
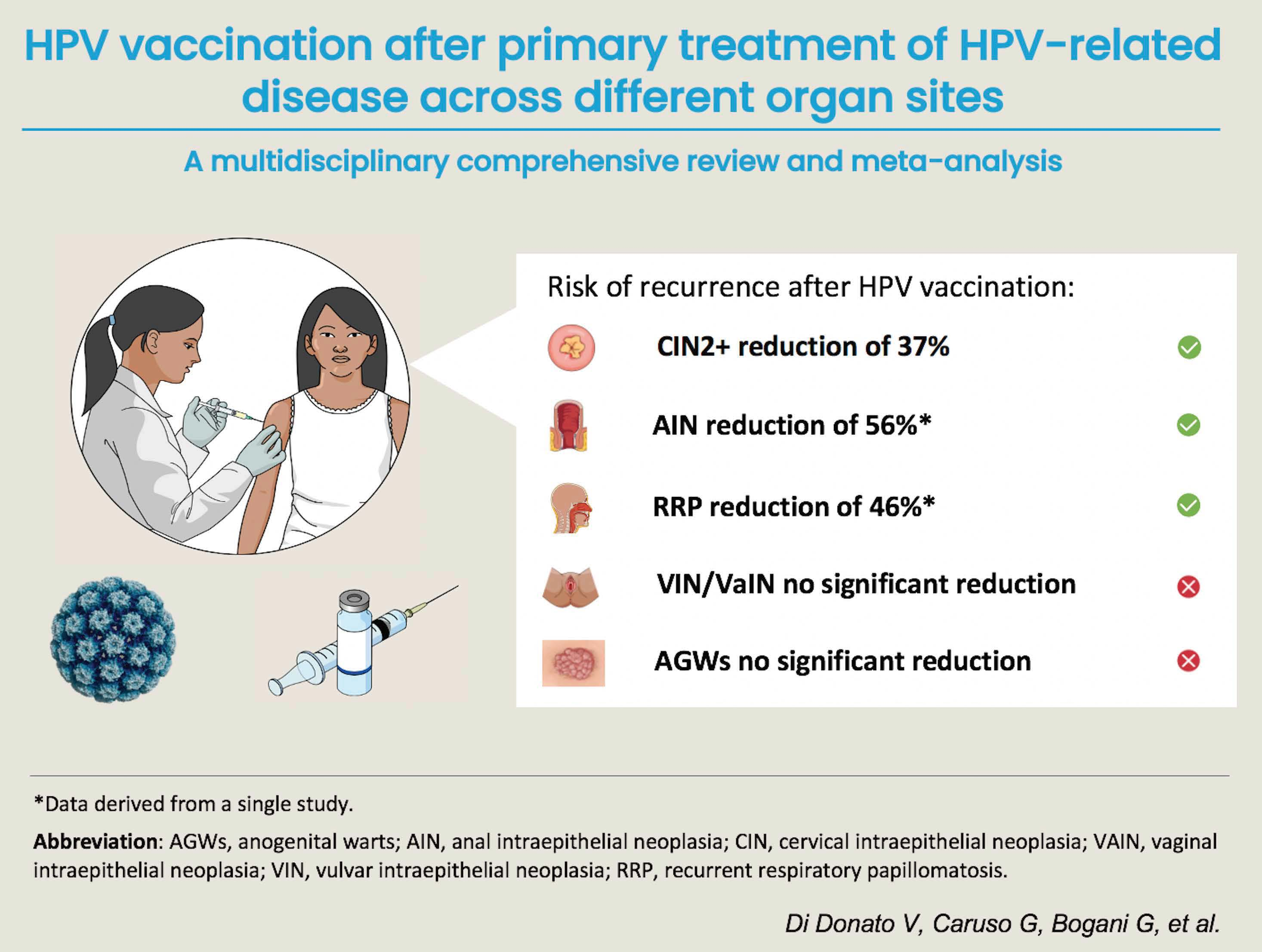
HPV Vaccination after Primary Treatment of HPV-Related Disease across Different Organ Sites: A Multidisciplinary Comprehensive Review and Meta-Analysis

 , , , , , , , , , , , , and
, , , , , , , , , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Methodologic Quality Assessment
2.3. Primary Outcomes
- Cervical intraepithelial neoplasia (CIN) recurrence;
- Anogenital warts (AGWs) recurrence;
- Vulvar intraepithelial neoplasia (VIN)/Vaginal intraepithelial neoplasia (VaIN) recurrence;
- Anal intraepithelial neoplasia (AIN) recurrence;
- Recurrent respiratory papillomatosis (RRP) recurrence;
- Penile intraepithelial neoplasia (PeIN) recurrence;
- Head and neck HPV-related disease recurrence.
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics
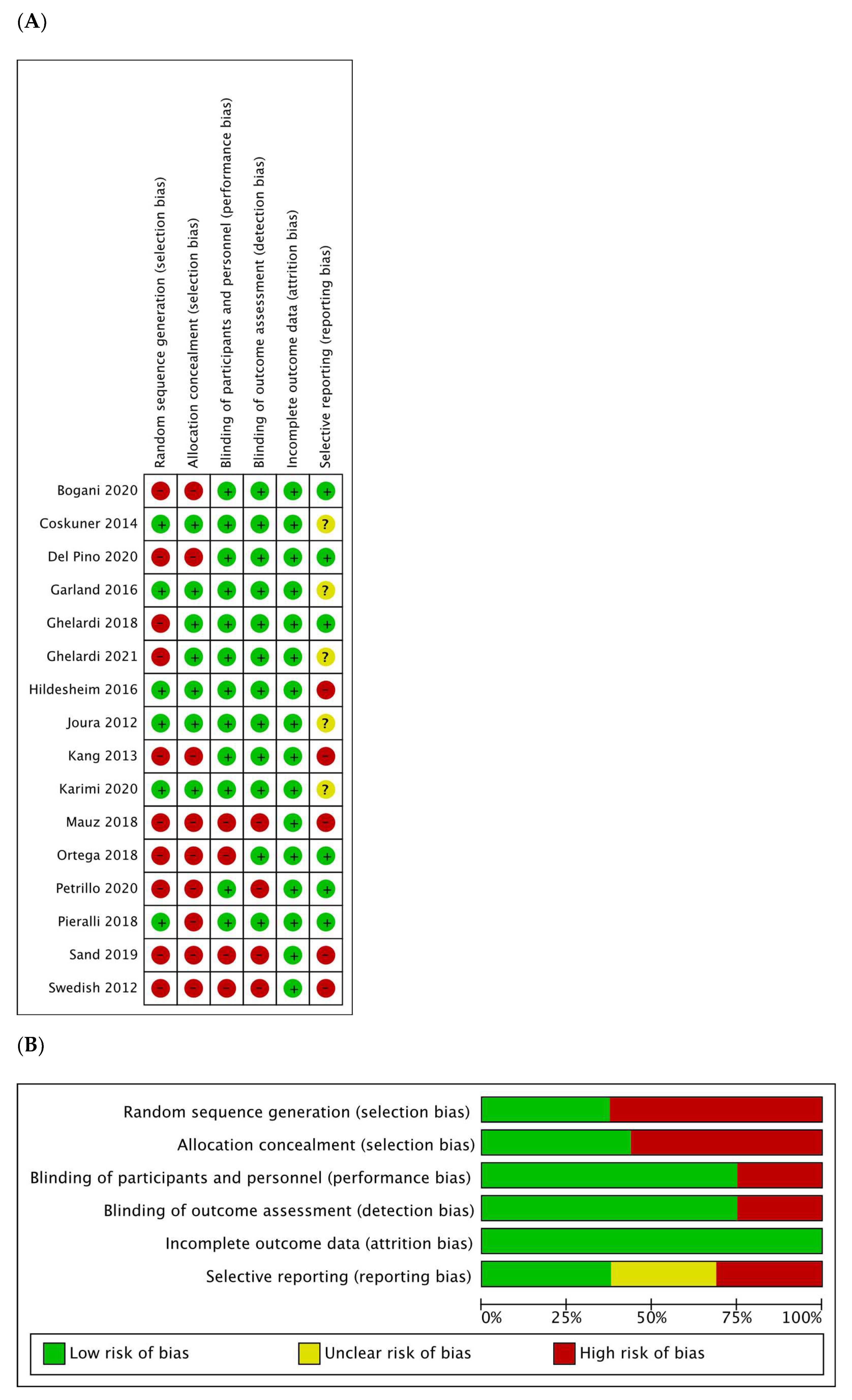
3.2. Risk of Bias
3.3. Effects of Interventions
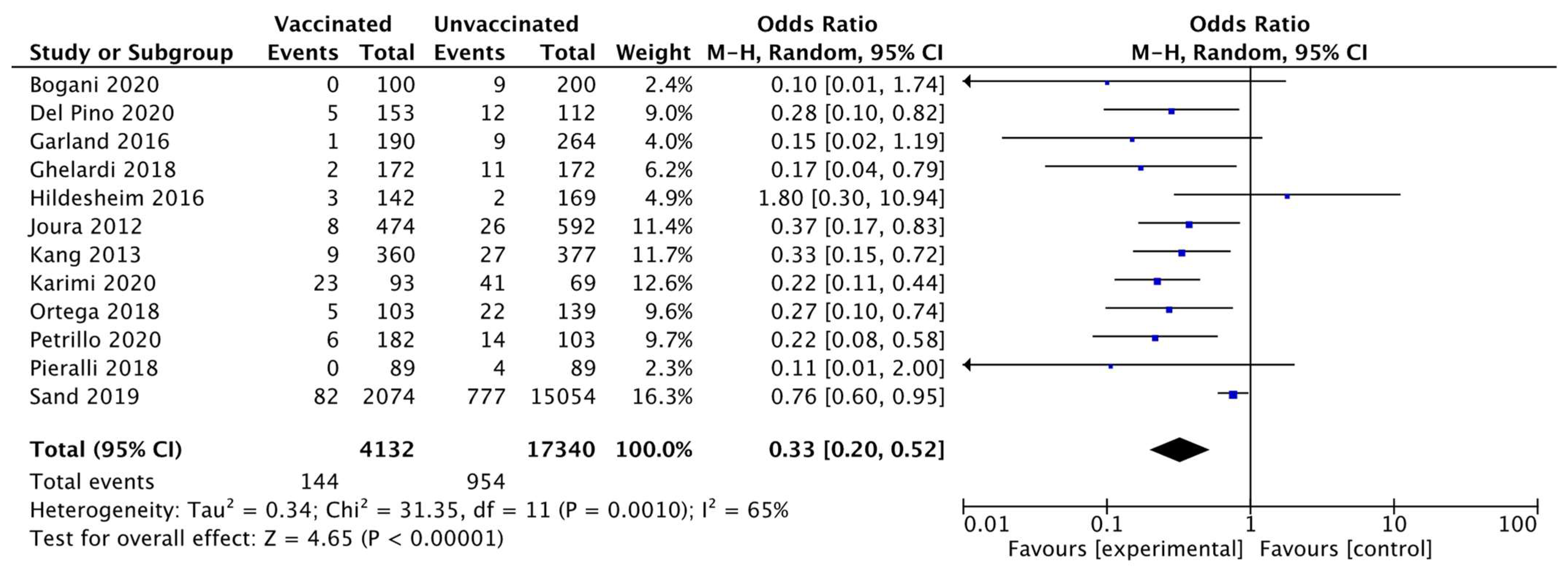
3.3.1. Cervical Intraepithelial Neoplasia Recurrence
3.3.2. Anogenital Warts Recurrence
3.3.3. Vaginal or Vulvar Intraepithelial Recurrence
3.3.4. Anal Intraepithelial Neoplasia Recurrence
3.3.5. Recurrent Respiratory Papillomatosis
3.3.6. Other Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Search Strategy (Pubmed/Medline Database)
- cervical intraepithelial neoplasia: “cervical intraepithelial neoplasia” [MeSH Terms] OR (“cervical” [All Fields] AND “intraepithelial” [All Fields] AND “neoplasia” [All Fields]) OR “cervical intraepithelial neoplasia” [All Fields] (14,638 results)
- vulvar intraepithelial neoplasia: “vulva” [MeSH Terms] OR “vulva” [All Fields] OR “vulvar” [All Fields]) AND (“carcinoma in situ” [MeSH Terms] OR (“carcinoma” [All Fields] AND “situ” [All Fields]) OR “carcinoma in situ” [All Fields] OR (“intraepithelial”[All Fields] AND “neoplasia” [All Fields]) OR “intraepithelial neoplasia” [All Fields] (1859 results)
- vaginal intraepithelial neoplasia: “vagina” [MeSH Terms] OR “vagina” [All Fields] OR “vaginal” [All Fields] OR “vaginally” [All Fields] OR “vaginals” [All Fields] OR “vaginitis” [MeSH Terms] OR “vaginitis” [All Fields] OR “vaginitides” [All Fields]) AND (“carcinoma in situ” [MeSH Terms] OR (“carcinoma”[All Fields] AND “situ” [All Fields]) OR “carcinoma in situ”[All Fields] OR (“intraepithelial”[All Fields] AND “neoplasia”[All Fields]) OR “intraepithelial neoplasia”[All Fields] (6582 results)
- anal intraepithelial neoplasia: “anal” [All Fields] AND (“carcinoma in situ” [MeSH Terms] OR (“carcinoma” [All Fields] AND “situ” [All Fields]) OR “carcinoma in situ” [All Fields] OR (“intraepithelial” [All Fields] AND “neoplasia” [All Fields]) OR “intraepithelial neoplasia” [All Fields] (1412 results)
- penile intraepithelial neoplasia: “penil” [All Fields] OR “penis” [MeSH Terms] OR “penis”[All Fields] OR “penile” [All Fields]) AND (“carcinoma in situ” [MeSH Terms] OR (“carcinoma” [All Fields] AND “situ” [All Fields]) OR “carcinoma in situ”[All Fields] OR (“intraepithelial”[All Fields] AND “neoplasia”[All Fields]) OR “intraepithelial neoplasia” [All Fields] (804 results)
- anogenital warts: “condylomata acuminata” [MeSH Terms] OR (“condylomata” [All Fields] AND “acuminata” [All Fields]) OR “condylomata acuminata” [All Fields] OR (“anogenital” [All Fields] AND “warts” [All Fields]) OR “anogenital warts” [All Fields] (6235 results)
- recurrent respiratory papillomatosis: “recurrent respiratory papillomatosis” [Supplementary Concept] OR “recurrent respiratory papillomatosis” [All Fields] OR “recurrent respiratory papillomatosis” [All Fields] (917 results)
- head and neck cancer: “head and neck neoplasms” [MeSH Terms] OR (“head” [All Fields] AND “neck” [All Fields] AND “neoplasms” [All Fields]) OR “head and neck neoplasms” [All Fields] OR (“head” [All Fields] AND “neck” [All Fields] AND “cancer” [All Fields]) OR “head and neck cancer” [All Fields] (362,181 results)
- human papillomavirus: “alphapapillomavirus” [MeSH Terms] OR “alphapapillomavirus” [All Fields] OR (“human” [All Fields] AND “papillomavirus” [All Fields]) OR “human papillomavirus” [All Fields] (44,121 results)
- HPV: “HPV” [All Fields] (47,109 results)
- vaccine: “vaccin” [Supplementary Concept] OR “vaccin” [All Fields] OR “vaccination” [MeSH Terms] OR “vaccination” [All Fields] OR “vaccinable” [All Fields] OR “vaccinal” [All Fields] OR “vaccinate” [All Fields] OR “vaccinated” [All Fields] OR “vaccinates” [All Fields] OR “vaccinating”[All Fields] OR “vaccinations”[All Fields] OR “vaccination’s” [All Fields] OR “vaccinator” [All Fields] OR “vaccinators” [All Fields] OR “vaccine’s” [All Fields] OR “vaccined” [All Fields] OR “vaccines” [MeSH Terms] OR “vaccines” [All Fields] OR “vaccine” [All Fields] OR “vaccins” [All Fields] (435,299 results)
- 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 (387,047 results)
- 9 OR 10 (57,597 results)
- 11 AND 12 AND 13 (3177 results)
References
- Sankaranarayanan, R. HPV vaccination: The most pragmatic cervical cancer primary prevention strategy. Int. J. Gynecol. Obstet. 2015, 131 (Suppl. 1), S33–S35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pils, S.; Joura, E.A. From the monovalent to the nine-valent HPV vaccine. Clin. Microbiol. Infect. 2015, 21, 827–833. [Google Scholar] [CrossRef] [Green Version]
- Radley, D.; Saah, A.; Stanley, M. Persistent infection with human papillomavirus 16 or 18 is strongly linked with high-grade cervical disease. Hum. Vaccines Immunother. 2016, 12, 768–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meites, E.; Szilagyi, P.G.; Chesson, H.W.; Unger, E.R.; Romero, J.R.; Markowitz, L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 698–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roden, R.B.S.; Stern, P.L. Opportunities and challenges for human papillomavirus vaccination in cancer. Nat. Rev. Cancer 2018, 18, 240–254. [Google Scholar] [CrossRef]
- Markowitz, L.E.; Dunne, E.F.; Saraiya, M.; Lawson, H.W.; Chesson, H.; Unger, E.R. Centers for Disease Control and Prevention (CDC); Advisory Committee on Immunization Practices (ACIP): Quadrivalent Human Papillomavirus Vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2007, 56, 1–24. [Google Scholar]
- Ranjeva, S.L.; Baskerville, E.B.; Dukic, V.; Villa, L.L.; Lazcano-Ponce, E.; Giuliano, A.R.; Dwyer, G.; Cobey, S. Recurring infection with ecologically distinct HPV types can explain high prevalence and diversity. Proc. Natl. Acad. Sci. USA 2017, 114, 13573–13578. [Google Scholar] [CrossRef] [Green Version]
- Mariz, F.C.; Bender, N.; Anantharaman, D.; Basu, P.; Bhatla, N.; Pillai, M.R.; Prabhu, P.R.; Sankaranarayanan, R.; Eriksson, T.; Pawlita, M.; et al. Peak neutralizing and cross-neutralizing antibody levels to human papillomavirus types 6/16/18/31/33/45/52/58 induced by bivalent and quadrivalent HPV vaccines. NPJ Vaccines 2020, 5, 14. [Google Scholar] [CrossRef] [Green Version]
- Athanasiou, A.; Bowden, S.; Paraskevaidi, M.; Fotopoulou, C.; Martin-Hirsch, P.; Paraskevaidis, E.; Kyrgiou, M. HPV vaccination and cancer prevention. Best Pract. Res. Clin. Obstet. Gynaecol. 2020, 65, 109–124. [Google Scholar] [CrossRef]
- Ault, K.A. Human papillomavirus vaccines and the potential for cross-protection between related HPV types. Gynecol. Oncol. 2007, 107, S31–S33. [Google Scholar] [CrossRef]
- de Vincenzo, R.; Ricci, C.; Conte, C.; Scambia, G. HPV vaccine cross-protection: Highlights on additional clinical benefit. Gynecol. Oncol. 2013, 130, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Saftlas, A.F.; Spracklen, C.N.; Ryckman, K.K.; Stockdale, C.K.; Penrose, K.; Ault, K.; Rubenstein, L.M.; Pinto, L.A. Influence of a loop electrosurgical excision procedure (LEEP) on levels of cytokines in cervical secretions. J. Reprod. Immunol. 2015, 109, 74–83. [Google Scholar] [CrossRef]
- Frazer, I.H. Interaction of human papillomaviruses with the host immune system: A well evolved relationship. Virology 2009, 384, 410–414. [Google Scholar] [CrossRef] [Green Version]
- Zurek Munk-Madsen, M.; Toft, L.; Kube, T.; Richter, R.; Ostergaard, L.; Søgaard, O.S.; Tolstrup, M.; Kaufmann, A.M. Cellular immunogenicity of human papillomavirus vaccines Cervarix and Gardasil in adults with HIV infection. Hum. Vaccines Immunother. 2018, 14, 909–916. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Madupu, R.; Karaoz, U.; Nossa, C.W.; Yang, L.; Yooseph, S.; Yachimski, P.S.; Brodie, E.L.; Nelson, K.E.; Pei, Z. Human papillomavirus community in healthy persons, defined by metagenomics analysis of human microbiome project shotgun sequencing data sets. J. Virol. 2014, 88, 4786–4797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonsson, A.; Forslund, O.; Ekberg, H.; Sterner, G.; Hansson, B.G. The Ubiquity and Impressive Genomic Diversity of Human Skin Papillomaviruses Suggest a Commensalic Nature of These Viruses. J. Virol. 2000, 74, 11636–11641. [Google Scholar] [CrossRef] [Green Version]
- Knobloch, K.; Yoon, U.; Vogt, P.M. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J. Cranio-Maxillofac. Surg. 2011, 39, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. (Updated March 2011); The Cochrane Collaboration: London, UK, 2001. [Google Scholar]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A Re-Analysis of the Cochrane Library Data: The Dangers of Unobserved Heterogeneity in Meta-Analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef]
- Joura, E.A.; Garland, S.M.; Paavonen, J.; Ferris, D.G.; Perez, G.; Ault, K.A.; Huh, W.K.; Sings, H.L.; James, M.K.; Haupt, R.M. For the FUTURE I and II Study Group, Effect of the human papillomavirus (HPV) quadrivalent vaccine in a subgroup of women with cervical and vulvar disease: Retrospective pooled analysis of trial data. BMJ 2012, 344, e1401. [Google Scholar] [CrossRef] [Green Version]
- Kang, W.D.; Choi, H.S.; Kim, S.M. Is vaccination with quadrivalent HPV vaccine after loop electrosurgical excision procedure effective in preventing recurrence in patients with high-grade cervical intraepithelial neoplasia (CIN2–3)? Gynecol. Oncol. 2013, 130, 264–268. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.M.; Paavonen, J.; Jaisamrarn, U.; Naud, P.; Salmerón, J.; Chow, S.; Apter, D.; Castellsagué, X.; Teixeira, J.C.; Skinner, S.R.; et al. For the HPV PATRICIA Study Group, Prior human papillomavirus-16/18 AS04-adjuvanted vaccination prevents recurrent high grade cervical intraepithelial neoplasia after definitive surgical therapy: Post-hoc analysis from a randomized controlled trial. Int. J. Cancer 2016, 139, 2812–2826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildesheim, A.; Gonzalez, P.; Kreimer, A.R.; Wacholder, S.; Schussler, J.; Rodriguez, A.C.; Porras, C.; Schiffman, M.; Sidawy, M.; Schiller, J.T.; et al. Impact of human papillomavirus (HPV) 16 and 18 vaccination on prevalent infections and rates of cervical lesions after excisional treatment. Am. J. Obstet. Gynecol. 2016, 215, 212.e1–212.e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghelardi, A.; Parazzini, F.; Martella, F.; Pieralli, A.; Bay, P.; Tonetti, A.; Svelato, A.; Bertacca, G.; Lombardi, S.; Joura, E.A. SPERANZA project: HPV vaccination after treatment for CIN2+. Gynecol. Oncol. 2018, 151, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Pieralli, A.; Bianchi, C.; Auzzi, N.; Fallani, M.G.; Bussani, C.; Fambrini, M.; Cariti, G.; Scarselli, G.; Petraglia, F.; Ghelardi, A. Indication of prophylactic vaccines as a tool for secondary prevention in HPV-linked disease. Arch. Gynecol. Obstet. 2018, 298, 1205–1210. [Google Scholar] [CrossRef]
- Ortega-Quiñonero, P.; Remezal-Solano, M.; Carazo-Díaz, M.C.; Prieto-Merino, D.; Urbano-Reyes, M.I.; de Guadiana-Romualdo, L.G.; Martínez-Cendán, J.P. Impact of the human papillomavirus vaccination on patients who underwent conization for high-grade cervical intraepithelial neoplasia. Eur. J. Gynaecol. Oncol. 2019, 40, 402–407. [Google Scholar]
- Sand, F.L.; Kjaer, S.K.; Frederiksen, K.; Dehlendorff, C. Risk of cervical intraepithelial neoplasia grade 2 or worse after conization in relation to HPV vaccination status. Int. J. Cancer 2020, 147, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, M.; Dessole, M.; Tinacci, E.; Saderi, L.; Muresu, N.; Capobianco, G.; Cossu, A.; Dessole, S.; Sotgiu, G.; Piana, A. Efficacy of HPV Vaccination in Women Receiving LEEP for Cervical Dysplasia: A Single Institution’s Experience. Vaccines 2020, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- del Pino, M.; Martí, C.; Torras, I.; Henere, C.; Munmany, M.; Marimon, L.; Saco, A.; Torné, A.; Ordi, J. HPV Vaccination as Adjuvant to Conization in Women with Cervical Intraepithelial Neoplasia: A Study under Real-Life Conditions. Vaccines 2020, 8, 245. [Google Scholar] [CrossRef]
- Bogani, G.; Raspagliesi, F.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Simoncini, T.; Petrillo, M.; Plotti, F.; Lopez, S.; Casarin, J.; et al. Assessing the Long-Term Role of Vaccination against HPV after Loop Electrosurgical Excision Procedure (LEEP): A Propensity-Score Matched Comparison. Vaccines 2020, 8, 717. [Google Scholar] [CrossRef]
- Karimi-Zarchi, M.; Allahqoli, L.; Nehmati, A.; Kashi, A.M.; Taghipour-Zahir, S.; Alkatout, I. Can the prophylactic quadrivalent HPV vaccine be used as a therapeutic agent in women with CIN? A randomized trial. BMC Public Health 2020, 20, 274. [Google Scholar] [CrossRef]
- Coskuner, E.R.; Ozkan, T.A.; Karakose, A.; Dillioglugil, O.; Cevik, I. Impact of the quadrivalent HPV vaccine on disease recurrence in men exposed to HPV Infection: A randomized study. J. Sex. Med. 2014, 11, 2785–2791. [Google Scholar] [CrossRef]
- Ghelardi, A.; Marrai, R.; Bogani, G.; Sopracordevole, F.; Bay, P.; Tonetti, A.; Lombardi, S.; Bertacca, G.; Joura, E.A. Surgical Treatment of Vulvar HSIL: Adjuvant HPV Vaccine Reduces Recurrent Disease. Vaccines 2021, 9, 83. [Google Scholar] [CrossRef] [PubMed]
- Swedish, K.A.; Factor, S.H.; Goldstone, S.E. Prevention of Recurrent High-Grade Anal Neoplasia with Quadrivalent Human Papillomavirus Vaccination of Men Who Have Sex with Men: A Nonconcurrent Cohort Study. Clin. Infect. Dis. 2012, 54, 891–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauz, P.S.; Schäfer, F.A.; Iftner, T.; Gonser, P. HPV vaccination as preventive approach for recurrent respiratory papillomatosis—A 22-year retrospective clinical analysis. BMC Infect. Dis. 2018, 18, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogani, G.; Raspagliesi, F.; di Donato, V.; Brusadelli, C.; Guerrisi, R.; Pinelli, C.; Casarin, J.; Ghezzi, F.; del Fabro, A.; Ditto, A.; et al. Spotlight on the role of human papillomavirus vaccines. Gynecol. Oncol. 2021, 160, 346–350. [Google Scholar] [CrossRef]
- Bogani, G.; Sopracordevole, F.; di Donato, V.; Ciavattini, A.; Ghelardi, A.; Lopez, S.; Simoncini, T.; Plotti, F.; Casarin, J.; Serati, M.; et al. High-risk HPV-positive and -negative high-grade cervical dysplasia: Analysis of 5-year outcomes. Gynecol. Oncol. 2021, 161, 173–178. [Google Scholar] [CrossRef]
- Bogani, G.; Donato, V.D.I.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Lopez, S.; Simoncini, T.; Plotti, F.; Casarin, J.; Serati, M.; et al. Recurrence rate after loop electrosurgical excision procedure (LEEP) and laser Conization: A 5-year follow-up study. Gynecol. Oncol. 2020, 159, 636–641. [Google Scholar] [CrossRef]
- di Donato, V.; Caruso, G.; Petrillo, M.; Kontopantelis, E.; Palaia, I.; Perniola, G.; Plotti, F.; Angioli, R.; Muzii, L.; Panici, P.B.; et al. Adjuvant HPV Vaccination to Prevent Recurrent Cervical Dysplasia after Surgical Treatment: A Meta-Analysis. Vaccines 2021, 9, 410. [Google Scholar] [CrossRef]
- Tumban, E. A Current Update on Human Papillomavirus-Associated Head and Neck Cancers. Viruses 2019, 11, 922. [Google Scholar] [CrossRef] [Green Version]
- Ndiaye, C.; Mena, M.; Alemany, L.; Arbyn, M.; Castellsagué, X.; Laporte, L.; Bosch, F.X.; de Sanjosé, S.; Trottier, H. HPV DNA, E6/E7 mRNA, and p16INK4a detection in head and neck cancers: A systematic review and meta-analysis. Lancet Oncol. 2014, 15, 1319–1331. [Google Scholar] [CrossRef]
- Marur, S.; D’Souza, G.; Westra, W.H.; Forastiere, A.A. HPV-associated head and neck cancer: A virus-related cancer epidemic. Lancet Oncol. 2010, 11, 781–789. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, K.J.; Jakobsen, K.K.; Jensen, J.S.; Grønhøj, C.; von Buchwald, C. The Effect of Prophylactic HPV Vaccines on Oral and Oropharyngeal HPV Infection—A Systematic Review. Viruses 2021, 13, 1339. [Google Scholar] [CrossRef] [PubMed]
- Näsman, A.; Du, J.; Dalianis, T. A global epidemic increase of an HPV-induced tonsil and tongue base cancer—Potential benefit from a pan-gender use of HPV vaccine. J. Intern. Med. 2020, 287, 134–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, K.; Grønhøj, C.; Hahn, C.H.; von Buchwald, C. Therapeutic human papillomavirus vaccines in head and neck cancer: A systematic review of current clinical trials. Vaccine 2018, 36, 6594–6605. [Google Scholar] [CrossRef]
- Dion, G.R.; Teng, S.; Boyd, L.R.; Northam, A.; Mason-Apps, C.; Vieira, D.; Amin, M.R.; Branski, R.C. Adjuvant Human Papillomavirus Vaccination for Secondary Prevention: A Systematic Review. JAMA Otolaryngol.—Head Neck Surg. 2017, 143, 614. [Google Scholar] [CrossRef]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [Green Version]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef] [Green Version]
- Jones, R.W.; Rowan, D.M.; Stewart, A.W. Vulvar intraepithelial neoplasia: Aspects of the natural history and outcome in 405 women. Obstet. Gynecol. 2005, 106, 1319–1326. [Google Scholar] [CrossRef]
- Karita, H.C.S.; Hauge, K.; Magaret, A.; Mao, C.; Schouten, J.; Grieco, V.; Xi, L.F.; Galloway, D.A.; Madeleine, M.M.; Wald, A. Effect of Human Papillomavirus Vaccine to Interrupt Recurrence of Vulvar and Anal Neoplasia (VIVA): A Trial Protocol. JAMA Netw. Open 2019, 2, e190819. [Google Scholar] [CrossRef] [Green Version]
- Chesson, H.W.; Ekwueme, D.U.; Saraiya, M.; Watson, M.; Lowy, D.R.; Markowitz, L.E. Estimates of the annual direct medical costs of the prevention and treatment of disease associated with human papillomavirus in the United States. Vaccine 2012, 30, 6016–6019. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year | Study Design | N. of Patients Age (Years) | Primary Endpoint (Recurrence) | HPV Vaccine Type and Time of Vaccination | Standard Treatment |
|---|---|---|---|---|---|
| CIN | |||||
| Joura et al., 2012 [20] | Post-hoc-pooled analysis of 2 RCT (FUTURE I and II) Follow-up 2.5 years (median) | 1066 15–26 | CIN 1+ CIN 2+ CIN 3 | 4-valent at day 1, month 2, and month 6 after surgery | LEEP (84.7%), cervical conization (12.5%), cryotherapy (0.7%), and other NA (2.1%) |
| Kang et al., 2013 [21] | Retrospective case-control Follow-up 3.5 years (median) | 737 20–45 | CIN 1+ CIN 2+ | 4-valent at week 1, month 2, and month 6 after surgery | LEEP |
| Garland et al., 2016 [22] | Post-hoc analysis of an RCT (PATRICIA) Follow-up 4 years | 454 15–25 | CIN 1+ CIN 2+ | 2-valent at months 0, 1, and 6 after surgery | LEEP |
| Hildesheim et al., 2016 [23] | Subgroup analysis of an RCT Follow-up 27.3 mo (median) | 311 18–25 | CIN 1+ CIN 2+ | 2-valent, 3 doses over 6 months after surgery | LEEP |
| Ghelardi et al., 2018 [24] | Prospective case-control (SPERANZA project) Follow-up 4 years | 344 18–45 | CIN 1+ CIN 2+ | 4-valent at day 30, month 2, and month 6 after surgery | LEEP |
| Pieralli et al., 2018 [25] | RCT Follow-up 3 years | 178 <45 | CIN 1+ CIN 2+ | 4-valent at months 0, 2 and 6 after surgery | Conization (83%), other NA (17%) |
| Ortega-Quinonero et al., 2019 [24,26] | Retrospective Follow-up 2 years | 242 18–65 | CIN 2+ | 2-/4-valent, first dose 0–1 month before or 0–1 month after surgery, other 2 doses over 6 months | LEEP |
| Sand et al., 2020 [27] | Prospective cohort | 17,128 17–51 | CIN 2+ | 2-/4-valent, first dose 0–3 months before or 0–12 months after surgery | Conization |
| Petrillo et al., 2020 [28] | Retrospective Follow-up 2 years | 285 32–47 | CIN 1+ CIN 2+ | 2-/4-valent, first dose 0–1 month after surgery | LEEP |
| Del Pino et al., 2020 [29] | Prospective Follow up 22.4 mo median | 265 26–64 | CIN 2+ | 2-valent at 0, 1 and 6 months after surgery 4-valent at 0, 2 and 6 months after surgery | Conization |
| Bogani et al., 2020 [30] | Retrospective, multicenter Follow-up 5 years | 300 18–89 | CIN 2+ | 2-/4-valent | LEEP |
| Karimi et al., 2020 [31] | RCT Follow-up 2 years | 242 28–36 | CIN 1+ CIN 2+ | 4-valent at months 0, 2 and 6 after conservative treatment | LEEP/Conization |
| AGWs | |||||
| Coskuner et al., 2014 [32] | RCT Follow-up 1 year | 171 men 26–42 | AGWs | 4-valent at months 0, 2 and 6 | Electrocautery ± local excision |
| Joura et al., 2012 [20] | Post-hoc-pooled analysis of 2 RCT (FUTURE I and II) Follow-up 2.5 years (median) | 485 15–26 | AGWs | 4-valent at day 1, month 2, and month 6 after surgery | Surgery |
| VIN | |||||
| Ghelardi et al., 2021 [33] | Prospective case-control Follow-up 2–7 years | 118 18–45 | VIN | 4-valent at day 1, month 2, and month 6 after surgery | Electrosurgical excision and/or laser vaporisation |
| Joura et al., 2012 [20] | Post-hoc-pooled analysis of 2 RCT (FUTURE I and II) Follow-up 2.5 years (median) | 622 15–26 | VIN | 4-valent at day 1, month 2, and month 6 after surgery | Surgery |
| AIN | |||||
| Swedish et al., 2012 [34] | Retrospective cohort study Follow-up 2 years | 202 men who had sex with men 20–72 | HGAIN | 4-valent at day 1, month 2, and month 6 after surgery | Local excision or ablation |
| RRP | |||||
| Mauz et al., 2018 [35] | Retrospective monocentric study Follow-up 7 years | 24 2–48 | RRP | 4-valent at day 0, week 8, and month 6 after surgery | Microdebridement and intralesional Cidofovir injection |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Donato, V.; Caruso, G.; Bogani, G.; Cavallari, E.N.; Palaia, G.; Perniola, G.; Ralli, M.; Sorrenti, S.; Romeo, U.; Pernazza, A.; et al. HPV Vaccination after Primary Treatment of HPV-Related Disease across Different Organ Sites: A Multidisciplinary Comprehensive Review and Meta-Analysis. Vaccines 2022, 10, 239. https://doi.org/10.3390/vaccines10020239
Di Donato V, Caruso G, Bogani G, Cavallari EN, Palaia G, Perniola G, Ralli M, Sorrenti S, Romeo U, Pernazza A, et al. HPV Vaccination after Primary Treatment of HPV-Related Disease across Different Organ Sites: A Multidisciplinary Comprehensive Review and Meta-Analysis. Vaccines. 2022; 10(2):239. https://doi.org/10.3390/vaccines10020239
Chicago/Turabian StyleDi Donato, Violante, Giuseppe Caruso, Giorgio Bogani, Eugenio Nelson Cavallari, Gaspare Palaia, Giorgia Perniola, Massimo Ralli, Sara Sorrenti, Umberto Romeo, Angelina Pernazza, and et al. 2022. "HPV Vaccination after Primary Treatment of HPV-Related Disease across Different Organ Sites: A Multidisciplinary Comprehensive Review and Meta-Analysis" Vaccines 10, no. 2: 239. https://doi.org/10.3390/vaccines10020239