
Fast, Reliable, and Simple Point-of-Care-like Adaptation of RT-qPCR for the Detection of SARS-CoV-2 for Use in Hospital Emergency Departments


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Sample Collection
2.2. Sample Processing, RNA Isolation and RT-qPCR
2.3. Generation of RT-qPCR Titration Curves
2.4. Statistical Analysis
3. Results
3.1. Adaptation and Validation of the Allplex SARS-CoV-2 qPCR Assay into a Direct qPCR Assay
3.2. Adaptation of dqPCR into a Point-of-Care Type dqPCR for SARS-CoV-2 Detection in a Clinical Setting
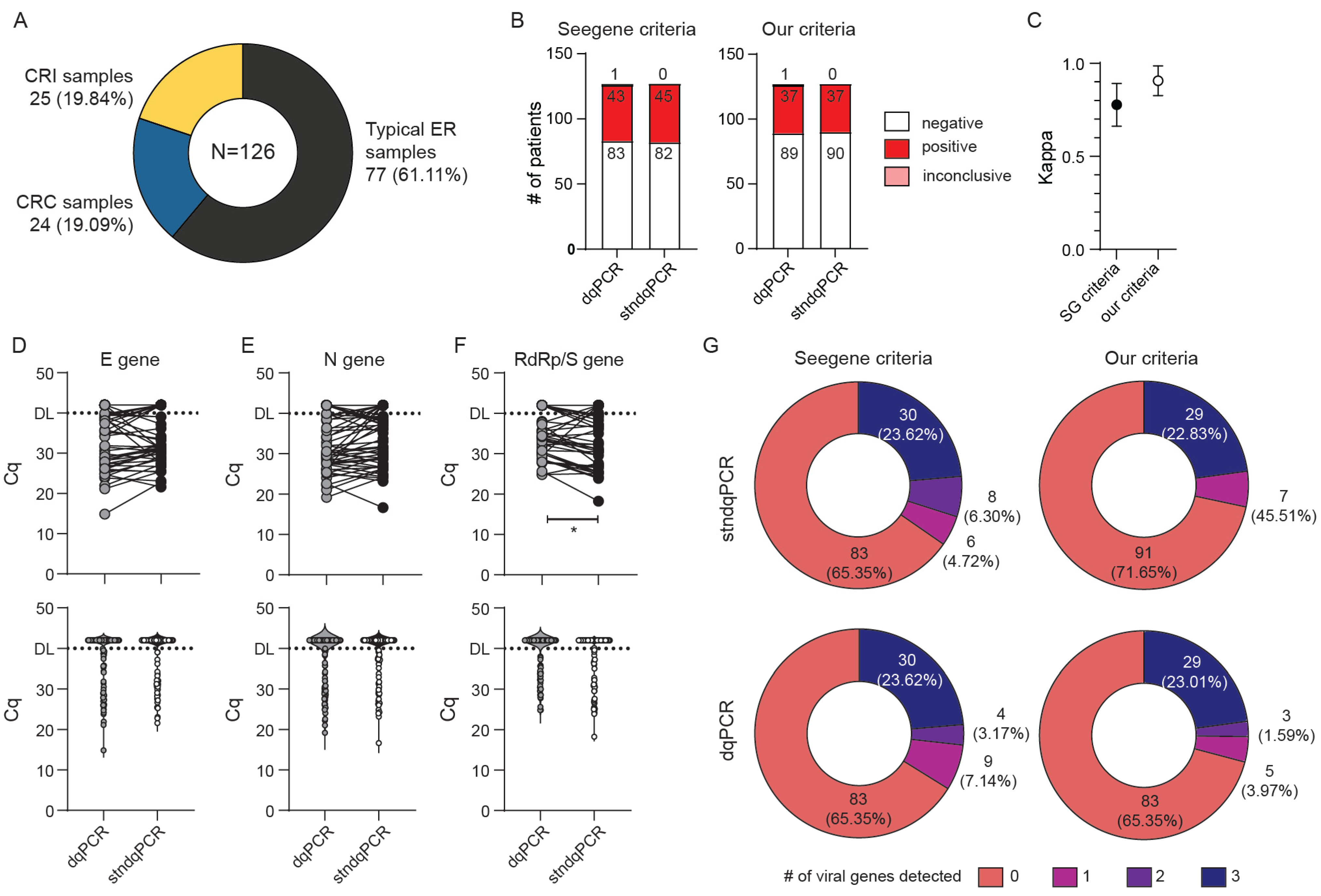
3.3. Validation of dqPCR Procedure Using Standardized Samples and Application to Pooled Sample Analyses
3.4. Application of POC-dqPCR within the ED Department—A 4-Month Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chirico, F.; Nucera, G.; Magnavita, N. COVID-19: Protecting healthcare workers is a priority. Infect. Control. Hosp. Epidemiol. 2020, 41, 1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yang, S.; Hung, M.; Tong, W.; Liu, Y. Protecting healthcare workers amid the COVID-19 crisis: A safety protocol in wuhan. Front. Public Health 2020, 8, 577499. [Google Scholar] [CrossRef] [PubMed]
- Premraj, A.; Aleyas, A.G.; Nautiyal, B.; Rasool, T.J. Nucleic acid and immunological diagnostics for SARS-CoV-2: Processes, platforms and pitfalls. Diagnostics 2020, 10, 866. [Google Scholar] [CrossRef] [PubMed]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M.; Butler, J.C. SARS-CoV-2 transmission from people without COVID-19 symptoms. JAMA Netw. Open 2021, 4, e2035057. [Google Scholar] [CrossRef] [PubMed]
- Muller, C.P. Do asymptomatic carriers of SARS-CoV-2 transmit the virus? Lancet Reg. Health Eur. 2021, 4, 100082. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of asymptomatic SARS-CoV-2 infection: A narrative review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef]
- Larremore, D.B.; Wilder, B.; Lester, E.; Shehata, S.; Burke, J.M.; Hay, J.A.; Tambe, M.; Mina, M.J.; Parker, R. Test sensitivity is secondary to frequency and turnaround time for COVID-19 screening. Sci. Adv. 2021, 7, 5393. [Google Scholar] [CrossRef] [PubMed]
- Freund, Y. The challenge of emergency medicine facing the COVID-19 outbreak. Eur. J. Emerg. Med. 2020, 27, 155. [Google Scholar] [CrossRef]
- Bruce, E.A.; Huang, M.L.; Perchetti, G.A.; Tighe, S.; Laaguiby, P.; Hoffman, J.J.; Gerrard, D.L.; Nalla, A.K.; Wei, Y.; Greninger, A.L.; et al. Direct RT-qPCR detection of SARS-CoV-2 RNA from patient nasopharyngeal swabs without an RNA extraction step. PLoS Biol. 2020, 18, e3000896. [Google Scholar] [CrossRef]
- Lübke, N.; Senff, T.; Scherger, S.; Hauka, S.; Andrée, M.; Adams, O.; Timm, J.; Walker, A. Extraction-free SARS-CoV-2 detection by rapid RT-qPCR universal for all primary respiratory materials. J. Clin. Virol. 2020, 130, 104579. [Google Scholar] [CrossRef] [PubMed]
- Smyrlaki, I.; Ekman, M.; Lentini, A.; de Sousa, N.R.; Papanicolaou, N.; Vondracek, M.; Aarum, J.; Safari, H.; Muradrasoli, S.; Rothfuchs, A.G.; et al. Massive and rapid COVID-19 testing is feasible by extraction-free SARS-CoV-2 RT-PCR. Nat. Commun. 2020, 11, 4812. [Google Scholar] [CrossRef] [PubMed]
- Kriegova, E.; Fillerova, R.; Kvapil, P. Direct-RT-qPCR detection of SARS-CoV-2 without RNA extraction as part of a COVID-19 testing strategy: From sample to result in one hour. Diagnostics 2020, 10, 605. [Google Scholar] [CrossRef] [PubMed]
- Avetyan, D.; Chavushyan, A.; Ghazaryan, H.; Melkonyan, A.; Stepanyan, A.; Zakharyan, R.; Hayrapetyan, V.; Atshemyan, S.; Martirosyan, G. SARS-CoV-2 detection by extraction-free qRT-PCR for massive and rapid COVID-19 diagnosis during a pandemic in Armenia. J. Virol. Methods 2021, 295, 114199. [Google Scholar] [CrossRef] [PubMed]
- Freppel, W.; Merindol, N.; Rallu, F.; Bergevin, M. Efficient SARS-CoV-2 detection in unextracted oro-nasopharyngeal specimens by rRT-PCR with the Seegene Allplex 2019-nCoV assay. Virol. J. 2020, 17, 196. [Google Scholar] [CrossRef] [PubMed]
- Freire-Paspuel, B.; Garcia-Bereguiain, M.A. Analytical and clinical evaluation of “AccuPower SARS-CoV-2 multiplex RT-PCR kit (Bioneer, South Korea)” and “allplex 2019-nCoV Assay (Seegene, South Korea)” for SARS-CoV-2 RT-PCR diagnosis: Korean CDC EUA as a quality control proxy for developing countries. Front. Cell Infect. Microbiol. 2021, 11, 630552. [Google Scholar] [PubMed]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Ferland, L.; Carvalho, C.; Dias, J.G.; Lamb, F.; Adlhoch, C.; Suetens, C.; Beauté, J.; Kinross, P.; Plachouras, D.; Hannila-Handelberg, T.; et al. Risk of hospitalization and risk of death for health care workers with COVID-19 in nine European countries, January 2020-January 2021. J. Hosp. Infect. 2021, 21, 6701. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.-T.; Liu, Z.-D.; Fan, Z.-W.; Zhao, L.; Cao, W.-C. Epidemiology of and risk factors for COVID-19 infection among health care workers: A multi-centre comparative study. Int. J. Environ. Res. Public Health 2020, 17, 7149. [Google Scholar] [CrossRef]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020, 20, 1401–1408. [Google Scholar] [CrossRef]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in health-care workers: A living systematic review and meta-analysis of prevalence, risk factors, clinical characteristics, and outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Singanayagam, A.; Patel, M.; Charlett, A.; Bernal, J.L.; Saliba, V.; Ellis, J.; Ladhani, S.; Zambon, M.; Gopal, R. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Eurosurveillance 2020, 25, 2001483. [Google Scholar] [CrossRef]
- La Scola, B.; Le Bideau, M.; Andreani, J.; Hoang, V.T.; Grimaldier, C.; Colson, P.; Gautret, P.; Raoult, D. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1059–1061. [Google Scholar] [CrossRef]
- Bal, A.; Brengel-Pesce, K.; Gaymard, A.; Quéromès, G.; Guibert, N.; Frobert, E.; Bouscambert, M.; Trabaud, M.A.; Allantaz-Frager, F.; Oriol, G.; et al. Clinical and laboratory characteristics of symptomatic healthcare workers with suspected COVID-19: A prospective cohort study. Sci. Rep. 2021, 11, 14977. [Google Scholar] [CrossRef]
- Braunstein, G.D.; Schwartz, L.; Hymel, P.; Fielding, J. False positive results with SARS-CoV-2 RT-PCR tests and how to evaluate a RT-PCR-positive test for the possibility of a false positive result. J. Occup. Environ. Med. 2021, 63, e159–e162. [Google Scholar] [CrossRef]
- Merindol, N.; Pépin, G.; Marchand, C.; Rheault, M.; Peterson, C.; Poirier, A.; Houle, C.; Germain, H.; Danylo, A. SARS-CoV-2 detection by direct rRT-PCR without RNA extraction. J. Clin. Virol. 2020, 128, 104423. [Google Scholar] [CrossRef] [PubMed]
- Lan, L.; Xu, D.; Ye, G.; Xia, C.; Wang, S.; Li, Y.; Xu, H. Positive RT-PCR test results in patients recovered from COVID-19. JAMA 2020, 323, 1502–1503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, A.T.; Tong, Y.X.; Zhang, S. Profile of RT-PCR for SARS-CoV-2: A preliminary study from 56 COVID-19 patients. Clin. Infect. Dis. 2020, 71, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Sender, R.; Bar-On, Y.M.; Gleizer, S.; Bernshtein, B.; Flamholz, A.; Phillips, R.; Milo, R. The total number and mass of SARS-CoV-2 virions. Proc. Natl. Acad. Sci. USA 2021, 118, e2024815118. [Google Scholar] [CrossRef] [PubMed]
- Drew, R.J.; O’Donnell, S.; LeBlanc, D.; McMahon, M.; Natin, D. The importance of cycle threshold values in interpreting molecular tests for SARS-CoV-2. Diagn. Microbiol. Infect. Dis. 2020, 98, 115130. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedure | stndqPCR | dqPCR |
|---|---|---|
| RNA isolation | On-column RNA isolation from 140 µL of UTM with 10 µL of IC added prior to isolation. Eluted into 50 µL of MG water. | None |
| Virus inactivation | None 1 | Aliquot of cca 1 mL heated at 70 °C for 10 min |
| qPCR reaction | 5 µL purified RNA sample 5 µL MOM 5 µL EM8 5 µL MG water | 10 µL heat inactivated sample 5 µL MOM 5 µL EM8 1 µL IC |
| Outcome | Seegene (SG) Criteria | Our Criteria |
|---|---|---|
| SARS-CoV-2 positive | Amplification of any SARS-CoV-2 specific amplicon (N, RdRp/S plus/minus E gen) at Cq < 40. | Amplification of any SARS-CoV-2 specific amplicon (N, RdRp/S) at Cq < 37 or two viral amplicons at Cq < 38. |
| SARS-CoV-2 negative | No amplification or Cq ≥ 40 for all viral amplicons. Cq for IC < 40. | No amplification or amplification of virus amplicons at Cq ≥ 38 or amplification of any single virus amplicon at Cq ≥ 37. Cq for IC < 37. The analysis is repeated if Cq for IC is ≥ 37. |
| Presumptive | Amplification of just E gene at Cq < 40. | Does not exist in our criteria. |
| Inconclusive | Does not exist in Seegene criteria. | Amplification of any SARS-CoV-2 specific amplicon—one (N, RdRp/S) at Cq ≥ 37 or two viral amplicons (E and N, E and RdRp/S, N and RdRp/S) at Cq ≥ 38. |
| Invalid | No amplification of any amplicons. | No amplification of any amplicons and IC ≥ 37. |
| Month | Criteria | Negative | Positive | Inconclusive | Presumptive | Invalid | Not Retested | Total |
|---|---|---|---|---|---|---|---|---|
| Month 1 | SG | 90.35% (1086) | 7.65% (92) | NA | 1.08% (13) | 0.92% (11) | 0.00% (0) | 1202 |
| OC | 89.93% (1081) | 3.49% (42) | 5.24% (63) | NA | 1.16% (14) | 0.17% (2) | ||
| Month 2 | SG | 95.84% (1795) | 2.78% (52) | NA | 0.11% (2) | 0.80% (15) | 0.48% (9) | 1873 |
| OC | 95.14% (1782) | 1.76% (33) | 1.12% (21) | NA | 0.85% (16) | 1.12% (21) | ||
| Month 3 | SG | 87.97% (2931) | 9.93% (331) | NA | 0.60% (20) | 1.23% (41) | 0.27% (9) | 3332 |
| OC | 87.15% (2904) | 8.37% (279) | 2.13% (71) | NA | 2.13% (46) | 0.00% (0) | ||
| Month 4 | SG | 83.20% (3169) | 14.49% (552) | NA | 1.00% (38) | 1.18% (45) | 0.13% (5) | 3809 |
| OC | 81.67% (3111) | 10.06% (383) | 5.41% (206) | NA | 1.47% (56) | 1.39% (53) |
| Month | Criteria | Negative | Positive | Inconclusive | Presumptive | Invalid | Not Retested | NR PP | Total |
|---|---|---|---|---|---|---|---|---|---|
| Month 1 | SG | 46.15% (6) | 0.00% (0) | NA | 0.00% (0) | 0.00% (0) | 53.84% (7) | 0.00% (0) | 13 |
| OC | 35.71 (20) | 0.00% | 0.00% (0) | NA | 0.00% (0) | 60.71% (34) | 3.57% (2) | 56 | |
| Month 2 | SG | 50.00% (1) | 0.00% (0) | NA | 0.00% (0) | 0.00% (0) | 50.00% (1) | 0.00 (0) | 2 |
| OC | 55.00% (11) | 10.00% (2) | 5.00% (1) | NA | 0.00% (0) | 20.00% (4) | 10% (2) | 20 | |
| Month 3 | SG | 47.06% (8) | 17.65% (3) | NA | 0.00% (0) | 0.00% (0) | 29.41% (5) | 5.88% (1) | 17 |
| OC | 33.87% (21) | 8.06% (5) | 0.00% (0) | NA | 0.00% (0) | 40.32% (25) | 17.74% (11) | 62 | |
| Month 4 | SG | 51.52% (17) | 0.00% (0) | NA | 0.00% (0) | 0.00% (0) | 48.48% (16) | 0.00% (0) | 33 |
| OC | 28.11% (52) | 4.32% (8) | 2.70% (5) | NA | 0.00% (0) | 61.08% (113) | 3.78% (7) | 185 |
| Month | E (Cq) | N (Cq) | RdRp/S (Cq) | Available Clinical Data at Time of Testing |
|---|---|---|---|---|
| Month 2 | 39.87 30.27 | 39.40 29.80 | NA 33.35 | known COVID patient treated in critical care |
| NA NA | 39.72 Other lab | NA Other lab | newly diagnosed, with pneumonia | |
| Month 3 | 34.13 23.48 | NA 25.27 | NA 33.03 | newly diagnosed, mild upper respiratory symptoms |
| 38.2 Other lab | NA Other lab | NA Other lab | known COVID patient | |
| 39.91 34.43 | NA 33.67 | NA NA | newly diagnosed, asymptomatic, surveillance testing | |
| 39.53 Other lab | NA Other lab | NA Other lab | newly diagnosed, asymptomatic, dialysis patient | |
| 39.04 Other lab | 37.16 Other lab | 38.9 Other lab | known COVID patient | |
| Month 4 | NA Other lab | 39,93 Other lab | NA Other lab | known COVID patient |
| NA Other lab | 37.74 Other lab | NA Other lab | known COVID patient | |
| NA Other lab | 39.54 Other lab | 39.99 Other lab | newly diagnosed, surveillance testing | |
| NA NA Other lab | 39.34 38.,51 Other lab | NA NA Other lab | newly diagnosed, surveillance testing | |
| NA 30.35 | 38.83 29.85 | NA 36.53 | newly diagnosed, treated for deep vein thrombosis, no respiratory symptoms | |
| NA 36,3 | 37,04 33,49 | NA NA | newly diagnosed, critical-care patient, had respiratory symptoms for 7 days before first test | |
| NA 34.18 | 37.74 33.28 | NA NA | newly diagnosed, asymptomatic | |
| NA Other lab | 37.36 Other lab | NA Other lab | newly diagnosed, had respiratory symptoms for 14 days prior to testing |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavletić, M.; Mazor, M.; Lerga, M.; Mileta, T.; Železnjak, J.; Ružić, T.; Ravlić, S.; Palčevski, D.; Kirinčić, J.; Mežnarić, S.; et al. Fast, Reliable, and Simple Point-of-Care-like Adaptation of RT-qPCR for the Detection of SARS-CoV-2 for Use in Hospital Emergency Departments. Viruses 2021, 13, 2413. https://doi.org/10.3390/v13122413
Pavletić M, Mazor M, Lerga M, Mileta T, Železnjak J, Ružić T, Ravlić S, Palčevski D, Kirinčić J, Mežnarić S, et al. Fast, Reliable, and Simple Point-of-Care-like Adaptation of RT-qPCR for the Detection of SARS-CoV-2 for Use in Hospital Emergency Departments. Viruses. 2021; 13(12):2413. https://doi.org/10.3390/v13122413
Chicago/Turabian StylePavletić, Martina, Marija Mazor, Mate Lerga, Tatjana Mileta, Jelena Železnjak, Tina Ružić, Sanda Ravlić, Dora Palčevski, Jelena Kirinčić, Silvestar Mežnarić, and et al. 2021. "Fast, Reliable, and Simple Point-of-Care-like Adaptation of RT-qPCR for the Detection of SARS-CoV-2 for Use in Hospital Emergency Departments" Viruses 13, no. 12: 2413. https://doi.org/10.3390/v13122413