
The Impact and Vaccination Coverage of Seasonal Influenza among Children Aged 6–59 Months in China in 2017–2018: An Internet Panel Survey

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Population and Estimation of Influenza-Associated Illness
3.2. IV Coverage among Children Aged 6–59 Months in China in 2017–2018
3.3. Knowledge and Attitudes toward Influenza Infection and Prevention
3.4. Healthcare-Seeking Behaviors Related to Influenza Infection and the Impact of Children Suffering from ILI on the Family
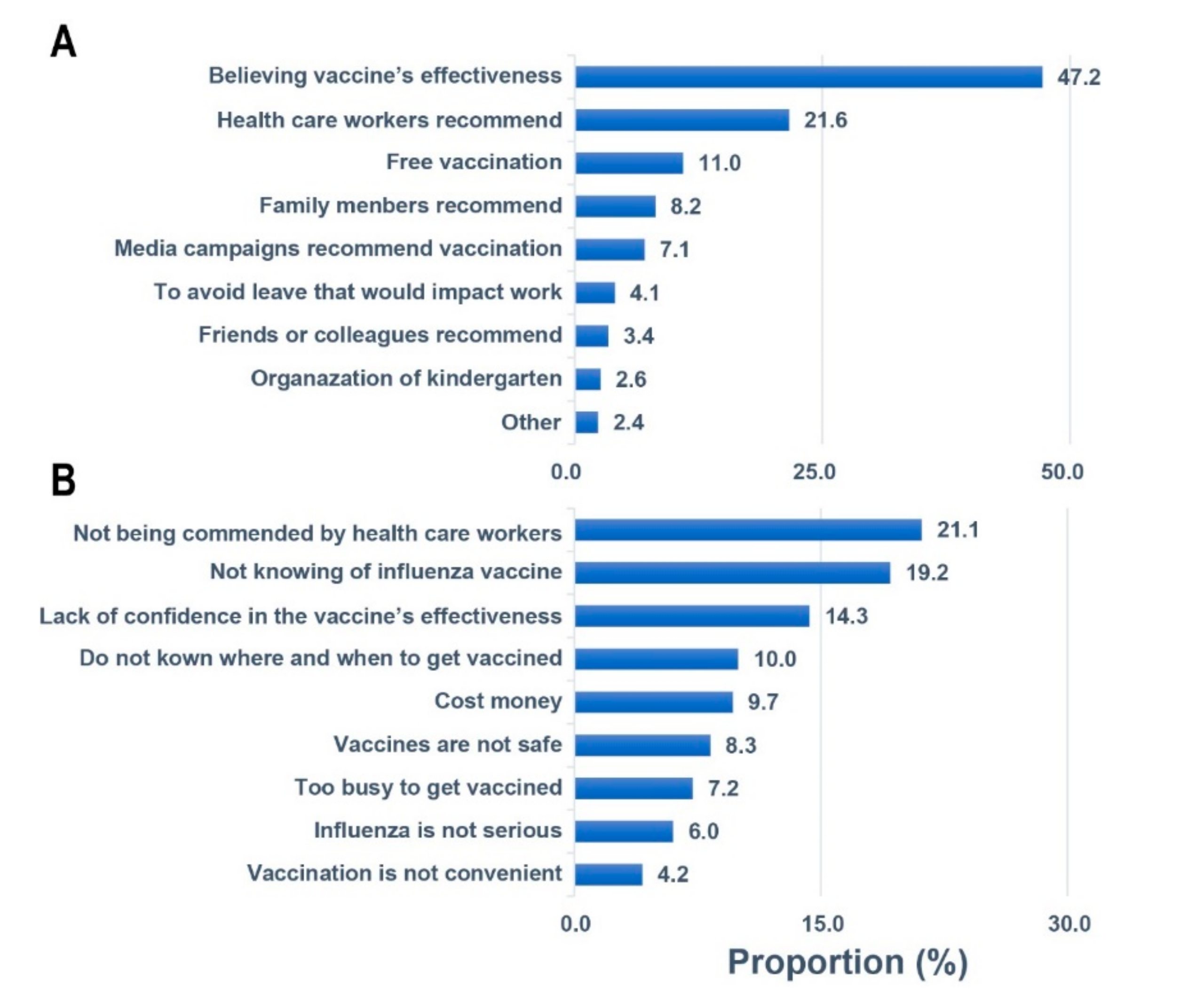
3.5. Factors Related to Willingness to Be Vaccinated for Influenza Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oliva, J.; Delgado-Sanz, C.; Larrauri, A. The Spanish Influenza Surveillance System. Estimating the burden of seasonal influenza in Spain from surveillance of mild and severe influenza disease, 2010-2016. Influenza Other Respir. Viruses 2018, 12, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Y.T.; Graitcer, S.B.; Nguyen, T.H.; Tran, D.N.; Pham, T.D.; Le, M.T.; Tran, H.N.; Bui, C.T.; Dang, D.T.; Nguyen, L.T.; et al. National surveillance for influenza and influenza-like illness in Vietnam, 2006−2010. Vaccine 2013, 31, 4368–4374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, W.J.; Viboud, C.; Simonsen, L.; Hirano, E.W.; Daufenbach, L.Z.; Miller, M.A. Seasonality of Influenza in Brazil: A Traveling Wave from the Amazon to the Subtropics. Am. J. Epidemiol. 2007, 165, 1434–1442. [Google Scholar] [CrossRef]
- Biezen, R.; Grando, D.; Mazza, D.; Brijnath, B. Why do we not want to recommend influenza vaccination to young children? A qualitative study of Australian parents and primary care providers. Vaccine 2018, 36, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.-J.; Zhang, H.-Y.; Ren, L.-L.; Lu, Q.-B.; Ren, X.; Zhang, C.-H.; Wang, Y.-F.; Lin, S.-H.; Zhang, X.-A.; Li, J.; et al. Etiological and epidemiological features of acute respiratory infections in China. Nat. Commun. 2021, 12, 5026. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; VAN Asten, L.; Wang, L.; Mcdonald, S.A.; Pan, Y.; Duan, W.; Zhang, L.; Sun, Y.; Zhang, Y.; Zhang, X.; et al. Estimated incidence and number of outpatient visits for seasonal influenza in 2015–2016 in Beijing, China. Epidemiol. Infect. 2017, 145, 3334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuzil, K.M.; Hohlbein, C.; Zhu, Y. Illness among schoolchildren during influenza season: Effect on school absenteeism, parental absenteeism from work, and secondary illness in families. Arch. Pediatr. Adolesc. Med. 2002, 156, 986–991. [Google Scholar] [CrossRef] [Green Version]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- Feng, L.; Yang, P.; Zhang, T.; Yang, J.; Fu, C.; Qin, Y.; Zhang, Y.; Ma, C.; Liu, Z.; Wang, Q.; et al. Technical guidelines for the application of seasonal influenza vaccine in China (2014–2015). Hum. Vaccines Immunother. 2015, 11, 2077–2101. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Muscatello, D.J.; Cao, Z.; Chughtai, A.A.; Costantino, V.; Zhang, D.; Yang, P.; Wang, Q.; MacIntyre, C.R. A model of influenza infection and vaccination in children aged under 5 years in Beijing, China. Hum. Vaccines Immunother. 2020, 16, 1685–1690. [Google Scholar] [CrossRef]
- Ren, X.; Geoffroy, E.; Tian, K.; Wang, L.; Feng, L.; Feng, J.; Qin, Y.; Wu, P.; Zhang, S.; Geng, M.; et al. Knowledge, Attitudes, and Behaviors (KAB) of Influenza Vaccination in China: A Cross-Sectional Study in 2017/2018. Vaccines 2019, 8, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, L.; Su, Q.; Xu, Z.; Feng, A.; Jin, H.; Wang, S.; Feng, Z. Seasonal influenza vaccination coverage rate of target groups in selected cities and provinces in China by season (2009/10 to 2011/12). PLoS ONE 2013, 8, e73724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awad, S.; Abdo, N.; Yusef, D.; Jawarneh, A.; Babaa, A.; Alwady, D.; Al-Bawayeh, H.; Kasrawi, I.; Amaireh, M.; Obeidat, M.; et al. Knowledge, attitudes and practices related to influenza illness and vaccination in children: Role of awareness campaigns in changing parents’ attitudes toward influenza vaccination in Jordan. Vaccine 2019, 37, 3303. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Quinn, S.C.; Kim, K.H.; Musa, D.; Hilyard, K.M.; Freimuth, V.S. The Social Ecological Model as a Framework for Determinants of 2009 H1N1 Influenza Vaccine Uptake in the United States. Health Educ. Behav. 2011, 39, 229–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bone, A.; Guthmann, J.-P.; Nicolau, J.; Lévy-Bruhl, D. Population and risk group uptake of H1N1 influenza vaccine in mainland France 2009–2010: Results of a national vaccination campaign. Vaccine 2010, 28, 8157–8161. [Google Scholar] [CrossRef]
- Maurer, J.; Uscher-Pines, L.; Harris, K.M. Perceived seriousness of seasonal and A(H1N1) influenzas, attitudes toward vaccination, and vaccine uptake among U.S. adults: Does the source of information matter? Prev. Med. 2010, 51, 185–187. [Google Scholar] [CrossRef]
- Sun, K.S.; Lam, T.P.; Kwok, K.W.; Lam, K.F.; Wu, D.; Ho, P.L. Seasonal influenza vaccine uptake among Chinese in Hong Kong: Barriers, enablers and vaccination rates. Hum. Vaccines Immunother. 2020, 16, 1675–1684. [Google Scholar] [CrossRef]
- Ramsey, M.A.; Marczinski, C.A. College students’ perceptions of H1N1 flu risk and attitudes toward vaccination. Vaccine 2011, 29, 7599–7601. [Google Scholar] [CrossRef] [Green Version]
- Eastwood, K.; Durrheim, D.N.; Jones, A.; Butler, M. Acceptance of pandemic (H1N1) 2009 influenza vaccination by the Australian public. Med. J. Aust. 2010, 192, 33–36. [Google Scholar] [CrossRef]
- Black, C.L.; Yue, X.; Ball, S.W.; Donahue, S.M.; Izrael, D.; de Perio, M.A.; Laney, A.S.; Williams, W.W.; Lindley, M.C.; Graitcer, S.B.; et al. Influenza Vaccination Coverage Among Health Care Personnel—United States, 2015–2016 Influenza Season. MMWR Morb. Mortal Wkly. Rep. 2016, 65, 1026–1031. [Google Scholar] [CrossRef] [Green Version]
- Shono, A.; Kondo, M. Factors associated with seasonal influenza vaccine uptake among children in Japan. BMC Infect. Dis. 2015, 15, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasa, T.; Wada, K. Reasons for and against receiving influenza vaccination in a working age population in Japan: A national cross-sectional study. BMC Public Health. 2013, 13, 647. [Google Scholar]
- Ye, C.; Zhu, W.; Yu, J.; Li, Z.; Hu, W.; Hao, L.; Wang, Y.; Xu, H.; Sun, Q.; Zhao, G. Low coverage rate and awareness of influenza vaccine among older people in Shanghai, China: A cross-sectional study. Hum. Vaccines Immunother. 2018, 14, 2715–2721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, V.J.; Le Saux, N.; Plint, A.C.; Correll, R.; Gaboury, I.; Ellis, E.; Tam, T.W.S. Factors influencing childhood influenza immunization. Can. Med. Assoc. J. 2003, 168, 39–41. [Google Scholar]
- Lin, C.; Nowalk, M.P.; Zimmerman, R.K.; Ko, F.-S.; Zoffel, L.; Hoberman, A.; Kearney, D.H. Beliefs and Attitudes about Influenza Immunization among Parents of Children with Chronic Medical Conditions over a Two-Year Period. J. Hered. 2006, 83, 874–883. [Google Scholar] [CrossRef] [Green Version]
- Gnanasekaran, S.K.; Finkelstein, J.A.; Hohman, K.; O’Brien, M.; Kruskal, B.; Lieu, T.A. Parental Perspectives on Influenza Vaccination Among Children with Asthma. Public Health Rep. 2006, 121, 181–188. [Google Scholar] [CrossRef]
- Allison, M.A.; Reyes, M.; Young, P.; Calame, L.; Sheng, X.; Weng, H.-Y.C.; Byington, C.L. Parental Attitudes About Influenza Immunization and School-Based Immunization for School-Aged Children. Pediatr. Infect. Dis. J. 2010, 29, 751–755. [Google Scholar] [CrossRef]
- Hays, R.D.; Liu, H.; Kapteyn, A. Use of Internet panels to conduct surveys. Behav. Res. Methods 2015, 47, 685–690. [Google Scholar] [CrossRef]
- Li, Z.; Yu, J.; Ren, X.; Ye, C.; Tian, K.; Feng, L.; Song, Y.; Cowling, B.J. Influenza Vaccination Coverage among Registered Nurses in China during 2017-2018: An Internet Panel Survey (Preprint). Vaccines 2019, 7, 134. [Google Scholar] [CrossRef]
- Liu, H.; Cella, D.; Gershon, R.; Shen, J.; Morales, L.S.; Riley, W.; Hays, R.D. Representativeness of the Patient-Reported Outcomes Measurement Information System Internet panel. J. Clin. Epidemiol. 2010, 63, 1169–1178. [Google Scholar] [CrossRef] [Green Version]
- Hill, H.A.; Singleton, J.A.; Yankey, D.; Elam-Evans, L.D.; Pingali, S.C.; Kang, Y. Vaccination Coverage by Age 24 Months Among Children Born in 2015 and 2016—National Immunization Survey-Child, United States, 2016–2018. MMWR Morb. Mortal Wkly. Rep. 2019, 68, 913–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woyessa, A.B.; Mengesha, M.; Belay, D.; Tayachew, A.; Ayele, W.; Beyene, B.; Kassa, W.; Zemelak, E.; Demissie, G.; Amare, B.; et al. Epidemiology of influenza in Ethiopia: Findings from influenza sentinel surveillance and respiratory infection outbreak investigations, 2009–2015. BMC Infect. Dis. 2018, 18, 449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groeneveld, G.H.; Spaan, W.J.; van der Hoek, W.; van Dissel, J.T. The severe flu season of 2017–2018: Making a case for the vaccination of healthcare professionals. Nederlands Tijdschrift Voor Geneeskunde 2018, 162, 6. [Google Scholar]
- Kochanek, M.; Böll, B.; Shimabukuro-Vornhagen, A.; Welte, T.; Wieland, U.; Pletz, M.; Hallek, M.; Fätkenheuer, G.; Salzberger, B. The 2017/2018 influenza season-business as usual? Internist 2018, 59, 1122–1124. [Google Scholar] [CrossRef]
- Feng, Z.J. Seasonal, avian and pandemic influenza: Are we prepared? Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 1017–1020. [Google Scholar]
- Paules, C.; Subbarao, K. Influenza. Lancet 2017, 390, 697–708. [Google Scholar] [CrossRef]
- Feng, L.; Li, Z.; Zhao, S.; Nair, H.; Lai, S.; Xu, W.; Li, M.; Wu, J.; Ren, L.; Liu, W.; et al. Viral etiologies of hospitalized acute lower respiratory infection patients in China, 2009–2013. PLoS ONE 2014, 9, e99419. [Google Scholar] [CrossRef]
- Ma, W.; Huo, X.; Zhou, M. The healthcare seeking rate of individuals with influenza like illness: A meta-analysis. Infect Dis. 2018, 50, 728–735. [Google Scholar] [CrossRef]
- Yuan, J.; Zhang, L.; Xu, W.; Shen, J.; Zhang, P.; Ma, H. Reported changes in health-related behaviours in Chinese urban residents in response to an influenza pandemic. Epidemiol. Infect 2009, 137, 988–993. [Google Scholar] [CrossRef]
- Spaulding, A.B.; Radi, D.; MacLeod, H.; Lynfield, R.; Larson, M.; Hyduke, T.; Dehnel, P.; Devries, A.S. Satisfaction and Public Health Cost of a Statewide Influenza Nurse Triage Line in Response to Pandemic H1N1 Influenza. PLoS ONE 2013, 8, e50492. [Google Scholar] [CrossRef]
- Meng, H.; Liao, Q.; Suen, L.K.P.; O’Donoghue, M.; Wong, C.M.; Yang, L. Healthcare seeking behavior of patients with influenza like illness: Comparison of the summer and winter influenza epidemics. BMC Infect. Dis. 2016, 16, 499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biggerstaff, M.; Jhung, M.A.; Reed, C.; Fry, A.M.; Balluz, L.; Finelli, L. Influenza-like illness, the time to seek healthcare, and influenza antiviral receipt during the 2010–2011 influenza season-United States. J. Infect. Dis. 2014, 210, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Tempia, S.; Moyes, J.; Cohen, A.L.; Walaza, S.; Edoka, I.; McMorrow, M.L.; Treurnicht, F.K.; Hellferscee, O.; Wolter, N.; von Gottberg, A.; et al. Health and economic burden of influenza-associated illness in South Africa, 2013-2015. Influenza Other Respir. Viruses 2019, 13, 484–495. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Zhang, T.; Wang, Y.; Gao, J.M.; Hua, J.; Tian, J.M.; Ding, Y.F.; Zhang, J.; Chen, L.L.; Li, J.Q.; et al. Clinical characteristics and economic burden of influenza among children under 5 years old, in Suzhou, 2011–2017. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 847–851. [Google Scholar] [PubMed]
- Yang, J.; Atkins, K.E.; Feng, L.; Pang, M.; Zheng, Y.; Liu, X.; Cowling, B.J.; Yu, H. Seasonal influenza vaccination in China: Landscape of diverse regional reimbursement policy, and budget impact analysis. Vaccine 2016, 34, 5724–5735. [Google Scholar] [CrossRef] [Green Version]
- Willis, G.A.; Preen, D.; Richmond, P.; Jacoby, P.; Effler, P.V.; Smith, D.W.; Robins, C.; Borland, M.L.; Levy, A.; Keil, A.D.; et al. The impact of influenza infection on young children, their family and the health care system. Influ. Other Respir. Viruses 2018, 13, 18–27. [Google Scholar] [CrossRef] [Green Version]
- Lam, W.; Dawson, A.; Fowler, C. The Health Literacy of Hong Kong Chinese Parents with Preschool Children in Seasonal Influenza Prevention: A Multiple Case Study at Household Level. PLoS ONE 2015, 10, e0143844. [Google Scholar] [CrossRef]
- Chuang, Y.-C.; Huang, Y.-L.; Tseng, K.-C.; Yen, C.-H.; Yang, L.-H. Social Capital and Health-Protective Behavior Intentions in an Influenza Pandemic. PLoS ONE 2015, 10, e0122970. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Population n = 4719 (%) | ILI Symptoms n = 1913 (%) | p-Value |
|---|---|---|---|
| Sex | 0.174 | ||
| Male | 2471 (52.4) | 1041 (42.1) | |
| Female | 2248 (47.6) | 872 (38.8) | |
| Age in months | <0.001 | ||
| 6–11 | 1868 (39.6) | 559 (29.9) | |
| 12–23 | 1604 (34.0) | 735 (45.8) | |
| 24–35 | 620 (13.1) | 272 (43.9) | |
| 36–47 | 402 (8.5) | 203 (50.5) | |
| 48–59 | 225 (4.8) | 144 (64.0) | |
| Region | 0.152 | ||
| North | 1854 (39.3) | 728 (39.2) | |
| South | 2865 (60.7) | 1185 (41.3) | |
| Province | <0.001 | ||
| Guangdong | 1303 (27.6) | 479 (36.8) | |
| Henan | 846 (17.9) | 305 (36.1) | |
| Guangxi | 994 (21.1) | 456 (45.9) | |
| Sichuan | 545 (11.5) | 250 (45.9) | |
| Shandong | 716 (15.2) | 287 (40.1) | |
| Tianjin | 315 (6.7) | 136 (43.2) |
| Characteristics | Number Vaccinated | Number Unvaccinated | Unknown | p-Value |
|---|---|---|---|---|
| Sex | 0.958 | |||
| Male | 972 (39.3) | 1251 (50.6) | 248 (10.0) | |
| Female | 885 (39.4) | 1143 (50.8) | 220 (9.8) | |
| Age in months | <0.001 | |||
| 6–11 | 551 (25.9) | 1104 (59.1) | 213 (11.4) | |
| 12–23 | 733 (45.7) | 726 (45.3) | 145 (9.0) | |
| 24–35 | 319 (51.5) | 243 (39.2) | 58 (9.4) | |
| 36–47 | 179 (44.5 | 189 (47.0) | 34 (8.5) | |
| 48–59 | 75 (33.3) | 132 (58.7) | 18 (8.0) | |
| Region | ||||
| North | 548 (29.6) | 1109 (59.8) | 197 (10.6) | <0.001 |
| South | 1309 (45.7) | 1285 (44.9) | 271 (9.5) | |
| Province | <0.001 | |||
| Guangdong | 612 (47.0) | 594 (45.6) | 97 (7.4) | |
| Henan | 350 (35.2) | 516 (51.9) | 128 (12.9) | |
| Guangxi | 388 (45.9) | 347 (41.0) | 111 (13.1) | |
| Sichuan | 309 (43.2) | 344 (48.0) | 63 (8.8) | |
| Shandong | 117 (21.5) | 383 (70.3) | 45 (8.3) | |
| Tianjin | 81 (25.7) | 210 (66.7) | 24 (7.6) | |
| Total | 1857 (39.4) | 2394 (50.7) | 468 (9.9) |
| Characteristics | 6–59 Months | p-Value | Province | p-Value | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6–11 | 12–23 | 24–35 | 36–47 | 48–59 | Guangdong | Henan | Guangxi | Sichuan | Shandong | Tianjin | ||||
| Distinction of flu and cold | 0.572 | <0.001 | ||||||||||||
| Yes | 1457 (78.0) | 1251 (78.0) | 498 (80.3) | 319 (79.4) | 175 (77.8) | 992 (76.1) | 767 (77.2) | 633 (74.8) | 547 (80.2) | 462 (84.8) | 272 (86.3) | 3700 (78.4) | ||
| No | 63 (3.4) | 58 (3.6) | 22 (3.5) | 19 (4.7) | 12 (5.3) | 49 (3.8) | 37 (3.7) | 30 (3.5) | 34 (4.7) | 15 (2.8) | 9 (2.9) | 174 (3.7) | ||
| Unknown | 348 (18.6) | 295 (18.4) | 100 (16.1) | 64 (15.9) | 38 (16.9) | 262 (20.1) | 190 (19.1) | 183 (21.6) | 108 (15.1) | 68 (12.5) | 34 (10.8) | 845 (17.9) | ||
| Serious illness induced by flu | 0.975 | <0.001 | ||||||||||||
| Yes | 1520 (81.4) | 1319 (82.2) | 509 (82.1) | 334 (83.1) | 179 (79.6) | 1075 (82.5) | 747 (75.2) | 680 (80.4) | 612 (85.5) | 467 (85.7) | 280 (88.9) | 3861 (81.8) | ||
| No | 73 (3.9) | 57 (3.6) | 21 (3.4) | 14 (3.5) | 8 (3.6) | 39 (3.0) | 52 (5.2) | 32 (3.8) | 19 (2.7) | 17 (3.1) | 14 (4.4) | 173 (3.7) | ||
| Unknown | 275 (14.7) | 228 (14.2) | 90 (14.5) | 54 (13.4) | 38 (16.9) | 189 (14.5) | 195 (19.6) | 134 (15.8) | 85 (11.9) | 61 (11.2) | 21 (6.7) | 685 (14.5) | ||
| Washing hands | 0.009 | <0.001 | ||||||||||||
| Yes | 1172 (62.7) | 1103 (68.8) | 423 (68.2) | 275 (68.4) | 146 (64.9) | 906 (69.5) | 596 (60.0) | 578 (68.3) | 425 (59.4) | 390 (71.6) | 224 (71.1) | 3119 (66.1) | ||
| No | 557 (29.8) | 403 (25.1) | 156 (25.2) | 108 (18.4) | 59 (26.2) | 333 (25.6) | 311 (31.3) | 198 (23.4) | 230 (32.1) | 135 (24.8) | 76 (24.1) | 1283 (27.2) | ||
| Unknown | 139 (7.4) | 98 (6.1) | 41 (6.6) | 19 (4.7) | 20 (8.9) | 64 (4.9) | 87 (8.8) | 70 (8.3) | 61 (8.5) | 20 (3.7) | 15 (4.8) | 317 (6.7) | ||
| Mask wearing | <0.001 | <0.001 | ||||||||||||
| Yes | 854 (45.7) | 566 (35.3) | 217 (35.0) | 155 (38.6) | 94 (41.8) | 478 (36.7) | 379 (38.1) | 293 (34.6) | 297 (41.5) | 274 (50.3) | 165 (52.4) | 1886 (40.0) | ||
| No | 917 (49.1) | 957 (59.7) | 374 (60.3) | 235 (58.5) | 125 (55.6) | 774 (59.4) | 551 (55.4) | 479 (58.7) | 391 (54.6) | 253 (46.4) | 142 (45.1) | 2608 (55.3) | ||
| Unknown | 97 (5.2) | 81 (5.0) | 29 (4.7) | 12 (3.0) | 6 (2.7) | 51 (3.9) | 64 (6.4) | 56 (6.6) | 28 (3.9) | 18 (3.3) | 8 (2.5) | 225 (4.8) | ||
| Self-segregation | 0.093 | 0.011 | ||||||||||||
| Yes | 1568 (83.9) | 1362 (84.9) | 512 (82.6) | 330 (82.1) | 180 (80.0) | 1127 (86.5) | 793 (79.8) | 704 (83.2) | 596 (83.2) | 463 (85.0) | 269 (85.4) | 3952 (83.7) | ||
| No | 236 (12.6) | 189 (11.8) | 85 (13.7) | 66 (16.4) | 34 (15.1) | 141 (10.8) | 157 (15.8) | 109 (12.9) | 101 (14.1) | 65 (11.9) | 37 (11.7) | 610 (12.9) | ||
| Unknown | 64 (3.4) | 53 (3.3) | 23 (3.7) | 6 (1.5) | 11 (4.9) | 35 (2.7) | 44 (4.4) | 33 (3.9) | 19 (2.7) | 17 (3.1) | 9 (2.9) | 157 (3.3) | ||
| Characteristics | Influenza-Positive n = 1913 (%) | Influenza-Negative n = 2806 (%) | p-Value |
|---|---|---|---|
| Distinction of flu and cold | <0.001 | ||
| Yes | 1458 (76.2) | 2242 (79.9) | |
| No | 96 (5.0) | 78 (2.8) | |
| Unknown | 359 (18.8) | 486 (17.3) | |
| Serious illness induced by flu | 0.541 | ||
| Yes | 1518 (79.4) | 2343 (83.5) | |
| No | 64 (3.3) | 109 (3.9) | |
| Unknown | 331 (17.3) | 354 (12.6) | |
| Washing hands | 0.005 | ||
| Yes | 1247 (65.2) | 1872 (66.7) | |
| No | 572 (29.9) | 711 (25.3) | |
| Unknown | 94 (4.9) | 223 (7.9) | |
| Mask wearing | <0.001 | ||
| Yes | 647 (33.8) | 1239 (44.2) | |
| No | 1208 (63.1) | 1400 (49.9) | |
| Unknown | 58 (3.0) | 167 (6.0) | |
| Self-segregation | 0.245 | ||
| Yes | 1612 (84.3) | 2340 (83.4) | |
| No | 264 (13.8) | 346 (12.3) | |
| Unknown | 37 (1.9) | 120 (4.3) |
| Characteristics | 6–59 Months | Province | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6–11 | 12–23 | 24–35 | 36–47 | 48–59 | Guangdong | Henan | Guangxi | Sichuan | Shandong | Tianjin | ||
| Medical treatment seeking | ||||||||||||
| Yes | 516 (92.3) | 677 (92.1) | 247 (90.8) | 191 (94.1) | 136 (94.4) | 434 (90.6) | 436 (95.6) | 276 (90.5) | 271 (94.4) | 222 (88.8) | 128 (94.1) | 1767 (92.4) |
| No | 42 (7.5) | 49 (6.7) | 25 (9.2) | 10 (4.9) | 6 (4.2) | 43 (9.0) | 18 (3.9) | 23 (7.5) | 15 (5.2) | 25 (10.0) | 8 (5.9) | 132 (6.9) |
| Unknown | 1 (0.2) | 9 (1.2) | 0 (0) | 2 (1) | 2 (1.4) | 2 (0.4) | 2 (0.4) | 6 (2.0) | 1 (0.3) | 3 (1.2) | 0 (0) | 14 (0.7) |
| Treatment method | ||||||||||||
| Outpatient/emergency | 415 (58.2) | 592 (63.4) | 212 (61.8) | 162 (59.3) | 119 (64.0) | 393 (71.5) | 356 (59.8) | 222 (55.9) | 221 (57.3) | 188 (58.9) | 120 (61.9) | 1500 (61.2) |
| Be hospitalized | 111 (15.6) | 112 (12.0) | 34 (9.9) | 31 (11.4) | 26 (14.0) | 52 (9.5) | 93 (15.4) | 52 (13.1) | 75 (19.4) | 28 (8.8) | 14 (7.2) | 314 (12.8) |
| Drugstore | 158 (22.2) | 196 (21.0) | 84 (24.5) | 66 (24.2) | 36 (19.4) | 85 (15.5) | 141 (23.3) | 99 (24.9) | 77 (19.9) | 84 (26.3) | 54 (27.8) | 540 (22.0) |
| Rest with no treat | 29 (4.1) | 33 (3.5) | 13 (3.8) | 14 (5.1) | 4 (2.2) | 19 (3.5) | 14 (2.3) | 23 (5.8) | 13 (3.4) | 18 (5.6) | 6 (3.1) | 93 (3.8) |
| Unknown | 0 (0) | 1 (0.1) | 0 (0) | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 1 (0.3) | 0 (0) | 1 (0.3) | 0 (0) | 2 (0.1) |
| Hospital choosing | ||||||||||||
| Tertiary hospitals | 203 (30.6) | 302 (36.0) | 95 (29.7) | 88 (35.2) | 69 (41.3) | 203 (38.2) | 114 (19.9) | 104 (29.1) | 112 (31.8) | 139 (51.5) | 85 (54.5) | 757 (33.8) |
| Secondary hospitals | 165 (24.8) | 200 (23.9) | 76 (23.8) | 46 (18.4) | 31 (18.6) | 127 (23.9) | 124 (21.6) | 90 (25.2) | 105 (29.8) | 40 (14.8) | 32 (20.5) | 518 (23.1) |
| Community health service | 130 (19.6) | 166 (19.8) | 74 (23.1) | 62 (24.8) | 27 (16.2) | 139 (26.2) | 117 (20.4) | 74 (20.7) | 66 (18.8) | 47 (17.4) | 16 (10.3) | 459 (20.5) |
| Clinic/village doctor | 160 (24.1) | 166 (19.8) | 73 (22.8) | 53 (21.2) | 38 (22.8) | 59 (11.1) | 215 (37.5) | 85 (23.8) | 66 (18.8) | 42 (15.6) | 23 (14.7) | 490 (21.9) |
| Unknown | 6 (0.9) | 4 (0.5) | 2 (0.6) | 1 (0.4) | 2 (1.2) | 3 (0.6) | 3 (0.5) | 4 (1.1) | 3 (0.9) | 2 (07) | 0 (0) | 15 (0.6) |
| Medical expense (¥) | ||||||||||||
| 0–299 | 208 (40.5) | 224 (33.1) | 91 (36.8) | 52 (27.2) | 28 (20.6) | 168 (38.8) | 169 (38.8) | 113 (40.9) | 82 (30.5) | 44 (19.8) | 27 (21.1) | 603 (31.5) |
| 300–799 | 123 (23.9) | 199 (29.4) | 77 (31.2) | 66 (34.6) | 47 (34.6) | 147 (33.9) | 106 (24.3) | 80 (29.0) | 75 (27.9) | 66 (29.7) | 38 (29.7) | 512 (26.8) |
| 800–1499 | 56 (10.9) | 109 (16.1) | 34 (13.8) | 27 (14.1) | 20 (14.7) | 56 (12.9) | 65 (14.9) | 29 (10.5) | 28 (10.4) | 39 (17.6) | 29 (22.7) | 246 (12.9) |
| 1500–2999 | 53 (10.3) | 71 (10.5) | 23 (9.3) | 29 (15.2) | 20 (14.7) | 31 (7.2) | 52 (11.9) | 20 (7.2) | 37 (13.8) | 42 (18.9) | 14 (10.9) | 403 (21.1) |
| 3000 | 67 (13.0) | 61 (9.0) | 15 (6.1) | 12 (6.3) | 21 (15.4) | 25 (5.8) | 38 (8.7) | 25 (9.1) | 40 (14.9) | 29 (13.1) | 19 (14.8) | 176 (9.2) |
| Unknown | 7 (1.4) | 12 (1.8) | 7 (2.8) | 5 (2.6) | 0 (0) | 6 (1.4) | 6 (1.4) | 9 (3.3) | 7 (2.6) | 2 (0.9) | 1 (0.8) | 149 (7.8) |
| Personal-paid | ||||||||||||
| 100% | 367 (71.1) | 506 (74.4) | 167 (67.6) | 136 (71.2) | 89 (65.4) | 287 (66.1) | 315 (72.2) | 199 (72.1) | 184 (67.9) | 180 (81.1) | 100 (78.1) | 1265 (71.6) |
| 80–99% | 31 (6.0) | 34 (5.0) | 14 (5.7) | 11 (5.8) | 8 (5.9) | 29 (6.7) | 17 (3.9) | 15 (5.4) | 19 (7.0) | 9 (4.1) | 9 (7.0) | 98 (5.5) |
| 50–79% | 45 (8.7) | 54 (8.0) | 28 (11.3) | 15 (7.9) | 20 (14.7) | 22 (5.1) | 50 (11.5) | 26 (9.4) | 41 (15.1) | 13 (5.9) | 10 (7.8) | 162 (9.2) |
| 49–30% | 30 (5.8) | 26 (3.8) | 9 (3.6) | 10 (5.2) | 7 (5.1) | 27 (6.2) | 23 (5.3) | 11 (4.0) | 11 (4.1) | 7 (3.2) | 3 (2.3) | 82 (4.6) |
| <30% | 22 (4.3) | 25 (3.7) | 11 (4.5) | 12 (6.3) | 3 (2.2) | 43 (9.9) | 11 (2.5) | 6 (2.2) | 3 (1.1) | 5 (2.3) | 5 (3.9) | 73 (4.1) |
| Unknown | 21 (4.1) | 32 (4.7) | 18 (7.3) | 7 (3.7) | 9 (6.6) | 26 (6.0) | 20 (4.6) | 19 (6.9) | 13 (4.8) | 8 (3.6) | 1 (0.8) | 87 (4.9) |
| Characteristics | Absenteeism (%) | Median, Day (IQR *) |
|---|---|---|
| Sex | ||
| Male | 576 (58.8) | 3 (2, 5) |
| Female | 454 (55.6) | 3 (2, 5) |
| Age in months | ||
| 6–11 | 274 (52.2) | 2 (1, 2) |
| 12–23 | 383 (55.3) | 4.5 (2.5, 7) |
| 24–35 | 150 (58.8) | 3 (2, 7) |
| 36–47 | 121 (64.4) | 5 (2, 7.5) |
| 48–59 | 102 (75.0) | 5 (3, 10) |
| Region | ||
| North | 489 (61.7) | 4.5 (2, 6) |
| South | 541 (53.8) | 2 (1, 3) |
| Province | ||
| Guangdong | 263 (58.6) | 3 (1.3, 5) |
| Henan | 227 (53.6) | 6 (3, 9) |
| Guangxi | 131 (45.5) | 4 (2, 7) |
| Sichuan | 147 (54,9) | 5 (2, 7) |
| Shandong | 169 (70.4) | 5 (2.8, 10) |
| Tianjin | 93 (71.0) | 5 (2, 7) |
| Total | 1030 (57.3) | 3 (2, 5) |
| Characteristics | Yes (%) | No (%) | p-Value |
|---|---|---|---|
| Sex | 0.500 | ||
| Male | 2183 (88.3) | 288 (11.7) | |
| Female | 2000 (89.0) | 248 (11.0) | |
| Age in months | 0.002 | ||
| 6–11 | 1690 (90.5) | 178 (9.5) | |
| 12–23 | 1414 (88.2) | 190 (11.8) | |
| 24–35 | 545 (87.9) | 75 (12.1) | |
| 36–47 | 349 (86.8) | 53 (13.2) | |
| 48–59 | 185 (82.2) | 40 (17.8) | |
| Region | <0.001 | ||
| North | 1579 (85.2) | 275 (14.8) | |
| South | 2604 (90.9) | 261 (9.1) | |
| Province | <0.001 | ||
| Guangdong | 1202 (92.2) | 101 (7.8) | |
| Henan | 878 (88.3) | 116 (11.7) | |
| Guangxi | 758 (89.6) | 88 (10.4) | |
| Sichuan | 644 (89.9) | 72 (10.1) | |
| Shandong | 446 (81.8) | 99 (18.2) | |
| Tianjin | 225 (81.0) | 60 (19.0) | |
| Total | 4183 (88.6) | 536 (11.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Ren, X.; Tian, K.; Yu, J.; Zhu, A.; Zhang, L.; Gao, G.F.; Li, Z. The Impact and Vaccination Coverage of Seasonal Influenza among Children Aged 6–59 Months in China in 2017–2018: An Internet Panel Survey. Vaccines 2022, 10, 630. https://doi.org/10.3390/vaccines10040630
Zhang H, Ren X, Tian K, Yu J, Zhu A, Zhang L, Gao GF, Li Z. The Impact and Vaccination Coverage of Seasonal Influenza among Children Aged 6–59 Months in China in 2017–2018: An Internet Panel Survey. Vaccines. 2022; 10(4):630. https://doi.org/10.3390/vaccines10040630
Chicago/Turabian StyleZhang, Hangjie, Xiang Ren, Keqing Tian, Jianxing Yu, Aiqing Zhu, Lijie Zhang, George Fu Gao, and Zhongjie Li. 2022. "The Impact and Vaccination Coverage of Seasonal Influenza among Children Aged 6–59 Months in China in 2017–2018: An Internet Panel Survey" Vaccines 10, no. 4: 630. https://doi.org/10.3390/vaccines10040630