
Revenge of the Tick: Tick-Borne Diseases and the Eye in the Age of Climate Change and Globalisation
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methodology
3. Results
3.1. Adnexal Lesions
3.1.1. Eyelid Nodules (Present in the Same Location after the Tick Bites)
3.1.2. Surface/Conjunctival Lesions
3.2. Ophthalmic Lyme Disease
3.2.1. Ocular Surface: Follicular Conjunctivitis, Episcleritis, Scleritis
3.2.2. Keratitis
3.2.3. Intraocular Inflammation
3.2.4. Chronic Lid Inflammation
3.2.5. Orbital Inflammation
3.2.6. Neuro-Ophthalmic Manifestations and Neuroretinitis
3.2.7. Temporal Arteritis
3.3. Tularaemia and Oculoglandular Syndrome
3.3.1. Atypical Ophthalmic Manifestations of Oculoglandular Tularaemia
3.3.2. Ophthalmic Manifestations in Other Subtypes of Tularaemia, Other Than Oculoglandular Tularaemia
3.4. Babesiosis
3.5. Tick-Borne Relapsing Fever
Ocular Inflammation
3.6. Ehrlichiosis
3.7. Rocky Mountain Spotted Fever
3.7.1. Retinovascular Changes
3.7.2. Neuro-Ophthalmic Manifestations
3.7.3. Uveitis
3.8. Mediterranean Spotted Fever
3.8.1. Parinaud Oculoglandular Syndrome in Mediterranean Spotted Fever
3.8.2. Corneal Manifestations
3.8.3. Posterior Segment Manifestations
3.9. Toxoplasmosis
3.9.1. Posterior Uveitis
3.9.2. Primary Intraocular Lymphoma
3.10. Powassan Encephalitis
3.11. Tick-Borne Encephalitis
3.12. Colorado Tick Fever
4. Discussion
4.1. Proposal for Removal of Ticks from the Eye Surface and Subsequent Management
4.2. Prototype: Lyme Disease, The Immune System, and Pathways for Tick-Borne Disease Entry into the Eye
4.2.1. Entry of Borrelia into the Eye
4.2.2. Implications for Other Tick-Borne Bacteria
4.2.3. Corollary: Tick-Borne Viruses and Entry into the Eye
4.3. Climate Change and Air Travel
4.4. Travel Medicine: When to Consider Tick-Borne Diseases
- recent travel to endemic areas [11]; and
- systemic features associated with tick-borne illness, e.g., fever, characteristic rash.
Special Consideration: Atypical Presentations in the Immunocompromised and the Jarisch-Herxheimer Reaction (JHR)
4.5. Diagnostic Dilemmas: Intraocular Malignancies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

| Tick-Borne Disease | Tick Species Involved | Ocular Manifestations | Duration to Onset | Treatment | Outcomes |
|---|---|---|---|---|---|
| Adnexal lesions | Ixodes spp. I. nipponensis I. scapularis Dermacentor variabilis Rhipicephalus sanguineus Amblyomma americanum | Eyelid ulceration, eyelid inflammation (acute or chronic), eyelid oedema, painful eyelid nodule ± mucopurulent discharge, conjunctival injection, conjunctival nodule, conjunctival hyperaemia, corneal precipitates, corneal thinning and vascularisation, palpebral ptosis, vasculitis. | Not stated. No history of tick bite [8]. Not stated [9,10]. Not stated. History of travel to a region endemic for tick bites [11]. 6 months after experiencing tick attachment in a wooded area (Cape Cod, Massachusetts, USA) [12]. Immediately after foreign body sensation in the right eye while camping (Adirondacks, New York, USA) [21]. 5 days after a hunting trip in a rural area of Alabama, USA [22]. 10 months after exposure to a cloud of unidentified insects in southern Spain [84]. | Topical tetracaine was applied, followed by irrigation with topical chlorhexidine. Tick was removed with toothed forceps. Topical tobramycin ointment was then applied. [8]. Tick was separated from the eyelid with 26G needle tip, then removed with toothed forceps. Prophylactic doxycycline 100 mg was given for 1 week against tick-borne diseases [9]. Tick was removed with toothless forceps [10]. Ticked was removed with blunt forceps, followed by topical chloramphenicol and dexamethasone sodium phosphate twice/day for 2 weeks. [11]. Complete excision of the suspicious nodule under local anaesthesia [12]. Topical proparacaine was applied, followed by removal of the tick with a 30G needle. Topical polymyxin-trimethoprim eye drops thrice/day and loteprednol eye drops twice/day were started for 3 days. PO doxycycline 100 mg given as prophylaxis against Lyme disease [21]. Topical proparacaine 0.5% was applied, followed by phenylephrine 2.5% topically near the organism. Jeweller’s forceps were for elevation of conjunctiva. En bloc excision of the organism and surrounding conjunctiva was performed with Vannas scissors. Topical Bacitracin 4 times/day for 3 days was given [22]. Various antibiotic therapies were initially used, but had suboptimal results. Given irregular response to antibiotics and presence of vasculitis, azathioprine was started for immunosuppression, followed by topical cyclosporine to reduce surface inflammation [84]. | Full recovery [8,9,11,12,21,22,84]. Not stated [10]. |
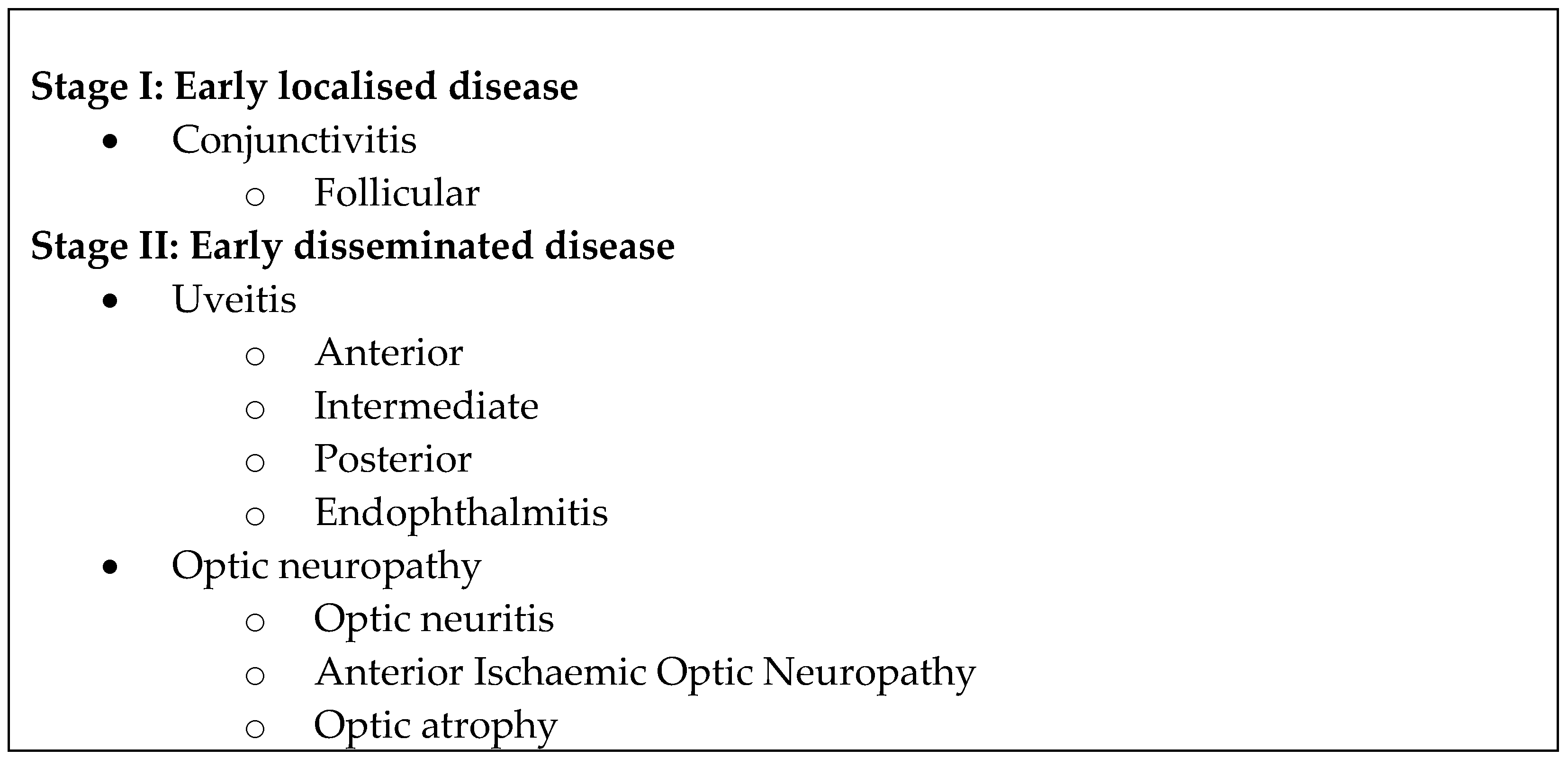
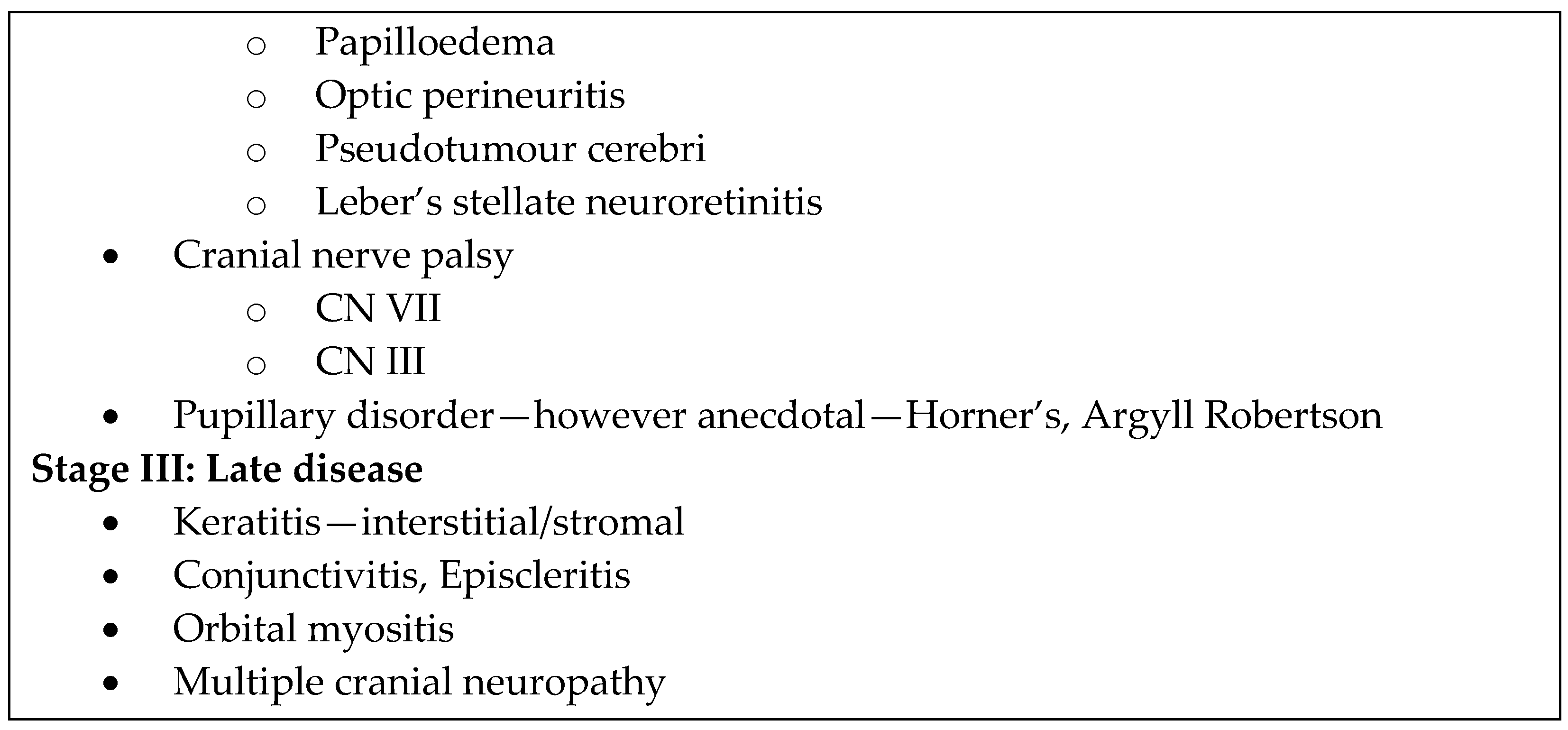
| Ophthalmic Lyme Disease | Ixodes spp. I. scapularis I. pacificus | Lids Erythema migrans on lids and periocular adnexae Palpebral oedema Blepharospasm. Conjunctiva Conjunctivitis (follicular) Symblepharon Subconjunctival haemorrhages. Episcleritis Scleritis Cornea Keratitis (exposure, interstitial, peripheral ulcerative, stromal) (associated with peripheral stromal oedema and mild corneal neovascularisation which is infrequent) Cogan’s syndrome. Pupils (Reversible) Horner’s syndrome Argyll Robertson Afferent pupillary defect Tonic pupils. Cranial Nerve Palsies CN3, 4, 6, 7 Paralytic strabismus. Uvea Iritis Cyclitis Iridocyclitis Choroiditis: Chorioretinitis, multifocal choroiditis, Birdshot chorioretinopathy, Acute posterior multifocal placoid pigment epitheliopathy Uveitis: Anterior, Intermediate (most common), Posterior, Panuveitis (granulomatous, associated with anterior synechiae) Posterior synechiae Inflammatory choroidal neovascular membrane. Vitreous Vitritis (anterior “spiderweb” vitritis without retinal involvement) Atypical pars planitis syndrome Pars planitis Vitreous clouding. Retina Retinitis Retinal vasculitis Atypical Eales disease syndromes Exudative retinal detachments Branch retinal artery occlusion with cotton wool spots Horseshoe-shaped retinal tear with inflammatory nodules on the flap Macular oedema Retinal venular occlusions: branch retinal vein occlusion Chorioretinal inflammatory foci Secondary retinitis pigmentosa Pigment epitheliitis. Optic Nerve Optic neuritis (retrobulbar neuritis) Optic perineuritis Neuroretinitis (Leber’s stellate) complications: full thickness macular hole and peripapillary retinal pigment epithelium detachments) Chiasmal optic neuritis Papilloedema (possibly associated with meningitis) Ischaemic optic neuropathy (anterior) Big blind spot syndrome Secondary optic atrophy. Orbit Orbit periostitis Periorbital oedema Orbital myositis (medial rectus, inferior rectus, lateral rectus), associated with lacrimal gland enlargement and optic nerve sheath contrast enhancement on MRI. Others Endophthalmitis Panophthalmitis Cortical blindness Intraocular inflammatory syndromes Pseudotumour cerebri Photophobia Acute visual loss Opsoclonus (Opsoclonus-myoclonus syndrome) Nystagmus (associated with partial CN VI palsy). Temporal Arteritis | 3 cases were described by Smith et. al. Case 1: The patient presented with blurred vision after 3 years of multiple facial palsies that were responsive to steroids. The patient had a tick bite while hunting in Everglades several years before and camped at Cape Cod 11 and 14 years prior to presentation. Case 2 and 3: not stated [81]. 4 weeks after the patient had Erythema chronicum migrans [83]. Sauer et. al. described 2 cases. Case 1: Current complication of horizontal diplopia developed after 3 years of recurrent episodes of right orbital swelling and pain. Case 2: Recent history of tick bite followed by Erythema migrans (no specific duration stated) [88]. 6 months after tick bite [89]. The patient was hunting and skinning deer in Southeast Pennsylvania the month before presentation and noticed a large tick on his neck 4 days prior to presentation [103]. Presented with a scotoma above fixation in the left eye after 2 months of floaters in both eyes and daily throbbing headaches [112]. Not stated [116]. The patient presented after a 1 month history of a dull temporal headache which was treated by a chiropractor [124]. | Successful treatment with topical Prednisolone acetate 1% every 4 h [46]. Topical corticosteroid therapy with prednisolone sodium phosphate (1%) four times/day, later started on PO doxycycline 100 mg twice/day for 21 days [47]. Successful treatment with Prednisolone acetate 1% eye drops four times daily [48]. Prednisone 60 mg was given with ocular complications developing after: rise in intraocular pressure, proptosis, conjunctival purulent discharge and rapid onset of a dense cataract [54]. PO doxycycline 100 mg twice/day for 7 days [67]. Systemic IV ceftriaxone for neuroretinitis [73]. Case 1, during a recurrence of retinal vasculitis: PO tetracycline 250 mg four times/day, 20 mg subtenon Kenalog (aqueous triamcinolone). Case 2: IV aqueous penicillin 20 million units daily. Case 3: PO Isoniazid for positive PPD skin test, subtenon Depomedrol injections, panretinal photocoagulation for increasing vitreous haemorrhage and neovascularisation, posterior vitrectomy with membrane peeling due to increasing traction and blood-obscuring laser treatment, IV Rocephin 2 g/day for 2 weeks at outpatient [81]. Treatment with corticosteroids failed to provide improvement, IV methicillin 12 g/day and IV gentamicin 80 mg every 8 h were then started after positive Lyme disease serology but vision worsened, followed by lensectomy and vitrectomy with repeated drainage of purulent vitreous debris and the administration of intravitreal gentamicin 0.2 mg and chloramphenicol 0.2 mg [83]. Case 1: PO doxycycline 200 mg/day. Case 2: Doxycycline 200 mg/day for 4 weeks [88]. IV ceftriaxone 1500 mg/day for 3 weeks [89]. After diagnosis of Lyme disease, was originally treated with PO tetracycline 500 mg 4 times/day, but then noticed unequal pupils and a drooping left lid. Following that, he was treated with 1% hydroxyamphetamine (Paredrine) and IV Ceftriaxone 1 g every 12 h for 10 days [103]. IV penicillin G 12 million units daily for 10 days [112]. Ceftriaxone 2 g/day [116]. Originally treated with prednisone 80 mg/day but the patient deteriorated. The patient was then given IV Decadron 8 mg every 6 h for 24 h which stabilised the vision in his nonamblyopic left eye. This was followed by his discharge and tapering of the corticosteroids. After a Borrelia-compatible spirochaete (but not B. burgdorferi) was identified in peripheral blood cultures, IV ceftriaxone sodium 2 g daily over 7 days was administered and a repeat peripheral blood culture yielded no evidence of spirochaetes. A 2nd course of steroids failed to improve the patient’s vision (counting fingers at 5 feet) [124]. | Uneventful full recovery [46,47,67,88,89,103,116]. Treatment resulted in recovery, but there was 1 recurrence which also resolved with similar therapy. No further recurrences occurred [48]. Developed dense cyclitic membrane in the eye and lost all functional visual activity, with the eye becoming phthisical. The patient was later given a cosmetic contact lens shell covering the phthisical left eye [54]. Case 1: Patient previously had multiple ocular manifestations which were resolved with a combination of antibiotics. For this particular recurrence of retinal vasculitis: the patient recovered well with the described treatment. Case 2: No follow-up was available for this patient since his discharge Case 3: Stabilised with no recurrence [81]. Eye became phthisical and all vision was lost [83]. Systemic symptoms and floaters improved with the fundi returning to normal, but the scotoma that the patient first presented with persisted and the patient’s VA remained unchanged [112]. Vision remained at counting fingers at 5 feet, loss of vision in the patient’s nonamblyopic left eye necessitated the patient to suddenly retire from dentistry [124]. |
| Tularaemia | Dermacentor spp. D. variabilis D. andersoni Amblyomma americanum | Oculoglandular tularaemia Conjunctival chemosis, episcleritis, conjunctivitis, ptosis, purulent secretions, periorbital oedema, conjunctival injection and hyperaemia, uveitis, conjunctival papule, conjunctival ulcer. Atypical for oculoglandular tularaemia Corneal oedema, raised intraocular pressure, dacryocystitis. Parinaud’s oculoglandular syndrome Associated with preauricular and submandibular lymphadenopathy. Conjunctivitis, periorbital ecchymosis, conjunctival nodules ± ulcers, eyelid oedema, conjunctival follicles with mucous discharge, corneal ulceration, hypopyon. | Tularaemia Case 1: 3 days after cat sneezed and secretions were projected into patient’s eye. Case 2: few days after contact with an ill cat. Case 3: few days after contact with an ill puppy [128]. 3 to 5 days after exposure to contaminated substances [129]. 3 weeks after exposure to an infected rabbit [130]. Few days, no history of tick bite. [131]. Not stated [132,138,139,140]. 2 days after laparotomy for lung biopsy [141]. Parinaud’s oculoglandular syndrome 3 weeks after contact with dead wild rabbit [125]. 5 days after contact with contaminated sewage water and tick bites [134]. Not stated [135]. 4 to 5 days after tick bite [137]. | Tularaemia Case 1: local cold boric compresses, triple-typhoid bacterial IV vaccine. Case 2: hourly instillations of 20% silver iodide followed by cold boric-acid compresses. Case 3: metaphen instillations, cold boric compresses [128]. Aminoglycoside or fluoroquinolone antibiotics for at least 10 days, or doxycycline for at least 15 days. Local therapy included ciprofloxacin and tobramycin eye drops/ointment [129]. Doxycycline 200 mg once/day, for 3 weeks [130]. Initially started on streptomycin and tetracycline, later switched to tetracycline-only targeted antibiotic therapy [131]. IM streptomycin 65 mg/kg/day twice/day for 7 days [132]. Raised intraocular pressure was lowered with IV and PO acetatcolamide, timolol and pilocarpine eyedrops. Laser iridotomy was done due to a narrow anterior chamber. Ciprofloxacin 500 mg twice/day for 10 days [138]. PO amoxicillin-clavulanic acid 1000 mg twice/day for 14 days and gentamicin eye drops. Surgical drainage for dacryocystitis [139]. PO amoxicillin-clavulanic acid 1 g twice/day and topical ciprofloxacin eye drops 4 times/day [140]. Gentamicin sulfate and tetracycline hydrochloride [141]. Parinaud’s oculoglandular syndrome IM streptomycin and IV nafcillin [125]. 10-day course of gentamicin [134]. PO doxycycline 100 mg every 12 h for 10 days [135]. Doxycycline hyclate 100 mg twice/day for 3 weeks and 14 mg/mL topical fortified gentamicin sulfate eye drops hourly to affected eye [137]. | Not stated [128,129,131,132,134,135,140]. Visual loss with central scotoma [130]. Required corneal transplantation due to persistent medial opacities [137]. Intraocular pressure of the right eye decreased from 68 mmHg at first presentation to 26 mmHg at the half-year mark follow-up. Vision was normal [138]. Full recovery [139]. |
| Babesiosis | Ixodes scapularis | Conjunctival injection, retinal haemorrhages, retinal nerve fibre layer infarct, conjunctivitis, eyelid oedema. | 2 months after visiting Shelter Island in New York [142]. 3 months after a blood transfusion [143]. Few months after a blood transfusion [144]. | Not stated [142]. Doxycycline 200 mg/day and trimethoprim-sulfamethoxazole 160/800/per day [143]. Extensive doses of penicillin, hydrocortisone and peritoneal dialysis [144]. | Full recovery [142,143]. Death [144]. |
| Tick-borne Relapsing Fever | Ornithodoros spp. O. hermsi O. parkeri O. turicata | Anterior uveitis, intermediate uveitis, optic neuritis, choroiditis, vitritis, endophthalmitis, floaters, acute iridocyclitis, chronic cyclitis, posterior synechiae, marginal keratitis followed by multiple corneal erosions. | Case 1: 2 months after generalised aches and pains with recurrent episodes of fever, 1 week after an episode of relapsing fever. Case 2: 2 months after pain in head and eyes associated with relapsing fever. Case 3: Not stated. Case 4: 4 months after relapsing fever, with the most recent month having no relapse [147]. Systemic illness occurred 10 days after the patient had been camping in a forest cabin in Eastern Oregon [149]. | For posterior synechiae: mydriatic agents (atropine), 2% cocaine eye drops and heat. For marginal keratitis: 2% silver nitrate [147]. IV Ceftriaxone 1 g twice/day for 3 days, followed by PO cephuroxime 250 mg twice/day for 4 weeks was given for presumed sinusitis noted on computer tomography. Symptoms resolved but the patient developed floaters and blurred vision OD afterwards. Topical prednisolone acetate was given but inflammation persisted, then doxycycline 100 mg/day for 4 weeks was added on to the corticosteroid eye drops for presumed residual infection [149]. | Uneventful full recovery [147,149]. |
| Powassan Encephalitis | Ixodes spp. I. cookei I. marxi I. spinipalpis I. scapularis Dermacentor andersoni | Retinal vein tortuosity, optic disc oedema, ophthalmoplegia, multifocal choroiditis. | Few days after initial symptoms of nausea and vomiting, diarrhoea, dizziness, diplopia and incoordination [196]. | Combination of ceftriaxone, ampicillin and acyclovir [196]. | Residual ophthalmoplegia [196]. |
| Ehrlichiosis | Amblyomma americanum Dermacentor variabilis | CN IV palsy, optic neuritis, disc oedema, orbital myositis, posterior uveitis, cystoid macular oedema, retinal vasculitis, epiretinal membrane. | 12 days after constitutional symptoms of fever, chills, myalgia and malaise [153]. 18 days after initial systemic symptoms [154]. 6 weeks after constitutional symptoms of high fever, myalgia and arthralgia [155]. 1 month after subjective deterioration in vision [156]. | Antibiotics and corticosteroids—oral doxycycline, sub-Tenon triamcinolone injection. PO doxycycline [153]. PO doxycycline 100 mg twice/day [154]. PO doxycycline 100 mg twice/day [155]. Sub-Tenon triamcinolone for both eyes and a prophylactic course of PO doxycycline 100 mg twice/day for 2 weeks [156]. | Full recovery [153,154,155]. Clinical improvement of macular oedema [156]. |
| Rocky Mountain Spotted Fever | Dermacentor spp. D. variabilis D. andersoni Rhipicephalus sanguineus | Conjunctival vasculitis, retinal vasculitis, choroidal vasculitis, conjunctival injection, periorbital oedema, uveitis, keratic precipitates, anterior chamber and vitreous cells. Retinovascular Cotton wool spots, cotton wool exudates, macular oedema, retinal oedema, vascular sheathing, venous tortuosity, retinal artery or vein occlusion, intraretinal haemorrhage and exudates, retinitis, retinal artery sheathing, flame-shaped haemorrhages, macular star figures. Neuro-ophthalmic Disc oedema, optic neuritis, optic neuropathy, neuroretinitis, optic nerve oedema, papilloedema. | Presley reported 6 cases. Case 1: Not stated. Case 2: 10 days after a tick was removed from the patient’s scalp. Case 3: 1 week after the patient removed 2 ticks from his body, and another tick was removed on the day of admission. Case 4: 2 weeks after a tick was removed from the patient’s scalp. Case 5: 6 days after the patient’s father had removed an unattached tick from the patient. Case 6: A history of possible tick bite 2 weeks prior to admission [164]. 10 days after tick bite [165]. 5 days after travel to Mexico, without exposure to stray animals, insects or tick bites [166]. 2 weeks after tick bite [167]. Several months after sustaining tick bites [168]. Presented after a 1-week history of papular skin lesions, associated with 2 weeks of systemic symptoms. She also lived alone with her dog in a Philadelphia tenement. [169]. | Not stated [164]. IV chloramphenicol, PO tetracycline [165]. 14 days of doxycycline [166]. PO doxycycline 100 mg every 12 h for 60 days [167]. PO doxycycline 100 mg twice/day for 14 days [168]. Supportive therapy (IV fluids), IV tetracycline [169]. | Not stated [164]. Uneventful full recovery [165,166,169]. Slow and incomplete recovery of vision (improvement in visual acuity and visual fields) with resolution of optic disc swelling and development of optic disc pallor [167]. Improvement of optic nerve oedema with VA remaining at 20/40 OD and improvement of VA to 20/100 OS. Macular star figures persisted [168]. |
| Mediterranean Spotted Fever | Rhipicephalus sanguineus | Parinaud’s oculoglandular syndrome, corneal manifestations, posterior segment manifestations, dacryoadenitis, multifocal retinitis. Parinaud’s oculoglandular syndrome Conjunctivitis—swollen eyelids, conjunctival hyperemia, and chemosis with mucopurulent discharge. Corneal Manifestations Keratitis, corneal ulcers (ameboid-type), ciliary injection, corneal oedema, corneal inflammatory infiltrates, mild infiltration of the anterior stroma. Posterior Segment Manifestations Acute anterior ischemic optic neuropathy, RAPD, retinal vasculitis, haemorrhages (optic disc, intraretinal, white-centred retinal, subretinal), branch retinal artery and vein occlusions, retinal detachment (serous), optic disc oedema, cotton-wool spots and retinitis with mild vitreous inflammatory reaction, optic disc staining, juxtavascular white retinal lesions, focal vascular sheathing, multiple arterial plaques, macular star, cystoid macular oedema, retinal vascular leakage, delayed filling in a branch retinal vein, multiple hypofluorescent choroidal dots. Ocular complaints: decreased vision, paracentral scotoma, floaters and ocular redness due to conjunctivitis or anterior uveitis. | Average duration of fever before ophthalmic examination was 7 days (range, 3–15). For the 9 (out of 30) patients who had ocular complaints: interval from the onset of fever to ocular symptoms ranged from 2 to 5 days [174]. 4 weeks after the patient had an accidental projection of a jet of contaminated water into his left eye. Could not recall any history of tick bite [175]. 14 days after constitutional symptoms. Tick bite present on left leg [178]. 4 days after the onset of a fever. No history of tick bite [179]. | PO doxycycline for 2 weeks [174]. PO doxycycline 100 mg twice/day for 2 weeks [175]. PO doxycycline 100 mg/12 h, while keratitis was treated with atropine 1% plus tetracycline ointment every twelve hours and occlusion [178]. Doxycycline 200 mg/day for a week [179]. | One eye had retinal neovascularization at the 6-month follow-up, but a further follow-up of 6 months reported no other abnormalities. All posterior segment findings at the acute stage resolved in 3 to 10 weeks; final VA was 20/20 in 42 of 45 affected eyes; a decreased final VA was related to RPE changes due to cystoid macular oedema (1 eye) and age-related cataract (2 eyes) [174]. Uneventful recovery [175,178]. Clinical improvement: BCVA counting fingers OD and 20/20 OS increased to 20/400 OD and 20/20 OS. Optic disc oedema OD was replaced by pallor, otherwise the patient recovered [179]. |
| Colorado Tick Fever | Dermacentor andersoni | Retro-orbital pain, photophobia and conjunctival injection. | NIL | Supportive treatment [199]. | NIL |
| Toxoplasmosis | Studies have suggested the possibility of transmission of Toxoplasma gondii through the following ticks: Dermacentor variabilis, Dermacentor andersoni, Amblyomma americanum, Dermacentor reticulatus, Ixodes ricinus, Amblyomma cajennense complex, mainly Amblyomma sculptum, Ornithodorus moubata and Haemaphysalis longicornis | Posterior uveitis. Particularly focal retinochoroiditis. Less commonly: serous macular detachment, retinal vasculitis, retinal detachment, neuroretinitis, papillitis, disc haemorrhages with venous engorgement, optic atrophy secondary to optic nerve involvement, macular star, cystoid macular oedema, chronic iridocyclitis, cataract formation, secondary glaucoma, band keratopathy. Association with primary intraocular lymphoma. Focal retinitis with surrounding retinal and macular pigmentary changes, vitritis, cells and flare of anterior chamber and vitreous cells. | 2 month history of foggy vision without systemic symptoms [192]. | Recommended: A combination of antiprotozoal agents, systemic steroids if no contraindication, topical steroids and cycloplegics if anterior segment inflammation is present. Initial treatment was for presumed ocular toxoplasmosis with trimethoprim 160 mg and sulfamethoxazole 800 mg twice/day which resolved the focal retinitis. Patient later had recurrences of increased floaters and blurred vision, and was restarted on antibiotics. Systemic chemotherapy was instituted upon diagnosis of lymphoma [192]. | Patient did not respond to chemotherapy and died shortly thereafter [192]. |
| Tick-Borne Encephalitis | Ixodes spp. I. ricinus I. persulcatus | Non-granulomatous anterior uveitis, flame-shaped and dot retinal haemorrhages, vitritis, vitreous haze and cells. | 6 weeks after a tick bite, where he experienced a flu-like illness 10 days later but no erythema migrans [197]. | Topical prednisolone acetate 1% 6 times/day for anterior uveitis. Empirical IV acyclovir 10 mg/kg thrice/day was initiated for possible herpes meningoencephalitis with retinal involvement [197]. | Full recovery [197]. |
References
- Heylen, D.; Lasters, R.; Adriaensen, F.; Fonville, M.; Sprong, H.; Matthysen, E. Ticks and Tick-Borne Diseases in the City: Role of Landscape Connectivity and Green Space Characteristics in a Metropolitan Area. Sci. Total Environ. 2019, 670, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Climate Change Indicators: Lyme Disease. Available online: https://www.epa.gov/climate-indicators/climate-change-indicators-lyme-disease#:~:text=Studies%20provide%20evidence%20that%20climate,are%20strongly%20influenced%20by%20temperature (accessed on 14 August 2022).
- Beard, C.B.; Eisen, R.J.; Barker, C.M.; Garofalo, J.F.; Hahn, M.; Hayden, M.; Monaghan, A.J.; Ogden, N.H.; Schramm, P.J. Chapter 5: Vectorborne Diseases. In The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment; Climate and Health Assessment; US Global Change Research Program: Washington, DC, USA, 2016; pp. 129–156. [Google Scholar]
- Centers for Disease Control and Prevention. Ticks—Diseases Transmitted by Ticks. Available online: https://www.cdc.gov/ticks/diseases/index.html (accessed on 2 July 2022).
- Raja, H.; Starr, M.R.; Bakri, S.J. Ocular Manifestations of Tick-Borne Diseases. Surv. Ophthalmol. 2016, 61, 726–744. [Google Scholar] [CrossRef] [PubMed]
- Ben-Harari, R.R. Tick Transmission of Toxoplasmosis. Expert Rev. Anti-Infect. Ther. 2019, 17, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Relapsing Fever—Transmission. Available online: https://www.cdc.gov/relapsing-fever/transmission/index.html (accessed on 2 July 2022).
- Lai, K.W.; Lim, D.K.A.; Lim, B.X.H.; Yuen, Y.S.; Lim, C.H.L. Ticked off: A Case of a Tick Involving the Lower Eyelid. CJEM 2020, 22, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Han, E.-T.; Han, S.B. Tick Infestation of the Upper Eyelid. Korean J. Ophthalmol. 2020, 34, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Uzair, M.; Varma, D. Tick Infestation of Upper Eyelid. Indian J. Ophthalmol. 2020, 68, 2269. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Shrestha, S.; Shrestha, A.; Suwal, B.; Sharma, S. Tick Infestation Masquerading as a Nodule in the Eye Lid. Nepal J. Ophthalmol. 2020, 12, 106–109. [Google Scholar] [CrossRef]
- Rai, R.; Yoon, M.K.; Stacy, R.C. Tick Infestation of the Eyelid with Histopathologic Characterization. Ophthalmic Plast. Reconstr. Surg. 2016, 32, e55–e58. [Google Scholar] [CrossRef]
- Parajuli, S.; Sunar, P.; Yadav, S. Tick Infestation on the Lower Eyelid in an Elderly Female: A Case Report. J. Parasit. Dis. 2021, 45, 118–120. [Google Scholar] [CrossRef]
- Uzun, A.; Gök, M.; İşcanlı, M.D. Tick Infestation of Eyelid: Two Case Reports. Turk. J. Ophthalmol. 2016, 46, 248–250. [Google Scholar] [CrossRef]
- Jaroudi, M.O.; Mansour, A.M.; Ma’luf, R.; Meduri, A.; Tawil, A.; Younis, M.H. Large Tick (Ixodes) Infestation of the Upper Eyelid Presenting as Eyelid Mass and Preseptal Cellulitis. Case Rep. Ophthalmol. 2019, 10, 403–407. [Google Scholar] [CrossRef]
- Samaha, A.; Green, W.R.; Traboulsi, E.I.; Ma’luf, R. Tick Infestation of the Eyelid. Am. J. Ophthalmol. 1998, 125, 263–264. [Google Scholar] [CrossRef]
- Singh, M.; Gopalakrishnakone, P.; Yeoh, R.L.S. Ixodes Tick Infestation of the Eyelid of a Child. Can. J. Ophthalmol. 2006, 41, 783–784. [Google Scholar] [CrossRef]
- Arias-Peso, B.; Subías-Perié, M. Hard Tick Infestation of the Eyelid. Med. Clin. 2021, 157, 265. [Google Scholar] [CrossRef]
- Varma, R.R.; Varma, P.; Kumar, A. Tick Infestation of the Eyelid. Rev. Soc. Bras. Med. Trop. 2020, 53, e20190599. [Google Scholar] [CrossRef]
- Park, J.; Suh, E. Tick Infestation of the Eyelid and Removal with Forceps and Punch Biopsy. J. Craniofac. Surg. 2016, 27, 2098–2100. [Google Scholar] [CrossRef]
- Kuriakose, R.K.; Grant, L.W.; Chin, E.K.; Almeida, D.R.P. Deer Tick Masquerading as Pigmented Conjunctival Lesion. Am. J. Ophthalmol. Case Rep. 2017, 5, 97–98. [Google Scholar] [CrossRef]
- Willen, C.; Mullen, G.R.; Yee, J.; Read, R.W. Conjunctival Attachment of a Tick: Clinicopathologic Report of a Case. J. Emerg. Med. 2011, 40, e41–e44. [Google Scholar] [CrossRef]
- Kanar, H.S.; Karaman, S. Optical Coherence Tomography Guided Conjunctival Tick Infestation Treatment: A Case Report. Photodiagn. Photodyn. Ther. 2021, 34, 102219. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Lyme Disease Home Page. Available online: https://www.cdc.gov/lyme/index.html (accessed on 2 July 2022).
- MacDonald, A.B. Lyme Disease. A Neuro-Ophthalmologic View. J. Clin. Neuroophthalmol. 1987, 7, 185–190. [Google Scholar] [CrossRef]
- Karma, A.; Mikkilä, H. Ocular Manifestations and Treatment of Lyme Disease. Curr. Opin. Ophthalmol. 1996, 7, 7–12. [Google Scholar] [CrossRef]
- Smith, J.L. Ocular Lyme Borreliosis—1991. Int. Ophthalmol. Clin. 1991, 31, 17–38. [Google Scholar] [CrossRef]
- Zaidman, G.W. The Ocular Manifestations of Lyme Disease. Int. Ophthalmol. Clin. 1997, 37, 13–28. [Google Scholar] [CrossRef]
- Winward, K.E.; Smith, J.L.; Culbertson, W.W.; Paris-Hamelin, A. Ocular Lyme Borreliosis. Am. J. Ophthalmol. 1989, 108, 651–657. [Google Scholar] [CrossRef]
- Lesser, R.L. Ocular Manifestations of Lyme Disease. Am. J. Med. 1995, 98, 60S–62S. [Google Scholar] [CrossRef]
- Bertuch, A.W.; Rocco, E.; Schwartz, E.G. Lyme Disease: Ocular Manifestations. Ann. Ophthalmol. 1988, 20, 376–378. [Google Scholar] [CrossRef]
- Mora, P.; Carta, A. Ocular Manifestations of Lyme Borreliosis in Europe. Int. J. Med. Sci. 2009, 6, 124–125. [Google Scholar] [CrossRef] [Green Version]
- Aaberg, T.M. The Expanding Ophthalmologic Spectrum of Lyme Disease. Am. J. Ophthalmol. 1989, 107, 77–80. [Google Scholar] [CrossRef]
- Karma, A.; Seppälä, I.; Mikkilä, H.; Kaakkola, S.; Viljanen, M.; Tarkkanen, A. Diagnosis and Clinical Characteristics of Ocular Lyme Borreliosis. Am. J. Ophthalmol. 1995, 119, 127–135. [Google Scholar] [CrossRef]
- Mikkilä, H.O.; Seppälä, I.J.; Viljanen, M.K.; Peltomaa, M.P.; Karma, A. The Expanding Clinical Spectrum of Ocular Lyme Borreliosis. Ophthalmology 2000, 107, 581–587. [Google Scholar] [CrossRef]
- Berglöff, J.; Gasser, R.; Feigl, B. Ophthalmic Manifestations in Lyme Borreliosis. A Review. J. Neuroophthalmol. 1994, 14, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Winterkorn, J.M. Lyme Disease: Neurologic and Ophthalmic Manifestations. Surv. Ophthalmol. 1990, 35, 191–204. [Google Scholar] [CrossRef]
- Hu, L. Clinical Manifestations of Lyme Disease in Adults. Available online: https://www.uptodate.com/contents/clinical-manifestations-of-lyme-disease-in-adults (accessed on 14 July 2022).
- Kornmehl, E.W.; Lesser, R.L.; Jaros, P.; Rocco, E.; Steere, A.C. Bilateral Keratitis in Lyme Disease. Ophthalmology 1989, 96, 1194–1197. [Google Scholar] [CrossRef]
- Miyashiro, M.J.; Yee, R.W.; Patel, G.; Ruiz, R.S. Lyme Disease Associated with Unilateral Interstitial Keratitis. Cornea 1999, 18, 115–116. [Google Scholar] [CrossRef]
- Sathiamoorthi, S.; Smith, W.M. The Eye and Tick-Borne Disease in the United States. Curr. Opin. Ophthalmol. 2016, 27, 530–537. [Google Scholar] [CrossRef]
- Steere, A.C.; Malawista, S.E.; Snydman, D.R.; Shope, R.E.; Andiman, W.A.; Ross, M.R.; Steele, F.M. Lyme Arthritis: An Epidemic of Oligoarticular Arthritis in Children and Adults in Three Connecticut Communities. Arthritis Rheum. 1977, 20, 7–17. [Google Scholar] [CrossRef]
- Mombaerts, I.M.; Maudgal, P.C.; Knockaert, D.C. Bilateral Follicular Conjunctivitis as a Manifestation of Lyme Disease. Am. J. Ophthalmol. 1991, 112, 96–97. [Google Scholar] [CrossRef]
- Zaidman, G.W. Episcleritis and Symblepharon Associated with Lyme Keratitis. Am. J. Ophthalmol. 1990, 109, 487–488. [Google Scholar] [CrossRef]
- Sainz de la Maza, M.; Hemady, R.K.; Foster, C.S. Infectious Scleritis: Report of Four Cases. Doc. Ophthalmol. 1993, 83, 33–41. [Google Scholar] [CrossRef]
- Orlin, S.E.; Lauffer, J.L. Lyme Disease Keratitis. Am. J. Ophthalmol. 1989, 107, 678–680. [Google Scholar] [CrossRef]
- Oldham, G.W.; Seitzman, G.D. Unilateral Posterior Stromal Keratitis Possibly Secondary to Lyme Disease. Cornea 2013, 32, 196–198. [Google Scholar] [CrossRef]
- Baum, J.; Barza, M.; Weinstein, P.; Groden, J.; Aswad, M. Bilateral Keratitis as a Manifestation of Lyme Disease. Am. J. Ophthalmol. 1988, 105, 75–77. [Google Scholar] [CrossRef]
- Bertuch, A.W.; Rocco, E.; Schwartz, E.G. Eye Findings in Lyme Disease. Conn. Med. 1987, 51, 151–152. [Google Scholar]
- Flach, A.J.; Lavoie, P.E. Episcleritis, Conjunctivitis, and Keratitis as Ocular Manifestations of Lyme Disease. Ophthalmology 1990, 97, 973–975. [Google Scholar] [CrossRef]
- Fox, G.M.; Heilskov, T.; Smith, J.L. Cogan’s Syndrome and Seroreactivity to Lyme Borreliosis. J. Clin. Neuroophthalmol. 1990, 10, 83–87. [Google Scholar]
- Balcer, L.J.; Winterkorn, J.M.; Galetta, S.L. Neuro-Ophthalmic Manifestations of Lyme Disease. J. Neuroophthalmol. 1997, 17, 108–121. [Google Scholar] [CrossRef]
- De Luise, V.P.; O’Leary, M.J. Peripheral Ulcerative Keratitis Related to Lyme Disease. Am. J. Ophthalmol. 1991, 111, 244–245. [Google Scholar] [CrossRef]
- Kauffmann, D.J.; Wormser, G.P. Ocular Lyme Disease: Case Report and Review of the Literature. Br. J. Ophthalmol. 1990, 74, 325–327. [Google Scholar] [CrossRef] [Green Version]
- Bernard, A.; Seve, P.; Abukhashabh, A.; Roure-Sobas, C.; Boibieux, A.; Denis, P.; Broussolle, C.; Mathis, T.; Kodjikian, L. Lyme-Associated Uveitis: Clinical Spectrum and Review of Literature. Eur. J. Ophthalmol. 2020, 30, 874–885. [Google Scholar] [CrossRef]
- Howlett, J.M.; Booth, A.P. Ocular Inflammation as a Manifestation of Lyme Borreliosis. BMJ 2012, 345, e4721. [Google Scholar] [CrossRef]
- Amer, R.; Brannan, S.; Forrester, J.V. Inflammatory Choroidal Neovascular Membrane in Presumed Ocular Lyme Borreliosis. Acta. Ophthalmol. 2009, 87, 346–348. [Google Scholar] [CrossRef]
- Mahne, J.; Kranjc, B.S.; Strle, F.; Ružić-Sabljić, E.; Arnež, M. Panuveitis Caused by Borrelia burgdorferi Sensu Lato Infection. Pediatr. Infect. Dis. J. 2015, 34, 102–104. [Google Scholar] [CrossRef]
- Sibony, P.; Halperin, J.; Coyle, P.K.; Patel, K. Reactive Lyme Serology in Optic Neuritis. J. Neuroophthalmol. 2005, 25, 71–82. [Google Scholar] [CrossRef]
- Rothova, A.; Kuiper, H.; Spanjaard, L.; Dankert, J.; Breebaart, A.C. Spiderweb Vitritis in Lyme Borreliosis. Lancet 1991, 337, 490–491. [Google Scholar] [CrossRef]
- Kuiper, H.; Koelman, J.H.; Hager, M.J. Vitreous Clouding Associated with Lyme Borreliosis. Am. J. Ophthalmol. 1989, 108, 453–454. [Google Scholar] [CrossRef]
- Schubert, H.D.; Greenebaum, E.; Neu, H.C. Cytologically Proven Seronegative Lyme Choroiditis and Vitritis. Retina 1994, 14, 39–42. [Google Scholar] [CrossRef]
- Krist, D.; Wenkel, H. Posterior Scleritis Associated with Borrelia burgdorferi (Lyme Disease) Infection. Ophthalmology 2002, 109, 143–145. [Google Scholar] [CrossRef]
- Winward, K.E.; Smith, J.L. Ocular Disease in Caribbean Patients with Serologic Evidence of Lyme Borreliosis. J. Clin. Neuroophthalmol. 1989, 9, 65–70. [Google Scholar]
- Boutros, A.; Rahn, E.; Nauheim, R. Iritis and Papillitis as a Primary Presentation of Lyme Disease. Ann. Ophthalmol. 1990, 22, 24–25. [Google Scholar]
- Bodine, S.R.; Marino, J.; Camisa, T.J.; Salvate, A.J. Multifocal Choroiditis with Evidence of Lyme Disease. Ann. Ophthalmol. 1992, 24, 169–173. [Google Scholar]
- Bialasiewicz, A.A.; Ruprecht, K.W.; Naumann, G.O.; Blenk, H. Bilateral Diffuse Choroiditis and Exudative Retinal Detachments with Evidence of Lyme Disease. Am. J. Ophthalmol. 1988, 105, 419–420. [Google Scholar] [CrossRef]
- Havuz, E.; Güdül Havuz, S. Lyme Disease Atypically Presenting with a Singular Symptom: Unilateral Chorioretinitis. Eur. J. Ophthalmol. 2021, 31, NP151–NP156. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.C.; Marek, N.; Kodner, C. Infection of Syrian Hamsters with Lyme Disease Spirochetes. J. Clin. Microbiol. 1984, 20, 1099–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duray, P.H.; Johnson, R.C. The Histopathology of Experimentally Infected Hamsters with the Lyme Disease Spirochete, Borrelia burgdorferi. Exp. Biol. Med. 1986, 181, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Preac-Mursic, V.; Pfister, H.W.; Spiegel, H.; Burk, R.; Wilske, B.; Reinhardt, S.; Böhmer, R. First Isolation of Borrelia burgdorferi from an Iris Biopsy. J. Clin. Neuroophthalmol. 1993, 13, 155–161, discussion 162. [Google Scholar] [PubMed]
- Tusa, R.J.; Newman, S.A.; Winterkorn, J.M.S. Neuro-Ophthalmological Disorders: Diagnostic Work-Up and Management; Marcel Dekker: New York, NY, USA, 1995; pp. 74–80. [Google Scholar]
- Lesser, R.L.; Kornmehl, E.W.; Pachner, A.R.; Kattah, J.; Hedges, T.R.; Newman, N.M.; Ecker, P.A.; Glassman, M.I. Neuro-Ophthalmologic Manifestations of Lyme Disease. Ophthalmology 1990, 97, 699–706. [Google Scholar] [CrossRef]
- Issa, R.; DeSouza, S.A.M. Recurrent Bilateral Chorioretinitis with Positive Lyme Serology: A Case Report. J. Med. Case. Rep. 2021, 15, 253. [Google Scholar] [CrossRef]
- Niutta, A.; Barcaroli, I.; Palombi, E. Monolateral Chorioretinitis with Multiple Foci in One Case of Lyme Disease. Ann. Ophthalmol. 1993, 25, 257–261. [Google Scholar]
- Wolf, M.D.; Folk, J.C.; Nelson, J.A.; Peeples, M.E. Acute, Posterior, Multifocal, Placoid, Pigment Epitheliopathy and Lyme Disease. Arch. Ophthalmol. 1992, 110, 750. [Google Scholar] [CrossRef]
- Framme, C.; Sachs, H.G.; Gabler, B.; Roider, J. Fundus Autofluorescence in APMPPE in Association with Lyme Disease. Retina 2002, 22, 653–657. [Google Scholar] [CrossRef]
- Suttorp-Schulten, M.S.; Luyendijk, L.; van Dam, A.P.; de Keizer, R.J.; Baarsma, G.S.; Bos, P.J.; Rothova, A. Birdshot Chorioretinopathy and Lyme Borreliosis. Am. J. Ophthalmol. 1993, 115, 149–153. [Google Scholar] [CrossRef]
- Agarwal, A.; Rübsam, A.; zur Bonsen, L.; Pichi, F.; Neri, P.; Pleyer, U. A Comprehensive Update on Retinal Vasculitis: Etiologies, Manifestations and Treatments. J. Clin. Med. 2022, 11, 2525. [Google Scholar] [CrossRef]
- Leys, A.M.; Schönherr, U.; Lang, G.E.; Naumann, G.O.; Goubau, P.; Honore, A.; Valvekens, F. Retinal Vasculitis in Lyme Borreliosis. Bull. Soc. Belg. Ophtalmol. 1995, 259, 205–214. [Google Scholar]
- Smith, J.L.; Winward, K.E.; Nicholson, D.F.; Albert, D.W. Retinal Vasculitis in Lyme Borreliosis. J. Clin. Neuroophthalmol. 1991, 11, 7–15. [Google Scholar] [CrossRef]
- Zierhut, M.; Kreissig, I.; Pickert, A. Panuveitis with Positive Serological Tests for Syphilis and Lyme Disease. J. Clin. Neuroophthalmol. 1989, 9, 71–75, discussion 76–78. [Google Scholar]
- Steere, A.C.; Duray, P.H.; Kauffmann, D.J.; Wormser, G.P. Unilateral Blindness Caused by Infection with the Lyme Disease Spirochete, Borrelia burgdorferi. Ann. Intern. Med. 1985, 103, 382–384. [Google Scholar] [CrossRef]
- Murillo, G.; Ramírez, B.; Romo, L.A.; Muñoz-Sanz, A.; Hileeto, D.; Calonge, M. Oculopalpebral Borreliosis as an Unusual Manifestation of Lyme Disease. Cornea 2013, 32, 87–90. [Google Scholar] [CrossRef]
- Seidenberg, K.B.; Leib, M.L. Orbital Myositis with Lyme Disease. Am. J. Ophthalmol. 1990, 109, 13–16. [Google Scholar] [CrossRef]
- Holak, H.; Holak, N.; Huzarska, M.; Holak, S. Tick Inoculation in an Eyelid Region: Report on Five Cases with One Complication of the Orbital Myositis Associated with Lyme Borreliosis. Klin. Ocz. 2006, 108, 220–224. [Google Scholar]
- Carvounis, P.E.; Mehta, A.P.; Geist, C.E. Orbital Myositis Associated with Borrelia burgdorferi (Lyme Disease) infection. Ophthalmology 2004, 111, 1023–1028. [Google Scholar] [CrossRef]
- Sauer, A.; Speeg-Schatz, C.; Hansmann, Y. Two Cases of Orbital Myositis as a Rare Feature of Lyme Borreliosis. Case Rep. Infect. Dis. 2011, 2011, 372470. [Google Scholar] [CrossRef]
- Xu, L.; Winn, B.J.; Odel, J.G. Lyme-Associated Orbital Inflammation Presenting as Painless Subacute Unilateral Ptosis. J. Neuroophthalmol. 2012, 32, 246–248. [Google Scholar] [CrossRef]
- Douglas, V.P.; Douglas, K.A.A.; Reinshagen, K.L.; Chwalisz, B.K. Case 292: Lyme Neuroborreliosis. Radiology 2021, 300, 484–488. [Google Scholar] [CrossRef]
- Bababeygy, S.R.; Quiros, P.A. Isolated Trochlear Palsy Secondary to Lyme Neuroborreliosis. Int. Ophthalmol. 2011, 31, 493–495. [Google Scholar] [CrossRef]
- Albermann, K.; Blunck, W.; Helwig, H. Neuro-Ophthalmological Manifestations of Tick-Borne Borreliosis: A Case Report. Eur. J. Pediatr. 1993, 152, 1046–1047. [Google Scholar] [CrossRef]
- Burkhard, C.; Gleichmann, M.; Wilhelm, H. Optic Nerve Lesion Following Neuroborreliosis: A Case Report. Eur. J. Ophthalmol. 2001, 11, 203–206. [Google Scholar] [CrossRef] [Green Version]
- Clark, J.R.; Carlson, R.D.; Sasaki, C.T.; Pachner, A.R.; Steere, A.C. Facial Paralysis in Lyme Disease. Laryngoscope 1985, 95, 1341–1345. [Google Scholar]
- Sharma, V.; Biswas, S. Self-Limiting Fourth and Sixth Cranial Nerve Palsy after Lyme Disease. J. Pediatr. Ophthalmol. Strabismus 2010, 47, 114–116. [Google Scholar] [CrossRef]
- Ackermann, R.; Rehse-Küpper, B.; Gollmer, E.; Schmidt, R. Chronic Neurologic Manifestations of Erythema Migrans Borreliosis. Ann. N. Y. Acad. Sci. 1988, 539, 16–23. [Google Scholar] [CrossRef]
- Pachner, A.R. Spirochetal Diseases of the CNS. Neurol. Clin. 1986, 4, 207–222. [Google Scholar] [CrossRef]
- Reik, L.; Steere, A.C.; Bartenhagen, N.H.; Shope, R.E.; Malawista, S.E. Neurologic Abnormalities of Lyme Disease. Medicine 1979, 58, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Stiernstedt, G.; Gustafsson, R.; Karlsson, M.; Svenungsson, B.; Sköldenberg, B. Clinical Manifestations and Diagnosis of Neuroborreliosis. Ann. N. Y. Acad. Sci. 1988, 539, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.L. Neuro-Ocular Lyme Borreliosis. Neurol. Clin. 1991, 9, 35–53. [Google Scholar] [CrossRef]
- Škiljić, D.; Gustavsson, M.; Dotevall, L.; Norrsell, K.; Grönlund, M.A. Ophthalmological Findings in Neuroborreliosis-a Prospective Study Performed in Western Sweden. Acta. Ophthalmol. 2019, 97, 44–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zrinsćak, O.; Masnec-Paskvalin, S.; Corak, M.; Baćani, B.; Mandić, Z. Paralytic Strabismus as a Manifestation of Lyme Borreliosis. Coll. Antropol. 2005, 29, 137–139. [Google Scholar] [PubMed]
- Glauser, T.A.; Brennan, P.J.; Galetta, S.L. Reversible Horner’s Syndrome and Lyme Disease. J. Clin. Neuroophthalmol. 1989, 9, 225–228. [Google Scholar] [PubMed]
- Reik, L.; Burgdorfer, W.; Donaldson, J.O. Neurologic Abnormalities in Lyme Disease without Erythema Chronicum Migrans. Am. J. Med. 1986, 81, 73–78. [Google Scholar] [CrossRef]
- Boudreault, K.; Durand, M.L.; Rizzo, J.F. Investigation-Directed Approach to Inflammatory Optic Neuropathies. Semin. Ophthalmol. 2016, 31, 117–130. [Google Scholar] [CrossRef]
- Bhatti, M.T. Optic Neuropathy from Viruses and Spirochetes. Int. Ophthalmol. Clin. 2007, 47, 37–66. [Google Scholar] [CrossRef]
- Mata-Moret, L.; Garcia-Villanueva, C.; Monferrer-Adsuara, C.; Castro Navarro, V.; Cervera-Taulet, E. Atypical Papillitis: An Isolated Manifestation of Lyme Disease. Eur. J. Ophthalmol. 2020, 30, NP46–NP52. [Google Scholar] [CrossRef]
- Scott, I.U.; Silva-Lepe, A.; Siatkowski, R.M. Chiasmal Optic Neuritis in Lyme Disease. Am. J. Ophthalmol. 1997, 123, 136–138. [Google Scholar] [CrossRef]
- Blanc, F.; Ballonzoli, L.; Marcel, C.; De Martino, S.; Jaulhac, B.; de Seze, J. Lyme Optic Neuritis. J. Neurol. Sci. 2010, 295, 117–119. [Google Scholar] [CrossRef]
- Stricker, R.B.; Lautin, A. Lyme Disease and Optic Neuritis: Long-Term Follow-up of Seropositive Patients. Neurology 2003, 61, 1162, author reply 1162–1163. [Google Scholar] [CrossRef]
- Krim, E.; Guehl, D.; Burbaud, P.; Lagueny, A. Retrobulbar Optic Neuritis: A Complication of Lyme Disease? J. Neurol. Neurosurg. Psychiatry 2007, 78, 1409–1410. [Google Scholar] [CrossRef] [Green Version]
- Lightman, D.A.; Brod, R.D. Branch Retinal Artery Occlusion Associated with Lyme Disease. Arch. Ophthalmol. 1991, 109, 1198–1199. [Google Scholar] [CrossRef]
- Wu, G.; Lincoff, H.; Ellsworth, R.M.; Haik, B.G. Optic Disc Edema and Lyme Disease. Ann. Ophthalmol. 1986, 18, 252–255. [Google Scholar]
- Peter, L.; Jung, J.; Tilikete, C.; Ryvlin, P.; Mauguiere, F. Opsoclonus-Myoclonus as a Manifestation of Lyme Disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 1090–1091. [Google Scholar] [CrossRef]
- Correll, M.H.; Datta, N.; Arvidsson, H.S.S.; Melsom, H.A.; Thielberg, A.K.; Bjerager, M.; Brodsky, M.C.; Saunte, J.P. Lyme Neuroborreliosis: A Treatable Cause of Acute Ocular Motor Disturbances in Children. Br. J. Ophthalmol. 2015, 99, 1401–1404. [Google Scholar] [CrossRef]
- Gibaud, M.; Pauvert, O.; Gueden, S.; Durigneux, J.; Van Bogaert, P. Opsoclonus in a Child with Neuroborreliosis: Case Report and Review of the Literature. Arch. Pediatr. 2019, 26, 118–119. [Google Scholar] [CrossRef]
- Babu, K.; Murthy, P.R. Neuroretinitis as a Manifestation of Lyme Disease in South India: A Case Report. Ocul. Immunol. Inflamm. 2010, 18, 97–98. [Google Scholar] [CrossRef]
- Vanya, M.; Fejes, I.; Jako, M.; Tula, A.; Terhes, G.; Janaky, M.; Bartfai, G. Lyme Disease Associated Neuroretinitis-Case Report. Acta Microbiol. Immunol. Hung. 2015, 62, 403–408. [Google Scholar] [CrossRef]
- Guliani, B.P.; Kumar, S.; Chawla, N.; Mehta, A. Neuroretinitis as Presenting and the Only Presentation of Lyme Disease: Diagnosis and Management. Indian J. Ophthalmol. 2017, 65, 250–252. [Google Scholar] [CrossRef]
- Karma, A.; Stenborg, T.; Summanen, P.; Immonen, I.; Mikkilä, H.; Seppälä, I. Long-Term Follow-up of Chronic Lyme Neuroretinitis. Retina 1996, 16, 505–509. [Google Scholar] [CrossRef]
- Lima, L.H.; Nascimento, F.A.; Itikawa, H.; Sato, M. Lyme Disease and Interdigitation Zone Loss on Optical Coherence Tomography. Retina 2021, 41, e28–e29. [Google Scholar] [CrossRef]
- Buckle, M.; Majid, M.A.; Lee, R.; Steeples, L.R. Full-Thickness Macular Hole: A Rare Complication of Borrelia burgdorferi Neuroretinitis. BMJ Case Rep. 2017, 2017, bcr-2016-219019. [Google Scholar] [CrossRef]
- Koch, F.; Augustin, A.J.; Böker. Neuroborreliosis with Retinal Pigment Epithelium Detachments. Ger. J. Ophthalmol. 1996, 5, 12–15. [Google Scholar]
- Pizzarello, L.D.; MacDonald, A.B.; Semlear, R.; DiLeo, F.; Berger, B. Temporal Arteritis Associated with Borrelia Infection. A Case Report. J. Clin. Neuroophthalmol. 1989, 9, 3–6. [Google Scholar] [CrossRef]
- Thompson, S.; Omphroy, L.; Oetting, T. Parinaud’s Oculoglandular Syndrome Attributable to an Encounter with a Wild Rabbit. Am. J. Ophthalmol. 2001, 131, 283–284. [Google Scholar] [CrossRef]
- Petersen, J.M.; Mead, P.S.; Schriefer, M.E. Francisella tularensis: An Arthropod-Borne Pathogen. Vet. Res. 2009, 40, 9. [Google Scholar] [CrossRef] [Green Version]
- Gürcan, Ş. Epidemiology of Tularemia. Balk. Med. J. 2014, 31, 3–10. [Google Scholar] [CrossRef]
- Siniscal, A.A. Oculoglandular Tularemia; Report of Three Cases with Unusual Contacts. Am. J. Ophthalmol. 1946, 29, 698–710. [Google Scholar] [PubMed]
- Eren Gok, S.; Kocagul Celikbas, A.; Baykam, N.; Atay Buyukdemirci, A.; Eroglu, M.N.; Evren Kemer, O.; Dokuzoguz, B. Evaluation of Tularemia Cases Focusing on the Oculoglandular Form. J. Infect. Dev. Ctries. 2014, 8, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Terrada, C.; Azza, S.; Bodaghi, B.; Le Hoang, P.; Drancourt, M. Rabbit Hunter Uveitis: Case Report of Tularemia Uveitis. BMC Ophthalmol. 2016, 16, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosker, M.; Sener, D.; Kilic, O.; Akil, F.; Yilmaz, M.; Ozturk, O.; Cokugras, H.; Camcioglu, Y.; Akcakaya, N. A Case of Oculoglandular Tularemia Resistant to Medical Treatment. Scand. J. Infect. Dis. 2013, 45, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Bloom, M.E.; Shearer, W.T.; Barton, L.L. Oculoglandular Tularemia in an Inner City Child. Pediatrics 1973, 51, 564–566. [Google Scholar] [CrossRef]
- Arjmand, P.; Yan, P.; O’Connor, M.D. Parinaud Oculoglandular Syndrome 2015: Review of the Literature and Update on Diagnosis and Management. J. Clin. Exp. Ophthalmol. 2015, 6, 1000443. [Google Scholar] [CrossRef] [Green Version]
- Halperin, S.A.; Gast, T.; Ferrieri, P. Oculoglandular Syndrome Caused by Francisella tularensis. Clin. Pediatr. 1985, 24, 520–522. [Google Scholar] [CrossRef]
- Altuntas, E.E.; Polat, K.; Durmuş, K.; Uysal, I.Ö.; Müderris, S. Tularemia and the Oculoglandular Syndrome of Parinaud. Braz. J. Infect. Dis. 2012, 16, 90–91. [Google Scholar] [CrossRef] [Green Version]
- Kantardjiev, T.; Padeshki, P.; Ivanov, I.N. Diagnostic Approaches for Oculoglandular Tularemia: Advantages of PCR. Br. J. Ophthalmol. 2007, 91, 1206–1208. [Google Scholar] [CrossRef] [Green Version]
- Steinemann, T.L.; Sheikholeslami, M.R.; Brown, H.H.; Bradsher, R.W. Oculoglandular Tularemia. Arch. Ophthalmol. 1999, 117, 132–133. [Google Scholar] [CrossRef]
- Pärssinen, O.; Rummukainen, M. Acute Glaucoma and Acute Corneal Oedema in Association with Tularemia. Acta Ophthalmol. Scand. 1997, 75, 732–734. [Google Scholar] [CrossRef]
- Celik, T.; Yuksel, D.; Kosker, M.; Turkoglu, E.B. Unilateral Acute Dacryocystitis Associated with Oculoglandular Tularemia: A Case Report. Semin. Ophthalmol. 2013, 28, 91–93. [Google Scholar] [CrossRef]
- Köse, H.C.; Hoşal, M.B. A Rare Complication of Oropharyngeal Tularemia: Dacryocystitis. Turk. J. Ophthalmol. 2019, 49, 164–167. [Google Scholar] [CrossRef]
- Marcus, D.M.; Frederick, A.R.; Hodges, T.; Allan, J.D.; Albert, D.M. Typhoidal Tularemia. Arch. Ophthalmol. 1990, 108, 118–119. [Google Scholar] [CrossRef]
- Zweifach, P.H.; Shovlin, J. Retinal Nerve Fiber Layer Infarct in a Patient with Babesiosis. Am. J. Ophthalmol. 1991, 112, 597–598. [Google Scholar] [CrossRef]
- Strizova, Z.; Havlova, K.; Patek, O.; Smrz, D.; Bartunkova, J. The First Human Case of Babesiosis Mimicking Reiter’s Syndrome. Folia Parasitol. 2020, 67, 31. [Google Scholar] [CrossRef]
- Fitzpatrick, J.E.P.; Kennedy, C.C.; McGeown, M.G.; Oreopoulos, D.G.; Robertson, J.H.; Soyannwo, M.A. Further Details of Third Recorded Case of Redwater (Babesiosis) in Man. Br. Med. J. 1969, 4, 768. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Relapsing Fever-Distribution. Available online: https://www.cdc.gov/relapsing-fever/distribution/index.html (accessed on 14 July 2022).
- Dworkin, M.S.; Anderson, D.E., Jr.; Schwan, T.G.; Shoemaker, P.C.; Banerjee, S.N.; Kassen, B.O.; Burgdorfer, W. Tick-Borne Relapsing Fever in the Northwestern United States and Southwestern Canada. Clin. Infect. Dis. 1998, 26, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, J.B. Ocular Complications in Relapsing Fever. Br. J. Ophthalmol. 1943, 27, 68–80. [Google Scholar] [CrossRef] [Green Version]
- Cadavid, D.; Barbour, A.G. Neuroborreliosis during Relapsing Fever: Review of the Clinical Manifestations, Pathology, and Treatment of Infections in Humans and Experimental Animals. Clin. Infect. Dis. 1998, 26, 151–164. [Google Scholar] [CrossRef] [Green Version]
- Lim, L.L.; Rosenbaum, J.T. Borrelia hermsii Causing Relapsing Fever and Uveitis. Am. J. Ophthalmol. 2006, 142, 348–349. [Google Scholar] [CrossRef]
- Magnarelli, L.A. Serologic Diagnosis of Lyme Disease. Ann. N. Y. Acad. Sci. 1988, 539, 154–161. [Google Scholar] [CrossRef]
- Ganguly, S.; Mukhopadhayay, S.K. Tick-Borne Ehrlichiosis Infection in Human Beings. J. Vector Borne Dis. 2008, 45, 273–280. [Google Scholar]
- Stone, J.H.; Dierberg, K.; Aram, G.; Dumler, J.S. Human Monocytic Ehrlichiosis. JAMA 2004, 292, 2263–2270. [Google Scholar] [CrossRef]
- Lee, M.S.; Goslee, T.E.; Lessell, S. Ehrlichiosis Optic Neuritis. Am. J. Ophthalmol. 2003, 135, 412–413. [Google Scholar] [CrossRef]
- Carter, N.; Miller, N.R. Fourth Nerve Palsy Caused by Ehrlichia Chaffeensis. J. Neuroophthalmol. 1997, 17, 47–50. [Google Scholar] [CrossRef]
- Pendse, S.; Bilyk, J.R.; Lee, M.S. The Ticking Time Bomb. Surv. Ophthalmol. 2006, 51, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Raja, H.; Mercer, R.C.; Bakri, S.J. Presumed Posterior Uveitis Related to Ehrlichia Exposure. Retin. Cases Brief Rep. 2016, 10, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Patel, S. Rocky Mountain Spotted Fever (RMSF)—Epidemiology. Available online: https://emedicine.medscape.com/article/228042-overview#a6 (accessed on 14 July 2022).
- Salinas, L.J.; Greenfield, R.A.; Little, S.E.; Voskuhl, G.W. Tickborne Infections in the Southern United States. Am. J. Med. Sci. 2010, 340, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Demma, L.J.; Traeger, M.S.; Nicholson, W.L.; Paddock, C.D.; Blau, D.M.; Eremeeva, M.E.; Dasch, G.A.; Levin, M.L.; Singleton, J.; Zaki, S.R.; et al. Rocky Mountain Spotted Fever from an Unexpected Tick Vector in Arizona. N. Engl. J. Med. 2005, 353, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Rocky Mountain Spotted Fever—Epidemiology and Statistics. Available online: https://www.cdc.gov/rmsf/stats/index.html (accessed on 14 July 2022).
- Lange, J.V. Documented Rocky Mountain Spotted Fever in Wintertime. JAMA 1982, 247, 2403. [Google Scholar] [CrossRef]
- Walker, D.H. Rocky Mountain Spotted Fever: A Seasonal Alert. Clin. Infect. Dis. 1995, 20, 1111–1117. [Google Scholar] [CrossRef]
- Lam, B.L. Rocky Mountain Spotted Fever. Ann. Ophthalmol. 2006, 38, 3–4. [Google Scholar] [CrossRef]
- Presley, G.D. Fundus Changes in Rocky Mountain Spotted Fever. Am. J. Ophthalmol. 1969, 67, 263–267. [Google Scholar] [CrossRef]
- Smith, T.W.; Burton, T.C. The Retinal Manifestations of Rocky Mountain Spotted Fever. Am. J. Ophthalmol. 1977, 84, 259–262. [Google Scholar] [CrossRef]
- Moore, S.M.; McAllister, M.A.; Thomas, T.O. Rickettsia rickettsii Infection as an Unusual Cause of Pediatric Retinitis: A Case Report. Am. J. Ophthalmol. Case Rep. 2022, 26, 101566. [Google Scholar] [CrossRef]
- Nazarian, S.M.; Shaon, K.Y.; Schwankhaus, J.D.; Chacko, J.G.; Hudgins, P.A.; Brat, D.J. Bilateral Optic Neuropathy after Erythematous Rash. Bilateral Anterior Optic Neuropathy Due to RMSF. J. Neuroophthalmol. 2015, 35, 201–204. [Google Scholar] [CrossRef]
- Vaphiades, M.S. Rocky Mountain Spotted Fever as a Cause of Macular Star Figure. J. Neuroophthalmol. 2003, 23, 276–278. [Google Scholar] [CrossRef] [Green Version]
- Cherubini, T.D.; Spaeth, G.L. Anterior Nongranulomatous Uveitis Associated with Rocky Mountain Spotted Fever. First Report of a Case. Arch. Ophthalmol. 1969, 81, 363–365. [Google Scholar] [CrossRef]
- Rovery, C.; Raoult, D. Mediterranean Spotted Fever. Infect. Dis. Clin. N. Am. 2008, 22, 515–530. [Google Scholar] [CrossRef]
- Rovery, C.; Brouqui, P.; Raoult, D. Questions on Mediterranean Spotted Fever a Century after Its Discovery. Emerg. Infect. Dis. 2008, 14, 1360–1367. [Google Scholar] [CrossRef]
- Spernovasilis, N.; Markaki, I.; Papadakis, M.; Mazonakis, N.; Ierodiakonou, D. Mediterranean Spotted Fever: Current Knowledge and Recent Advances. Trop. Med. Infect. Dis. 2021, 6, 172. [Google Scholar] [CrossRef]
- Balasundaram, M.B.; Manjunath, M.; Baliga, G.; Kapadi, F. Ocular Manifestations of Rickettsia conorii in South India. Indian J. Ophthalmol. 2018, 66, 1840–1844. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, M.; Ladjimi, A.; Chakroun, M.; Messaoud, R.; Yahia, S.B.; Zaouali, S.; Romdhane, F.B.; Bouzouaia, N. Posterior Segment Manifestations of Rickettsia conorii Infection. Ophthalmology 2004, 111, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Abroug, N.; Khairallah-Ksiaa, I.; Kahloun, R.; Khochtali, S.; Zaouali, S.; Khairallah, M. Parinaud’s Oculoglandular Syndrome Revealing Subclinical Rickettsia conorii Infection. Int. Ophthalmol. 2015, 35, 717–719. [Google Scholar] [CrossRef] [PubMed]
- Pinna, A. Ocular Manifestations of Rickettsiosis: 1. Mediterranean Spotted Fever: Laboratory Analysis and Case Reports. Int. J. Med. Sci. 2009, 6, 126–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinna, A.; Sotgiu, M.; Carta, F.; Zanetti, S.; Fadda, G. Oculoglandular Syndrome in Mediterranean Spotted Fever Acquired through the Eye. Br. J. Ophthalmol. 1997, 81, 172. [Google Scholar] [CrossRef] [Green Version]
- Alio, J.; Ruiz-Beltran, R.; Herrera, I.; Artola, A.; Ruiz-Moreno, J.M. Rickettsial Keratitis in a Case of Mediterranean Spotted Fever. Eur. J. Ophthalmol. 1992, 2, 41–43. [Google Scholar] [CrossRef]
- Khairallah, M.; Zaouali, S.; Ben Yahia, S.; Ladjimi, A.; Messaoud, R.; Jenzeri, S.; Attia, S. Anterior Ischemic Optic Neuropathy Associated with Rickettsia conorii Infection. J. Neuroophthalmol. 2005, 25, 212–214. [Google Scholar] [CrossRef]
- Díez Ruíz, A.; Ramos Jiménez, A.; López Ruz, M.A.; Gil Extremera, B. Boutonneuse Fever Transmitted by Conjunctival Inoculation. Klin. Wochenschr. 1988, 66, 1212–1213. [Google Scholar] [CrossRef]
- Esgin, H.; Akata, F. Bilateral Multiple Retinal Hyperfluorescent Dots in a Presumed Rickettsia conorii Infection. Retina 2001, 21, 535–537. [Google Scholar] [CrossRef]
- Ng, S.K.; Simon, S.; Gilhotra, J.S. Macular Hole Following Rickettsia conorii Infection. Can. J. Ophthalmol. 2013, 48, e147–e148. [Google Scholar] [CrossRef]
- Khairallah, M.; Yahia, S.B.; Jelliti, B.; Ben Romdhane, F.; Loussaief, C.; Attia, S.; Toumi, A.; Messaoud, R.; Chakroun, M. Diagnostic Value of Ocular Examination in Mediterranean Spotted Fever. Clin. Microbiol. Infect. 2009, 15, 273–274. [Google Scholar] [CrossRef]
- Chmielewski, T.; Fiecek, B.; Lewandowska, G.; Rastawicki, W.; Tylewska-Wierzbanowska, S. Francisella tularensis/Rickettsia spp. Co-Infections in Patients with Skin Changes and Lymphadenopathy. Arch. Med. Sci. 2018, 14, 357–360. [Google Scholar] [CrossRef] [Green Version]
- Sudharshan, S.; Ganesh, S.; Biswas, J. Current Approach in the Diagnosis and Management of Posterior Uveitis. Indian J. Ophthalmol. 2010, 58, 29. [Google Scholar] [CrossRef]
- Sherman, M.D.; Nozik, R.A. Other Infections of the Choroid and Retina. Toxoplasmosis, Histoplasmosis, Lyme Disease, Syphilis, Tuberculosis, and Ocular Toxocariasis. Infect. Dis. Clin. N. Am. 1992, 6, 893–908. [Google Scholar] [CrossRef]
- Mikkilä, H.; Seppälä, I.; Leirisalo-Repo, M.; Immonen, I.; Karma, A. The Etiology of Uveitis: The Role of Infections with Special Reference to Lyme Borreliosis. Acta Ophthalmol. Scand. 1997, 75, 716–719. [Google Scholar] [CrossRef]
- Park, Y.-H.; Nam, H.-W. Clinical Features and Treatment of Ocular Toxoplasmosis. Korean J. Parasitol. 2013, 51, 393–399. [Google Scholar] [CrossRef]
- Kraushar, M.F.; Gluck, S.B.; Pass, S. Toxoplasmic Retinochoroiditis Presenting s Serous Detachment of the Macula. Ann. Ophthalmol. 1979, 11, 1513–1514. [Google Scholar]
- Eckert, G.U.; Melamed, J.; Menegaz, B. Optic Nerve Changes in Ocular Toxoplasmosis. Eye 2007, 21, 746–751. [Google Scholar] [CrossRef] [Green Version]
- Alipanahi, R.; Sayyahmelli, S. Acute Papillitis in Young Female with Toxoplasmosis. Middle East Afr. J. Ophthalmol. 2011, 18, 249. [Google Scholar] [CrossRef] [Green Version]
- Sauer, T.C.; Meyers, S.M.; Shen, D.; Vegh, S.; Vygantas, C.; Chan, C.-C. Primary Intraocular (Retinal) Lymphoma after Ocular Toxoplasmosis. Retin. Cases Brief Rep. 2010, 4, 160–163. [Google Scholar] [CrossRef]
- Nord, J.M.; Goldberg, N.R. Novel Case of Multifocal Choroiditis Following Powassan Virus Infection. Ocul. Immunol. Inflamm. 2021; Online early access. [Google Scholar] [CrossRef]
- Starolis, M.W.; Perez, O.; Powell, E.A. Clinical Features and Laboratory Diagnosis of Emerging Arthropod-Transmitted Viruses: A Report from the Pan American Society for Clinical Virology Clinical Practice Committee. J. Clin. Virol. 2020, 132, 104651. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Powassan Virus—Statistics & Maps. Available online: https://www.cdc.gov/powassan/statistics.html (accessed on 10 July 2022).
- Lessell, S.; Collins, T.E. Ophthalmoplegia in Powassan Encephalitis. Neurology 2003, 60, 1726–1727. [Google Scholar] [CrossRef]
- Voulgari, N.; Blanc, C.-M.; Guido, V.; Rossi, D.C.; Guex-Crosier, Y.; Hoogewoud, F. Tick-Borne Encephalitis Related Uveitis: A Case Report. BMC Ophthalmol. 2021, 21, 315. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Tickborne Diseases of the United States—Colorado Tick Fever. Available online: https://www.cdc.gov/ticks/tickbornediseases/ctf.html (accessed on 18 July 2022).
- Romero, J.R.; Simonsen, K.A. Powassan Encephalitis and Colorado Tick Fever. Infect. Dis. Clin. N. Am. 2008, 22, 545–559. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Yeung, L.; Sun, C.-C.; Ku, W.-C.; Yang, J.-W. Contact Dermatitis on the Lower Eyelid Related to Tick Infestation: A Case Report in Taiwan. Taiwan J. Ophthalmol. 2016, 6, 201–203. [Google Scholar] [CrossRef]
- Bowes, O.M.B.; Legg, G.; Haines, R.; Vardy, S.J. Tick Infestation of the Upper Eyelid. Can. J. Ophthalmol. 2015, 50, e39–e40. [Google Scholar] [CrossRef] [Green Version]
- Lantos, P.M.; Rumbaugh, J.; Bockenstedt, L.K.; Falck-Ytter, Y.T.; Aguero-Rosenfeld, M.E.; Auwaerter, P.G.; Baldwin, K.; Bannuru, R.R.; Belani, K.K.; Bowie, W.R.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease. Clin. Infect. Dis. 2021, 72, e1–e48. [Google Scholar] [CrossRef]
- Wormser, G.P.; Dattwyler, R.J.; Shapiro, E.D.; Halperin, J.J.; Steere, A.C.; Klempner, M.S.; Krause, P.J.; Bakken, J.S.; Strle, F.; Stanek, G.; et al. The Clinical Assessment, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2006, 43, 1089–1134. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Tickborne Diseases of the United States—Lyme Disease Prophylaxis after Tick Bite. Available online: https://www.cdc.gov/ticks/tickbornediseases/tick-bite-prophylaxis.html (accessed on 14 August 2022).
- Reibaldi, M.; Faro, S.; Motta, L.; Longo, A. Intravitreal Triamcinolone for Macular Edema in Lyme Disease. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 457–458. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Tickborne Diseases of the United States—Lyme Disease. Available online: https://www.cdc.gov/ticks/tickbornediseases/lyme.html (accessed on 20 August 2022).
- Centers for Disease Control and Prevention. Lyme Disease—Neurologic Lyme Disease. Available online: https://www.cdc.gov/lyme/treatment/NeurologicLyme.html (accessed on 1 September 2022).
- Jowett, N.; Gaudin, R.A.; Banks, C.A.; Hadlock, T.A. Steroid Use in Lyme Disease-Associated Facial Palsy Is Associated with Worse Long-Term Outcomes. Laryngoscope 2017, 127, 1451–1458. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.P.; McKenna, D.; Scavarda, C.; Karmen, C. Outcome of Facial Palsy from Lyme Disease in Prospectively Followed Patients Who Had Received Corticosteroids. Diagn. Microbiol. Infect. Dis. 2018, 91, 336–338. [Google Scholar] [CrossRef] [PubMed]
- Kalish, R.A.; Kaplan, R.F.; Taylor, E.; Jones-Woodward, L.; Workman, K.; Steere, A.C. Evaluation of Study Patients with Lyme Disease, 10-20-Year Follow-Up. J. Infect. Dis. 2001, 183, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Monco, J.C.; Villar, B.F.; Alen, J.C.; Benach, J.L. Borrelia burgdorferi in the Central Nervous System: Experimental and Clinical Evidence for Early Invasion. J. Infect. Dis. 1990, 161, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Suttorp-Schulten, M.S.; Kuiper, H.; Kijlstra, A.; van Dam, A.P.; Rothova, A. Long-Term Effects of Ceftriaxone Treatment on Intraocular Lyme Borreliosis. Am. J. Ophthalmol. 1993, 116, 571–575. [Google Scholar] [CrossRef]
- Pachner, A.R. Neurologic Manifestations of Lyme Disease, the New “Great Imitator”. Rev. Infect. Dis. 1989, 11, S1482–S1486. [Google Scholar] [CrossRef]
- Taylor, A.W.; Kaplan, H.J. Ocular Immune Privilege in the Year 2010: Ocular Immune Privilege and Uveitis. Ocul. Immunol. Inflamm. 2010, 18, 488–492. [Google Scholar] [CrossRef]
- Streilein, J.W. Ocular Immune Privilege: The Eye Takes a Dim but Practical View of Immunity and Inflammation. J. Leukoc. Biol. 2003, 74, 179–185. [Google Scholar] [CrossRef]
- Caspi, R.R. Ocular Autoimmunity: The Price of Privilege? Immunol. Rev. 2006, 213, 23–35. [Google Scholar] [CrossRef]
- Rupprecht, T.A.; Koedel, U.; Fingerle, V.; Pfister, H.-W. The Pathogenesis of Lyme Neuroborreliosis: From Infection to Inflammation. Mol. Med. 2008, 14, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Cadavid, D.; O’Neill, T.; Schaefer, H.; Pachner, A.R. Localization of Borrelia burgdorferi in the Nervous System and other Organs in a Nonhuman Primate Model of Lyme Disease. Lab. Investig. 2000, 80, 1043–1054. [Google Scholar] [CrossRef] [Green Version]
- Pachner, A.R.; Steiner, I. Lyme Neuroborreliosis: Infection, Immunity, and Inflammation. Lancet. Neurol. 2007, 6, 544–552. [Google Scholar] [CrossRef]
- Kuenzle, S.; von Büdingen, H.-C.; Meier, M.; Harrer, M.D.; Urich, E.; Becher, B.; Goebels, N. Pathogen Specificity and Autoimmunity Are Distinct Features of Antigen-Driven Immune Responses in Neuroborreliosis. Infect. Immun. 2007, 75, 3842–3847. [Google Scholar] [CrossRef] [Green Version]
- Chmielewski, T.; Brydak-Godowska, J.; Fiecek, B.; Rorot, U.; Sędrowicz, E.; Werenowska, M.; Kopacz, D.; Hevelke, A.; Michniewicz, M.; Kęcik, D.; et al. Bacterial Tick-Borne Diseases Caused by Bartonella spp., Borrelia burgdorferi Sensu Lato, Coxiella burnetii, and Rickettsia spp. among Patients with Cataract Surgery. Med. Sci. Monit. 2014, 20, 927–931. [Google Scholar] [CrossRef] [Green Version]
- Rifkin, L.M.; Vadboncoeur, J.; Minkus, C.C.; Dunn, E.N.; Moorthy, R.S.; Bhatt, N.; Sen, H.N.; Taggart, M.G.; Vitale, A.T.; Goldstein, D.A. The Utility of Lyme Testing in the Workup of Ocular Inflammation. Ocul. Immunol. Inflamm. 2021, 29, 149–153. [Google Scholar] [CrossRef]
- Bernard, A.; Kodjikian, L.; Abukhashabh, A.; Roure-Sobas, C.; Boibieux, A.; Denis, P.; Broussolle, C.; Seve, P. Diagnosis of Lyme-Associated Uveitis: Value of Serological Testing in a Tertiary Centre. Br. J. Ophthalmol. 2018, 102, 369–372. [Google Scholar] [CrossRef]
- Lim, W.-K.; Mathur, R.; Koh, A.; Yeoh, R.; Chee, S.-P. Ocular Manifestations of Dengue Fever. Ophthalmology 2004, 111, 2057–2064. [Google Scholar] [CrossRef]
- Kurane, I.; Ennis, F.E. Immunity and Immunopathology in Dengue Virus Infections. Semin. Immunol. 1992, 4, 121–127. [Google Scholar]
- Kurane, I.; Innis, B.L.; Nimmannitya, S.; Nisalak, A.; Meager, A.; Janus, J.; Ennis, F.A. Activation of T Lymphocytes in Dengue Virus Infections. High Levels of Soluble Interleukin 2 Receptor, Soluble CD4, Soluble CD8, Interleukin 2, and Interferon-Gamma in Sera of Children with Dengue. J. Clin. Investig. 1991, 88, 1473–1480. [Google Scholar] [CrossRef]
- Semenza, J.C.; Suk, J.E. Vector-Borne Diseases and Climate Change: A European Perspective. FEMS Microbiol. Lett. 2018, 365, fnx244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouchard, C.; Dibernardo, A.; Koffi, J.; Wood, H.; Leighton, P.A.; Lindsay, L.R. Increased Risk of Tick-Borne Diseases with Climate and Environmental Changes. Can. Commun. Dis. Rep. 2019, 45, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.S.; Dautel, H.; Estrada-Peña, A.; Kahl, O.; Lindgren, E. Effects of Climate Change on Ticks and Tick-Borne Diseases in Europe. Interdiscip. Perspect. Infect. Dis. 2009, 2009, 593232. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Pena, A. Tick-Borne Pathogens, Transmission Rates and Climate Change. Front. Biosci. 2009, 14, 2674. [Google Scholar] [CrossRef]
- Süss, J.; Klaus, C.; Gerstengarbe, F.; Werner, P.C. What Makes Ticks Tick? Climate Change, Ticks, and Tick-Borne Diseases. J. Travel Med. 2008, 15, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, E.; Tälleklint, L.; Polfeldt, T. Impact of Climatic Change on the Northern Latitude Limit and Population Density of the Disease-Transmitting European Tick Ixodes Ricinus. Environ. Health Perspect. 2000, 108, 119–123. [Google Scholar] [CrossRef]
- Mannelli, A.; Bertolotti, L.; Gern, L.; Gray, J. Ecology of Borrelia burgdorferi Sensu Lato in Europe: Transmission Dynamics in Multi-Host Systems, Influence of Molecular Processes and Effects of Climate Change. FEMS Microbiol. Rev. 2012, 36, 837–861. [Google Scholar] [CrossRef] [Green Version]
- Johnson, N.; Paul Phipps, L.; McFadzean, H.; Barlow, A.M. An Outbreak of Bovine Babesiosis in February 2019, Triggered by above Average Winter Temperatures in Southern England and Co-Infection with Babesia Divergens and Anaplasma Phagocytophilum. Parasites Vectors 2020, 13, 305. [Google Scholar] [CrossRef]
- Tälleklint, L.; Jaenson, T.G. Increasing Geographical Distribution and Density of Ixodes Ricinus (Acari: Ixodidae) in Central and Northern Sweden. J. Med. Entomol. 1998, 35, 521–526. [Google Scholar] [CrossRef]
- Zając, Z.; Kulisz, J.; Woźniak, A.; Bartosik, K.; Khan, A. Seasonal Activity of Dermacentor Reticulatus Ticks in the Era of Progressive Climate Change in Eastern Poland. Sci. Rep. 2021, 11, 20382. [Google Scholar] [CrossRef]
- Gillingham, E.L.; Cull, B.; Pietzsch, M.E.; Phipps, L.P.; Medlock, J.M.; Hansford, K. The Unexpected Holiday Souvenir: The Public Health Risk to UK Travellers from Ticks Acquired Overseas. Int. J. Environ. Res. Public Health 2020, 17, 7957. [Google Scholar] [CrossRef]
- Jensenius, M.; Parola, P.; Raoult, D. Threats to International Travellers Posed by Tick-Borne Diseases. Travel Med. Infect. Dis. 2006, 4, 4–13. [Google Scholar] [CrossRef]
- Jensenius, M.; Fournier, P.-E.; Raoult, D. Tick-Borne Rickettsioses in International Travellers. Int. J. Infect. Dis. 2004, 8, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Mikkilä, H.; Karma, A.; Viljanen, M.; Seppälä, I. The Laboratory Diagnosis of Ocular Lyme Borreliosis. Graefes Arch. Clin. Exp. Ophthalmol. 1999, 237, 225–230. [Google Scholar] [CrossRef]
- Caplash, S.; Gangaputra, S.; Kesav, N.; Akanda, M.; Vitale, S.; Kodati, S.; Marques, A.; Sen, H.N. Usefulness of Routine Lyme Screening in Patients with Uveitis. Ophthalmology 2019, 126, 1726–1728. [Google Scholar] [CrossRef]
- Hunt, L. Ocular Lyme Disease. Insight J. Am. Soc. Ophthalmic Regist. Nurses 1996, 21, 56–57. [Google Scholar] [CrossRef]
- Kazi, H.; de Groot-Mijnes, J.D.F.; Ten Dam-van Loon, N.H.; Ossewaarde-van Norel, J.; Oosterheert, J.J.; de Boer, J.H. No Value for Routine Serologic Screening for Borrelia burgdorferi in Patients with Uveitis in the Netherlands. Am. J. Ophthalmol. 2016, 166, 189–193. [Google Scholar] [CrossRef]
- Rothova, A.; Suttorp-Van Schulten, M.S. Diagnosis and Clinical Characteristics of Ocular Lyme Borreliosis. Am. J. Ophthalmol. 1995, 120, 263–264. [Google Scholar] [CrossRef]
- Mikkilä, H.; Seppälä, I.; Leirisalo-Repo, M.; Karma, A. The Significance of Serum Anti-Borrelia Antibodies in the Diagnostic Work-up of Uveitis. Eur. J. Ophthalmol. 1997, 7, 251–255. [Google Scholar] [CrossRef]
- Maraspin, V.; Lotric-Furlan, S.; Cimperman, J.; Ruzić-Sabljić, E.; Strle, F. Erythema Migrans in the Immunocompromised Host. Wien. Klin. Wochenschr. 1999, 111, 923–932. [Google Scholar]
- Eiferman, V.; Guenno, G.L.; Boiret-Dupré, N.; Barres, B.; Luciani, L.; Fournier, P.E. Atypical Borrelia garinii Infection in an Immunocompromised Patient Mimicking High-Grade Lymphoma. Int. J. Infect. Dis. 2022, 121, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Mrzljak, A.; Novak, R.; Pandak, N.; Tabain, I.; Franusic, L.; Barbic, L.; Bogdanic, M.; Savic, V.; Mikulic, D.; Pavicic-Saric, J.; et al. Emerging and Neglected Zoonoses in Transplant Population. World J. Transplant. 2020, 10, 47–63. [Google Scholar] [CrossRef] [PubMed]
- Nathavitharana, R.R.; Mitty, J.A. Diseases from North America: Focus on Tick-Borne Infections. Clin. Med. 2015, 15, 74–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowen, L.; Nath, A.; Smith, B. CNS Immune Reconstitution Inflammatory Syndrome. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 152, pp. 167–176. [Google Scholar] [CrossRef]
- Walker, N.F.; Scriven, J.; Meintjes, G.; Wilkinson, R.J. Immune Reconstitution Inflammatory Syndrome in HIV-Infected Patients. HIV AIDS 2015, 7, 49–64. [Google Scholar] [CrossRef]
- Müller, M.; Wandel, S.; Colebunders, R.; Attia, S.; Furrer, H.; Egger, M. Immune Reconstitution Inflammatory Syndrome in Patients Starting Antiretroviral Therapy for HIV Infection: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2010, 10, 251–261. [Google Scholar] [CrossRef] [Green Version]
- Rb-Silva, R.; Nobrega, C.; Reiriz, E.; Almeida, S.; Sarmento-Castro, R.; Correia-Neves, M.; Horta, A. Toxoplasmosis-Associated IRIS Involving the CNS: A Case Report with Longitudinal Analysis of T Cell Subsets. BMC Infect. Dis. 2017, 17, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahani, L.; Hamill, R.J. Therapeutics Targeting Inflammation in the Immune Reconstitution Inflammatory Syndrome. Transl. Res. 2016, 167, 88–103. [Google Scholar] [CrossRef] [PubMed]
- Tremont-Lukats, I.W.; Garciarena, P.; Juarbe, R.; El-Abassi, R.N. The Immune Inflammatory Reconstitution Syndrome and Central Nervous System Toxoplasmosis. Ann. Intern. Med. 2009, 150, 656–657. [Google Scholar] [CrossRef] [Green Version]
- Dinardo, A.R.; Lewis, D.S.; Koo, H.L.; Goodman, J.C.; Chiao, E.; Andrade, R. Paradoxical Immune Reconstitution Inflammatory Syndrome Due to Toxoplasmic Encephalitis: Two Cases and Review of Initiation of Antiretroviral Timing in Toxoplasmic Encephalitis IRIS. F1000Res 2013, 2, 133. [Google Scholar] [CrossRef]
- Kung, D.H.; Hubenthal, E.A.; Kwan, J.Y.; Shelburne, S.A.; Goodman, J.C.; Kass, J.S. Toxoplasmosis Myelopathy and Myopathy in an AIDS Patient: A Case of Immune Reconstitution Inflammatory Syndrome? Neurologist 2011, 17, 49–51. [Google Scholar] [CrossRef]
- Cabral, R.F.; Valle Bahia, P.R.; Gasparetto, E.L.; Chimelli, L. Immune Reconstitution Inflammatory Syndrome and Cerebral Toxoplasmosis. AJNR Am. J. Neuroradiol. 2010, 31, E65–E66. [Google Scholar] [CrossRef] [Green Version]
- Johnson, T.; Nath, A. Immune Reconstitution Inflammatory Syndrome and the Central Nervous System. Curr. Opin. Neurol. 2011, 24, 284–290. [Google Scholar] [CrossRef]
- Chang, C.C.; Sheikh, V.; Sereti, I.; French, M.A. Immune Reconstitution Disorders in Patients with HIV Infection: From Pathogenesis to Prevention and Treatment. Curr. HIV/AIDS Rep. 2014, 11, 223–232. [Google Scholar] [CrossRef]
- Dhakal, A.; Sbar, E. Jarisch Herxheimer Reaction in StatPearls; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Negussie, Y.; Remick, D.G.; DeForge, L.E.; Kunkel, S.L.; Eynon, A.; Griffin, G.E. Detection of Plasma Tumor Necrosis Factor, Interleukins 6, and 8 during the Jarisch-Herxheimer Reaction of Relapsing Fever. J. Exp. Med. 1992, 175, 1207–1212. [Google Scholar] [CrossRef]
- Guerrier, G.; Doherty, T. Comparison of Antibiotic Regimens for Treating Louse-Borne Relapsing Fever: A Meta-Analysis. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 483–490. [Google Scholar] [CrossRef]
- Khurana, S.; Dubey, M.L.; Malla, N. Association of Parasitic Infections and Cancers. Indian J. Med. Microbiol. 2005, 23, 74–79. [Google Scholar] [CrossRef]
- Biernat, M.M.; Wróbel, T. Bacterial Infection and Non-Hodgkin B-Cell Lymphoma: Interactions between Pathogen, Host and the Tumor Environment. Int. J. Mol. Sci. 2021, 22, 7372. [Google Scholar] [CrossRef]
- Ribeiro, D.A.; Pereira, P.C.M.; Machado, J.M.; Silva, S.B.; Pessoa, A.W.P.; Salvadori, D.M.F. Does Toxoplasmosis Cause DNA Damage? An Evaluation in Isogenic Mice under Normal Diet or Dietary Restriction. Mutat. Res. 2004, 559, 169–176. [Google Scholar] [CrossRef]
- Grimwood, J.; Mineo, J.R.; Kasper, L.H. Attachment of Toxoplasma Gondii to Host Cells Is Host Cell Cycle Dependent. Infect. Immun. 1996, 64, 4099–4104. [Google Scholar] [CrossRef] [Green Version]
- Coppens, I.; Joiner, K.A. Host but Not Parasite Cholesterol Controls Toxoplasma Cell Entry by Modulating Organelle Discharge. Mol. Biol. Cell. 2003, 14, 3804–3820. [Google Scholar] [CrossRef] [Green Version]
- Shinitzky, M.; Inbar, M. Difference in Microviscosity Induced by Different Cholesterol Levels in the Surface Membrane Lipid Layer of Normal Lymphocytes and Malignant Lymphoma Cells. J. Mol. Biol. 1974, 85, 603–615. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Disease | Aetiological Organism | Transmission |
|---|---|---|
| Borreliosis | Borrelia burgdorferi sensu lato | Several tick species of the genus Ixodes. |
| Tularaemia | Francisella tularensis | Ticks of the species Dermacentor variabilis (Say), Dermacentor andersoni (Stiles), Amblyomma americanum (Linnaeus) |
| Babesiosis | Intraerythrocytic protozoa of the order Piroplasmida, family Babesiidae and genus Babesia | Ixodes scapularis |
| Ehrlichiosis | Intracellular Gram-negative bacteria of genus Ehrlichia | Amblyomma americanum and Dermacentor variabilis |
| Rickettsiosis | Obligate intracellular bacteria groups of the genus Rickettsia Orientia tsutsugamushi | Various tick species |
| Toxoplasmosis | Toxoplasma gondii | Tick species of the genera Ixodes, Dermacentor, Amblyomma |
| Tick-borne Encephalitis | Tick-borne encephalitis virus, a member of the Flaviviridae family | Tick species of the genus Ixodes |
| Powassan Encephalitis | Powassan virus, a member of the Flaviviridae family | Tick species of the genus Ixodes |
| Colorado Tick Fever | Coltivirus, a member of the Reoviridae family | Tick species of the genus Dermacentor |
| Tick-borne Relapsing Fever | Bacteria species of the genus Borrelia | Tick species of the genus Ornithodoros |
| Anatomical Involvement | Tick Species | Ocular Manifestation |
|---|---|---|
| External ocular and adnexal involvement | I. nipponensis I. scapularis D. variabilis D. andersoni R. sanguineus A. americanum | Eyelid ulceration, eyelid inflammation (acute or chronic), eyelid oedema, painful eyelid nodule ± mucopurulent discharge, palpebral ptosis, erythema migrans on lids and periocular adnexae, palpebral oedema, blepharospasm, orbit periostitis, periorbital oedema, orbital myositis (medial rectus, inferior rectus, lateral rectus) associated with lacrimal gland enlargement, dacryoadenitis, dacryocystitis, periorbital ecchymosis, conjunctival follicles with mucous discharge |
| Anterior segment | I. ricinus I. persulcatus I. scapularis I. pacificus D. variabilis D. andersoni D. reticulatus, and H. longicornis R. sanguineus A. americanum A. cajennense complex, mainly A. sculptum O. hermsi O. parkeri O. turicata O. moubata | Non-granulomatous anterior uveitis, conjunctival injection, conjunctival papule, conjunctival ulcer, conjunctival nodule, conjunctival hyperaemia, corneal precipitates, corneal thinning and vascularisation, cells and flare of anterior chamber, follicular conjunctivitis, symblepharon, subconjunctival haemorrhages, episcleritis, scleritis, keratitis (exposure, interstitial, peripheral ulcerative, stromal), Cogan’s syndrome, Horner’s syndrome, Argyll-Robertson pupil, afferent pupillary defect, tonic pupils, iritis, cyclitis (acute and chronic), iridocyclitis, uveitis (anterior, intermediate, posterior, panuveitis—granulomatous, associated with anterior synechiae), posterior synechiae, pars planitis, cataract formation, secondary glaucoma, band keratopathy, corneal ulcers (ameboid-type), ciliary injection, corneal oedema, corneal inflammatory infiltrates, mild infiltration of the anterior stroma, endophthalmitis, conjunctival chemosis, hypopyon, conjunctival vasculitis |
| Posterior segment | I. ricinus I. persulcatus I. scapularis I. cookei I. marxi I. spinipalpis D. variabilis D. andersoni D. reticulatus R. sanguineus A. americanum A. cajennense complex, mainly A. sculptum O. moubata H. longicornis | Haemorrhages (intraretinal, disc with venous engorgement, white-centred retinal, subretinal, flame-shaped), vitritis, vitreous haze and cells, focal retinitis with surrounding retinal and macular pigmentary changes, multifocal retinitis, cells and flare of vitreous cells, retinal vasculitis, posterior uveitis (focal retinochoroiditis), serous macular detachment, retinal detachment, choroiditis (chorioretinitis, multifocal choroiditis, Birdshot chorioretinopathy, acute posterior multifocal placoid pigment epitheliopathy), inflammatory choroidal neovascular membrane, vitritis (anterior ‘spiderweb’ vitritis without retinal involvement), vitreous clouding, atypical Eales disease syndromes, exudative retinal detachments, branch retinal artery occlusion with cotton wool spots, branch retinal vein occlusion, chorioretinal horseshoe-shaped retinal tear with inflammatory nodules on the flap, chorioretinal inflammatory foci, secondary retinitis pigmentosa, pigment epitheliitis, macular star, macular oedema, secondary glaucoma, full thickness macular hole, peripapillary retinal pigment epithelium detachments, big blind spot syndrome, optic disc staining, juxtavascular white retinal lesions, focal vascular sheathing, multiple arterial plaques, retinal vascular leakage, delayed filling in a branch retinal vein, multiple hypofluorescent choroidal dots, endophthalmitis, retinal nerve fibre layer infarct, retinal oedema, venous tortuosity, choroidal vasculitis, epiretinal membrane |
| Optic neuropathy | I. cookei I. marxi I. spinipalpis I. scapularis I. ricinus D. variabilis D. andersoni D. reticulatus R. sanguineus A. americanum A. cajennense complex, mainly A. sculptum O. hermsi O. parkeri O. turicata O. moubata H. longicornis | Neuroretinitis, papillitis (optic neuritis), optic atrophy secondary to optic nerve involvement, cranial nerve palsies (CN 3, 4, 6, 7), paralytic strabismus, acute anterior ischaemic optic neuropathy, optic perineuritis, papilloedema, optic nerve sheath contrast enhancement, disc oedema, optic nerve oedema |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, X.L.; Lau, B.Y.Y.; Chan, C.X.C.; Lim, D.K.A.; Lim, B.X.H.; Lim, C.H.L. Revenge of the Tick: Tick-Borne Diseases and the Eye in the Age of Climate Change and Globalisation. Zoonotic Dis. 2022, 2, 183-227. https://doi.org/10.3390/zoonoticdis2040017
Ng XL, Lau BYY, Chan CXC, Lim DKA, Lim BXH, Lim CHL. Revenge of the Tick: Tick-Borne Diseases and the Eye in the Age of Climate Change and Globalisation. Zoonotic Diseases. 2022; 2(4):183-227. https://doi.org/10.3390/zoonoticdis2040017
Chicago/Turabian StyleNg, Xin Le, Berdjette Y. Y. Lau, Cassandra X. C. Chan, Dawn K. A. Lim, Blanche X. H. Lim, and Chris H. L. Lim. 2022. "Revenge of the Tick: Tick-Borne Diseases and the Eye in the Age of Climate Change and Globalisation" Zoonotic Diseases 2, no. 4: 183-227. https://doi.org/10.3390/zoonoticdis2040017