
Pregnancy Outcomes among Pregnant Persons after COVID-19 Vaccination: Assessing Vaccine Safety in Retrospective Cohort Analysis of U.S. National COVID Cohort Collaborative (N3C)
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Overall Structure
2.2. Ethical Reviews
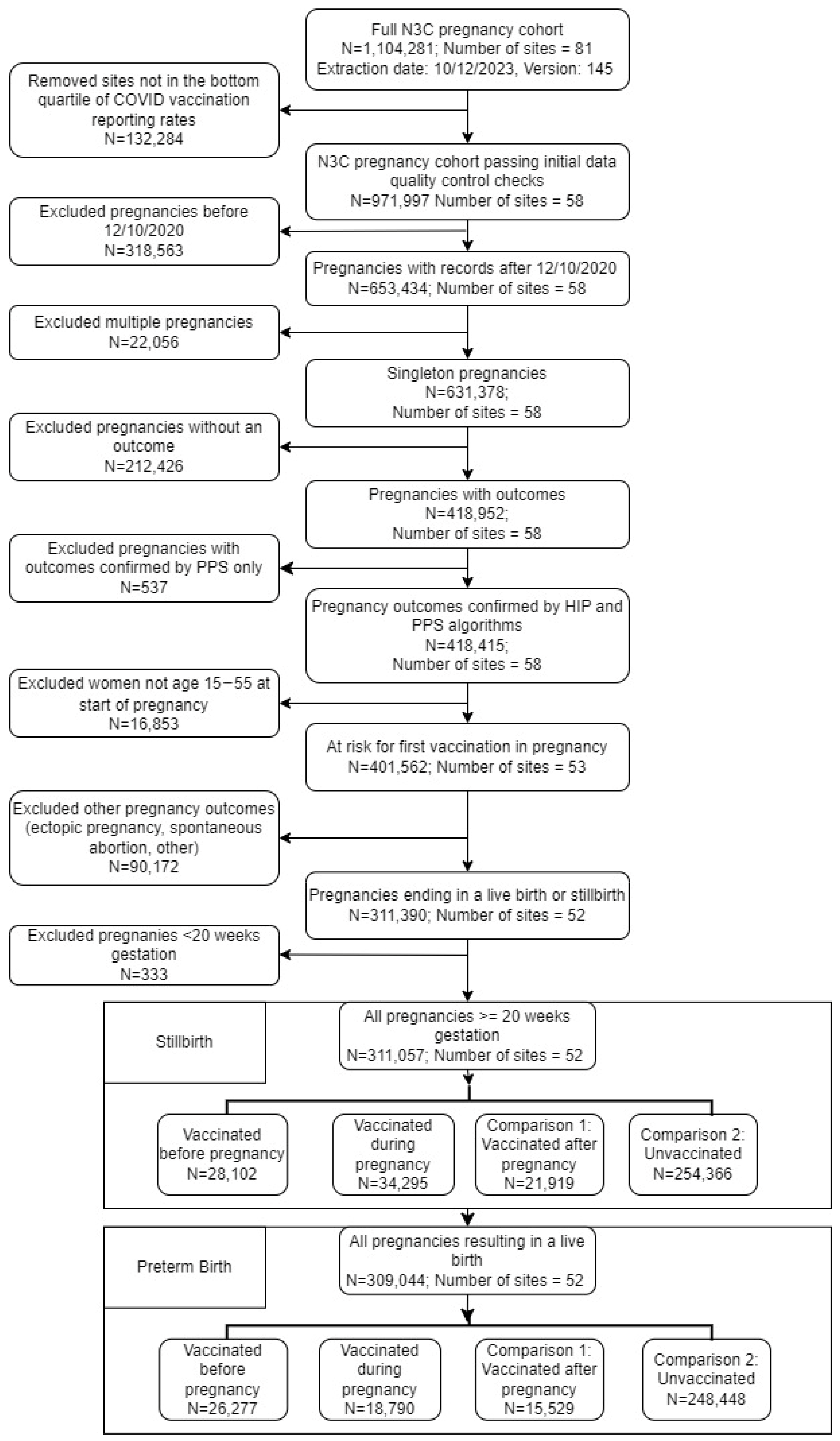
2.3. Study Design and Analytic Sample
2.4. Exposures
2.5. Outcomes
2.6. Covariates
2.7. Statistical Analyses
3. Results
3.1. Sample Description and Baseline Characteristics
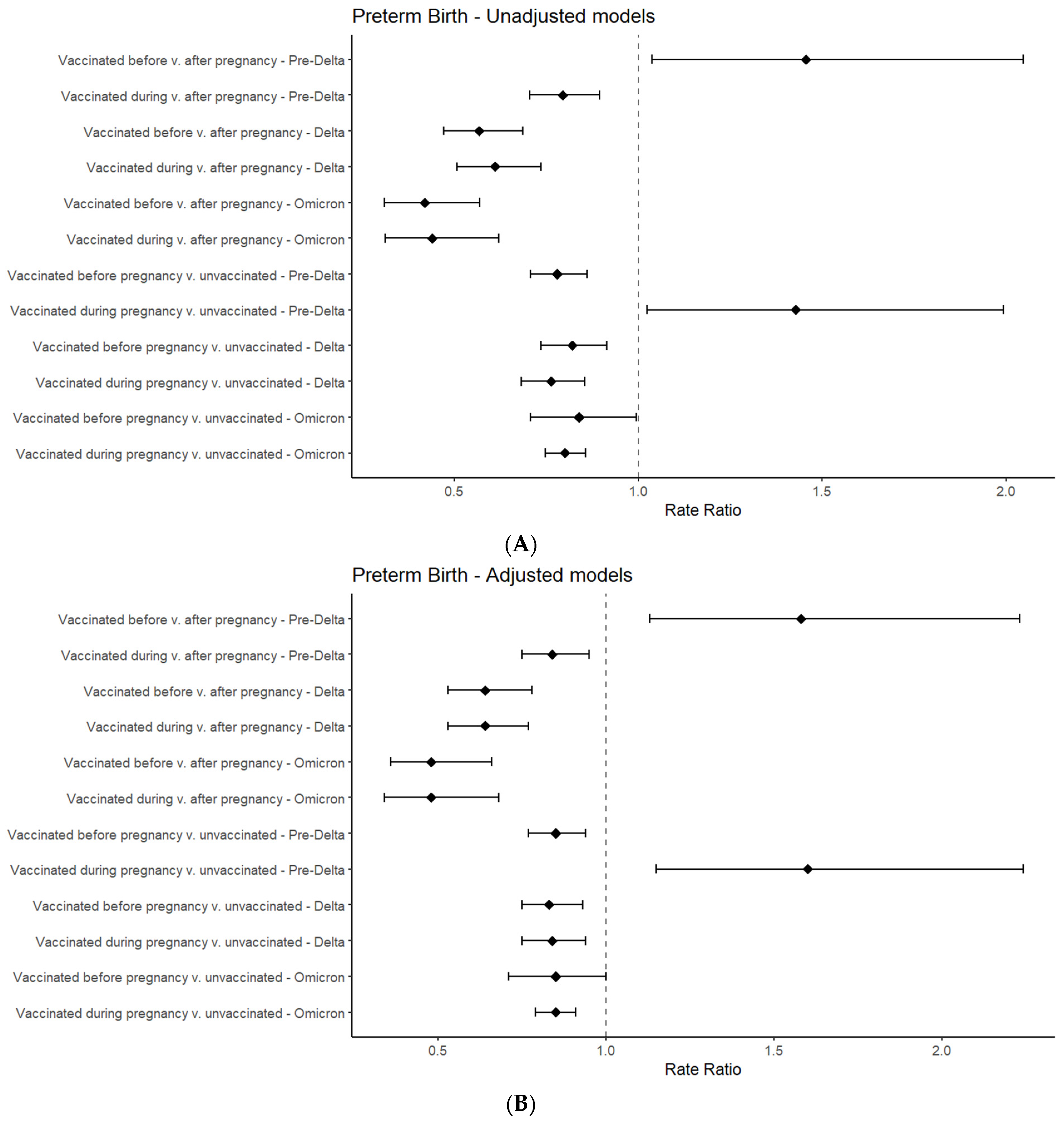
3.2. Regression Results for Preterm Birth
3.3. Regression Results for Stillbirth
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
N3C Attribution
Data Partners with Released Data
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Lau, J.J.; Cheng, S.M.S.; Leung, K.; Lee, C.K.; Hachim, A.; Tsang, L.C.H.; Yam, K.W.H.; Chaothai, S.; Kwan, K.K.H.; Chai, Z.Y.H.; et al. Real-world COVID-19 vaccine effectiveness against the Omicron BA.2 variant in a SARS-CoV-2 infection-naive population. Nat. Med. 2023, 29, 348–357. [Google Scholar] [CrossRef]
- Buchan, S.A.; Chung, H.; Brown, K.A.; Austin, P.C.; Fell, D.B.; Gubbay, J.B.; Nasreen, S.; Schwartz, K.L.; Sundaram, M.E.; Tadrous, M.; et al. Estimated Effectiveness of COVID-19 Vaccines Against Omicron or Delta Symptomatic Infection and Severe Outcomes. JAMA Netw. Open 2022, 5, e2232760. [Google Scholar] [CrossRef]
- Self, W.H.; Tenforde, M.W.; Rhoads, J.P.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; et al. Comparative Effectiveness of Moderna, Pfizer-BioNTech, and Janssen (Johnson & Johnson) Vaccines in Preventing COVID-19 Hospitalizations Among Adults Without Immunocompromising Conditions—United States, March–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1337–1343. [Google Scholar] [CrossRef]
- Qin, Q.; Wilkins, K.J.; Jones, S.E.; Bradwell, K.R.; Chan, L.; Sun, J.; Anzalone, J.; Zheng, Q.; Liebman, M.; Mariona, F.; et al. Evaluating COVID-19 Vaccine Effectiveness among Pregnant Persons in the U.S.: Retrospective Cohort Analysis from a Nationally Sampled Cohort in N3C. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4174295 (accessed on 7 December 2023).
- Rubin, R. Pregnant People’s Paradox—Excluded From Vaccine Trials Despite Having a Higher Risk of COVID-19 Complications. JAMA 2021, 325, 1027. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Effectiveness and Safety of COVID-19 Vaccine among Pregnant Women in Real-World Studies: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 246. [Google Scholar] [CrossRef]
- Pratama, N.R.; Wafa, I.A.; Budi, D.S.; Putra, M.; Wardhana, M.P.; Wungu, C.D.K. mRNA COVID-19 vaccines in pregnancy: A systematic review. PLoS ONE 2022, 17, e0261350. [Google Scholar] [CrossRef]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. Coronavirus disease 2019 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, 303.e1–303.e17. [Google Scholar] [CrossRef]
- Collier, A.-R.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Bondzie, E.A.; Sellers, D.; et al. Immunogenicity of COVID-19 mRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Trinchillo, M.G.; Di Girolamo, R.; Raffone, A.; Saccone, G.; Iorio, G.G.; Gabrielli, O.; Maruotti, G.M. COVID-19 vaccine and pregnancy outcomes: A systematic review and meta-analysis. Int. J. Gynecol. Obstet. 2022, 159, 651–661. [Google Scholar] [CrossRef]
- Seasely, A.R.; Blanchard, C.T.; Arora, N.; Battarbee, A.N.M.; Casey, B.M.; Dionne-Odom, J.M.; Sinkey, R.G.; Szychowski, J.M.; Tita, A.T.; Subramaniam, A.; et al. Maternal and Perinatal Outcomes Associated With the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Delta (B.1.617.2) Variant. Obstet. Gynecol. 2021, 138, 842–844. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, A.D.; Brunkard, J.M.; Boehmer, T.K.; Peterson, E.; Adjei, S.; Binder, A.M.; Cobb, S.; Graff, P.; Hidalgo, P.; Panaggio, M.J.; et al. Trends in Disease Severity and Health Care Utilization During the Early Omicron Variant Period Compared with Previous SARS-CoV-2 High Transmission Periods—United States, December 2020–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Haendel, M.A.; Chute, C.G.; Bennett, T.D.; Eichmann, D.A.; Guinney, J.; Kibbe, W.A.; Payne, P.R.O.; Pfaff, E.R.; Robinson, P.N.; Saltz, J.H.; et al. The National COVID Cohort Collaborative (N3C): Rationale, design, infrastructure, and deployment. J. Am. Med. Inform. Assoc. 2021, 28, 427–443. [Google Scholar] [CrossRef] [PubMed]
- Bennett, T.D.; Moffitt, R.A.; Hajagos, J.G.; Amor, B.; Anand, A.; Bissell, M.M.; Bradwell, K.R.; Bremer, C.; Byrd, J.B.; Denham, A.; et al. Clinical Characterization and Prediction of Clinical Severity of SARS-CoV-2 Infection Among US Adults Using Data From the US National COVID Cohort Collaborative. JAMA Netw. Open 2021, 4, e2116901. [Google Scholar] [CrossRef]
- National Institutes of Health. National Center for Advancing Translational Sciences (NCATS). 2023. Available online: https://ncats.nih.gov/n3c (accessed on 7 December 2023).
- Jones, S.E.; Chan, L.E.; McMurry, J.A.; Olson-Chen, C.; Tarleton, J.; Wilkins, K.J.; Ly, V.; Ljazouli, S.; Qin, Q.; Faherty, E.G.; et al. Who is pregnant? Defining real-world data-based pregnancy episodes in the National COVID Cohort Collaborative (N3C). JAMIA Open 2023, 6, ooad067. [Google Scholar] [CrossRef]
- Food and Drug Administration. FDA Takes Key Action in Fight Against COVID-19 By Issuing Emergency Use Authorization for First COVID-19 Vaccines Against COVID-19 By Issuing Emergency Use Authorization for First COVID-19 Vaccine. In FDA News Release; 11 December 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19 (accessed on 7 December 2023).
- Centers for Disease Control and Prevention. What Is Stillbirth? Stillbirth. 29 September 2022. Available online: https://www.cdc.gov/ncbddd/stillbirth/facts.html (accessed on 20 December 2023).
- Prasad, S.; Kalafat, E.; Blakeway, H.; Townsend, R.; O’brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Le Doare, K.; Ladhani, S.; et al. Systematic review and meta-analysis of the effectiveness and perinatal outcomes of COVID-19 vaccination in pregnancy. Nat. Commun. 2022, 13, 2414. [Google Scholar] [CrossRef]
- Ciapponi, A.; Berrueta, M.; Parker, E.P.; Bardach, A.; Mazzoni, A.; Anderson, S.A.; Argento, F.J.; Ballivian, J.; Bok, K.; Comandé, D.; et al. Safety of COVID-19 vaccines during pregnancy: A systematic review and meta-analysis. Vaccine 2023, 41, 3688–3700. [Google Scholar] [CrossRef]
- Keller-Stanislawski, B.; Englund, J.A.; Kang, G.; Mangtani, P.; Neuzil, K.; Nohynek, H.; Pless, R.; Lambach, P.; Zuber, P. Safety of immunization during pregnancy: A review of the evidence of selected inactivated and live attenuated vaccines. Vaccine 2014, 32, 7057–7064. [Google Scholar] [CrossRef]
- Maier, C.; Kapsner, L.A.; Mate, S.; Prokosch, H.-U.; Kraus, S. Patient Cohort Identification on Time Series Data Using the OMOP Common Data Model. Appl. Clin. Inform. 2021, 12, 057–064. [Google Scholar] [CrossRef]
- Boytchev, H. Maternal RSV vaccine: Further analysis is urged on preterm births. BMJ 2023, 381, p1021. [Google Scholar] [CrossRef]
- Howards, P.P.; Hertz-Picciotto, I.; Weinberg, C.R.; Poole, C. Misclassification of Gestational Age in the Study of Spontaneous Abortion. Am. J. Epidemiol. 2006, 164, 1126–1136. [Google Scholar] [CrossRef]
- Quinn, J.-A.; Munoz, F.M.; Gonik, B.; Frau, L.; Cutland, C.; Mallett-Moore, T.; Kissou, A.; Wittke, F.; Das, M.; Nunes, T.; et al. Preterm birth: Case definition & guidelines for data collection, analysis, and presentation of immunisation safety data. Vaccine 2016, 34, 6047–6056. [Google Scholar] [CrossRef]
- World Health Organization. Preterm Birth. 10 May 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 7 December 2023).
- Vress, D. Future vaccines in pregnancy. Best. Pract. Res. Clin. Obstet. Gynaecol. 2021, 76, 96–106. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. SARS-CoV-2 Variant Classifications and Definitions. 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html#anchor_1632158775384 (accessed on 7 December 2023).
- Hilbe, J.M. Modeling Count Data; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar] [CrossRef]
- Fay, M.P. Two-sided Exact Tests and Matching Confidence Intervals for Discrete Data. R J. 2010, 2, 53. [Google Scholar] [CrossRef]
- Oster, R.A.; Hilbe, J.M. An Examination of Statistical Software Packages for Parametric and Nonparametric Data Analyses Using Exact Methods. Am. Stat. 2008, 62, 74–84. [Google Scholar] [CrossRef]
- Fleming-Dutra, K.E.; Zauche, L.H.; Roper, L.E.; Ellington, S.R.; Olson, C.K.; Sharma, A.J.; Woodworth, K.R.; Tepper, N.; Havers, F.; Oliver, S.E.; et al. Safety and Effectiveness of Maternal COVID-19 Vaccines Among Pregnant People and Infants. Obstet. Gynecol. Clin. N. Am. 2023, 50, 279–297. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S.; Zhang, X.; Platt, R.W. Analyzing Risks of Adverse Pregnancy Outcomes. Am. J. Epidemiol. 2014, 179, 361–367. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. End of Public Health Emergency. 12 September 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/end-of-phe.html (accessed on 7 December 2023).
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Edlow, A.G.; Castro, V.M.; Shook, L.L.; Haneuse, S.; Kaimal, A.J.; Perlis, R.H. Sex-Specific Neurodevelopmental Outcomes Among Offspring of Mothers With SARS-CoV-2 Infection During Pregnancy. JAMA Netw. Open 2023, 6, e234415. [Google Scholar] [CrossRef]
- Jorgensen, S.C.J.; Drover, S.S.M.; Fell, D.B.; Austin, P.C.; D’souza, R.; Guttmann, A.; Buchan, S.A.; Wilson, S.E.; Nasreen, S.; Schwartz, K.L.; et al. Newborn and Early Infant Outcomes Following Maternal COVID-19 Vaccination During Pregnancy. JAMA Pediatr. 2023, 177, 1314. [Google Scholar] [CrossRef]
- Torche, F.; Nobles, J. Vaccination, immunity, and the changing impact of COVID-19 on infant health. Proc. Natl. Acad. Sci. USA 2023, 120, e2311573120. [Google Scholar] [CrossRef]
- Abu-Raya, B.; Madhi, S.A.; Omer, S.B.; Amirthalingam, G.; Giles, M.L.; Flanagan, K.L.; Zimmermann, P.; O’ryan, M.; Safadi, M.A.; Papaevangelou, V.; et al. Global Perspectives on Immunization Against SARS-CoV-2 During Pregnancy and Priorities for Future Research: An International Consensus Paper from the World Association of Infectious Diseases and Immunological Disorders. Front. Immunol. 2021, 12, 808064. [Google Scholar] [CrossRef]
- Whitaker, J.A.; Sahly, H.M.E.; Healy, C.M. mRNA vaccines against respiratory viruses. Curr. Opin. Infect. Dis. 2023, 36, 385–393. [Google Scholar] [CrossRef]
- Karam, M.; Daoud, G. mRNA vaccines: Past, present, future. Asian J. Pharm. Sci. 2022, 17, 491–522. [Google Scholar] [CrossRef]
- The PREVENT Working Group. Pregnant Women & Vaccines Against Emerging Epidemic Threats: Ethics Guidance for Preparedness, Research, and Response. 2018. Available online: https://bioethics.jhu.edu/wp-content/uploads/2022/06/PREVENT-Web.pdf (accessed on 7 December 2023).
- The PHASES Working Group. Ending the Evidence Gap for Pregnant Women around HIV & Co-Infections: A Call to Action. 2020. Available online: https://static1.squarespace.com/static/53f27090e4b0dbe1ff72f27c/t/5f07a624880c7766cd9a8160/1594336808166/PHASES_Guidance_Full_Report_and_Guidance_%28July_2020%29.pdf (accessed on 7 December 2023).
- American College of Obstetricians and Gynecologists. Committee Opinion No. 646: Ethical Considerations for Including Women as Research Participants. Obstet. Gynecol. 2015, 126, e100–e107. [Google Scholar] [CrossRef]
- Board on Health Sciences Policy, Health and Medicine Division, National Academies of Sciences, Engineering, and Medicine. Research with Pregnant and Lactating Persons: Mitigating Risk and Liability: Proceedings of a Workshop-in Brief; Forstag, E.H., Ed.; National Academies Press: Washington, DC, USA, 2023. [Google Scholar] [CrossRef]
- Sun, J.; Zheng, Q.; Madhira, V.; Olex, A.L.; Anzalone, A.J.; Vinson, A.; Singh, J.A.; French, E.; Abraham, A.G.; Mathew, J.; et al. Association Between Immune Dysfunction and COVID-19 Breakthrough Infection After SARS-CoV-2 Vaccination in the US. JAMA Intern. Med. 2022, 182, 153. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-19 Vaccinations in the United States. COVID Data Tracker. 11 May 2023. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-onedose-pop-total (accessed on 28 December 2023).
- Centers for Disease Control and Prevention. Reproductive Health. Preterm Birth. 2023. Available online: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm (accessed on 7 December 2023).
- Centers for Disease Control and Prevention. Data and Statistics. How Many Babies Are Stillborn? 2022. Available online: https://www.cdc.gov/ncbddd/stillbirth/data.html (accessed on 7 December 2023).




{kind=link}
{kind=link}
{kind=link}
| Variable Category | Category Level | Vaccinated before Pregnancy n = 26,433 | Vaccinated during Pregnancy n = 18,863 | Vaccinated after Pregnancy n = 15,597 | Unvaccinated n = 250,164 |
|---|---|---|---|---|---|
| Age in years, median (IQR) | 31 (28–34) | 31 (27–34) | 30 (26–34) | 29 (25–33) | |
| Race/ethnicity 2 | American Indian or Alaska Native | 178 (0.7%) | 72 (0.4%) | 75 (0.5%) | 1073 (0.4%) |
| Asian/Asian American | 1667 (6.3%) | 1173 (6.2%) | 917 (5.9%) | 11,019 (4.4%) | |
| Black/African American | 3156 (11.9%) | 2548 (13.5%) | 2883 (18.5%) | 47,893 (19.1%) | |
| Hawaiian or Pacific Islander | 157 (0.6%) | 79 (0.4%) | 68 (0.4%) | 1180 (0.5%) | |
| Hispanic | 1437 (5.4%) | 1136 (6%) | 978 (6.3%) | 17,139 (6.9%) | |
| Other | 168 (0.6%) | 81 (0.4%) | 104 (0.7%) | 2182 (0.9%) | |
| White | 15,793 (59.7%) | 10,648 (56.4%) | 7897 (50.6%) | 128,674 (51.4%) | |
| Missing | 3877 (14.7%) | 3126 (16.6%) | 2675 (17.2%) | 41,004 (16.4%) | |
| Region of participant residence | Midwest | 3295 (12.5%) | 2696 (14.3%) | 1799 (11.5%) | 36,194 (14.5%) |
| Northeast | 1596 (6%) | 1986 (10.5%) | 1841 (11.8%) | 23,425 (9.4%) | |
| South | 10,627 (40.2%) | 7338 (38.9%) | 5370 (34.4%) | 61,819 (24.7%) | |
| West | 3947 (14.9%) | 2329 (12.3%) | 1777 (11.4%) | 22,479 (9%) | |
| Missing | 6968 (26.4%) | 4514 (23.9%) | 4810 (30.8%) | 10,6247 (42.5%) | |
| Insurance | Medicare/Medicaid | 2148 (8.1%) | 2019 (10.7%) | 1829 (11.7%) | 35,433 (14.2%) |
| Private | 6570 (24.9%) | 4703 (24.9%) | 3414 (21.9%) | 38,763 (15.5%) | |
| Other | 1127 (4.3%) | 592 (3.1%) | 434 (2.8%) | 2480 (1%) | |
| None/Missing | 16,588 (62.8%) | 11,549 (61.2%) | 9920 (63.6%) | 173,488 (69.3%) | |
| Dominant COVID-19 variant period for majority of pregnancy duration | Pre-Delta | 410 (1.6%) | 9357 (49.6%) | 13,425 (86.1%) | 115,043 (46%) |
| Delta | 6814 (25.8%) | 6936 (36.8%) | 1836 (11.8%) | 54,806 (21.9%) | |
| Omicron | 19,209 (72.7%) | 2570 (13.6%) | 336 (2.2%) | 80,315 (32.1%) | |
| Primigravida | 2446 (9.3%) | 1803 (9.6%) | 1298 (8.3%) | 19,121 (7.6%) | |
| Number of chronic comorbidities | None | 13,735 (52%) | 10,276 (54.5%) | 8178 (52.4%) | 129,128 (51.6%) |
| 1 | 8354 (31.6%) | 5764 (30.6%) | 5021 (32.2%) | 82,359 (32.9%) | |
| 2 | 3015 (11.4%) | 1974 (10.5%) | 1685 (10.8%) | 27,810 (11.1%) | |
| 3 | 907 (3.4%) | 608 (3.2%) | 524 (3.4%) | 7916 (3.2%) | |
| 4 | 308 (1.2%) | 182 (1%) | 134 (0.9%) | 2181 (0.9%) | |
| 5 or more | 114 (0.4%) | 59 (0.3%) | 55 (0.4%) | 770 (0.3%) | |
| Chronic comorbidities | Hypertension | 2204 (8.3%) | 1312 (7%) | 1080 (6.9%) | 16,071 (6.4%) |
| Kidney disease | 564 (2.1%) | 369 (2%) | 284 (1.8%) | 4123 (1.6%) | |
| Type 1 diabetes | 333 (1.3%) | 252 (1.3%) | 188 (1.2%) | 2818 (1.1%) | |
| Type 2 diabetes | 1046 (4%) | 708 (3.8%) | 538 (3.4%) | 8664 (3.5%) | |
| Asthma | 3907 (14.8%) | 2569 (13.6%) | 2213 (14.2%) | 34,501 (13.8%) | |
| Cardiovascular disease | 2711 (10.3%) | 1718 (9.1%) | 1381 (8.9%) | 25,937 (10.4%) | |
| Chronic obstructive pulmonary disease | 58 (0.2%) | 35 (0.2%) | 37 (0.2%) | 508 (0.2%) | |
| Obesity | 8117 (30.7%) | 5613 (29.8%) | 5069 (32.5%) | 81,907 (32.7%) | |
| Any smoking or substance use | 270 (1%) | <20 | <20 | 3126 (1.2%) | |
| Any prior stillbirth | 114 (0.4%) | 94 (0.5%) | 55 (0.4%) | 1265 (0.5%) | |
| Any prior preterm birth | 598 (2.3%) | 328 (1.7%) | 267 (1.7%) | 5281 (2.1%) | |
| Trimester of COVID-19 infection in current pregnancy | No COVID-19 infection recorded during pregnancy | 20,696 (78.3%) | 16,203 (85.9%) | 13,545 (86.8%) | 206,657 (82.6%) |
| 1st trimester | 1077 (4.1%) | 437 (2.3%) | 341 (2.2%) | 5660 (2.3%) | |
| 2nd trimester | 2035 (7.7%) | 818 (4.3%) | 609 (3.9%) | 12,778 (5.1%) | |
| 3rd trimester | 2625 (9.9%) | 1405 (7.4%) | 1102 (7.1%) | 25,069 (10%) | |
| Trimester of COVID-19 vaccination in current pregnancy | 1st trimester | - | 5047 (27%) | - | - |
| 2nd trimester | - | 7365 (39%) | - | - | |
| 3rd trimester | - | 6451 (34%) | - | - | |
| Experienced COVID-19 infection prior to pregnancy | 4194 (15.9%) | 1120 (5.9%) | 414 (2.7%) | 15,327 (6.1%) | |
| Outcome of current pregnancy: preterm birth | 1279 (4.8%) | 877 (4.6%) | 920 (5.9%) | 14,610 (5.8%) | |
| Outcome of current pregnancy: stillbirth | 156 (0.6%) | 73 (0.4%) | 68 (0.4%) | 1716 (0.7%) | |
| Manufacturer of first COVID-19 vaccine received | AstraZeneca | <20 | - | - | - |
| Janssen | 1466 (5.5%) | 688 (3.6%) | 760 (4.9%) | - | |
| Moderna | 6410 (24.2%) | 3703 (19.6%) | 3033 (19.4%) | - | |
| Pfizer | 18,171 (68.7%) | 14,011 (74.3%) | 11,515 (73.8%) | - | |
| Missing | 369 (1.4%) | 461 (2.4%) | 289 (1.9%) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faherty, E.A.G.; Wilkins, K.J.; Jones, S.; Challa, A.; Qin, Q.; Chan, L.E.; Olson-Chen, C.; Tarleton, J.L.; Liebman, M.N.; Mariona, F.; et al. Pregnancy Outcomes among Pregnant Persons after COVID-19 Vaccination: Assessing Vaccine Safety in Retrospective Cohort Analysis of U.S. National COVID Cohort Collaborative (N3C). Vaccines 2024, 12, 289. https://doi.org/10.3390/vaccines12030289
Faherty EAG, Wilkins KJ, Jones S, Challa A, Qin Q, Chan LE, Olson-Chen C, Tarleton JL, Liebman MN, Mariona F, et al. Pregnancy Outcomes among Pregnant Persons after COVID-19 Vaccination: Assessing Vaccine Safety in Retrospective Cohort Analysis of U.S. National COVID Cohort Collaborative (N3C). Vaccines. 2024; 12(3):289. https://doi.org/10.3390/vaccines12030289
Chicago/Turabian StyleFaherty, Emily A. G., Kenneth J. Wilkins, Sara Jones, Anup Challa, Qiuyuan Qin, Lauren E. Chan, Courtney Olson-Chen, Jessica L. Tarleton, Michael N. Liebman, Federico Mariona, and et al. 2024. "Pregnancy Outcomes among Pregnant Persons after COVID-19 Vaccination: Assessing Vaccine Safety in Retrospective Cohort Analysis of U.S. National COVID Cohort Collaborative (N3C)" Vaccines 12, no. 3: 289. https://doi.org/10.3390/vaccines12030289