Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Severe Invasive Disease Caused by Serotype 3 Streptococcus Pneumoniae in Italian Children

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Case Definition
2.3. Laboratory Methods
2.4. Evaluation of IPD Incidence and Impact of Vaccination
2.5. Statistical Analysis
3. Results
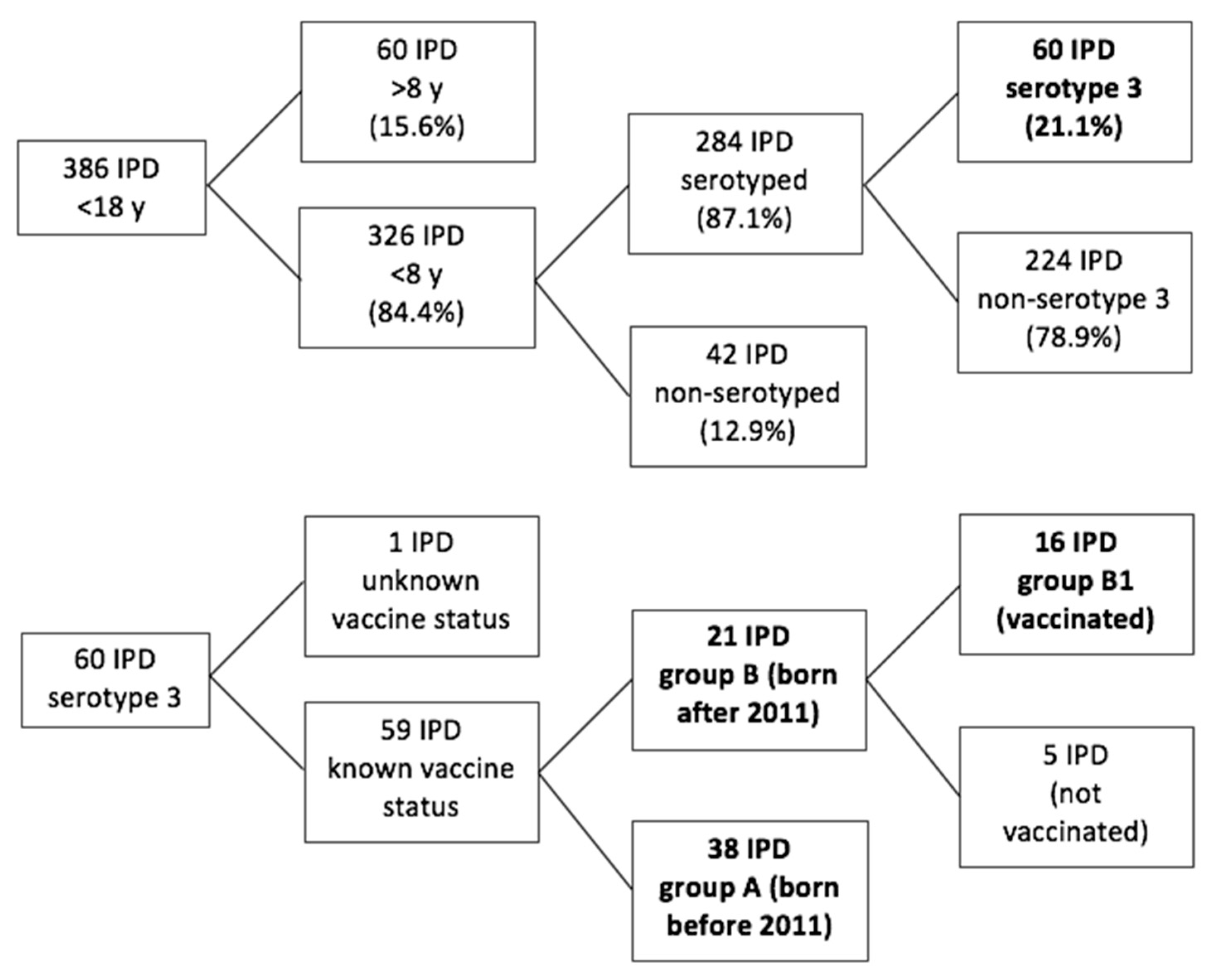
3.1. Demographic Data of Study Populations and IPD Serotype Distribution
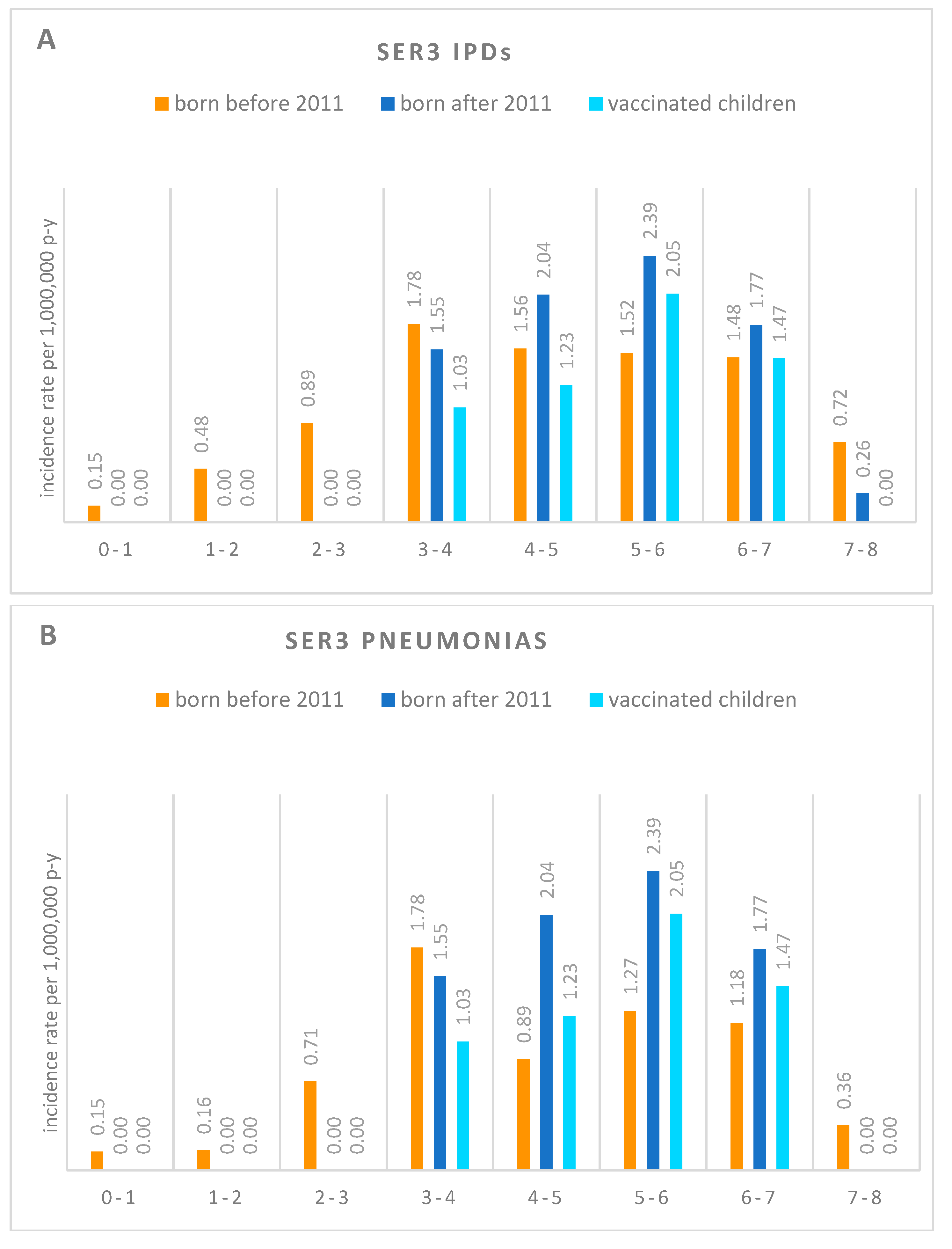
3.2. Impact of PCV13 on ser3 IPD Incidence Rates in a Cohort of Italian Children under 8
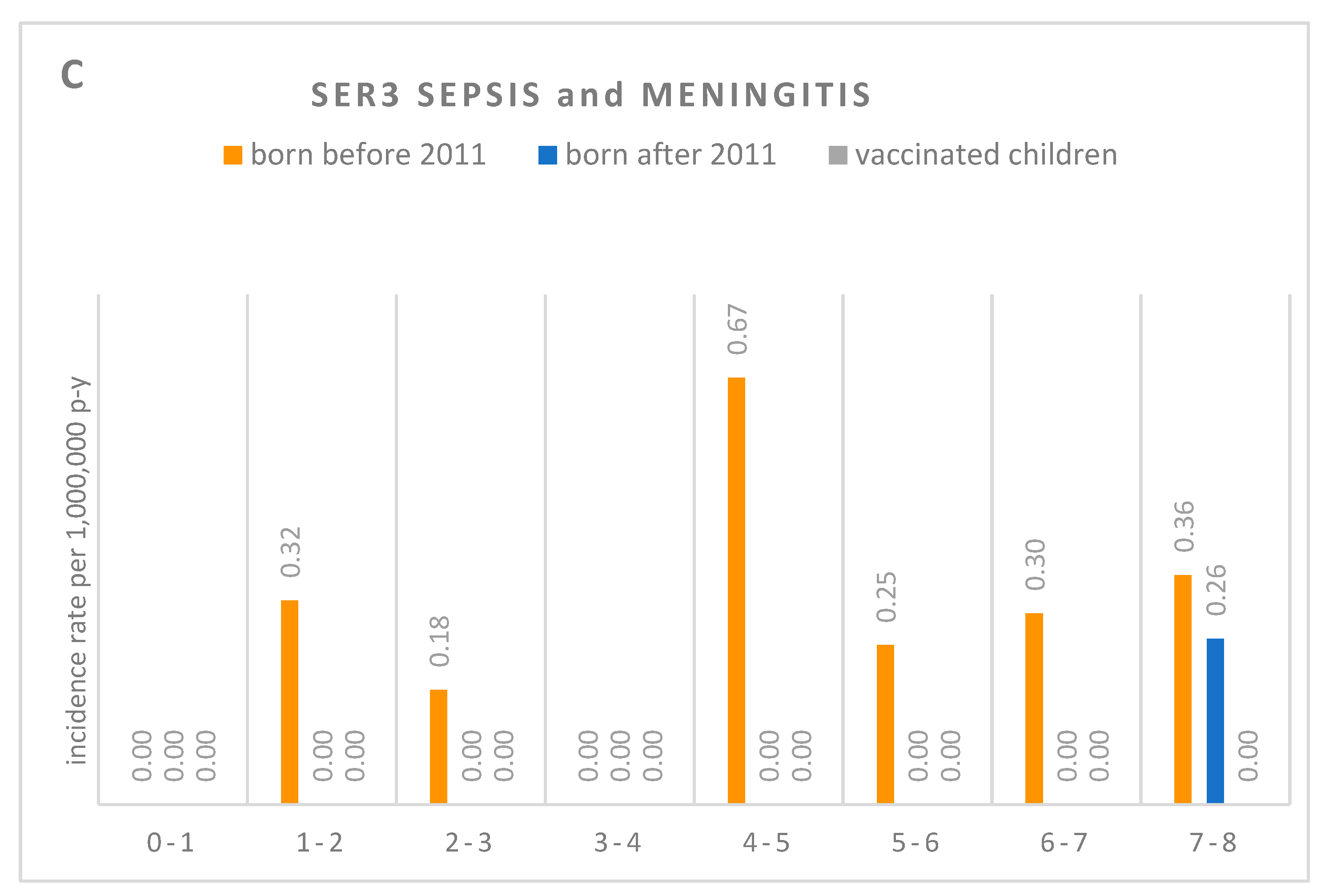
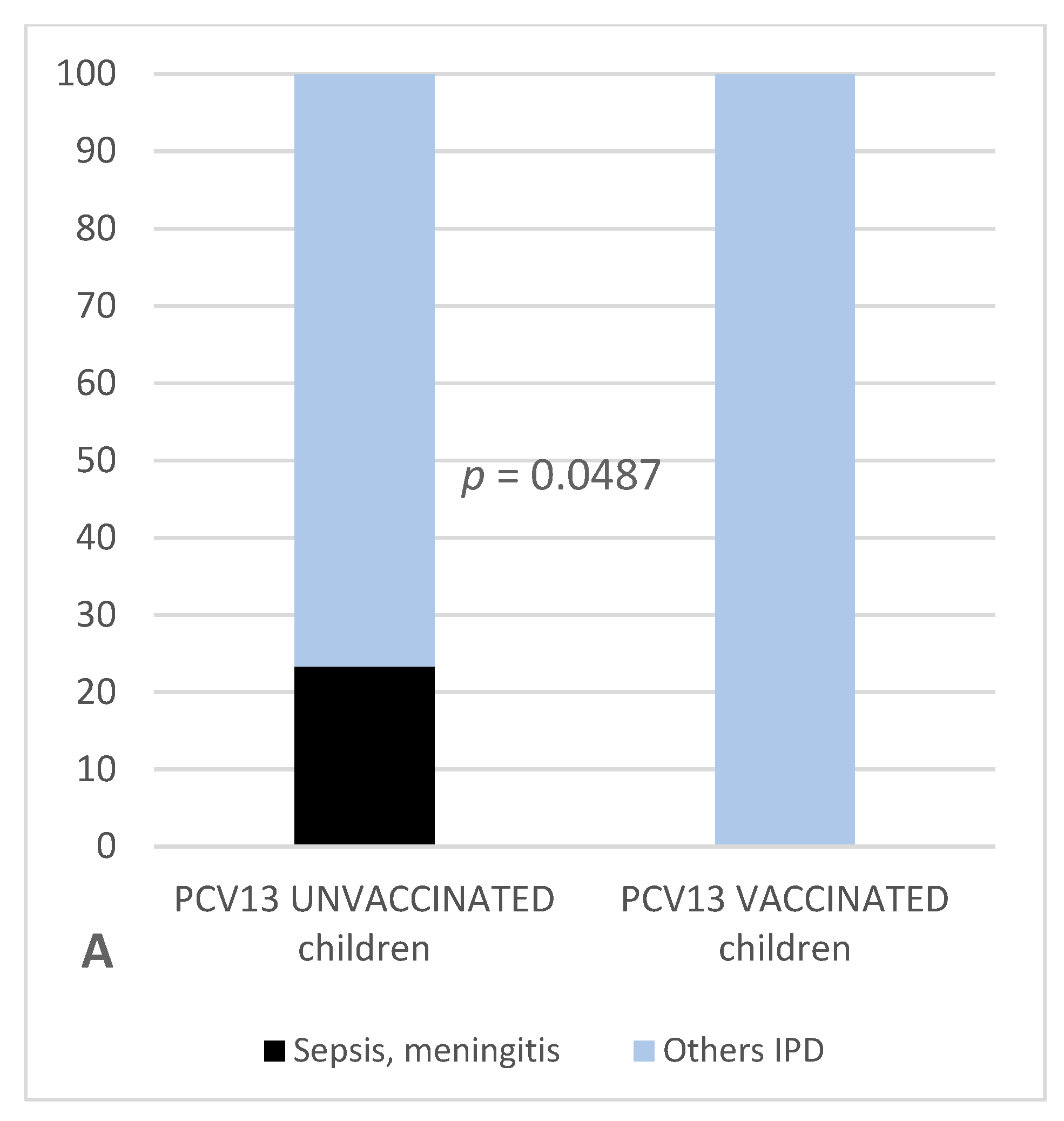
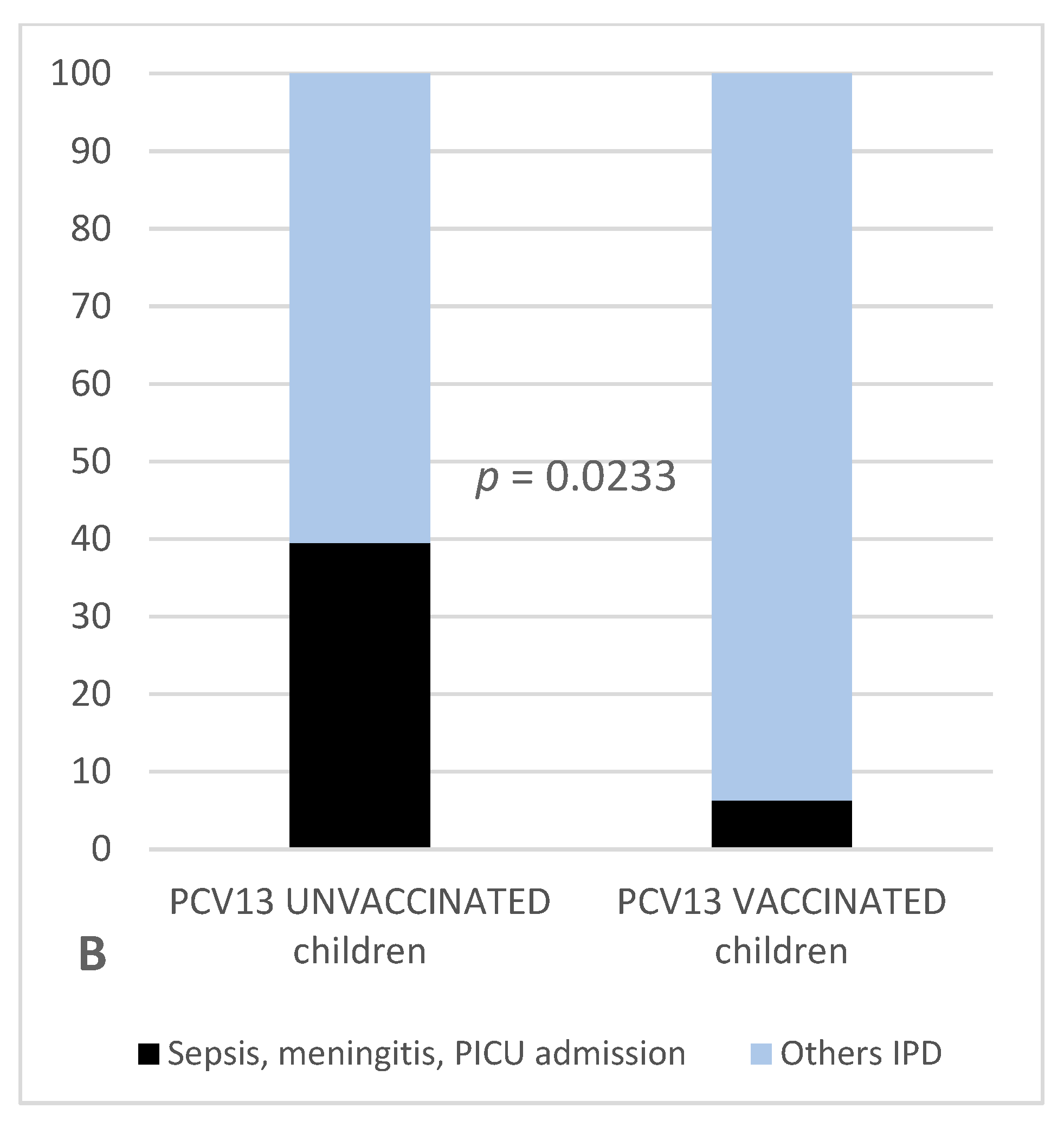
3.3. Impact of PCV13 on Different Clinical Presentation of ser3 Infection in Italian Children under 8
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Linley, E.; Bell, A.; Gritzfeld, J.F.; Borrow, R. Should Pneumococcal Serotype 3 Be Included in Serotype-Specific Immunoassays? Vaccines 2019, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.J.; Waight, P.A.; Burbidge, P.; Pearce, E.; Roalfe, L.; Zancolli, M.; Slack, M.; Ladhani, S.N.; Miller, E.; Goldblatt, D. Serotype-specific effectiveness and correlates of protection for the 13-valent pneumococcal conjugate vaccine: A postlicensure indirect cohort study. Lancet Infect. Dis. 2014, 14, 839–846. [Google Scholar] [CrossRef]
- Waight, P.A.; Andrews, N.J.; Ladhani, N.J.; Sheppard, C.L.; Slack, M.P.E.; Miller, E. Effect of the 13-valent pneumococcal conjugate vaccine on invasive pneumococcal disease in England and Wales 4 years after its introduction: An observational cohort study. Lancet Infect. Dis. 2015, 15, 629. [Google Scholar] [CrossRef]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Holtzman, C.; Harrison, L.H.; Zansky, S.M.; Rosen, J.B.; Reingold, A.; Scherzinger, K.; et al. Effectiveness of 13-valent pneumococcal conjugate vaccine for prevention of invasive pneumococcal disease in children in the USA: A matched case-control study. Lancet Respir. Med. 2016, 4, 399–406. [Google Scholar] [CrossRef]
- Silva-Costa, C.; Brito, M.J.; Pinho, M.D.; Friães, A.; Aguiar, S.I.; Ramirez, M.; Melo-Cristino, J. Portuguese Group for the Study of Streptococcal Infections; Portuguese Study Group of Invasive Pneumococcal Disease of the Pediatric Infectious Disease Society Pediatric Complicated Pneumonia Caused by Streptococcus pneumoniae Serotype 3 in 13-Valent Pneumococcal Conjugate Vaccinees, Portugal, 2010–2015. Emerg. Infect. Dis. 2018, 24, 1307–1314. [Google Scholar] [PubMed]
- Horácio, A.N.; Silva-Costa, C.; Lopes, J.P.; Ramirez, M.; Melo-Cristino, J. Portuguese Group for the Study of Streptococcal Infections Serotype 3 Remains the Leading Cause of Invasive Pneumococcal Disease in Adults in Portugal (2012–2014) Despite Continued Reductions in Other 13-Valent Conjugate Vaccine Serotypes. Front. Microbiol. 2016, 7, 1616. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Serranti, D.; Nieddu, F.; Moriondo, M.; Casini, A.; Lodi, L.; de Benedictis, F.M.; De Vitis, E.; Cavone, F.; Cortimiglia, M.; et al. Significant impact of pneumococcal conjugate vaccination on pediatric parapneumonic effusion: Italy 2006–2018. Vaccine 2019, 37, 2704–2711. [Google Scholar] [CrossRef] [PubMed]
- Madhi, F.; Levy, C.; Morin, L.; Minodier, P.; Dubos, F.; Zenkhri, F.; Dommergues, M.A.; Mezgueldi, E.; Levieux, K.; Pneumonia Study Group; et al. Change in Bacterial Causes of Community-Acquired Parapneumonic Effusion and Pleural Empyema in Children 6 Years After 13-Valent Pneumococcal Conjugate Vaccine Implementation. J. Pediatr. Infect. Dis. Soc. 2018. [Google Scholar] [CrossRef] [PubMed]
- Bender, J.M.; Ampofo, K.; Korgenski, K.; Daly, J.; Pavia, A.T.; Mason, E.O.; Byington, C.L. Pneumococcal necrotizing pneumonia in Utah: Does serotype matter? Clin. Infect. Dis. 2008, 46, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Salamon, D.; Marcon, M.; Nahm, M.H. Pneumococcal Serotypes Causing Pneumonia with Pleural Effusion in Pediatric Patients. J. Clin. Microbiol. 2011, 49, 534–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, E.H.; Zhang, F.; Lu, Y.-J.; Malley, R. Capsular Polysaccharide (CPS) Release by Serotype 3 Pneumococcal Strains Reduces the Protective Effect of Anti-Type 3 CPS Antibodies. Clin. Vaccine Immunol. 2016, 23, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Lexau, C.; Bennett, N.M.; Petit, S.; Zansky, S.M.; Harrison, L.H.; Reingold, A.; et al. Effect of use of 13-valent pneumococcal conjugate vaccine in children on invasive pneumococcal disease in children and adults in the USA: Analysis of multisite, population-based surveillance. Lancet Infect. Dis. 2015, 15, 301–309. [Google Scholar] [CrossRef]
- Van der Linden, M.; Falkenhorst, G.; Perniciaro, S.; Fitzner, C.; Imöhl, M. Effectiveness of Pneumococcal Conjugate Vaccines (PCV7 and PCV13) against Invasive Pneumococcal Disease among Children under Two Years of Age in Germany. PLoS ONE 2016, 11, E0161257. [Google Scholar] [CrossRef] [PubMed]
- Sings, H.L.; De Wals, P.; Gessner, B.D.; Isturiz, R.; Laferriere, C.; McLaughlin, J.M.; Pelton, S.; Schmitt, H.-J.; Suaya, J.A.; Jodar, L. Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine Against Invasive Disease Caused by Serotype 3 in Children: A Systematic Review and Meta-Analysis of Observational Studies. Clin. Infect. Dis. 2018, 68, 2135–2143. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.L. Why we need pneumococcal vaccine effectiveness studies. Lancet Respir. Med. 2016, 4, 343–345. [Google Scholar] [CrossRef]
- WHO. World Health Organization, 2010. In Proceedings of the Ninth Global Vaccine Research Forum and Parallel Satellite Symposia, Bamako, Mali, 6–9 December 2009. [Google Scholar]
- Azzari, C.; Nieddu, F.; Moriondo, M.; Indolfi, G.; Canessa, C.; Ricci, S.; Bianchi, L.; Serranti, D.; Poggi, G.M.; Resti, M. Underestimation of Invasive Meningococcal Disease in Italy. Emerg. Infect. Dis. 2016, 22, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Invasive Pneumococcal Disease/2010 Case Definition. Available online: https://wwwn.cdc.gov/nndss/conditions/invasive-pneumococcal-disease/case-definition/2010/ (accessed on 22 September 2019).
- Resti, M.; Moriondo, M.; Cortimiglia, M.; Indolfi, G.; Canessa, C.; Becciolini, L.; Bartolini, E.; de Benedictis, F.M.; de Martino, M.; Azzari, C.; et al. Community-acquired bacteremic pneumococcal pneumonia in children: Diagnosis and serotyping by real-time polymerase chain reaction using blood samples. Clin. Infect. Dis. 2010, 51, 1042–1049. [Google Scholar] [CrossRef]
- Tan, T.Q.; Mason, E.O.; Wald, E.R.; Barson, W.J.; Schutze, G.E.; Bradley, J.S.; Givner, L.B.; Yogev, R.; Kim, K.S.; Kaplan, S.L. Clinical characteristics of children with complicated pneumonia caused by Streptococcus pneumoniae. Pediatrics 2002, 110, 1–6. [Google Scholar] [CrossRef]
- Harris, M.; Clark, J.; Coote, N.; Fletcher, P.; Harnden, A.; McKean, M.; Thomson, A. British Thoracic Society Standards of Care Committee British Thoracic Society guidelines for the management of community acquired pneumonia in children: Update 2011. Thorax 2011, 66 (Suppl. 2), ii1–ii23. [Google Scholar] [CrossRef]
- Sawicki, G.S.; Lu, F.L.; Valim, C.; Cleveland, R.H.; Colin, A.A. Necrotising pneumonia is an increasingly detected complication of pneumonia in children. Eur. Respir. J. 2008, 31, 1285–1291. [Google Scholar] [CrossRef]
- Balfour-Lynn, I.M.; Abrahamson, E.; Cohen, G.; Hartley, J.; King, S.; Parikh, D.; Spencer, D.; Thomson, A.H.; Urquhart, D. Paediatric Pleural Diseases Subcommittee of the BTS Standards of Care Committee BTS guidelines for the management of pleural infection in children. Thorax 2005, 60 (Suppl. 1), i1–i21. [Google Scholar] [CrossRef]
- Goldstein, B.; Giroir, B.; Randolph, A. International Consensus Conference on Pediatric Sepsis International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr. Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S. Acute bacterial meningitis in infants and children. Lancet Infect. Dis. 2010, 10, 32–42. [Google Scholar] [CrossRef]
- Nieddu, F.; Moriondo, M.; De Vitis, E.; Ricci, S.; Indolfi, G.; Resti, M.; Vocale, C.; Landini, M.P.; Sartor, A.; Azzari, C.; et al. PCV13 serotype decrease in Italian adolescents and adults in the post-PCV13 era: Herd protection from children or secular trend? Vaccine 2017, 35, 1544–1550. [Google Scholar] [CrossRef] [PubMed]
- Modak, J.K.; Steinhoff, M.C.; Zaman, K.; Islam, M.; El Arifeen, S.; Saha, S.K. Detection and serotyping of lyophilized nonculturable pneumococcal isolates. J. Clin. Microbiol. 2012, 50, 3388–3390. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Moriondo, M.; Indolfi, G.; Cortimiglia, M.; Canessa, C.; Becciolini, L.; Lippi, F.; de Martino, M.; Resti, M. Realtime PCR is more sensitive than multiplex PCR for diagnosis and serotyping in children with culture negative pneumococcal invasive disease. PLoS ONE 2010, 5, e9282. [Google Scholar] [CrossRef]
- Azzari, C.; Moriondo, M.; Cortimiglia, M.; Valleriani, C.; Canessa, C.; Indolfi, G.; Ricci, S.; Nieddu, F.; de Martino, M.; Resti, M.; et al. Potential serotype coverage of three pneumococcal conjugate vaccines against invasive pneumococcal infection in Italian children. Vaccine 2012, 30, 2701–2705. [Google Scholar] [CrossRef]
- Vaccinazioni Dell’età Pediatrica. Anno 2017 (Coorte 2015) Coperture Vaccinali a 24 Mesi (per 100 Abitanti), Calcolate sui Riepiloghi Inviati DALLE REGIONI e PP.AA. (per Singolo Antigene); Ministry of Health: Rome, Italy, 2017. Available online: https://www.quotidianosanita.it/allegati/allegato5380868.pdf (accessed on 22 September 2019).
- Vaccinazioni Dell’età Pediatrica. Anno 2017 (Coorte 2014) Coperture* Vaccinali (per 100 Abitanti) a 36 Mesi, Calcolate sui Riepiloghi Inviati Dalle Regioni e PP.AA. (per Singolo Antigene); Ministry of Health: Rome, Italy, 2017. Available online: https://www.quotidianosanita.it/allegati/allegato5380868.pdf (accessed on 22 September 2019).
- Vaccinazioni Dell’età Pediatrica. Anno 2017 (Coorte 2013) Coperture* Vaccinali (per 100 Abitanti) a 48 Mesi, Calcolate sui Riepiloghi Inviati Dalle Regioni e PP.AA. (per Singolo Antigene); Ministry of Health: Rome, Italy, 2017. Available online: https://www.quotidianosanita.it/allegati/allegato5380868.pdf (accessed on 22 September 2019).
- Demo-Geodemo—Mappe, Popolazione, Statistiche Demografiche dell’ISTAT. Available online: http://demo.istat.it/ (accessed on 2 December 2018).
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 23 September 2019).
- Domínguez, Á.; Ciruela, P.; Hernández, S.; García-García, J.J.; Soldevila, N.; Izquierdo, C.; Moraga-Llop, F.; Díaz, A.F.; de Sevilla, M.; González-Peris, S.; et al. Effectiveness of the 13-valent pneumococcal conjugate vaccine in preventing invasive pneumococcal disease in children aged 7–59 months. A matched case-control study. PLoS ONE 2017, 12, e0183191. [Google Scholar] [CrossRef]
- WHO/Pneumococcal Conjugate Vaccines. Available online: http://www.who.int/biologicals/publications/trs/areas/vaccines/pneumo/en/ (accessed on 12 August 2018).
- Jódar, L.; Butler, J.; Carlone, G.; Dagan, R.; Goldblatt, D.; Käyhty, H.; Klugman, K.; Plikaytis, B.; Siber, G.; Kohberger, R.; et al. Serological criteria for evaluation and licensure of new pneumococcal conjugate vaccine formulations for use in infants. Vaccine 2003, 21, 3265–3272. [Google Scholar] [CrossRef]
- Prymula, R.; Peeters, P.; Chrobok, V.; Kriz, P.; Novakova, E.; Kaliskova, E.; Kohl, I.; Lommel, P.; Poolman, J.; Prieels, J.-P.; et al. Pneumococcal capsular polysaccharides conjugated to protein D for prevention of acute otitis media caused by both Streptococcus pneumoniae and non-typable Haemophilus influenzae: A randomised double-blind efficacy study. Lancet 2006, 367, 740–748. [Google Scholar] [CrossRef]
- Approved Products > Prevnar 13. Available online: http://wayback.archive-it.org/7993/20170722071714/https://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm201667.htm (accessed on 12 August 2018).
- Poolman, J.; Kriz, P.; Feron, C.; Di-Paolo, E.; Henckaerts, I.; Miseur, A.; Wauters, D.; Prymula, R.; Schuerman, L. Pneumococcal serotype 3 otitis media, limited effect of polysaccharide conjugate immunisation and strain characteristics. Vaccine 2009, 27, 3213–3222. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.C.; Madhi, S.A. Review on the immunogenicity and safety of PCV-13 in infants and toddlers. Expert Rev. Vaccines 2011, 10, 951–980. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A. Correlates of protection induced by vaccination. Clin. Vaccine Immunol. CVI 2010, 17, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Italian Health Institute. Surveillance of Invasive Bacterial Diseases in Italy. 2017 “INTERIM” REPORT. Available online: http://old.iss.it/binary/mabi/cont/InterimReport2017.pdf (accessed on 20 August 2019).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Groups | Ser3 IPD | Ser3 Pneumonias | Ser3 Sepsis/Meningitis |
|---|---|---|---|
| Children born before 2011 | 0.99 (0.96–1.02) | 0.76 (0.60–0.92) | 0.24 (−0.04–0.52) |
| Crude incidence rates | |||
| Children born after 2011 | 0.87 (0.73–1.01) | 0.85 (0.70–1.01) | 0.02 (−0.25–0.29) |
| Age-standardized incidence rates | |||
| Vaccinated children | 0.62 (0.38–0.86) | 0.62 (0.38–0.86) | 0.00 (NaN) |
| Age-standardized incidence rates |
| Children Born before PCV13 Introduction | Type of Infection | Children Born after PCV13 Introduction | Children Vaccinated with PCV13 |
|---|---|---|---|
| 29 | Complicated Pneumonias
| 21 | 16 |
| 11 | 11 | 8 | |
| 17 | 9 | 8 | |
| 1 | 1 | 0 | |
| 4 | Sepsis | 0 | 0 |
| 5 | Meningitis | 1 | 0 |
| 38 | Total | 22 | 16 |
| PCV13 Unvaccinated | Type of Infection | PCV13 Vaccinated |
|---|---|---|
| 33 | Complicated Pneumonias
| 16 |
| 13 | 8 | |
| 18 | 8 | |
| 2 | 0 | |
| 4 | Sepsis | 0 |
| 6 | Meningitis | 0 |
| 43 | Total | 16 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lodi, L.; Ricci, S.; Nieddu, F.; Moriondo, M.; Lippi, F.; Canessa, C.; Mangone, G.; Cortimiglia, M.; Casini, A.; Lucenteforte, E.; et al. Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Severe Invasive Disease Caused by Serotype 3 Streptococcus Pneumoniae in Italian Children. Vaccines 2019, 7, 128. https://doi.org/10.3390/vaccines7040128
Lodi L, Ricci S, Nieddu F, Moriondo M, Lippi F, Canessa C, Mangone G, Cortimiglia M, Casini A, Lucenteforte E, et al. Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Severe Invasive Disease Caused by Serotype 3 Streptococcus Pneumoniae in Italian Children. Vaccines. 2019; 7(4):128. https://doi.org/10.3390/vaccines7040128
Chicago/Turabian StyleLodi, Lorenzo, Silvia Ricci, Francesco Nieddu, Maria Moriondo, Francesca Lippi, Clementina Canessa, Giusi Mangone, Martina Cortimiglia, Arianna Casini, Ersilia Lucenteforte, and et al. 2019. "Impact of the 13-Valent Pneumococcal Conjugate Vaccine on Severe Invasive Disease Caused by Serotype 3 Streptococcus Pneumoniae in Italian Children" Vaccines 7, no. 4: 128. https://doi.org/10.3390/vaccines7040128