
Leaving No One Behind: Interventions and Outcomes of the COVID-19 Vaccine Maximising Uptake Programme

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. BNSSG CCG COVID-19 Maximising Uptake Programme
2.2. Study Design
- COVID-19 vaccine uptake data from BNSSG Clinical Commissioning Group (CCG) and vaccine update data among national priority subgroups from the national vaccination uptake data system from December 2020 to May 2021.
- Data on numbers, geographic locations and vaccinations delivered during the outreach and engagement activities supplied by the MUG leads, BNSSG CCG, and Sirona Care and Health (a local community healthcare provider).
- Routinely collected quantitative and qualitative data, supplied by the BNSSG CCG Insights and Engagement team, between December 2020 and May 2021, including before and after outreach/engagement brief surveys, online public engagement surveys and vaccination follow up interviews with people from vaccine priority cohorts. These engagement surveys and interviews were carried out before and after outreach clinics to explore people’s satisfaction with the vaccination clinics and identify areas for development to inform the organisation and delivery of future clinics.
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Engagement and Communication with People and Communities
3.2. Ourtreach Activities
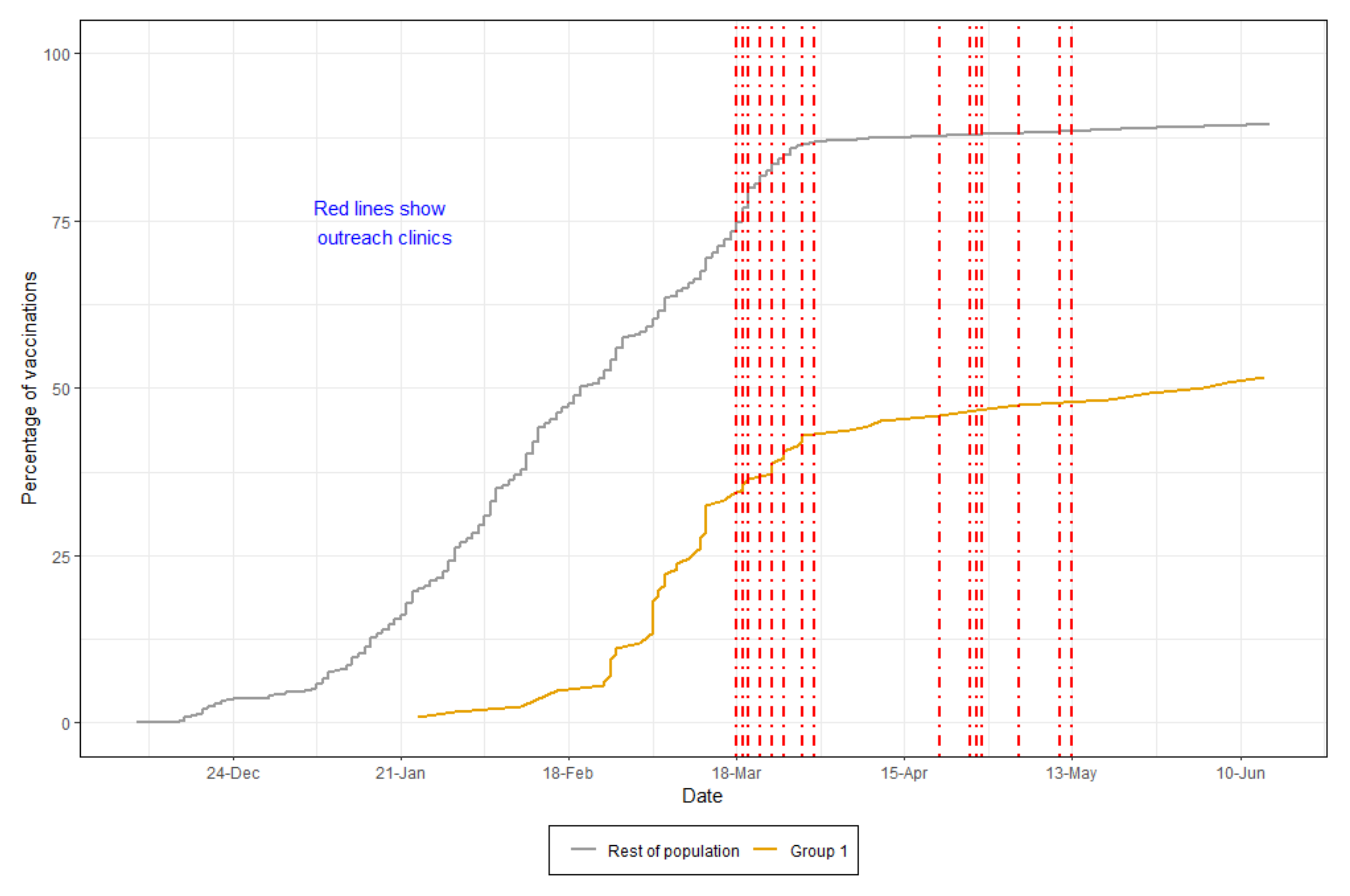
3.2.1. Group 1: Homeless People
- Onsite clinics at hotels, hostels and other accommodations
- Engagement with homeless people, on the street, though trusted individuals and homeless support workers
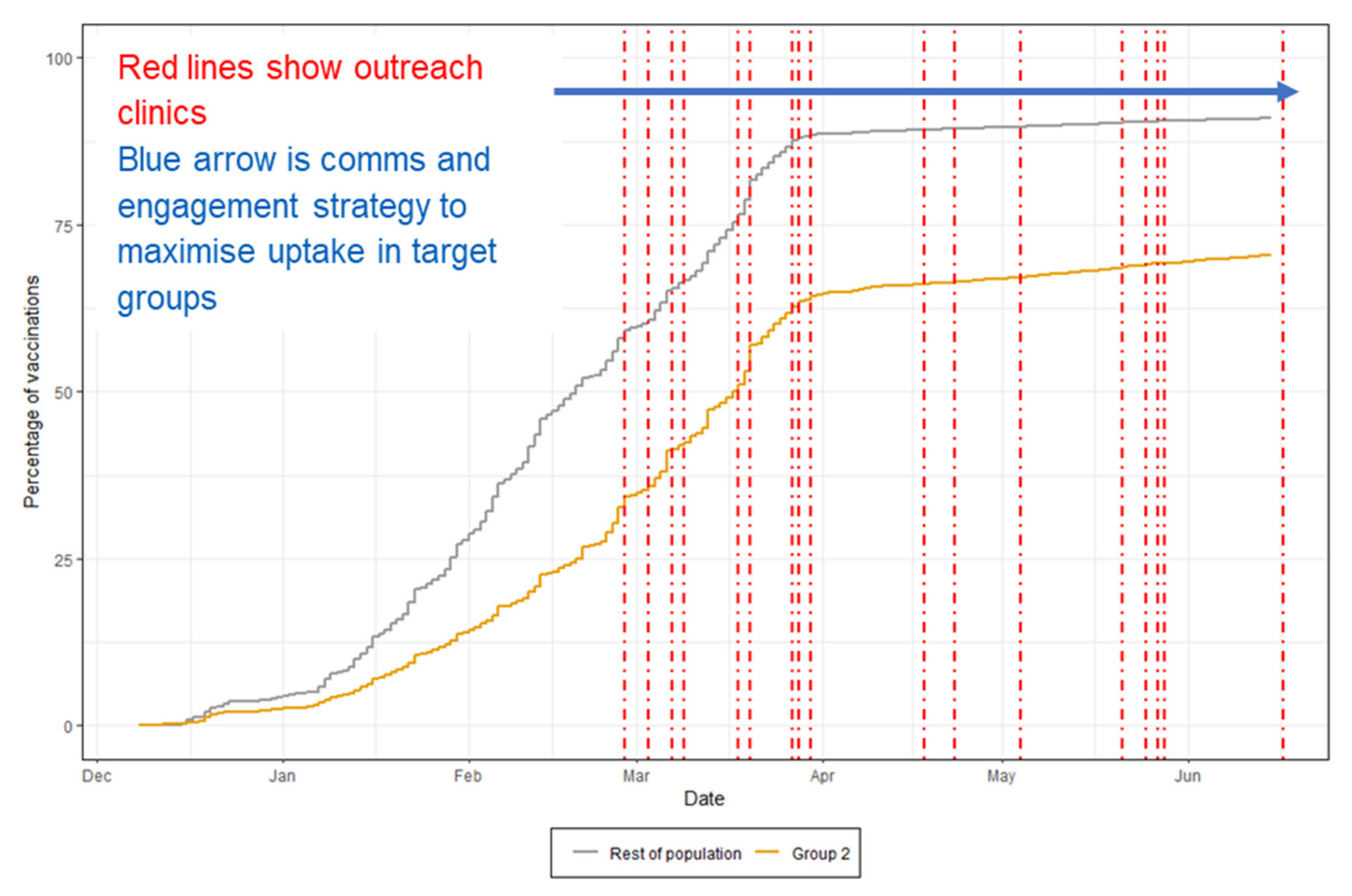
3.2.2. Group 2: Non-English-Speaking People, People from Minority Ethnic Groups, Refugees, and Asylum Seekers
3.2.3. Group 3: Gypsy, Roma, Travelers (GRT) and Boatpeople
3.2.4. Group 4: Those Who Would Struggle to Access Vaccination Centres, Such as People with Learning Difficulties (LD), Serious Mental Illness (SMI), People with Physical and Sensory Impairment, People with Drug & Alcohol (DA) Dependence, and People with Dementia
- Developing medical records searching strategies to identify patients, e.g., with SMI using the definition by the Quality and Outcomes Framework (QOF) and also prioritising people with eating disorders due to their clinical vulnerability.
- Adapting processes within large scale vaccination centres, Sirona Care and Health and PCN sites to accommodate the needs of people from this group—e.g., learning disability needs for appointment time, quiet setting and limited waiting.
- Maintaining regular communication with primary care teams through meetings and electronic bulletins.
3.3. Programme Costs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline (accessed on 15 November 2021).
- Islam, N.; Shkolnikov, V.M.; Acosta, R.J.; Klimkin, I.; Kawachi, I.; Irizarry, R.A.; Alicandro, G.; Khunti, K.; Yates, T.; Jdanov, D.A.; et al. Excess deaths associated with COVID-19 pandemic in 2020: Age and sex disaggregated time series analysis in 29 high income countries. BMJ 2021, 373, n1137. [Google Scholar] [CrossRef] [PubMed]
- Deaths within 28 Days of Positive Test by Date of Death. Available online: https://coronavirus.data.gov.uk/details/deaths (accessed on 1 March 2022).
- Disparities in the Risk and Outcomes of COVID-19. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/908434/Disparities_in_the_risk_and_outcomes_of_COVID_August_2020_update.pdf (accessed on 15 November 2021).
- Melchior, M.; du Loû, A.D.; Gosselin, A.; Datta, G.D.; Carabali, M.; Merckx, J.; Kaufman, J.S. Migrant status, ethnicity and COVID-19: More accurate European data are greatly needed. Clin. Microbiol. Infect. 2021, 27, 160–162. [Google Scholar] [CrossRef] [PubMed]
- Fabiani, M.; Mateo-Urdiales, A.; Andrianou, X.; Bella, A.; Del Manso, M.; Bellino, S.; Rota, M.C.; Boros, S.; Vescio, M.F.; D’Ancona, F.P.; et al. Epidemiological characteristics of COVID-19 cases in non-Italian nationals notified to the Italian surveillance system. Eur. J. Public Health 2021, 31, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Baena-Díez, J.M.; Barroso, M.; Cordeiro-Coelho, S.I.; Díaz, J.L.; Grau, M. Impact of COVID-19 outbreak by income: Hitting hardest the most deprived. J. Public Health 2020, 42, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Risk for COVID-19 Infection, Hospitalization, and Death by Race/Ethnicity. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 16 November 2021).
- Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Gethings, O.; Vihta, K.-D.; Jones, J.; House, T.; VanSteenHouse, H.; Bell, I.; et al. Impact of vaccination on new SARS-CoV-2 infections in the United Kingdom. Nat. Med. 2021, 27, 1370–1378. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Impact of COVID-19 Vaccines on Mortality in England. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/977249/PHE_COVID-19_vaccine_impact_on_mortality_March.pdf (accessed on 16 November 2021).
- COVID-19 Vaccine Coverage and Targeted Interventions to Improve Vaccination Uptake. Available online: https://post.parliament.uk/covid-19-vaccine-coverage-and-targeted-interventions-to-improve-vaccination-uptake/ (accessed on 16 November 2021).
- Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 16 November 2021).
- Yadegari, I.; Omidi, M.; Smith, S.R. The herd-immunity threshold must be updated for multi-vaccine strategies and multiple variants. Sci. Rep. 2021, 11, 22970. [Google Scholar] [CrossRef]
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav. Immun. 2021, 94, 41–50. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Coronavirus and Vaccine Hesitancy, Great Britain. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandvaccinehesitancygreatbritain/9august2021 (accessed on 13 March 2022).
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Woolf, K.; McManus, I.C.; Martin, C.A.; Nellums, L.B.; Guyatt, A.L.; Melbourne, C.; Bryant, L.; Gogoi, M.; Wobi, F.; Al-Oraibi, A.; et al. Ethnic differences in SARS-CoV-2 vaccine hesitancy in United Kingdom healthcare workers: Results from the UK-REACH prospective nationwide cohort study. Lancet Reg. Health Eur. 2021, 9, 100180. [Google Scholar] [CrossRef] [PubMed]
- Lockyer, B.; Islam, S.; Rahman, A.; Dickerson, J.; Pickett, K.; Sheldon, T.; Wright, J.; McEachan, R.; Sheard, L.; Bradford Institute for Health Research COVID-19 Scientific Advisory Group. Understanding COVID-19 misinformation and vaccine hesitancy in context: Findings from a qualitative study involving citizens in Bradford, UK. Health Expect. 2021, 24, 1158–1167. [Google Scholar] [CrossRef]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.; Duffy, B. Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic. Psychol. Med. 2021, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Woodhead, C.; Onwumere, J.; Rhead, R.; Bora-White, M.; Chui, Z.; Clifford, N.; Connor, L.; Gunasinghe, C.; Harwood, H.; Meriez, P.; et al. Race, ethnicity and COVID-19 vaccination: A qualitative study of UK healthcare staff. Ethn. Health 2021, 6, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Bielecki, K.; Kirolos, A.; Willocks, L.J.; Pollock, K.G.; Gorman, D.R. Low uptake of nasal influenza vaccine in Polish and other ethnic minority children in Edinburgh, Scotland. Vaccine 2019, 37, 693–697. [Google Scholar] [CrossRef]
- Loiacono, M.M.; Mahmud, S.M.; Chit, A.; van Aalst, R.; Kwong, J.C.; Mitsakakis, N.; Skinner, L.; Thommes, E.; Bricout, H.; Grootendorst, P. Patient and practice level factors associated with seasonal influenza vaccine uptake among at-risk adults in England, 2011 to 2016: An age-stratified retrospective cohort study. Vaccine X 2020, 100054, 100054. [Google Scholar] [CrossRef]
- National Immunisation Programme: Health Equity Audit. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/957670/immnstn-equity_AUDIT_v11.pdf (accessed on 16 November 2021).
- Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 5 November 2021).
- Understanding and Addressing the Barriers and Facilitators for Influenza and COVID-19 Vaccine Uptake among NHS Employees in Wales: Research and Evaluation Qualitative Insights and Co-Produced Interventions. Available online: https://phw.nhs.wales/publications/publications1/understanding-and-addressing-the-barriers-and-facilitators-for-influenza-and-covid-19-vaccine-uptake-among-nhs-employees-in-wales-report/ (accessed on 16 November 2021).
- Bateman, J.; Cox, N.; Rajagopala, L.; Ford, M.; Jasim, M.; Mulherin, D.; Venkatachalam, S.; Douglas, B.; Hirsch, G.; Sheeran, T. COVID-19 vaccination advice via SMS-based video to improve vaccination uncertainty in at-risk groups. Lancet Rheumatol. 2021, 3, e399–e401. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. Effective incentives for increasing COVID-19 vaccine uptake. Psychol. Med. 2021, 20, 1–3. [Google Scholar] [CrossRef]
- Annual Report and Accounts 2019/20. Available online: https://bnssgccg.nhs.uk/library/annual-report-and-accounts-201920/ (accessed on 16 November 2021).
- The Population of Bristol (December 2021). Available online: https://www.bristol.gov.uk/documents/20182/33904/Population+of+Bristol+September+2021.pdf/e6cb7ac8-278c-c351-9dcc-07a83fb4fe23?t=1632843439676 (accessed on 5 February 2022).
- Healthier Together. Available online: https://bnssghealthiertogether.org.uk/what-is-healthier-together/ (accessed on 27 February 2022).
- English Indices of Deprivation 2019. Available online: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2019 (accessed on 27 February 2022).
- Berrou, I.; Hamilton, K.; Cook, C.; Armour, C.; Hughes, S.; Hancock, J.; Quigg, S.; Hajinur, H.; Srivastava, S.; Kenward, C.; et al. Co-designing a COVID-19 vaccination programme with communities: Insights from the Maximising Uptake Programme. BMC Public Health 2022. to be submitted. [Google Scholar]
- Richardson, J.; Godfrey, B.; Walklate, S. Rapid, remote and responsive research during COVID-19. Methodol. Innov. 2021, 14, 9. [Google Scholar] [CrossRef]
- BNSSG CCG Insights & Engagement team. Easton Community Centre COVID-19 vaccination clinic survey results. March 2021 & Outreach clinics COVID-19 Combined survey results. Summary Report and Overview, March 2021 & Outreach clinics COVID-19 Combined survey results. Summary Report and Overview, May 2021; unpublished reports. [Google Scholar]
- Priority Groups for Coronavirus (COVID-19) Vaccination: Advice from the JCVI. 30 December 2020. Available online: https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-30-december-2020 (accessed on 6 October 2021).
- Alcendor, D.J.; Juarez, P.D.; Matthews-Juarez, P.; Simon, S.; Nash, C.; Lewis, K.; Smoot, D. Meharry Medical College Mobile Vaccination Program: Implications for Increasing COVID-19 Vaccine Uptake among Minority Communities in Middle Tennessee. Vaccines 2022, 10, 211. [Google Scholar] [CrossRef] [PubMed]
- Increasing Vaccine Uptake. Available online: https://www.strategyunitwm.nhs.uk/publications/increasing-vaccine-uptake (accessed on 27 February 2022).
- Bell, S.; Saliba, V.; Ramsay, M.; Mounier-Jack, S. What have we learnt from measles outbreaks in 3 English cities? A qualitative exploration of factors influencing vaccination uptake in Romanian and Roma Romanian communities. BMC Public Health 2020, 20, 381. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Newton, P. Structural barriers to measles, mumps and rubella (MMR) immunisation uptake in Gypsy, Roma and Traveller communities in the United Kingdom. Crit. Public Health 2017, 27, 238–247. [Google Scholar] [CrossRef]
- Tankwanchi, A.S.; Bowman, B.; Garrison, M.; Larson, H.; Wiysonge, C.S. Vaccine hesitancy in migrant communities: A rapid review of latest evidence. Curr. Opin. Immunol. 2021, 71, 62–68. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Target Group | Outreach Activities 1 | Period | N Vaccines Given |
|---|---|---|---|
| Group 1: Homeless people | 51 | March–August 2021 | 504 |
| Group 2: Non-English-speaking people, people from minority ethnic groups, refugees, and asylum seekers | 93 | February–August 2021 | 7241 |
| Group 3: Gypsy, Roma, Travellers and boat people | 13 | March–August 2021 | 132 |
| Group 4: People with LD, SMI, Physical and sensory impairments, D&A dependence, dementia | 5 | June–August 2021 | 102 |
| Total | 162 | 7979 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berrou, I.; Hamilton, K.; Cook, C.; Armour, C.; Hughes, S.; Hancock, J.; Quigg, S.; Hajinur, H.; Srivastava, S.; Kenward, C.; et al. Leaving No One Behind: Interventions and Outcomes of the COVID-19 Vaccine Maximising Uptake Programme. Vaccines 2022, 10, 840. https://doi.org/10.3390/vaccines10060840
Berrou I, Hamilton K, Cook C, Armour C, Hughes S, Hancock J, Quigg S, Hajinur H, Srivastava S, Kenward C, et al. Leaving No One Behind: Interventions and Outcomes of the COVID-19 Vaccine Maximising Uptake Programme. Vaccines. 2022; 10(6):840. https://doi.org/10.3390/vaccines10060840
Chicago/Turabian StyleBerrou, Ilhem, Kathryn Hamilton, Clare Cook, Clare Armour, Sian Hughes, Jude Hancock, Sally Quigg, Huda Hajinur, Seema Srivastava, Charlie Kenward, and et al. 2022. "Leaving No One Behind: Interventions and Outcomes of the COVID-19 Vaccine Maximising Uptake Programme" Vaccines 10, no. 6: 840. https://doi.org/10.3390/vaccines10060840