
Respiratory Syncytial Virus Infections in Polish Pediatric Patients from an Expert Perspective

 , , , , , ,
, , , , , ,
Abstract
:1. What Is Known
2. What Is New
3. Introduction
4. Methodology
5. Results
5.1. The Burden of RSV Disease in Poland
5.1.1. RSV Symptoms and Diagnosis
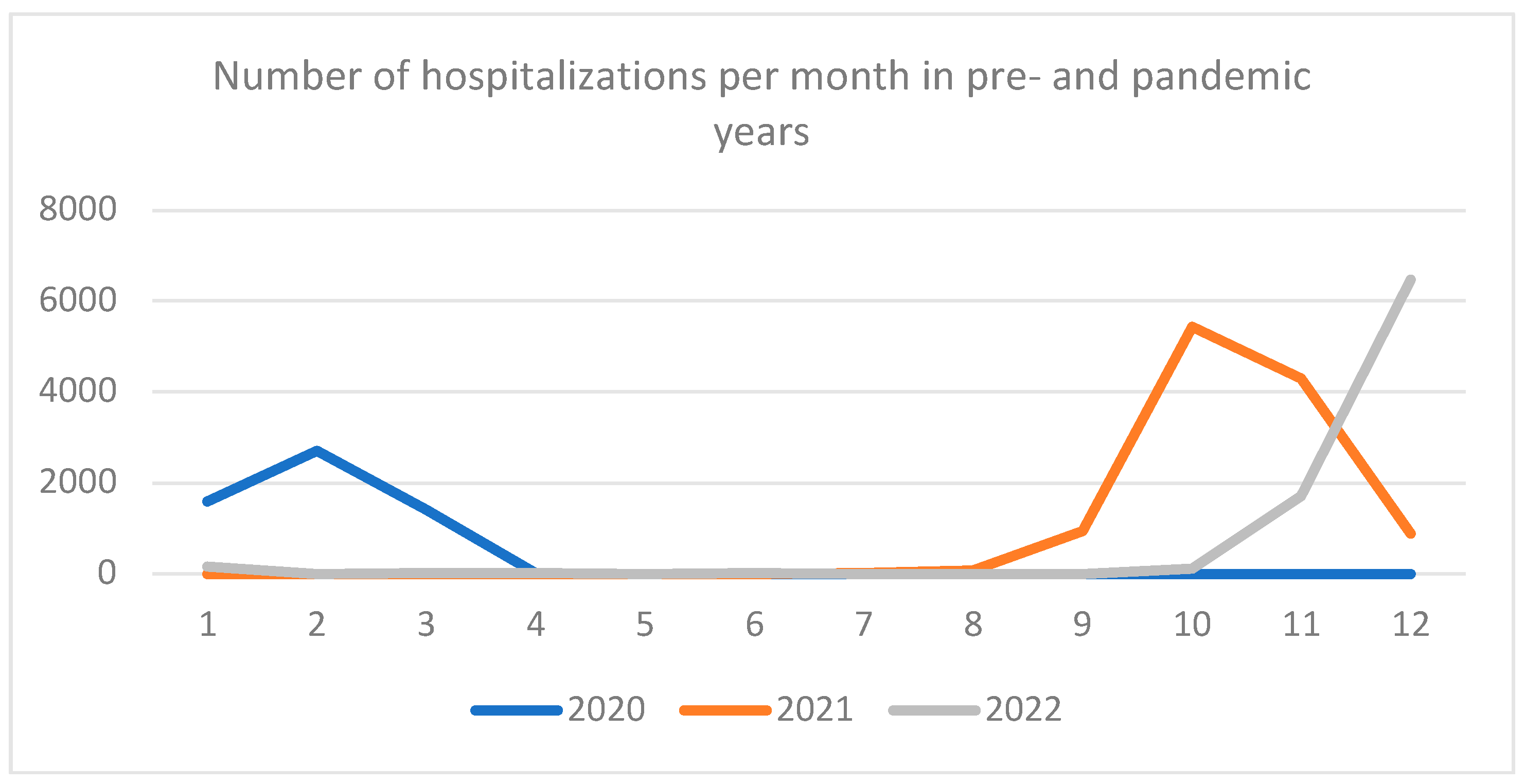
5.1.2. RSV-Related Hospitalizations
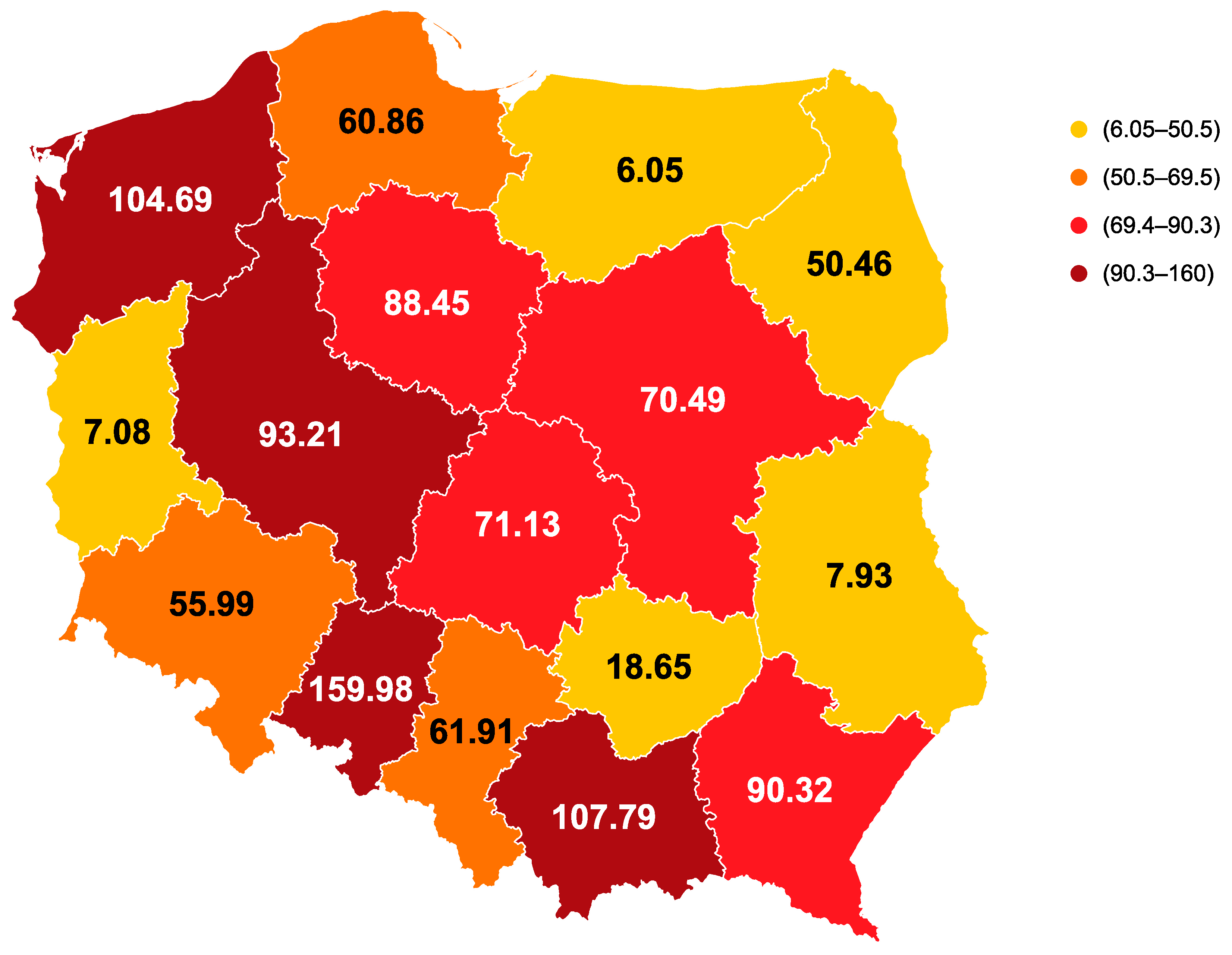
5.1.3. Outpatient Burden of RSV Disease
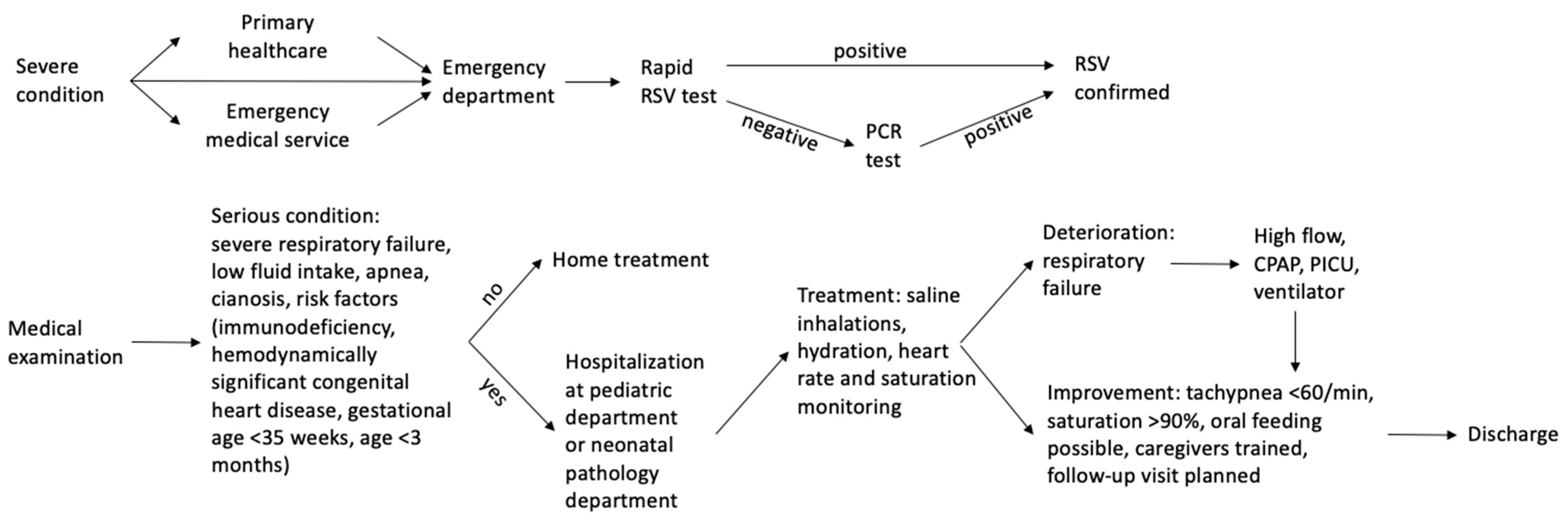
5.1.4. Patient Pathway
5.2. Management of RSV Infections
5.3. Prevention of RSV Infections
5.4. Epidemiology and Surveillance of RSV in Poland
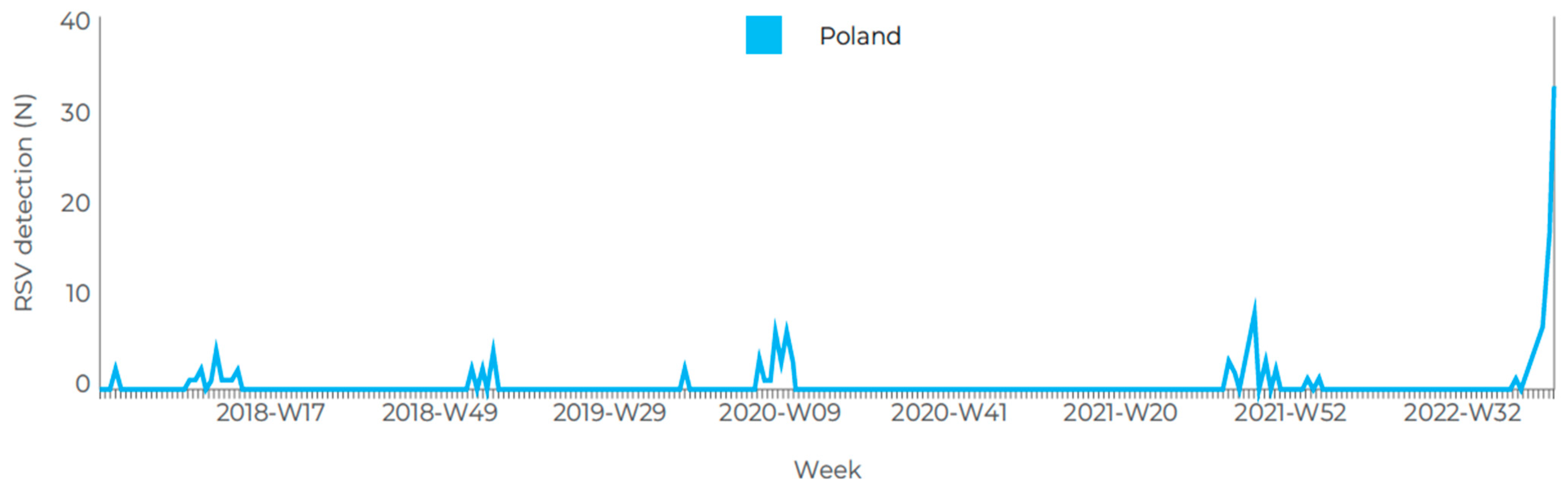
5.4.1. Seasonality of RSV Disease
5.4.2. Surveillance of RSV Infections
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARTI | acute respiratory tract infection |
| COVID-19 | coronavirus disease 2019 |
| EMA | European Medicines Agency |
| HFNC | high-flow nasal cannula |
| ICD-10 | International Classification of Diseases, Tenth Revision |
| PCR | polymerase chain reaction |
| RSV | respiratory syncytial virus |
References
- De Conto, F.; Conversano, F.; Medici, M.C.; Ferraglia, F.; Pinardi, F.; Arcangeletti, M.C.; Chezzi, C.; Calderaro, A. Epidemiology of human respiratory viruses in children with acute respiratory tract infection in a 3-year hospital-based survey in Northern Italy. Diagn. Microbiol. Infect. Dis. 2019, 94, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Tabatabai, J.; Ihling, C.M.; Manuel, B.; Rehbein, R.M.; Schnee, S.V.; Hoos, J.; Pfeil, J.; Grulich-Henn, J.; Schnitzler, P. Viral Etiology and Clinical Characteristics of Acute Respiratory Tract Infections in Hospitalized Children in Southern Germany (2014–2018). Open Forum Infect. Dis. 2023, 10, ofad110. [Google Scholar] [CrossRef]
- Takashima, M.D.; Grimwood, K.; Sly, P.D.; Lambert, S.B.; Chappell, K.J.; Watterson, D.; Ware, R.S. Epidemiology of respiratory syncytial virus in a community birth cohort of infants in the first 2 years of life. Eur. J. Pediatr. 2021, 180, 2125–2135. [Google Scholar] [CrossRef] [PubMed]
- Rząd, M.; Kanecki, K.; Lewtak, K.; Tyszko, P.; Szwejkowska, M.; Goryński, P.; Nitsch-Osuch, A. Human respiratory syncytial virus infections among hospitalized children in Poland during 2010–2020: Study based on the national hospital registry. J. Clin. Med. 2022, 11, 6451. [Google Scholar] [CrossRef] [PubMed]
- Glezen, W.P.; Taber, L.H.; Frank, A.L.; Kasel, J.A. Risk of primary infection and reinfection with respiratory syncytial virus. Am. J. Dis. Child. 1986, 140, 543–546. [Google Scholar] [CrossRef]
- Nair, H.; Nokes, D.J.; Gessner, B.D.; Dherani, M.; Madhi, S.A.; Singleton, R.J.; O’Brien, K.L.; Roca, A.; Wright, P.F.; Bruce, N.; et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: A systematic review and meta-analysis. Lancet 2010, 375, 1545–1555. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Black, C.P. Systematic review of the biology and medical management of respiratory syncytial virus infection. Respir. Care 2003, 48, 209–231. [Google Scholar]
- Crowe, J.E. Respiratory syncytial virus. In Nelson Textbook of Pediatrics, 20th ed.; Kliegman, R.M., Stanton, B.F., St. Geme, J.W., Schor, N.F., Eds.; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Rha, B.; Curns, A.T.; Lively, J.Y.; Campbell, A.P.; Englund, J.A.; Boom, J.A.; Azimi, P.H.; Weinberg, G.A.; Staat, M.A.; Selvarangan, R.; et al. Respiratory syncytial virus-associated hospitalizations among young children: 2015–2016. Pediatrics 2020, 146, e20193611. [Google Scholar] [CrossRef]
- Hall, C.B.; Weinberg, G.A.; Iwane, M.K.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Auinger, P.; Griffin, M.R.; Poehling, K.A.; Erdman, D.; et al. The burden of respiratory syncytial virus infection in young children. N. Engl. J. Med. 2009, 360, 588–598. [Google Scholar] [CrossRef]
- Hall, C.B.; Weinberg, G.A.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Schultz, A.F.; Poehling, K.A.; Szilagyi, P.G.; Griffin, M.R.; Williams, J.V.; et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics 2013, 132, e341–e348. [Google Scholar] [CrossRef] [PubMed]
- Lange, J.; Kozielski, J.; Bartolik, K.; Kabicz, P.; Targowski, T. Analysis of the incidence of acute respiratory diseases in the paediatric population in Poland in the light of the “Health Needs Map”. Adv. Respir. Med. 2020, 88, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Cegielska, K.; Pogonowska, M.; Kalicki, B. An analysis of respiratory syncytial virus infections in children up to 24 months old hospitalized in the Department of Paediatrics, Paediatric Nephrology and Allergology of the Military Institute of Medicine between 2016 and 2017. Pediatr. Med. Rodz. 2018, 14, 69–77. [Google Scholar] [CrossRef]
- Pancer, K.; Ciaćka, A.; Gut, W.; Lipka, B.; Mierzejewska, J.; Milewska-Bobula, B.; Smorczewska-Kiljan, A.; Jahnz-Rózyk, K.; Dzierzanowska, D.; Madaliński, K.; et al. Infections caused by RSV among children and adults during two epidemic seasons. Pol. J. Microbiol. 2011, 60, 253–258. [Google Scholar] [CrossRef]
- Pancer, K.W.; Gut, W.; Abramczuk, E.; Lipka, B.; Litwińska, B. Non-influenza viruses in acute respiratory infections among young children. High prevalence of HMPV during the H1N1V.2009 pandemic in Poland. Przegl. Epidemiol. 2014, 68, 627–632. [Google Scholar] [PubMed]
- Wrotek, A.; Czajkowska, M.; Jackowska, T. Seasonality of Respiratory Syncytial Virus Hospitalization. Adv. Exp. Med. Biol. 2020, 1279, 93–100. [Google Scholar] [CrossRef]
- Homaira, N.; Oei, J.L.; Mallitt, K.A.; Abdel-Latif, M.E.; Hilder, L.; Bajuk, B.; Lui, K.; Ferson, M.; Nurkic, A.; Chambers, G.M.; et al. High burden of RSV hospitalization in very young children: A data linkage study. Epidemiol. Infect. 2016, 144, 1612–1621. [Google Scholar] [CrossRef]
- Stein, R.T.; Bont, L.J.; Zar, H.; Polack, F.P.; Park, C.; Claxton, A.; Borok, G.; Butylkova, Y.; Wegzyn, C. Respiratory syncytial virus hospitalization and mortality: Systematic review and meta-analysis. Pediatr. Pulmonol. 2017, 52, 556–569. [Google Scholar] [CrossRef]
- Del Riccio, M.; Spreeuwenberg, P.; Osei-Yeboah, R.; Johannesen, C.K.; Vazquez Fernandez, L.; Teirlinck, A.C.; Wang, X.; Heikkinen, T.; Bangert, M.; Caini, S.; et al. Defining the Burden of Disease of RSV in the European Union: Estimates of RSV-associated hospitalisations in children under 5 years of age. A systematic review and modelling study. J. Infect. Dis. 2023, jiad188. [Google Scholar] [CrossRef]
- Wrotek, A.; Czajkowska, M.; Jackowska, T. Nosocomial infections in patients hospitalized with respiratory syncytial virus: A practice review. Adv. Exp. Med. Biol. 2020, 1271, 1–10. [Google Scholar] [CrossRef]
- Pogonowska, M.; Guzek, A.; Goscinska, A.; Rustecka, A.; Kalicki, B. Compensatory epidemic of RSV infections during the COVID-19 pandemic. An analysis of infections in children hospitalised in the Department of Paediatrics, Paediatric Nephrology and Allergology of the Military Medical Institute in Warsaw in 2020–2021. Pediatr. Med. Rodz.-Paediatr. Fam. Med. 2022, 18, 52–57. [Google Scholar] [CrossRef]
- Mapa Potrzeb Zdrowotnych w Zakresie Lecznictwa Szpitalnego dla Polski. Available online: https://mpz.mz.gov.pl/wp-content/uploads/2019/06/17_polska.pdf (accessed on 19 June 2019).
- Qiu, W.; Zheng, C.; Huang, S.; Zhang, Y.; Chen, Z. Epidemiological trend of RSV infection before and during COVID-19 pandemic: A three-year consecutive study in China. Infect. Drug Resist. 2022, 15, 6829–6837. [Google Scholar] [CrossRef]
- Casalegno, J.S.; Ploin, D.; Cantais, A.; Masson, E.; Bard, E.; Valette, M.; Fanget, R.; Targe, S.C.; Myar-Dury, A.F.; Doret-Dion, M.; et al. Characteristics of the delayed respiratory syncytial virus epidemic, 2020/2021, Rhône Loire, France. Euro Surveill 2021, 26, 2100630. [Google Scholar] [CrossRef] [PubMed]
- Fourgeaud, J.; Toubiana, J.; Chappuy, H.; Delacourt, C.; Moulin, F.; Parize, P.; Scemla, A.; Abid, H.; Leruez-Ville, M.; Frange, P. Impact of public health measures on the post-COVID-19 respiratory syncytial virus epidemics in France. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2389–2395. [Google Scholar] [CrossRef] [PubMed]
- Pruccoli, G.; Castagno, E.; Raffaldi, I.; Denina, M.; Barisone, E.; Baroero, L.; Timeus, F.; Rabbone, I.; Monzani, A.; Terragni, G.M.; et al. The importance of RSV epidemiological surveillance: A multicenter observational study of RSV infection during the COVID-19 pandemic. Viruses 2023, 15, 280. [Google Scholar] [CrossRef] [PubMed]
- Cieślak, K.; Kowalczyk, D.; Szymański, K.; Hallmann-Szelińska, E.; Brydak, L.B. Influenza and influenza-like viruses: Frequent infections in children under 14 years of age during the 2016/2017 epidemic season. Adv. Exp. Med. Biol. 2018, 1114, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Hallmann-Szelińska, E.; Bednarska, K.; Kondratiuk, K.; Rabczenko, D.; Brydak, L.B. Viral infections in children in the 2014/2015 epidemic season in Poland. Adv. Exp. Med. Biol. 2016, 912, 51–56. [Google Scholar] [CrossRef]
- Woźniak-Kosek, A.; Czarkowski, M.P.; Staszewska, E.; Kondej, B.; Brydak, L.B. Grypa w Polsce w 2010 roku. Przegl. Epidemiol. 2012, 66, 599–604. [Google Scholar]
- Kondratiuk, K.; Czarkowski, M.P.; Hallmann-Szelińska, E.; Staszewska, E.; Bednarska, K.; Cielebąk, E.; Brydak, L.B. Influenza in Poland in 2013 and 2013/2014 epidemic season. Przegl. Epidemiol. 2016, 70, 407–419. [Google Scholar]
- Bednarska, K.; Hallmann-Szelińska, E.; Kondratiuk, K.; Brydak, L.B. Evaluation of the activity of influenza and influenza-like viruses in the epidemic season 2013/2014. Adv. Exp. Med. Biol. 2015, 857, 1–7. [Google Scholar] [CrossRef]
- Bednarska, K.; Hallmann-Szelińska, E.; Kondratiuk, K.; Brydak, L.B. Antigenic drift of A/H3N2/virus and circulation of influenza-like viruses during the 2014/2015 influenza season in Poland. Adv. Exp. Med. Biol. 2016, 905, 33–38. [Google Scholar] [CrossRef]
- Byambasuren, S.; Paradowska-Stankiewicz, I.; Brydak, L.B. Epidemic influenza seasons from 2008 to 2018 in Poland: A focused review of virological characteristics. Adv. Exp. Med. Biol. 2020, 1251, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Czarkowski, M.P.; Hallmann-Szelińska, E.; Staszewska, E.; Bednarska, K.; Kondratiuk, K.; Brydak, L.B. Influenza in Poland in 2011-2012 and in 2011/2012 and 2012/2013 epidemic seasons. Przegl. Epidemiol. 2014, 68, 455–463, 559–565. [Google Scholar] [PubMed]
- Łuniewska, K.; Szymański, K.; Hallmann-Szelińska, E.; Kowalczyk, D.; Sałamatin, R.; Masny, A.; Brydak, L.B. Infections caused by influenza viruses among children in Poland during the 2017/18 epidemic season. Adv. Exp. Med. Biol. 2019, 1211, 97–102. [Google Scholar] [CrossRef]
- Liczba zachorowań i zapadalność na 100 tys. ludności., Zakład Epidemiologii Chorób Zakaźnych i Nadzoru NIZP PZH—PIB Departament Przeciwepidemiczny i Ochrony Sanitarnej Granic GIS, Choroby zakaźne i zatrucia w Polsce—2023 r. Available online: http://wwwold.pzh.gov.pl/oldpage/epimeld/2023/index_mp.html (accessed on 30 April 2023).
- Xing, Y.; Proesmans, M. New therapies for acute RSV infections: Where are we? Eur. J. Pediatr. 2019, 178, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Hryniewicz, W.; Albrecht, P.; Radzikowski, A. Rekomendacje Postępowania w Pozaszpitalnych Zakażeniach Układu Oddechowego; Narodowy Instytut Leków: Warszawa, Poland, 2016. [Google Scholar]
- Franklin, D.; Babl, F.E.; Schlapbach, L.J.; Oakley, E.; Craig, S.; Neutze, J.; Furyk, J.; Fraser, J.F.; Jones, M.; Whitty, J.A.; et al. A randomized trial of high-flow oxygen therapy in infants with bronchiolitis. N. Engl. J. Med. 2018, 378, 1121–1131. [Google Scholar] [CrossRef]
- Franklin, D.; Shellshear, D.; Babl, F.E.; Hendrickson, R.; Williams, A.; Gibbons, K.; McEnery, K.; Kennedy, M.; Pham, T.M.; Acworth, J.; et al. High flow in children with respiratory failure: A randomised controlled pilot trial—A paediatric acute respiratory intervention study. J. Paediatr. Child. Health 2021, 57, 273–281. [Google Scholar] [CrossRef]
- Kwon, J.W. High-flow nasal cannula oxygen therapy in children: A clinical review. Clin. Exp. Pediatr. 2020, 63, 3–7. [Google Scholar] [CrossRef]
- Ralston, S.L.; Lieberthal, A.S.; Meissner, H.C.; Alverson, B.K.; Baley, J.E.; Gadomski, A.M.; Johnson, D.W.; Light, M.J.; Maraqa, N.F.; Mendonca, E.A.; et al. Clinical practice guideline: The diagnosis, management, and prevention of bronchiolitis. Pediatrics 2014, 134, e1474–e1502. [Google Scholar] [CrossRef]
- Fedorczak, A.; Zielińska, N.; Nosek-Wasilewska, P.; Mikołajczyk, K.; Lisiak, J.; Zeman, K.; Tkaczyk, M. Comparison of COVID-19 and RSV infection courses in infants and children under 36 months hospitalized in paediatric department in fall and winter season 2021/2022. J. Clin. Med. 2022, 11, 7088. [Google Scholar] [CrossRef]
- Sosnowska, J.; Konarska, Z.; Feleszko, W. Real life management of RSV bronchiolitis and comparison with existing practice guidelines. In Proceedings of the European Academy of Allergy and Clinical Immunology Congress, Vienna, Austria, 11–15 June 2016. [Google Scholar] [CrossRef]
- Haładaj, K.; Fijałkowski, B.; Chlebna-Sokół, D. Clinical aspects and treatment of respiratory syncytial virus infection in infants in the first 6 months of life. Przegl. Epidemiol. 2011, 65, 605–608. (In Polish) [Google Scholar] [PubMed]
- Wrotek, A.; Czajkowska, M.; Jackowska, T. Antibiotic treatment in patients with bronchiolitis. Adv. Exp. Med. Biol. 2019, 1211, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Wrotek, A.; Czajkowska, M.; Jackowska, T. Chest radiography in children hospitalized with bronchiolitis. Adv. Exp. Med. Biol. 2019, 1222, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Kusak, B.; Grzesik, E.; Konarska-Gabryś, K.; Pacek, Z.; Piwowarczyk, B.; Lis, G. Bronchiolitis in children—Do we choose wisely? Dev. Period Med. 2018, 22, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Rogovik, A.L.; Carleton, B.; Solimano, A.; Goldman, R.D. Palivizumab for the prevention of respiratory syncytial virus infection. Can. Fam. Physician 2010, 56, 769–772. [Google Scholar]
- Helwich, E.; Miszczak-Knecht, M.; Sands, D.; Emich-Widera, E. Stanowisko ekspertów dotyczące rozszerzenia wskazań do profilaktyki ciężkich infekcji wirusem syncytium nabłonka oddechowego (RSV) za pomocą paliwizumabu u noworodków i niemowląt. Stand. Med./Pediatr. 2022, 19, 549–555. [Google Scholar]
- Keam, S.J. Nirsevimab: First Approval. Drugs 2023, 83, 181–187. [Google Scholar] [CrossRef]
- Hammitt, L.L.; Dagan, R.; Yuan, Y.; Baca Cots, M.; Bosheva, M.; Madhi, S.A.; Muller, W.J.; Zar, H.J.; Brooks, D.; Grenham, A.; et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N. Engl. J. Med. 2022, 386, 837–846. [Google Scholar] [CrossRef]
- Álvarez García, F.J.; Cilleruelo Ortega, M.J.; Álvarez Aldeán, J.; Garcés-Sánchez, M.; Garrote Llanos, E.; Iofrío de Arce, A.; Montesdeoca Melián, A.; Navarro Gómez, M.L.; Pineda Solas, V.; Rivero Calle, I.; et al. Immunisation schedule of the Spanish Association of Paediatrics: 2023 Recommendations. An. Pediatr. (Engl. Ed.) 2023, 98, 58.e1–58.e10. [Google Scholar] [CrossRef]
- Stratégie de Prévention des Bronchiolites à VRS des Nourrissons Avis des Sociétés Savantes Françaises de Pédiatrie. Available online: https://www.infovac.fr/docman-marc/public/bulletins/2023/1869-lien-1-strategie-de-prevention-des-bronchiolites-a-vrs-des-nourrissons/file (accessed on 30 April 2023).
- Sun, M.; Lai, H.; Na, F.; Li, S.; Qiu, X.; Tian, J.; Zhang, Z.; Ge, L. Monoclonal Antibody for the Prevention of Respiratory Syncytial Virus in Infants and Children A Systematic Review and Network Meta-analysis. JAMA Netw. Open 2023, 6, e230023. [Google Scholar] [CrossRef]
- Chuang, Y.C.; Lin, K.P.; Wang, L.A.; Yeh, T.K.; Liu, P.Y. The impact of the COVID-19 pandemic on respiratory syncytial virus infection: A narrative review. Infect. Drug Resist. 2023, 16, 661–675. [Google Scholar] [CrossRef]
- Eden, J.S.; Sikazwe, C.; Xie, R.; Deng, Y.M.; Sullivan, S.G.; Michie, A.; Levy, A.; Cutmore, E.; Blyth, C.C.; Britton, P.N.; et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat. Commun. 2022, 13, 2884. [Google Scholar] [CrossRef] [PubMed]
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. Impact of COVID-19 on the changing patterns of respiratory syncytial virus infections. Infect. Dis. Rep. 2022, 14, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Davis, P.B.; Berger, N.A.; Kaelber, D.C.; Volkow, N.D.; Xu, R. Disruption in seasonality, patient characteristics and disparities of respiratory syncytial virus infection among young children in the US during and before the COVID-19 pandemic: 2010–2022. medRxiv 2022, 2022.11.29.22282887. [Google Scholar] [CrossRef]
- Bermúdez Barrezueta, L.; Matías Del Pozo, V.; López-Casillas, P.; Brezmes Raposo, M.; Gutiérrez Zamorano, M.; Pino Vázquez, M.A. Variation in the seasonality of the respiratory syncytial virus during the COVID-19 pandemic. Infection 2022, 50, 1001–1005. [Google Scholar] [CrossRef]
- Bozzola, E.; Barni, S.; Villani, A. Respiratory syncytial virus pediatric hospitalization in the COVID-19 era. Int. J. Environ. Res. Public Health 2022, 19, 15455. [Google Scholar] [CrossRef] [PubMed]
- Istel, M. Zakażenia RSV: Jak ich przybywa w Polsce i Europie. Konkret 24. 2023. Available online: https://konkret24.tvn24.pl/zdrowie/grypa-rsv-koronawirus-zakazenia-rsv-jak-przybywa-w-polsce-i-europie-6592401 (accessed on 4 January 2023).
- Wrotek, A.; Badyda, A.; Czechowski, P.O.; Owczarek, T.; Dąbrowiecki, P.; Jackowska, T. Air pollutants’ concentrations are associated with increased number of RSV hospitalizations in Polish children. J. Clin. Med. 2021, 10, 3224. [Google Scholar] [CrossRef]
- Jenkins, V.A.; Hoet, B.; Hochrein, H.; De Moerlooze, L. The quest for a respiratory syncytial virus vaccine for older adults: Thinking beyond the F protein. Vaccines 2023, 11, 382. [Google Scholar] [CrossRef]
- Obando-Pacheco, P.; Justicia-Grande, A.J.; Rivero-Calle, I.; Rodríguez-Tenreiro, C.; Sly, P.; Ramilo, O.; Mejías, A.; Baraldi, E.; Papadopoulos, N.G.; Nair, H.; et al. Respiratory syncytial virus seasonality: A global overview. J. Infect. Dis. 2018, 217, 1356–1364. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Broberg, E.K.; Campbell, H.; Nair, H.; European RSV Surveillance Network. Seasonality of respiratory syncytial virus and its association with meteorological factors in 13 European countries, week 40 2010 to week 39 2019. Euro Surveill 2022, 27, 2100619. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Publication | Epidemic Season | Proportion of RSV-Positive Samples in All Positive Non-Influenza Samples | Population |
|---|---|---|---|
| Kondratiuk et al. [31] | 2013/14 | 84% | General |
| Hallmann et al. [29] | 2014/15 | 96.2% | Pediatric |
| Woźniak-Kosek et al. [30] | 2010 | 66.7% | General |
| Czarkowski et al. [35] | 2011/12 | 87.5% | General |
| Bednarska et al. [33] | 2012/13 | 87% | General |
| Byambasuren et al. [34] | 2008/09 | 54.6% | General |
| Byambasuren et al. [34] | 2009/10 | 56.7% | General |
| Byambasuren et al. [34] | 2010/11 | 74% | General |
| Byambasuren et al. [34] | 2011/12 | 86.7% | General |
| Byambasuren et al. [34] | 2012/13 | 87% | General |
| Byambasuren et al. [34] | 2013/14 | 84.5% | General |
| Byambasuren et al. [34] | 2014/15 | 91.4% | General |
| Byambasuren et al. [34] | 2015/16 | 77.5% | General |
| Byambasuren et al. [34] | 2016/17 | 87.5% | General |
| Byambasuren et al. [34] | 2017/18 | 63.1% | General |
| Study | Inhaled Corticosteroids | Systemic Corticosteroids | Bronchodilator | Antibiotics | Chest X-ray | Supportive Care Only |
|---|---|---|---|---|---|---|
| Pogonowska et al. [22] | 85.2% | 55.7% | 90.2% | 100% | NA | NA |
| Fedorczak et al. [44] | 60.5% | 25.6% | 88.4% | 44.2% | NA | 2.3% |
| Cegielska et al. [14] | 66% | 34% | 93% | 69% | 75% | NA |
| Sosnowska et al. [45] | 12.2% | 6.1% | NA | 31.6% | 31.6% | NA |
| Haładaj et al. [46] | 87.5% (budesonide) | NA | NA | 93.7% | NA | NA |
| Wrotek et al. [47] | NA | NA | NA | 16% | NA | NA |
| Wrotek et al. [48] | NA | NA | NA | NA | 61% | NA |
| Kusak et al. [49] | 62.1% | 86.4% | 62.1% | 95.3% | NA | |
| Seasons | Inclusion Criteria |
|---|---|
| 2008–2009 | Children with BPD: |
| |
| 2009–2013 | Children with BPD: |
| |
| 2013–2018 | Children aged < 1 year and: |
| |
| 2018–February 2023 | Children: |
| |
| Since March 2023 | Children: |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borszewska-Kornacka, M.K.; Mastalerz-Migas, A.; Nitsch-Osuch, A.; Jackowska, T.; Paradowska-Stankiewicz, I.; Kuchar, E.; Mazela, J.; Helwich, E.; Czech, M.; Lauterbach, R.; et al. Respiratory Syncytial Virus Infections in Polish Pediatric Patients from an Expert Perspective. Vaccines 2023, 11, 1482. https://doi.org/10.3390/vaccines11091482
Borszewska-Kornacka MK, Mastalerz-Migas A, Nitsch-Osuch A, Jackowska T, Paradowska-Stankiewicz I, Kuchar E, Mazela J, Helwich E, Czech M, Lauterbach R, et al. Respiratory Syncytial Virus Infections in Polish Pediatric Patients from an Expert Perspective. Vaccines. 2023; 11(9):1482. https://doi.org/10.3390/vaccines11091482
Chicago/Turabian StyleBorszewska-Kornacka, Maria K., Agnieszka Mastalerz-Migas, Aneta Nitsch-Osuch, Teresa Jackowska, Iwona Paradowska-Stankiewicz, Ernest Kuchar, Jan Mazela, Ewa Helwich, Marcin Czech, Ryszard Lauterbach, and et al. 2023. "Respiratory Syncytial Virus Infections in Polish Pediatric Patients from an Expert Perspective" Vaccines 11, no. 9: 1482. https://doi.org/10.3390/vaccines11091482