S100A8/A9 in SLE that were correlated with SLEDAI scores (r = 0.28, p < 0.01). S100A8/A9 levels were also found to be significantly higher in SLE patients with arthritis32. Another study showed that serum concentrations of S100A8/A9 in patients with SLE are significantly higher and found a correlation between S100A8/A9 levels and SLEDAI scores (r = 0.219, p = 0.015)15.
In our study, however, serum S100A8/A9 levels of SLE patients with flares were not different from those of patients in which the flares were resolved. Comparing S100A8/A9 levels according to clinical manifestations of SLE including arthritis and serositis revealed no significant differences. Further, no correlation was found between S100A8/A9 levels and disease activity markers such as anti-dsDNA antibody and SLEDAI scores. These results were different from those of previous studies15,32. Although the reason is not clear, this may be due to difference in disease activity. The patients in our study had an average SLEDAI score of 10.74 ± 5.11, while patients in the previous study had an average SLEDAI score of 4.6 ± 0.715. The study designs (prospective vs cross-sectional) were also different. In previous studies, the correlation between SLEDAI scores and S100A8/A9 levels was found to be weak (each r = 0.28 and 0.219), but it is unclear whether patients with infection were included in the analysis.
Serum CRP, S100A8/A9, and procalcitonin levels of SLE patients with bacterial infections were significantly higher than those of SLE patients with flares, and decreased after the infections were resolved. The sensitivity and specificity of CRP for diagnosing infection was highest with a cutoff value of 1.35 mg/dl. These data suggest that CRP is still the most sensitive and specific marker for identifying bacterial infections in SLE. For validation of this value as the reference standard, further prospective studies with a larger sample size are needed.
Footnotes
-
Supported by the Brain Korea 21 project for Ajou University School of Medicine and a grant from the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare and Family Affairs, Republic of Korea (A080588).
- Accepted for publication November 8, 2011.








{kind=link}
{kind=link}