
Etiology of Clinical Community-Acquired Pneumonia in Swedish Children Aged 1–59 Months with High Pneumococcal Vaccine Coverage—The TREND Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Setting
2.2. Sampling and Microbiological Analyses
2.3. Study Variables
2.4. Statistical Methods
2.5. Ethics
3. Results
3.1. Sociodemographic Characteristics
3.2. Symptoms and Signs
3.3. Management and Treatment
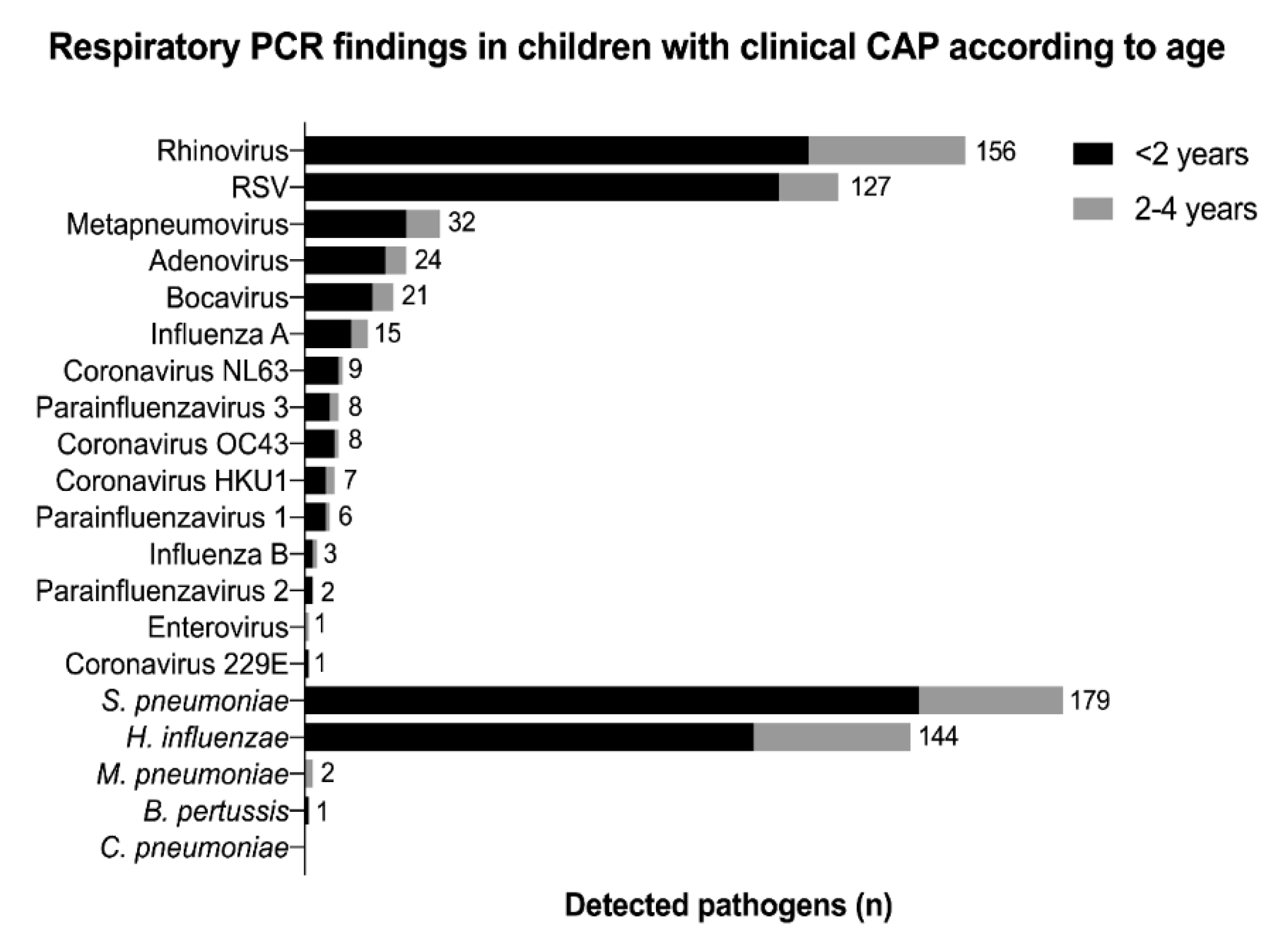
3.4. Microbiological Findings
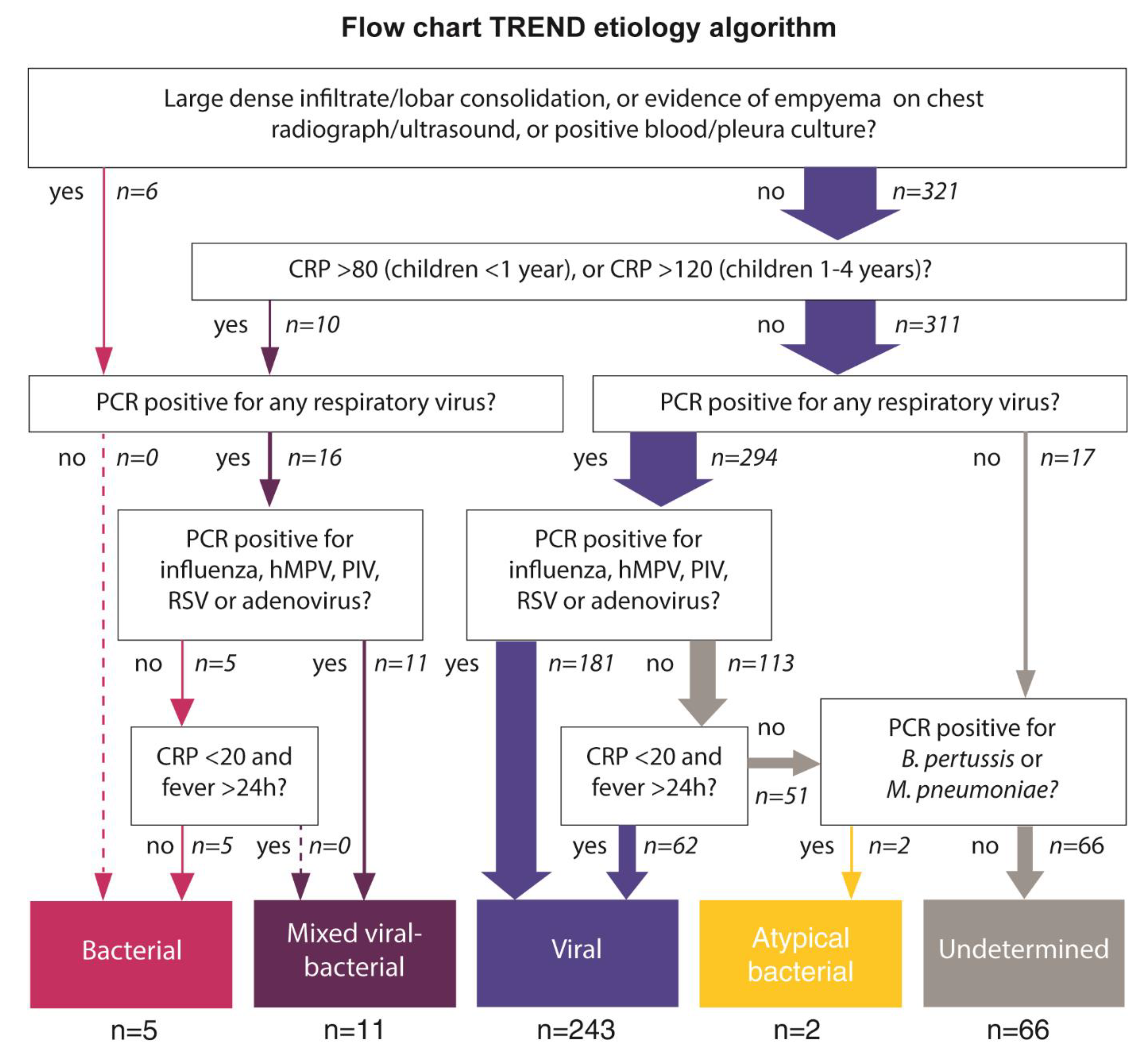
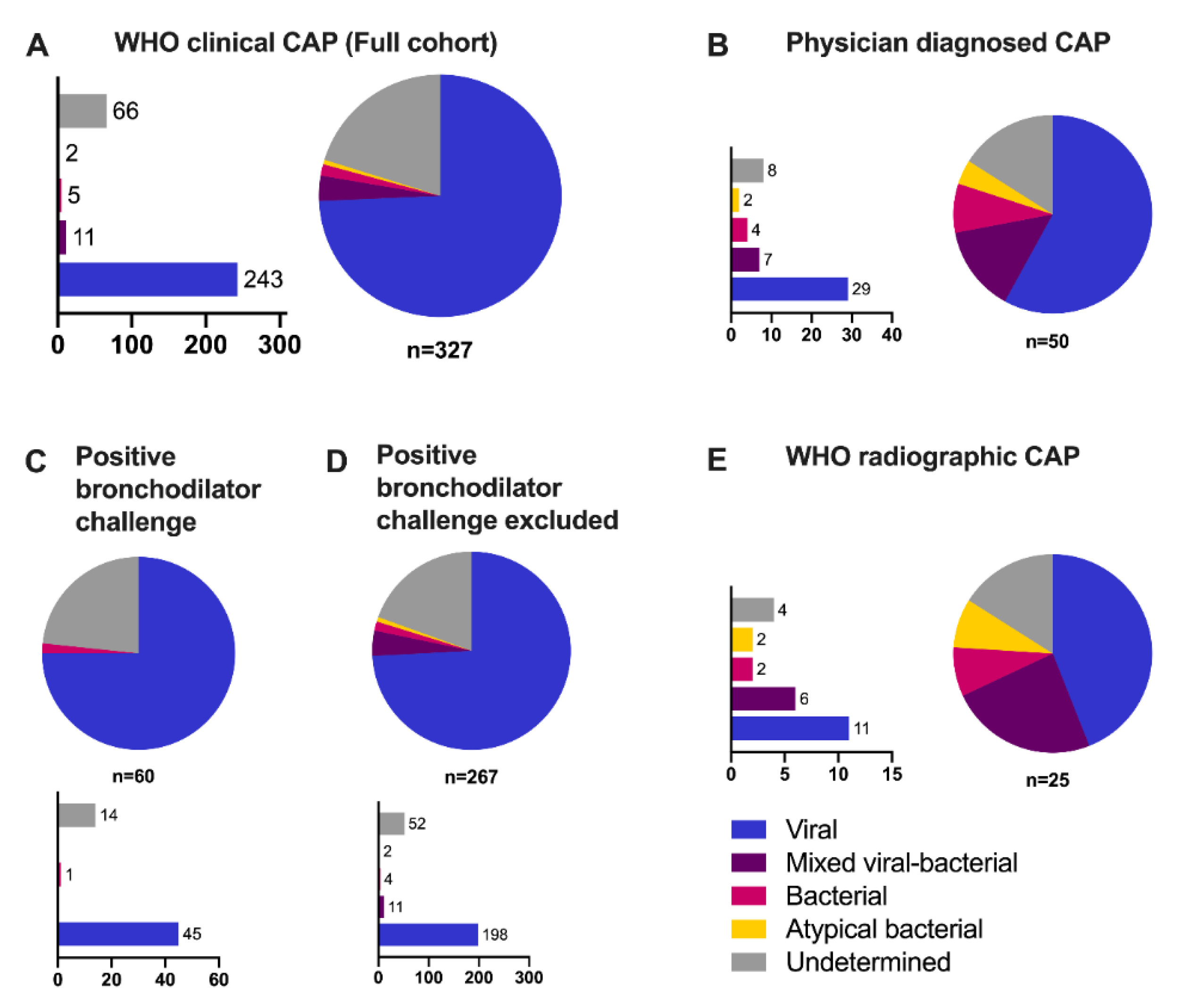
3.5. Etiological Classification
3.6. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lindstrand, A.; Bennet, R.; Galanis, I.; Blennow, M.; Ask, L.S.; Dennison, S.H.; Rinder, M.R.; Eriksson, M.; Henriques-Normark, B.; Ortqvist, A.; et al. Sinusitis and pneumonia hospitalization after introduction of pneumococcal conjugate vaccine. Pediatrics 2014, 134, e1528–e1536. [Google Scholar] [CrossRef] [Green Version]
- Wahl, B.; O’Brien, K.L.; Greenbaum, A.; Majumder, A.; Liu, L.; Chu, Y.; Lukšić, I.; Nair, H.; McAllister, D.A.; Campbell, H.; et al. Burden of streptococcus pneumoniae and haemophilus influenzae type b disease in children in the era of conjugate vaccines: Global, regional, and national estimates for 2000-15. Lancet Glob. Health 2018, 6, e744–e757. [Google Scholar] [CrossRef] [Green Version]
- Rhedin, S.; Lindstrand, A.; Hjelmgren, A.; Ryd-Rinder, M.; Ohrmalm, L.; Tolfvenstam, T.; Ortqvist, A.; Rotzen-Ostlund, M.; Zweygberg-Wirgart, B.; Henriques-Normark, B.; et al. Respiratory viruses associated with community-acquired pneumonia in children: Matched case-control study. Thorax 2015, 70, 847–853. [Google Scholar] [CrossRef] [Green Version]
- Zar, H.J.; Barnett, W.; Stadler, A.; Gardner-Lubbe, S.; Myer, L.; Nicol, M.P. Aetiology of childhood pneumonia in a well vaccinated south african birth cohort: A nested case-control study of the drakenstein child health study. Lancet. Respir. Med. 2016, 4, 463–472. [Google Scholar] [CrossRef] [Green Version]
- Causes of severe pneumonia requiring hospital admission in children without hiv infection from africa and asia: The perch multi-country case-control study. Lancet 2019, 394, 757–779. [CrossRef] [Green Version]
- Jain, S.; Williams, D.J.; Arnold, S.R.; Ampofo, K.; Bramley, A.M.; Reed, C.; Stockmann, C.; Anderson, E.J.; Grijalva, C.G.; Self, W.H.; et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N. Engl. J. Med. 2015, 372, 835–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhedin, S. Establishment of childhood pneumonia cause in the era of pneumococcal conjugate vaccines. Lancet. Respir. Med. 2016, 4, 423–424. [Google Scholar] [CrossRef]
- Deloria Knoll, M.; Fu, W.; Shi, Q.; Prosperi, C.; Wu, Z.; Hammitt, L.L.; Feikin, D.R.; Baggett, H.C.; Howie, S.R.C.; Scott, J.A.G.; et al. Bayesian estimation of pneumonia etiology: Epidemiologic considerations and applications to the pneumonia etiology research for child health study. Clin. Infect. Dis. 2017, 64, S213–s227. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.A.; Wonodi, C.; Moisi, J.C.; Deloria-Knoll, M.; DeLuca, A.N.; Karron, R.A.; Bhat, N.; Murdoch, D.R.; Crawley, J.; Levine, O.S.; et al. The definition of pneumonia, the assessment of severity, and clinical standardization in the pneumonia etiology research for child health study. Clin. Infect. Dis. 2012, 54, S109–S116. [Google Scholar] [CrossRef]
- Bénet, T.; Sánchez Picot, V.; Messaoudi, M.; Chou, M.; Eap, T.; Wang, J.; Shen, K.; Pape, J.W.; Rouzier, V.; Awasthi, S.; et al. Microorganisms associated with pneumonia in children <5 years of age in developing and emerging countries: The gabriel pneumonia multicenter, prospective, case-control study. Clin. Infect. Dis. 2017, 65, 604–612. [Google Scholar] [PubMed] [Green Version]
- Elemraid, M.A.; Sails, A.D.; Eltringham, G.J.; Perry, J.D.; Rushton, S.P.; Spencer, D.A.; Thomas, M.F.; Eastham, K.M.; Hampton, F.; Gennery, A.R.; et al. Aetiology of paediatric pneumonia after the introduction of pneumococcal conjugate vaccine. Eur. Respir. J. 2013, 42, 1595–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, A.S.; Inchley, C.S.; Aase, A.; Fjaerli, H.O.; Bull, R.; Aaberge, I.; Leegaard, T.M.; Nakstad, B. Etiology of pneumonia in a pediatric population with high pneumococcal vaccine coverage: A prospective study. Pediatr. Infect. Dis. J. 2016, 35, e69–e75. [Google Scholar] [CrossRef]
- de Steenhuijsen Piters, W.A.; Heinonen, S.; Hasrat, R.; Bunsow, E.; Smith, B.; Suarez-Arrabal, M.C.; Chaussabel, D.; Cohen, D.M.; Sanders, E.A.; Ramilo, O.; et al. Nasopharyngeal microbiota, host transcriptome, and disease severity in children with respiratory syncytial virus infection. Am. J. Respir. Crit. Care Med. 2016, 194, 1104–1115. [Google Scholar] [CrossRef] [PubMed]
- Fathima, P.; Blyth, C.C.; Lehmann, D.; Lim, F.J.; Abdalla, T.; de Klerk, N.; Moore, H.C. The impact of pneumococcal vaccination on bacterial and viral pneumonia in western australian children: Record linkage cohort study of 469589 births, 1996-2012. Clin. Infect. Dis. 2018, 66, 1075–1085. [Google Scholar] [CrossRef]
- WHO. Who Vaccine-Preventable Diseases: Monitoring System. 2020 Global Summary. Available online: https://apps.who.int/immunization_monitoring/globalsummary/countries?countrycriteria%5Bcountry%5D%5B%5D=SWE (accessed on 9 February 2021).
- Rambaud-Althaus, C.; Althaus, F.; Genton, B.; D’Acremont, V. Clinical features for diagnosis of pneumonia in children younger than 5 years: A systematic review and meta-analysis. Lancet Infect. Dis. 2015, 15, 439–450. [Google Scholar] [CrossRef]
- Wingerter, S.L.; Bachur, R.G.; Monuteaux, M.C.; Neuman, M.I. Application of the world health organization criteria to predict radiographic pneumonia in a us-based pediatric emergency department. Pediatr. Infect. Dis. J. 2012, 31, 561–564. [Google Scholar] [CrossRef]
- Rhedin, S.A.; Eklundh, A.; Ryd-Rinder, M.; Naucler, P.; Mårtensson, A.; Gantelius, J.; Zenk, I.; Andersson-Svahn, H.; Nybond, S.; Rasti, R.; et al. Introducing a new algorithm for classification of etiology in studies on pediatric pneumonia: Protocol for the trial of respiratory infections in children for enhanced diagnostics study. JMIR Res. Protoc. 2019, 8, e12705. [Google Scholar] [CrossRef]
- Andersson, M.E.; Olofsson, S.; Lindh, M. Comparison of the filmarray assay and in-house real-time pcr for detection of respiratory infection. Scand. J. Infect. Dis. 2014, 46, 897–901. [Google Scholar] [CrossRef]
- Rhedin, S.; Hamrin, J.; Naucler, P.; Bennet, R.; Rotzén-Östlund, M.; Färnert, A.; Eriksson, M. Respiratory viruses in hospitalized children with influenza-like illness during the h1n1 2009 pandemic in Sweden [corrected]. PLoS ONE 2012, 7, e51491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherian, T.; Mulholland, E.K.; Carlin, J.B.; Ostensen, H.; Amin, R.; de Campo, M.; Greenberg, D.; Lagos, R.; Lucero, M.; Madhi, S.A.; et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull. World Health Organ. 2005, 83, 353–359. [Google Scholar] [PubMed]
- Rhedin, S.; Lindstrand, A.; Rotzen-Ostlund, M.; Tolfvenstam, T.; Ohrmalm, L.; Rinder, M.R.; Zweygberg-Wirgart, B.; Ortqvist, A.; Henriques-Normark, B.; Broliden, K.; et al. Clinical utility of pcr for common viruses in acute respiratory illness. Pediatrics 2014, 133, e538–e545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herberg, J.A.; Kaforou, M.; Wright, V.J.; Shailes, H.; Eleftherohorinou, H.; Hoggart, C.J.; Cebey-López, M.; Carter, M.J.; Janes, V.A.; Gormley, S.; et al. Diagnostic test accuracy of a 2-transcript host rna signature for discriminating bacterial vs viral infection in febrile children. JAMA 2016, 316, 835–845. [Google Scholar] [CrossRef] [Green Version]
- Chochua, S.; D’Acremont, V.; Hanke, C.; Alfa, D.; Shak, J.; Kilowoko, M.; Kyungu, E.; Kaiser, L.; Genton, B.; Klugman, K.P.; et al. Increased nasopharyngeal density and concurrent carriage of streptococcus pneumoniae, haemophilus influenzae, and moraxella catarrhalis are associated with pneumonia in febrile children. PloS ONE 2016, 11, e0167725. [Google Scholar] [CrossRef] [Green Version]
- Lewnard, J.A.; Huppert, A.; Givon-Lavi, N.; Pettigrew, M.M.; Regev-Yochay, G.; Dagan, R.; Weinberger, D.M. Density, serotype diversity, and fitness of streptococcus pneumoniae in upper respiratory tract cocolonization with nontypeable haemophilus influenzae. J. Infect. Dis. 2016, 214, 1411–1420. [Google Scholar] [CrossRef] [Green Version]
- Karppinen, S.; Toivonen, L.; Schuez-Havupalo, L.; Teros-Jaakkola, T.; Waris, M.; Auranen, K.; Palmu, A.A.; Peltola, V. Effectiveness of the ten-valent pneumococcal haemophilus influenzae protein d conjugate vaccine (phid-cv10) against all respiratory tract infections in children under two years of age. Vaccine 2019, 37, 2935–2941. [Google Scholar] [CrossRef] [PubMed]
- Karppinen, S.; Teräsjärvi, J.; Auranen, K.; Schuez-Havupalo, L.; Siira, L.; He, Q.; Waris, M.; Peltola, V. Acquisition and transmission of streptococcus pneumoniae are facilitated during rhinovirus infection in families with children. Am. J. Respir. Crit. Care Med. 2017, 196, 1172–1180. [Google Scholar] [CrossRef]
- Keitel, K.; Kagoro, F.; Samaka, J.; Masimba, J.; Said, Z.; Temba, H.; Mlaganile, T.; Sangu, W.; Rambaud-Althaus, C.; Gervaix, A.; et al. A novel electronic algorithm using host biomarker point-of-care tests for the management of febrile illnesses in tanzanian children (e-poct): A randomized, controlled non-inferiority trial. PloS Med. 2017, 14, e1002411. [Google Scholar] [CrossRef] [PubMed]
- Jehan, F.; Nisar, I.; Kerai, S.; Balouch, B.; Brown, N.; Rahman, N.; Rizvi, A.; Shafiq, Y.; Zaidi, A.K.M. Randomized trial of amoxicillin for pneumonia in pakistan. N. Engl. J. Med. 2020, 383, 24–34. [Google Scholar] [CrossRef]
- Elfving, K.; Shakely, D.; Andersson, M.; Baltzell, K.; Ali, A.S.; Bachelard, M.; Falk, K.I.; Ljung, A.; Msellem, M.I.; Omar, R.S.; et al. Acute uncomplicated febrile illness in children aged 2–59 months in Zanzibar—Aetiologies, antibiotic treatment and outcome. PLoS ONE 2016, 11, e0146054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginsburg, A.S.; Mvalo, T.; Nkwopara, E.; McCollum, E.D.; Ndamala, C.B.; Schmicker, R.; Phiri, A.; Lufesi, N.; Izadnegahdar, R.; May, S. Placebo vs amoxicillin for nonsevere fast-breathing pneumonia in malawian children aged 2 to 59 months: A double-blind, randomized clinical noninferiority trial. JAMA Pediatr. 2019, 173, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Lindstrand, A.; Galanis, I.; Darenberg, J.; Morfeldt, E.; Naucler, P.; Blennow, M.; Alfvén, T.; Henriques-Normark, B.; Örtqvist, Å. Unaltered pneumococcal carriage prevalence due to expansion of non-vaccine types of low invasive potential 8years after vaccine introduction in stockholm, sweden. Vaccine 2016, 34, 4565–4571. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Viral Etiology (n = 243) | Bacterial/ Mixed Viral-Bacterial/ Atypical Etiology (n = 18) | Undetermined (n = 66) | All (n = 327) | p-Value |
|---|---|---|---|---|---|
| Characteristics | |||||
| Age (months), median IQR | 11 (4–18) | 17 (8–26) | 20 (9–26) | 13 (5–22) | <0.01 |
| 1–11 months | 126 (52) | 7 (39) | 20 (30) | 153 (47) | |
| 12–59 months | 117 (48) | 11 (61) | 46 (70) | 174 (53) | |
| Male sex | 149 (61) | 8 (44) | 43 (65) | 200 (61) | |
| Attending daycare | 92 (38) | 10 (59) | 33 (52) | 135 (42) | 0.058 |
| Breastfeeding | 83 (35) | 5 (28) | 18 (28) | 106 (33) | 0.503 |
| Parental smoking | 36 (15) | 1 (6) | 8 (12) | 45 (14) | 0.496 |
| Fully immunized a | 238 (99) | 17 (94) | 65 (100) | 320 (99) | 0.23 |
| Chronic disease | 73 (31) | 6 (35) | 28 (45) | 107 (34) | 0.236 |
| Asthma/wheezing | 61 (26) | 5 (29) | 25 (40) | 91 (29) | |
| Otherb | 12 (5) | 1 (6) | 3 (5) | 16 (5) | |
| University studies ≥1 parent | 176 (72) | 16 (89) | 55 (83) | 247 (76) | 0.075 |
| Clinical presentation | |||||
| Tachypnea c | 213 (88) | 16 (89) | 62 (94) | 291 (89) | 0.394 |
| Chest indrawings | 204 (84) | 12 (67) | 56 (85) | 272 (83) | 0.182 |
| Positive bronchodilator challenge d | 45 (19) | 1 (6) | 14 (21) | 60 (18) | 0.312 |
| Cough | 236 (98) | 17 (100) | 60 (97) | 313 (98) | 0.752 |
| Breathing troubles | 166 (79) | 11 (69) | 45 (83) | 222 (79) | 0.441 |
| Fever, ≥38° C | 103 (42) | 14 (78) | 21 (32) | 138 (42) | 0.002 |
| History of fever | 184 (80) | 18 (100) | 45 (78) | 247 (80) | 0.066 |
| Rhonchi/wheezing | 132 (55) | 3 (17) | 38 (58) | 173 (54) | 0.005 |
| Peripheral oxygen saturation <90% | 11 (5) | 6 (33) | 8 (13) | 25 (8) | <0.001 |
| Nasal flaring | 23 (10) | 1 (6) | 7 (11) | 31 (10) | 0.802 |
| Grunting | 14 (6) | 2 (11) | 6 (9) | 22 (7) | 0.512 |
| CRP mg/L median (IQR) | 9 (0–24) | 124,5 (97–165) | 22 (10–40) | 13 (0–33) | NA |
| CRP <20 mg/L | 67 (28) | 16 (89) | 41 (62) | 124 (38) | NA |
| CRP >60mg/L | 18 (7) | 14 (78) | 6 (9) | 38 (12) | NA |
| CRP >80mg/L | 10 (4) | 14 (78) | 4 (6) | 28 (9) | NA |
| Management/Treatment | Viral Etiology (n = 243) | Bacterial/ Mixed Viral-Bacterial/ Atypical Etiology (n = 18) | Undetermined (n = 66) | All (n = 327) | p-Value a |
|---|---|---|---|---|---|
| Antibiotics | 60 (25) | 15 (83) | 16 (24) | 91 (28) | <0.001 |
| Oral corticosteroids | 60 (25) | 2 (12) | 24 (36) | 86 (26) | 0.06 |
| Inhalation treatment | 213 (88) | 12 (67) | 58 (88) | 283 (87) | 0.039 |
| Intravenous fluid | 14 (6) | 7 (39) | 8 (12) | 29 (9) | <0.001 |
| Nasogastric tube | 20 (8) | 3 (17) | 4 (6) | 27 (8) | 0.317 |
| Oxygen treatment | 30 (12) | 5 (28) | 13 (20) | 48 (15) | 0.091 |
| High-flow nasal cannula | 21 (9) | 2 (11) | 5 (8) | 28 (9) | 0.872 |
| CPAP | 4 (2) | - | - | 4 (1) | 0.667 |
| Chest X-ray | 45 (19) | 15 (83) | 17 (26) | 77 (24) | <0.001 |
| Normal | 5 (11) | 1 (7) | 4 (24) | 10 (13) | |
| Other infiltrate | 30 (67) | 5 (33) | 10 (59) | 45 (58) | |
| Alveolar consolidation | 10 (22) | 3(20) | 3 (18) | 16 (21) | |
| Large dense infiltrate/ lobar consolidation | - | 6 (40) | - | 6 (8) | |
| Pleural effusion | 4 (9) | 6 (40) | 3 (18) | 13 (17) | |
| Evidence of empyema | - | - | - | - | |
| Admitted to hospital ward | 71 (29) | 8 (44) | 28 (42) | 107 (32) | 0.071 |
| Admitted to ICU | 1 (0,4) | 1 (6) | - | 2 (0.6) | 0.147 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eklundh, A.; Rhedin, S.; Ryd-Rinder, M.; Andersson, M.; Gantelius, J.; Gaudenzi, G.; Lindh, M.; Peltola, V.; Waris, M.; Nauclér, P.; et al. Etiology of Clinical Community-Acquired Pneumonia in Swedish Children Aged 1–59 Months with High Pneumococcal Vaccine Coverage—The TREND Study. Vaccines 2021, 9, 384. https://doi.org/10.3390/vaccines9040384
Eklundh A, Rhedin S, Ryd-Rinder M, Andersson M, Gantelius J, Gaudenzi G, Lindh M, Peltola V, Waris M, Nauclér P, et al. Etiology of Clinical Community-Acquired Pneumonia in Swedish Children Aged 1–59 Months with High Pneumococcal Vaccine Coverage—The TREND Study. Vaccines. 2021; 9(4):384. https://doi.org/10.3390/vaccines9040384
Chicago/Turabian StyleEklundh, Annika, Samuel Rhedin, Malin Ryd-Rinder, Maria Andersson, Jesper Gantelius, Giulia Gaudenzi, Magnus Lindh, Ville Peltola, Matti Waris, Pontus Nauclér, and et al. 2021. "Etiology of Clinical Community-Acquired Pneumonia in Swedish Children Aged 1–59 Months with High Pneumococcal Vaccine Coverage—The TREND Study" Vaccines 9, no. 4: 384. https://doi.org/10.3390/vaccines9040384