
COVID-19 Mortality in Vaccinated vs. Unvaccinated Liver & Kidney Transplant Recipients: A Single-Center United States Propensity Score Matching Study on Historical Data
 , ,
, , 
Abstract
:1. Introduction
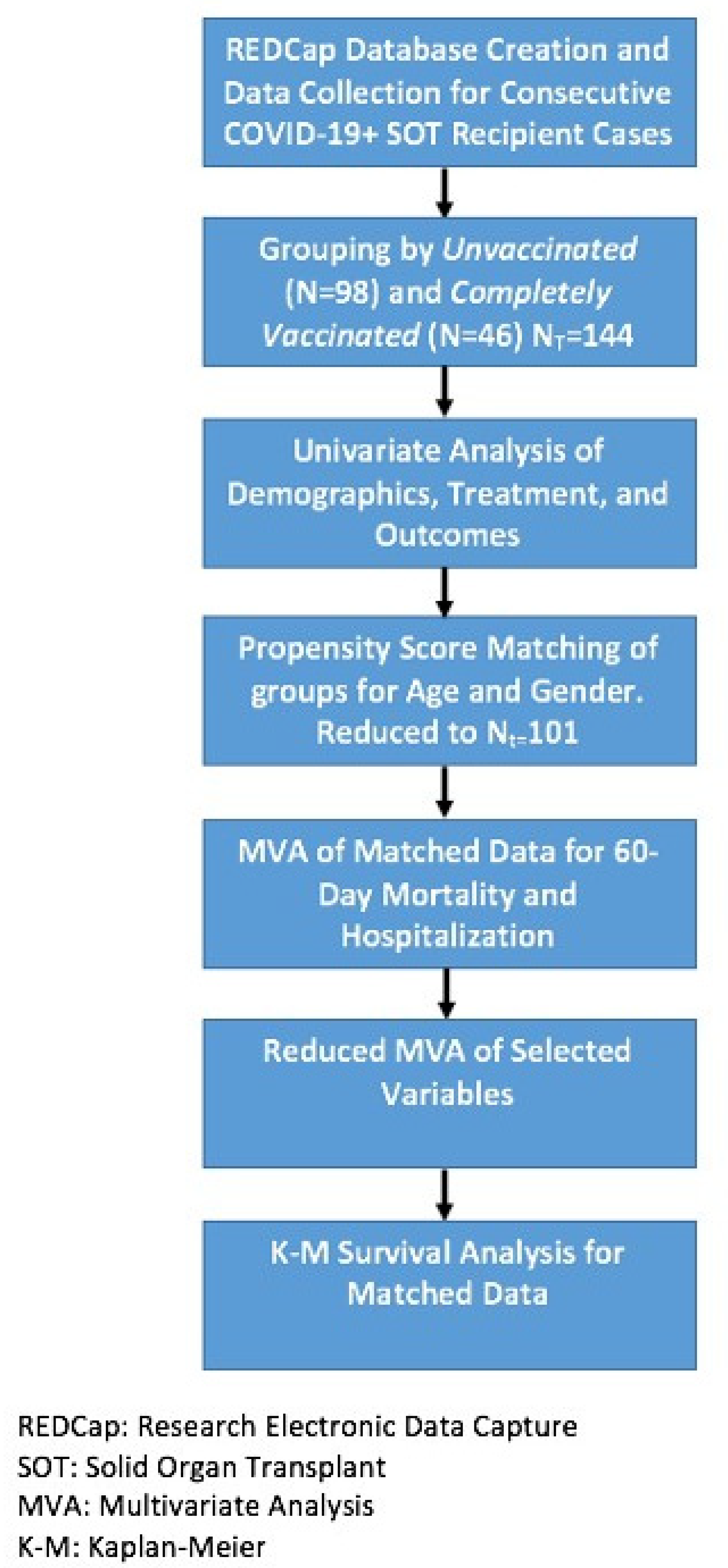
2. Methods
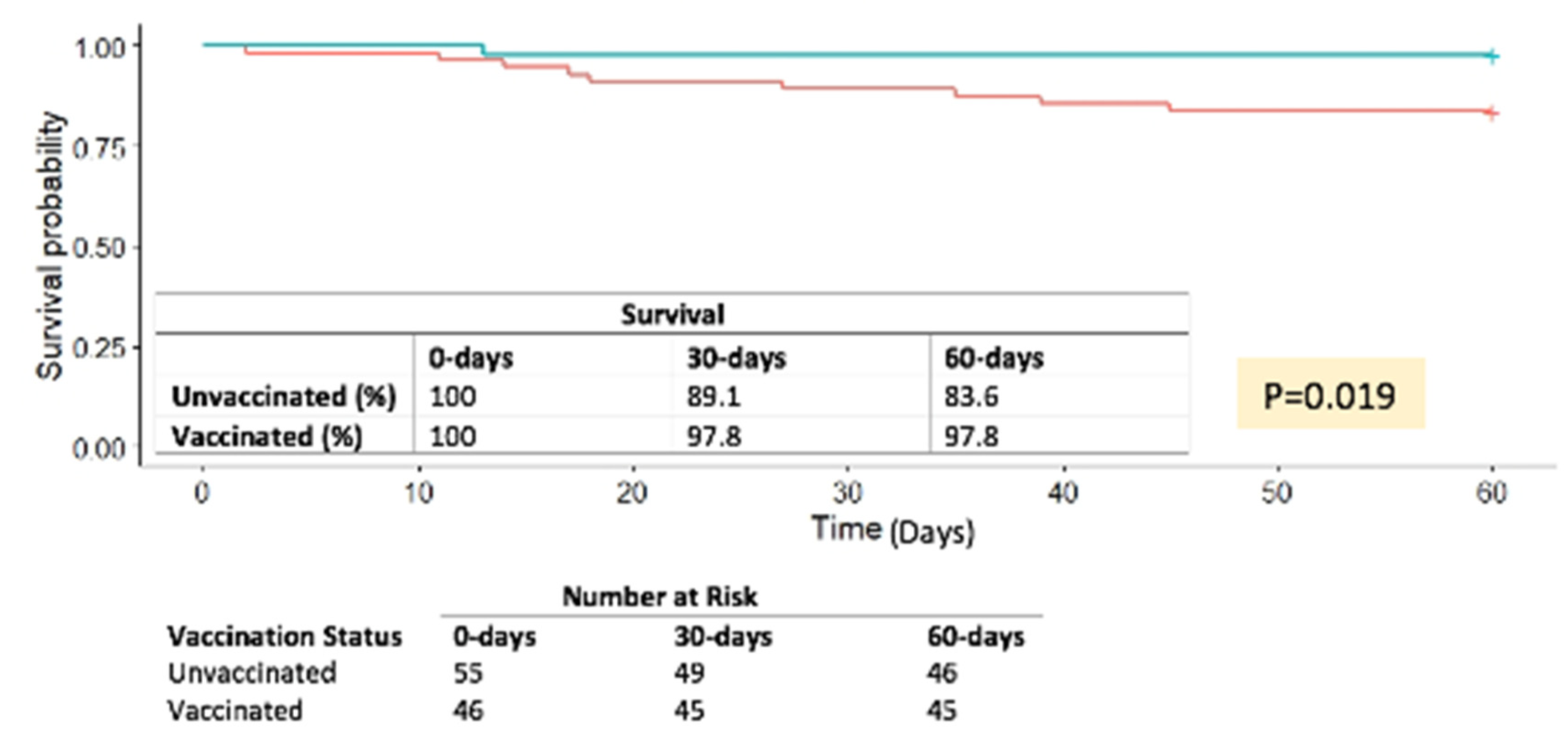
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus Disease 2019 |
| Mab | monoclonal antibody |
| OR | odds ratio |
| PSM | propensity score matching analysis |
| SLK | simultaneous liver kidney transplant |
| SOT | solid organ transplant |
References
- Ward, H.; Whitaker, M.; Flower, B.; Tang, S.N.; Atchison, C.; Darzi, A.; Donnelly, C.A.; Cann, A.; Diggle, P.J.; Ashby, D.; et al. Population antibody responses following COVID-19 vaccination in 212,102 individuals. Nat. Commun. 2022, 13, 907. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Stoesser, N.; Matthews, P.C.; Ayoubkhani, D.; Studley, R.; Bell, I.; Bell, J.I.; Newton, J.N.; Farrar, J.; Diamond, I.; et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nat. Microbiol. 2021, 6, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Hardgrave, H.O.T.; Bhusal, S.; Rude, M.K.; Sharma, A.; Gonzalez, M.; Khan, N.; Deneke, M.; Thandassery, R.; Patel, R.; Dare, R.; et al. The Impact of Transplant Type, Age, and Immunosuppresion on Post COVID-19 Infection Survival: A Single Center United States Prospective Cohort Study. Transpl. Int. 2021, 34, 349. [Google Scholar]
- Giorgakis, E.; Zehtaban, S.P.; Stevens, A.E.; Bhusal, S.; Burdine, L. COVID-19 in solid organ transplant recipients. Transpl. Infect. Dis. 2021, 23, e13419. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Ou, M.T.; Greenberg, R.S.; Teles, A.T.; Werbel, W.A.; Avery, R.K.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Safety of the First Dose of SARS-CoV-2 Vaccination in Solid Organ Transplant Recipients. Transplantation 2021, 105, e56–e57. [Google Scholar] [CrossRef]
- Ou, M.T.; Boyarsky, B.J.; Motter, J.D.; Greenberg, R.S.; Teles, A.T.; Ruddy, J.A.; Krach, M.R.; Jain, V.S.; Werbel, W.A.; Avery, R.K.; et al. Safety and Reactogenicity of 2 Doses of SARS-CoV-2 Vaccination in Solid Organ Transplant Recipients. Transplantation 2021, 105, 2170–2174. [Google Scholar] [CrossRef]
- Ravanan, R.; Mumford, L.; Ushiro-Lumb, I.; Callaghan, C.; Pettigrew, G.; Thorburn, D.; Gardiner, D.; Forsythe, J.; OTDT Clinical Team. Two Doses of SARS-CoV-2 Vaccines Reduce Risk of Death Due to COVID-19 in Solid Organ Transplant Recipients: Preliminary Outcomes From a UK Registry Linkage Analysis. Transplantation 2021, 105, e263–e264. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Barbur, I.; Chiang, T.P.; Ou, M.T.; Greenberg, R.S.; Teles, A.T.; Krach, M.R.; López, J.I.; Garonzik-Wang, J.M.; Avery, R.K.; et al. SARS-CoV-2 Messenger RNA Vaccine Immunogenicity in Solid Organ Transplant Recipients With Prior COVID-19. Transplantation 2021, 105, e270–e271. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Aslam, S.; Adler, E.; Mekeel, K.; Little, S.J. Clinical effectiveness of COVID-19 vaccination in solid organ transplant recipients. Transpl. Infect. Dis. 2021, 23, e13705. [Google Scholar] [CrossRef]
- Hasan, L.H.H.; Dare, R.; Giorgakis, E. Risk Factors for Hospital Admissions after Monoclonal Antibodies for COVID-19 Infection in Solid Organ Transplant Recipients. Transpl. Int. 2021, 34, 265–266. [Google Scholar]
- Sarrell, B.A.; Bloch, K.; El Chediak, A.; Kumm, K.; Tracy, K.; Forbes, R.C.; Langone, A.; Thomas, L.; Schlendorf, K.; Trindade, A.J.; et al. Monoclonal antibody treatment for COVID-19 in solid organ transplant recipients. Transpl. Infect. Dis. 2022, 24, e13759. [Google Scholar] [CrossRef]
- Wang, A.X.; Busque, S.; Kuo, J.; Singh, U.; Röeltgen, K.; Pinsky, B.A.; Chertow, G.M.; Scandling, J.D.; Lenihan, C.R. SARS-CoV-2 Neutralizing Monoclonal Antibodies for the Treatment of COVID-19 in Kidney Transplant Recipients. Kidney360 2022, 3, 133–143. [Google Scholar] [CrossRef]
- Yetmar, Z.A.; Beam, E.; O’Horo, J.C.; Ganesh, R.; Bierle, D.M.; Brumble, L.; Seville, M.T.; Razonable, R.R. Monoclonal Antibody Therapy for COVID-19 in Solid Organ Transplant Recipients. Open Forum Infect. Dis. 2021, 8, ofab255. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.Y.; Luo, J.C.; Su, Y.; Zhang, Y.J.; Tu, G.W.; Luo, Z. Propensity score matching with R: Conventional methods and new features. Ann. Transl. Med. 2021, 9, 812. [Google Scholar] [CrossRef] [PubMed]
- Hardgrave, A.W.H.; Night, J.; Klutts, G.; Krinock, D.; Osborn, T.; Bhusal, S.; Rude, M.K.; Burdine, L.; Giorgakis, E. COVID-19 Mortality in Vaccinated vs. Unvaccinated Solid Organ Transplant Recipients: A Single Center United States Propensity Score Matching Study. In Proceedings of the Transplantation Society 2022 Congress, Buenos Aires, Argentina, 10–14 September 2022. [Google Scholar]
- Salto-Alejandre, S.; Jiménez-Jorge, S.; Sabé, N.; Ramos-Martínez, A.; Linares, L.; Valerio, M.; Martín-Dávila, P.; Fernández-Ruiz, M.; Fariñas, M.C.; Blanes-Juliá, M.; et al. Risk factors for unfavorable outcome and impact of early post-transplant infection in solid organ recipients with COVID-19: A prospective multicenter cohort study. PLoS ONE 2021, 16, e0250796. [Google Scholar] [CrossRef]
- Yanez, N.D.; Weiss, N.S.; Romand, J.A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef] [PubMed]
- Nair, V.; Jandovitz, N.; Hirsch, J.S.; Nair, G.; Abate, M.; Bhaskaran, M.; Grodstein, E.; Berlinrut, I.; Hirschwerk, D.; Cohen, S.L.; et al. COVID-19 in kidney transplant recipients. Am. J. Transplant. 2020, 20, 1819–1825. [Google Scholar] [CrossRef]
- Okumura, K.; Nishida, S.; Dhand, A. Trends in COVID-19 Mortality Among Solid Organ Transplant Recipients: Implications for Prevention. Transplantation 2022, 106, e380–e381. [Google Scholar] [CrossRef]
- Schoot, T.S.; Kerckhoffs, A.P.M.; Hilbrands, L.B.; van Marum, R.J. Immunosuppressive Drugs and COVID-19: A Review. Front. Pharmacol. 2020, 11, 1333. [Google Scholar] [CrossRef]
- Werbel, W.A.; Boyarsky, B.J.; Ou, M.T.; Massie, A.B.; Tobian, A.A.R.; Garonzik-Wang, J.M.; Segev, D.L. Safety and Immunogenicity of a Third Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Ann. Intern. Med. 2021, 174, 1330–1332. [Google Scholar] [CrossRef]
- Hall, V.G.; Al-Alahmadi, G.; Solera, J.T.; Marinelli, T.; Cardinal, H.; Prasad, G.V.R.; De Serres, S.A.; Isaac, D.; Mainra, R.; Lamarche, C.; et al. Outcomes of SARS-CoV-2 Infection in Unvaccinated Compared With Vaccinated Solid Organ Transplant Recipients: A Propensity Matched Cohort Study. Transplantation 2022, 106, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients with Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063–1065. [Google Scholar] [CrossRef] [PubMed]
- Organization W.H. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 1 June 2022).
- Statistica. Rate of Coronavirus (COVID-19) Cases in the United States as of 1 June 2022, by State. Available online: https://www.statista.com/statistics/1109004/coronavirus-covid19-cases-rate-us-americans-by-state/ (accessed on 1 June 2022).
- Statistica. Death Rates from Coronavirus (COVID-19) in the United States as of 1 June 2022, by State. Available online: https://www.statista.com/statistics/1109011/coronavirus-covid19-death-rates-us-by-state/ (accessed on 1 June 2022).
- Foundation, N.K. Kidney Disease-Is Your State Hard Hit? Available online: https://www.kidney.org/news/newsroom/nr/KD_StateHardHit (accessed on 4 June 2022).
- Prevention CfDCa. Underlying Cause of Death 1999–2020. Available online: https://wonder.cdc.gov/wonder/help/ucd.html (accessed on 4 June 2022).



{kind=link}
{kind=link}
| Unvaccinated (N (%)) | Vaccinated (N (%)) | p | |
|---|---|---|---|
| N | 98 (68.06) | 46 (31.94) | |
| Age (mean (SD)) | 51.96 (13.53) | 49.48 (12.66) | 0.297 |
| Gender: | |||
| Male | 59 (60.20) | 23 (50.00) | 0.331 |
| Female | 39 (39.80) | 23 (50.00) | |
| Type of Transplant: | |||
| Liver | 21 (21.43) | 8 (17.39) | 0.805 |
| Kidney | 74 (75.51) | 36 (78.26) | |
| SLK | 3 (3.06) | 2 (4.35) | |
| Comorbidities: | |||
| Cancer | 3 (3.06) | 4 (8.70) | 0.294 |
| DM, HTN, Obesity * | 82 (83.67) | 4 (86.96) | 0.793 |
| CAD, CVA * | 12 (12.24) | 4 (8.70) | 0.728 |
| Mab Treatment | 18 (18.37) | 27 (58.70) | <0.001 |
| 60-day mortality | 11 (11.22) | 1 (2.17) | 0.131 |
| (a) | |||
|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p | |
| Vaccinated | 0.19 | 0.03–1.20 | 0.077 |
| Age | 1.22 | 1.11–1.33 | <0.001 |
| Female Sex | 0.13 | 0.03–0.53 | 0.005 |
| Kidney Transplant * | 40.93 | 4.53–370.12 | 0.001 |
| Mab Treatment | 0.06 | 0.01–0.57 | 0.014 |
| (b) | |||
| Vaccinated | 1.21 | 0.43–3.39 | 0.716 |
| Age | 1.05 | 1.01–1.10 | 0.018 |
| Female Sex | 0.55 | 0.21–1.45 | 0.223 |
| Kidney Transplant * | 5.65 | 1.12–28.28 | 0.036 |
| Mab Treatment | 0.62 | 0.20–1.86 | 0.385 |
| (a) | |||
|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p | |
| Vaccinated | 0.59 | 0.09–4.04 | 0.590 |
| Age | 1.23 | 1.09–1.38 | 0.001 |
| Female Gender | 0.12 | 0.02–0.67 | 0.017 |
| Kidney Transplant * | 50.57 | 3.92–651.83 | 0.003 |
| (b) | |||
| Vaccinated | 0.83 | 0.22–3.12 | 0.784 |
| Age | 1.06 | 1.00–1.13 | 0.048 |
| Female Gender | 0.60 | 0.17–2.13 | 0.423 |
| Kidney Transplant * | 5.4 | 0.79–37.17 | 0.085 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hardgrave, H.; Wells, A.; Nigh, J.; Klutts, G.; Krinock, D.; Osborn, T.; Bhusal, S.; Rude, M.K.; Burdine, L.; Giorgakis, E. COVID-19 Mortality in Vaccinated vs. Unvaccinated Liver & Kidney Transplant Recipients: A Single-Center United States Propensity Score Matching Study on Historical Data. Vaccines 2022, 10, 1921. https://doi.org/10.3390/vaccines10111921
Hardgrave H, Wells A, Nigh J, Klutts G, Krinock D, Osborn T, Bhusal S, Rude MK, Burdine L, Giorgakis E. COVID-19 Mortality in Vaccinated vs. Unvaccinated Liver & Kidney Transplant Recipients: A Single-Center United States Propensity Score Matching Study on Historical Data. Vaccines. 2022; 10(11):1921. https://doi.org/10.3390/vaccines10111921
Chicago/Turabian StyleHardgrave, Hailey, Allison Wells, Joseph Nigh, Garrett Klutts, Derek Krinock, Tamara Osborn, Sushma Bhusal, Mary K. Rude, Lyle Burdine, and Emmanouil Giorgakis. 2022. "COVID-19 Mortality in Vaccinated vs. Unvaccinated Liver & Kidney Transplant Recipients: A Single-Center United States Propensity Score Matching Study on Historical Data" Vaccines 10, no. 11: 1921. https://doi.org/10.3390/vaccines10111921