1. Introduction
Cardiovascular disease is responsible for a substantial part of mortality among the elderly and patients with diabetes, chronic kidney disease (CKD), hypertension, and osteoporosis. Vascular media calcification (i.e., so-called arteriosclerosis or Mönckeberg’s sclerosis) is a prominent aspect of cardiovascular disease in these patient populations. Vascular calcification is an active cell-regulated process in which the vascular smooth muscle cells (VSMCs) play a prominent role [
1].
One of the key events during the vascular calcification process is the transdifferentiation of VSMCs, a process that now potentially affords the capacity for being exploited as an important therapeutic target [
2]. Since transdifferentiated VSMCs actively deposit hydroxyapatite in the medial layer, it is generally accepted that they transdifferentiate towards an osteoblast/chondrocyte phenotype. However, since VSMCs originate from mesenchymal stem cells, dedifferentiated VSMCs could theoretically also transdifferentiate towards adipocytes instead of osteoblasts/chondrocytes. The phenotypic fate of cells depends on their exposure to extracellular stimuli, which will activate or inhibit different sets of signaling pathways. Osteoblast and chondrocyte differentiation is under the control of Wnt/β-catenin signaling. Peroxisome proliferator-activated receptor γ (PPARγ) signaling, on the other hand, is a strong inducer of adipocyte differentiation. In this context, it is worth mentioning that a regulating effect of PPARγ signaling on the vascular calcification process has been reported [
3,
4]. A regulatory protein that acts on both pathways is sclerostin [
5,
6]. Sclerostin is best known as an inhibitor of canonical Wnt/β-catenin signaling within the bone formation process. However, recent studies showed that sclerostin can also enhance adipocyte differentiation [
6]. In this context, it is important to recognize that in recent years, sclerostin has received growing interest with regard to its potential role in the development of vascular calcification, in addition to its effects on bone metabolism. An association between increased serum sclerostin levels and decreased mortality has been observed in hemodialysis patients [
7,
8]. This is in accordance with the concept that sclerostin may prevent/inhibit vascular calcifications in a manner reminiscent of its inhibitory action on bone formation, thereby reducing mortality. On the other hand, sclerostin, the expression of which until recently was thought to be confined to osteocytes, has now also been demonstrated in VSMCs and valve tissue adjacent to areas of calcification [
9,
10,
11]. Furthermore, CKD patients with aortic calcifications were found to have higher serum sclerostin levels compared with CKD patients without vascular calcification [
9,
10,
12]. In this context, it is worth mentioning that renal elimination of sclerostin increases with declining renal function [
13]. Moreover, sclerostin is a positively charged molecule which is easily filtered by the negatively charged glomerular membrane [
14]. Taken together, this allows us to put forward the hypothesis that sclerostin, originating from excessive local production in calcified vessels, may spill over to the serum by which it may prevent further progression of (vascular) calcifications and contribute to the high incidence of low bone turnover in CKD patients [
15].
In general, the precise role of sclerostin in VSMC transdifferentiation and the development of vascular calcifications, as well as its potential role in the bone–vascular axis, is poorly understood. This issue should be of particular clinical interest given the recent therapeutic introduction of an antisclerostin antibody treatment to stimulate bone formation [
16]. Since clinical data have shown an inverse association between circulating sclerostin levels and mortality in dialysis patients [
7], concerns have been raised about the cardiovascular safety of drugs targeting sclerostin [
17]. Furthermore, the ARCH study recently revealed that romosozumab, an antisclerostin antibody, increased the risk of serious adverse cardiovascular events in postmenopausal women with osteoporosis [
18].
To investigate our theory that sclerostin, produced by VSMCs in calcified vessels, may spill over to the serum and thereby, next to impacting the bone, prevent further progression of (vascular) calcifications, a rat warfarin model was employed. In contrast to other models of vascular calcification (animal models for CKD, diabetes, or osteoporosis), this model induces vascular calcifications in the absence of underlying bone pathologies. Hence, the disturbed mineral metabolism in CKD, diabetes, and osteoporosis patients (and animal models) seriously complicates the mechanistic understanding of bone–vascular interactions. In our experimental subjects, warfarin exposure prevented the production of biologically active matrix γ-carboxyglutamic acid protein (MGP) [
19,
20]. MGP is a local inhibitor of vascular calcification and in order to become biologically active, the protein undergoes post-translational γ-glutamyl carboxylation. This process, which takes place in concert with vitamin K (vitK) as a cofactor [
21], is prevented by warfarin since it inhibits vitK recycling. Furthermore, Beazley et al. demonstrated that activation of Wnt/β-catenin signaling was involved in warfarin-induced VSMC transdifferentiation, which resulted in calcification of the medial layers of the arterial wall [
22]. Nevertheless, the exact role of sclerostin in the VSMC transdifferentiation process, as well as its role in the bone–vascular axis, has not been thoroughly investigated so far in this model. Therefore, in this study, a time-dependent characterization of this model at the level of the vessels and the bone was coupled to an in-depth investigation of sclerostin biology.
3. Discussion
Many aspects of the vascular media calcification process remain cryptic. Although being generally accepted as the key event during the development of vascular calcification, knowledge of VSMC transdifferentiation is rather fragmentary. Moreover, at this stage, it is not clear which molecules exactly are key in the linkage between bone and vascular pathology (bone–vascular axis). Since the disturbed mineral and bone metabolism in CKD patients further complicates the understanding of the mechanisms underlying the bone–vascular coupling, an experimental animal model with warfarin-induced vascular calcification was applied in this study. This model gave us the opportunity to investigate vascular calcification and the bone–vascular axis, regardless of CKD-induced disturbed mineral balance and the resulting bone pathology. Indeed, serum calcium and phosphorous levels were similar between control and warfarin-exposed rats.
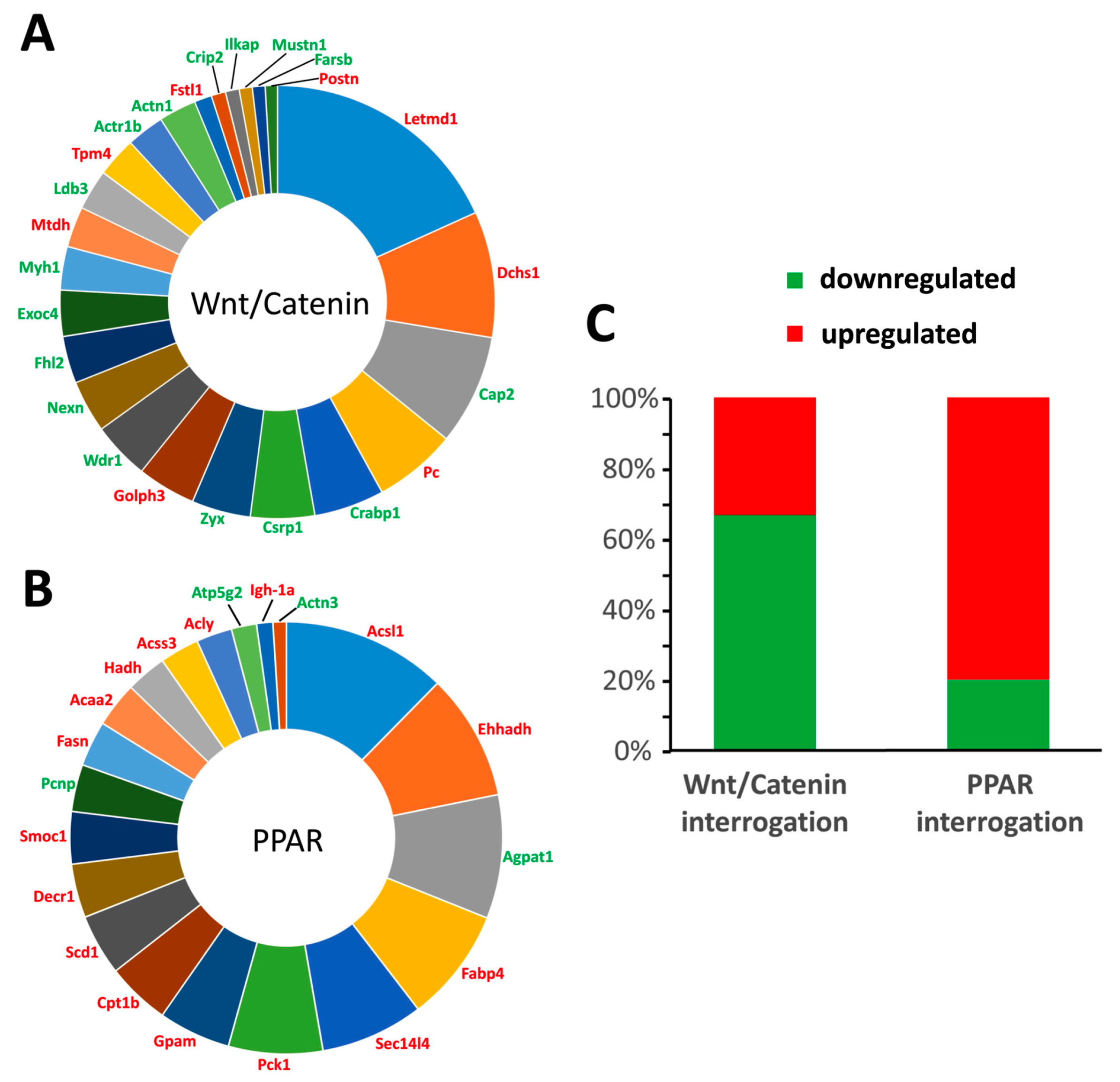
During the vascular calcification process, one of the key events is the transdifferentiation of VSMCs [
2]. Given the fact that VSMCs are of mesenchymal origin and that transdifferentiation of VSMCs induces soft tissue mineralization, a potential transdifferentiation towards an osteoblastic phenotype seems logical. Nevertheless, by further investigating the transdifferentiation process by means of an unbiased quantitative proteomic approach (isobaric tag for relative and absolute quantitation (iTRAQ) protein labeling and mass spectrometry), we showed that next to osteoblastic transdifferentiation involving Wnt/β-catenin signaling, adipocytic transdifferentiation as evidenced by PPARγ signaling was also evident. The latter finding thus is highly indicative of PPARγ signaling functioning as a regulatory factor during the vascular calcification process. Furthermore, it argues for the local vascular action of sclerostin by regulating the balance between both differentiation pathways, that is, inhibiting Wnt/β-catenin signaling on the one hand and inducing PPARγ signaling on the other.
An inverse relationship exists in the adipogenic and osteogenic lineage commitment, which may indicate that promoting the adipocyte phenotype may exert antagonistic effects on calcification, which is in line with the fact that PPARγ signaling counteracts vascular calcifications [
3,
4,
23] and our hypothesis that sclerostin may inhibit vascular calcification.
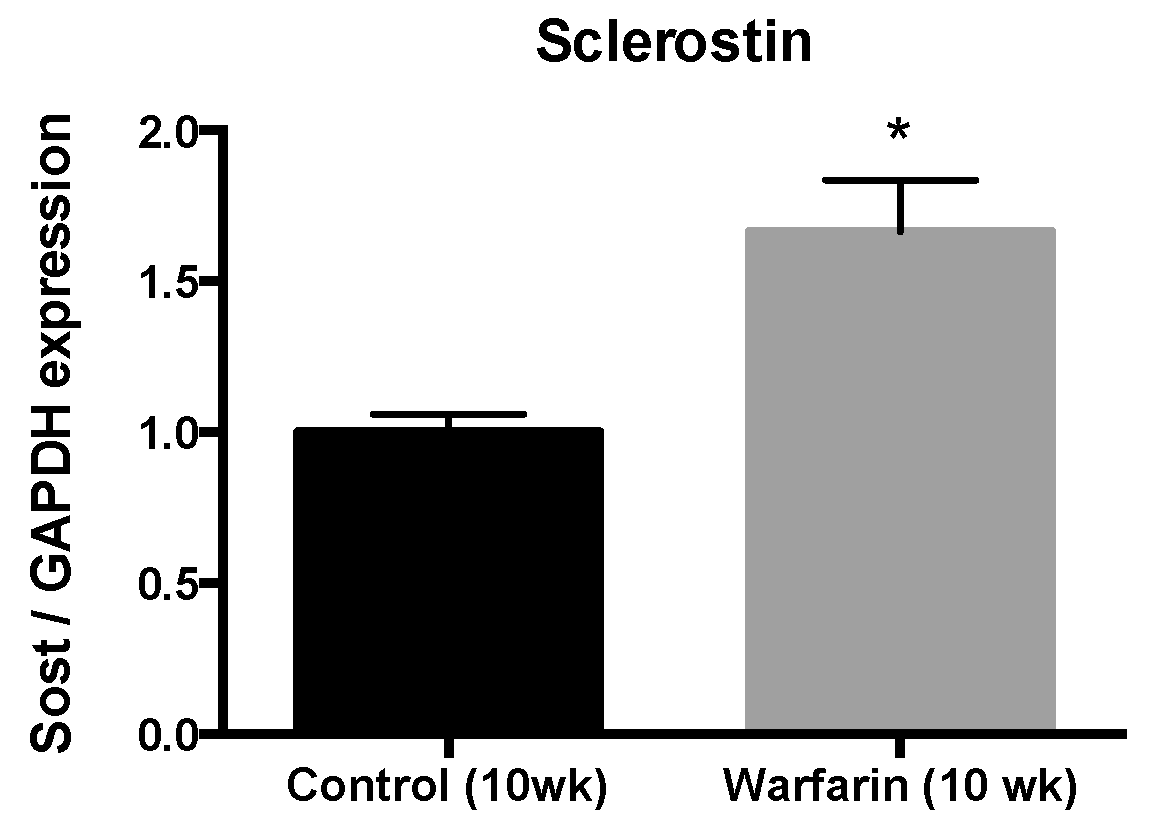
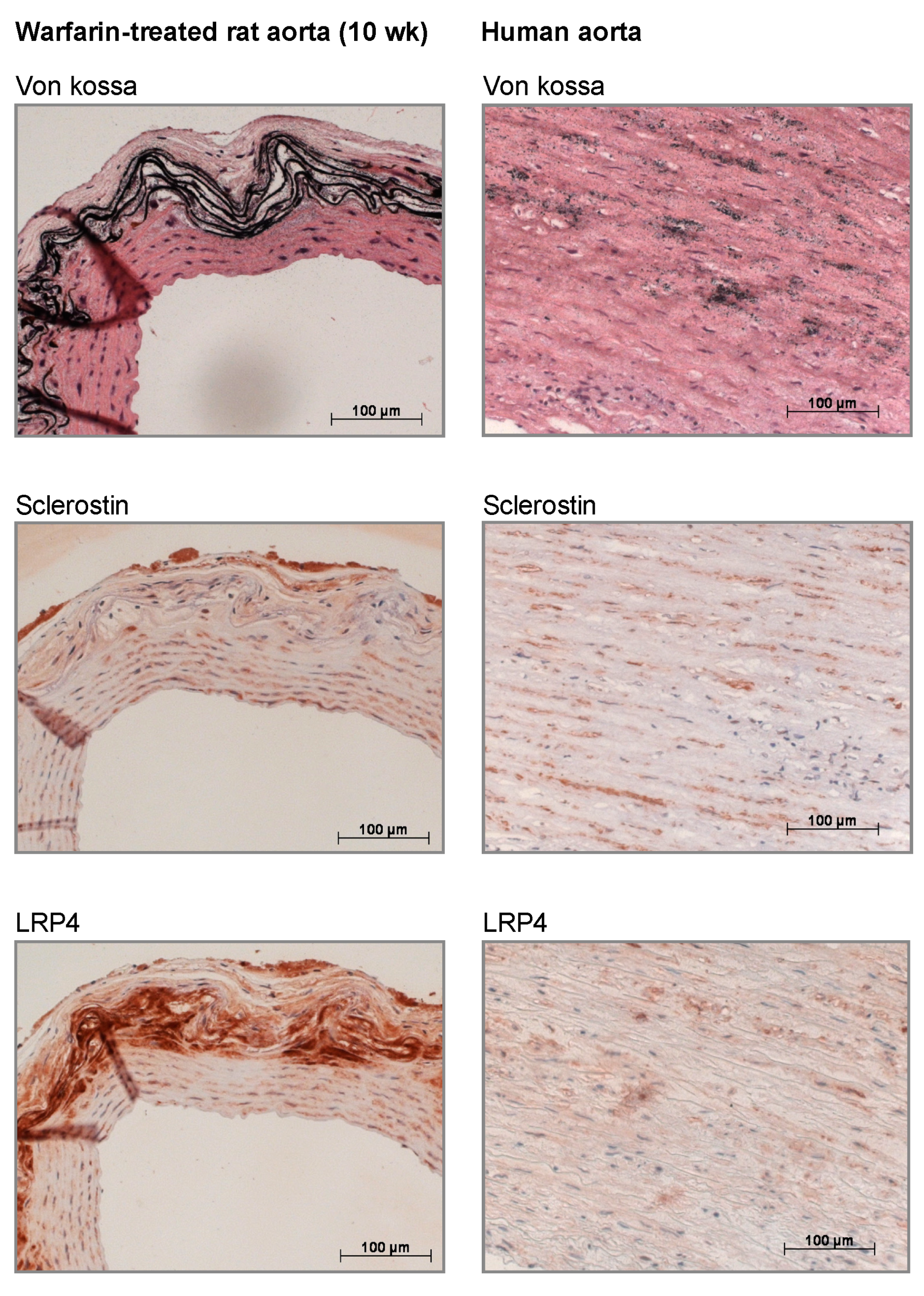
In our current study, we found that sclerostin was expressed at both the mRNA and protein level in calcified vessels, which is in line with earlier studies [
9,
11,
24]. Furthermore, LRP4 protein expression was strongly upregulated in the calcified vessels. LRP4 functions as an anchor for sclerostin in the bone [
25,
26]. Recently, we demonstrated that mice lacking functional LRP4 expression profoundly lacked sclerostin-positive osteocytes in contrast to wild-type mice, where >30% of osteocytes stained positive for sclerostin [
25]. More importantly, LRP4 transgenic mice showed a similar phenotype compared to that of SOST (the gene encoding sclerostin) knockout mice [
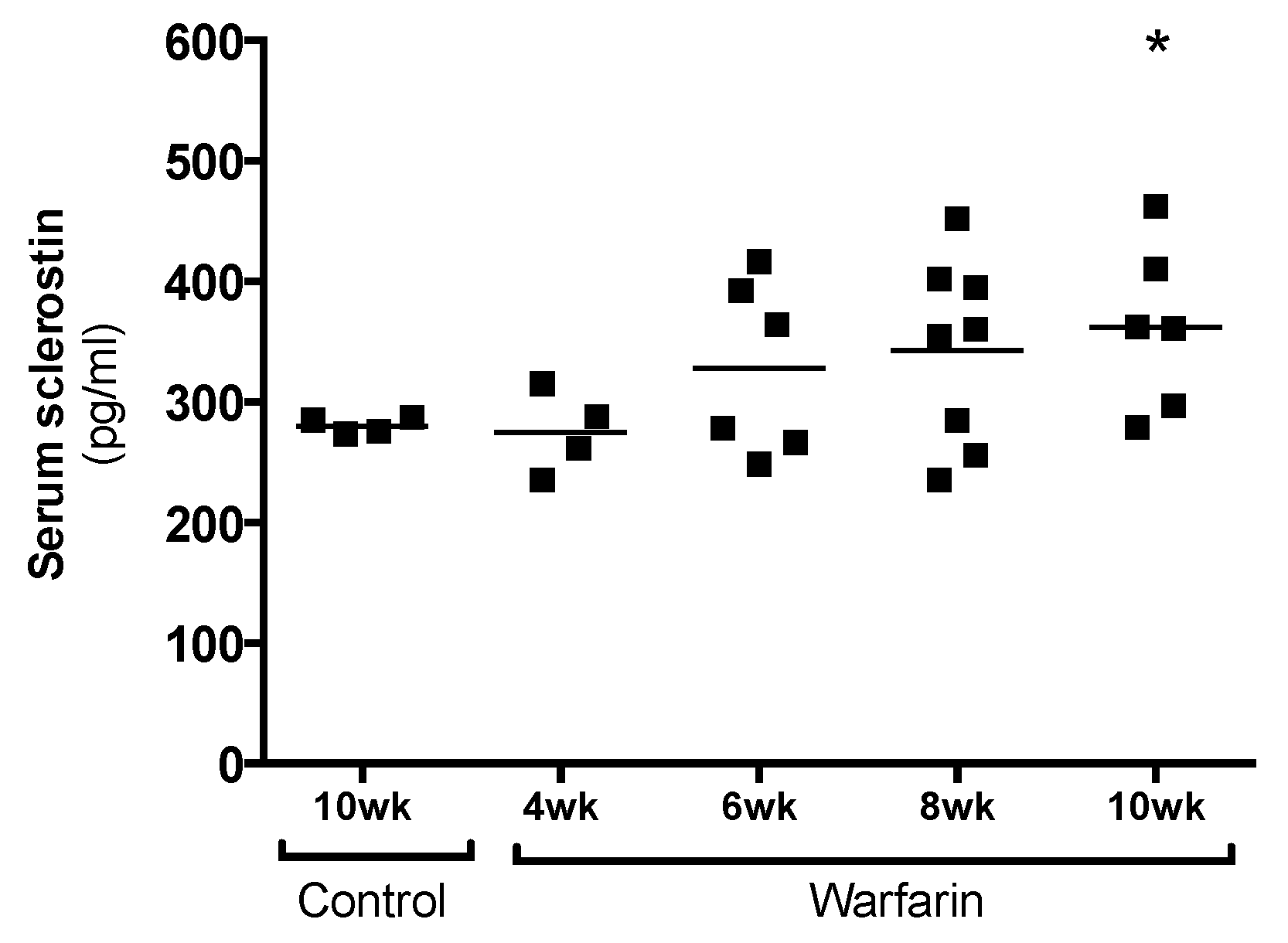
25]. The fact that LRP4 is clearly present in calcified vessels while virtually absent in normal vessels indicates that the sclerostin produced in the vessels is likely retained there to act locally. Moreover, the fact that we not only localized LRP4 and sclerostin in rat but also human calcified vessels underlines the clinical relevance of our findings. In addition to being retained in the vessels through LRP4 binding, part of the sclerostin produced in the vessels is likely to spill over to the serum. This was hypothesized earlier in a previous study by our group in which sclerostin was quantified in the serum of hemodialysis patients either clear of or presenting with vascular calcification [
7]. This may also explain the gradual increase in serum sclerostin levels of animals with progressing ectopic vascular calcification, as observed in our present study.
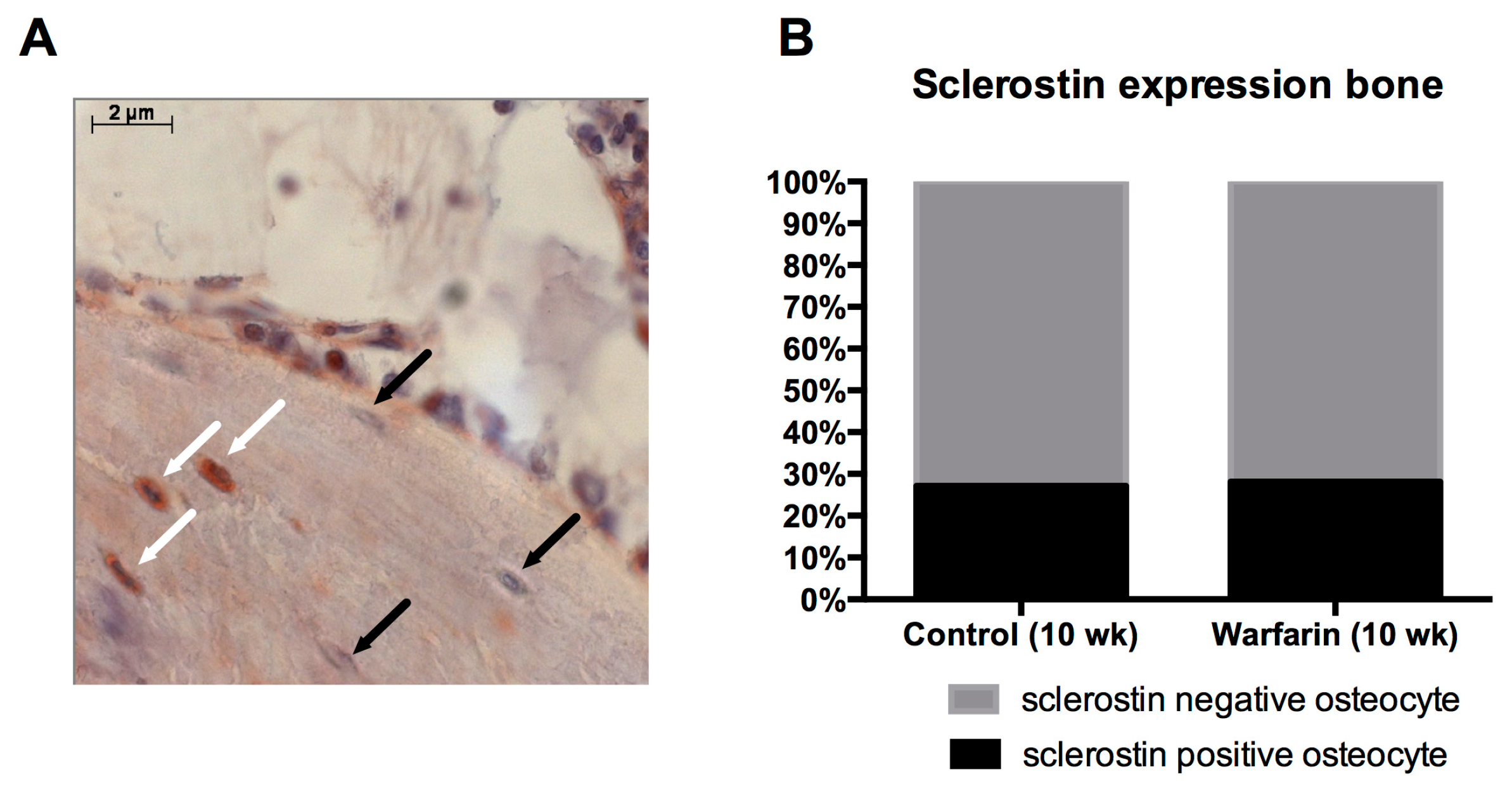
Osteocytic sclerostin production was investigated to ensure that the elevated serum sclerostin levels were due to sclerostin production by calcified vessels and did not originate from the osteocytes, which are the main source of sclerostin. Our finding that no differences were observed in the number of sclerostin-expressing osteocytes between control and warfarin-exposed rats strongly indicates that the bone is not likely to be responsible for the observed increased serum levels of sclerostin. Furthermore, we recently found sclerostin protein in the cell culture medium of in vitro calcifying VSMCs, proving that VSMCs should be able to secrete sclerostin towards the circulation (unpublished results).
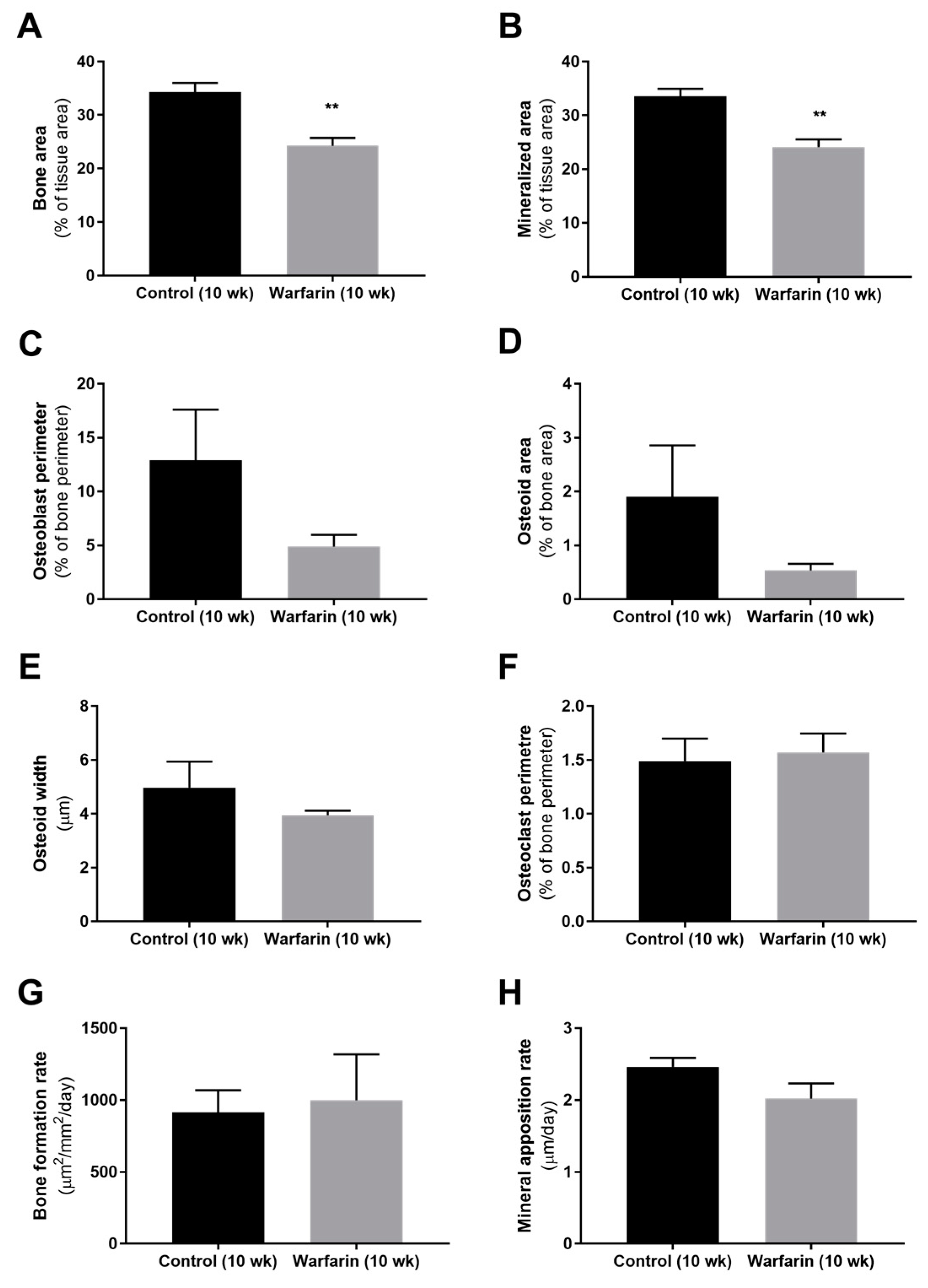
Bone histomorphometric analysis of warfarin-exposed animals revealed a mildly, however significantly decreased (mineralized) bone area after 10 weeks of warfarin exposure compared with control rats. This finding is in line with the decreased (although not significant) number of osteoblasts (osteoblast perimeter) and reduced (not significant) amount of associated osteoid material found. Mineralization of the deposited osteoid, however, remained intact, as reflected by the absence of any difference in osteoid width and mineral apposition rate. As indicated by the osteoclast perimeter, bone resorption also did not differ between groups. Given the particular role that has been ascribed to sclerostin at the level of the bone [
27], the rather mild effects on the bone observed in our present study can be potentially explained by the significant increase in vascular-derived serum sclerostin levels and are compatible with the contribution of vascular sclerostin to the high incidence of low bone turnover in CKD patients.
This study has a few limitations. Since this study was originally designed to only assess the degree of vascular calcification due to warfarin treatment, no urine was collected. Being able to measure the creatinine content in the urine would have made it possible to calculate the glomerular filtration rate (GFR), which is based on the measurement of urine and serum creatinine concentrations and the urinary volume, this is a more accurate measure of kidney function compared with serum creatinine concentration. Future experiments are needed to investigate to what extent increased renal production of sclerostin, in addition to calcified VSMC, contributes to increased serum levels of this protein.
Overall, this study demonstrated that the sclerostin biology in an animal model of vascular calcification is in agreement with the role of this protein in the vascular calcification process and the pathologically disturbed bone–vascular axis in patients suffering from vascular calcifications. Similar to its function in bone, it could be assumed that sclerostin is produced as a negative feedback mechanism to prevent excessive calcification. These results urge the investigation of the vascular safety of antisclerostin antibody treatment, which currently is ongoing in our laboratory. Hence, antisclerostin treatment is being developed as a bone anabolic treatment for patients with osteoporosis, who are at the same time at risk for vascular calcifications.
4. Materials and Methods
4.1. Statement of Ethics
All experimental procedures were conducted in compliance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals 85-23 (1996) and approved by the University of Antwerp Ethical Committee for Animal Experiments. The experimental procedure involving human arterial sections was approved by the ethics committee of the University of Antwerp (A03 043) on 18 December 2014.
4.2. Animals
Thirty 8-week-old male Wistar rats (Iffa Credo, Brussels, Belgium) were housed in standard cages (two per cage) at constant temperature and humidity and exposed to a 12 h light/dark cycle. All rats had free access to tap water and their assigned diet.
4.3. Induction of Vascular Calcification in the Rat Model
The animals were randomly assigned to the following experimental groups: control group (10 weeks (wk), n = 4) and warfarin-exposed groups (4 wk, n = 4; 6 wk, n = 6; 8 wk, n = 8; 10 wk, n = 8). Control rats were fed standard pellet chow for 10 weeks. Rats receiving the warfarin-containing diet (3 mg warfarin/g diet and 1.5 mg vitamin K1/g diet [
20], SSNIFF Spezialdiäten, Soest, Germany) were sacrificed at different time points (4, 6, 8, or 10 weeks) in order to evaluate the onset and further progression of vascular calcification.
4.4. Human Tissue
Human arterial tissue sections, obtained in the frame of organ donation, were used for histological purposes. After von Kossa staining, four male subjects were identified with severe vascular calcifications. These subjects were then selected for further immunohistochemical evaluation.
4.5. Serum Markers of Bone Metabolism and Renal Function
At sacrifice, rats were exsanguinated via the retro-orbital plexus after anesthesia with sodium pentobarbital (60 mg/kg, i.p., Nembutal, Ceva Santé Animale, Libourne, France) via intraperitoneal injection. Serum creatinine was measured according to the Jaffé method. Calcium levels were determined using flame atomic absorption spectrometry (Perkin-Elmer, Waltham, MA, USA) after diluting the sample in 0.1% La(NO3)3 to prevent chemical interference. Serum phosphorus levels were measured using the Ecoline®S Phosphate kit (Diasys, Holzheim, Germany).
4.6. Evaluation of Molecular Signaling Pathways Involved in VSMC Transdifferentiation
Mass spectrometry and quantitative proteomics (using iTRAQ labeling) were performed on the aortic samples of control rats and rats exposed to warfarin for 10 weeks. The aorta samples were ground completely in a protein extraction buffer (8 M urea, 2 M thiourea, 0.1% SDS in 50 mM triethylammonium bicarbonate solution). The concentrations of the proteins extracted from the aorta were quantified using the reducing agent and detergent compatible (RCDC) protein assay kit (Bio-Rad, Hercules, CA, USA). Equal amounts of proteins from each sample were reduced and alkylated by tris-2-carboxyethyl phosphine and 5-methyl-methanoethiosulphate, respectively, before trypsin digestion. The resulting peptides from each sample were labeled using iTRAQ reagents (Sciex, Redwood City, CA, USA) following the manufacturer’s instructions. To improve LC-MS/MS proteome coverage, samples were subjected to a 2D-LC fractionation system (Dionex ULTIMATE 3000, ThermoScientific, Waltham, MA, USA). The mixed peptides were first fractionated on a strong cationic exchange chromatography polysulfoethyl aspartamide column (1 × 150 mm, (Dionex)) and secondly separated on a nano-LC C18 column (200 Å, 2 μm, 75 μm × 25 cm (Dionex)). The nano-LC was coupled online to a QExactive™-Plus Orbitrap (ThermoScientific) mass spectrometer. The nano-LC eluents were infused to the Orbitrap mass spectrometer with a capillary at 1.7 KV on a nanoelectrospray ionization (nano-ESI) source at a flow rate of 300 nL/min. Data-dependent acquisition in positive ion mode was performed for a selected mass range of 350–1800 m/z at MS1 level (140,000 resolution) and MS2 level (17,500 resolution). The raw data were analyzed by Proteome Discoverer 2.0 software (ThermoScientific) using Sequest HT as search engine against the rattus norvegicus UniProt/SwissProt database with a threshold of confidence above 99% (false discovery rate less than 1%). The list of identified proteins containing iTRAQ ratios of expression levels over control samples was then generated.
4.7. Bioinformatic Analysis
Proteins identified according to the statistical MS cut-offs described previously were then subsequently used for bioinformatic analyses. To identify the significantly altered proteins (i.e., proteins differentially expressed due to warfarin exposure), raw iTRAQ ratios (control:warfarin) were first log
2 transformed. Following log
2 ratio transformation, differentially expressed protein (DEP) lists were created by identifying only proteins that possessed log
2-transformed iTRAQ ratios two standard deviations (
p < 0.05) from the calculated mean background expression variation level. Significant DEP lists (comprising proteins elevated or reduced in their expression in response to warfarin) were then employed for further bioinformatics deconvolution using diverse informatics platforms including Ingenuity Pathway. LSA of the warfarin DEP lists was performed as previously described using GeneIndexer [
28]. LSA is a computational natural language processing investigation technique capable of elucidating latent prosaic connections between interrogator concepts (e.g., biomedical phrases such as PPAR) and biomedical terms (e.g., a specific protein gene symbol).
4.8. Evaluation of Vascular Calcification
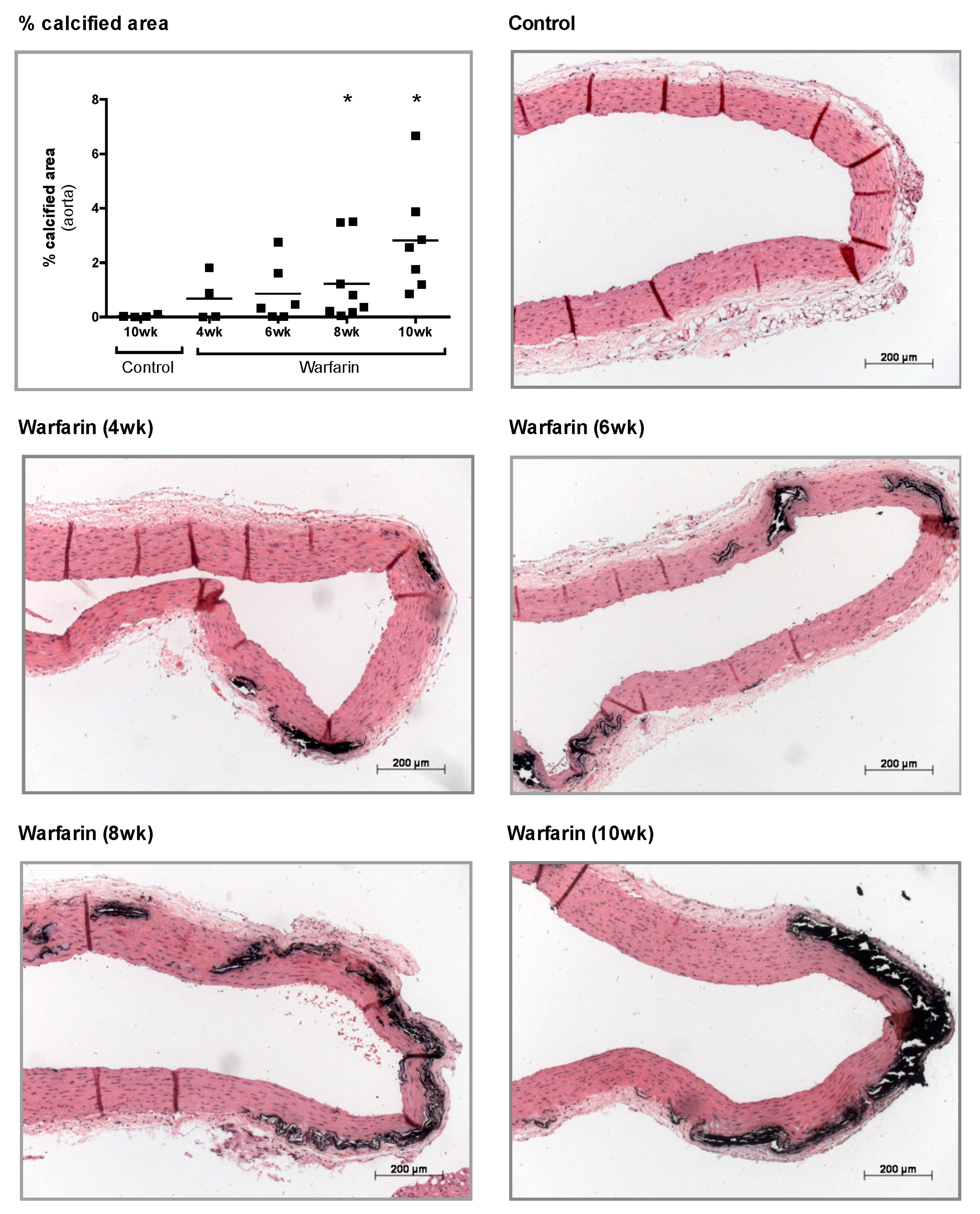
At sacrifice, aorta, left femoral, and left carotid arteries were isolated. For histological analyses, thoracic aortae were fixed in neutral buffered formalin for 90 min and cut into 2–3 mm thick rings. These rings were then embedded upright in paraffin, of which 4 μm sections were cut and stained for calcification with von Kossa and counterstained with hematoxylin and eosin (H&E). Calcification was evaluated using Axiovision image analysis software (Release 4.5, Carl Zeiss, Oberkochen, Germany). Two color thresholds allowed separation of the calcified area (von Kossa positive, black areas) and the remaining tissue area. The percentage calcified area is defined as the von Kossa positive area versus the total tissue area (von Kossa positive area plus the remaining tissue area).
To determine the calcium content, the proximal part of the abdominal aorta, the left carotid, and femoral arteries were weighed on a precision balance. The tissue samples were then digested overnight in 65% HNO3 at 60 °C, followed by dilution in 0.1% La(NO3)3 to eliminate chemical interference during flame atomic absorption spectrometry. Results were expressed as mg calcium/g wet tissue.
4.9. Evaluation of Bone Metabolism
To allow histomorphometric analysis of dynamic bone parameters, all animals received an intraperitoneal injection of 30 mg/kg tetracycline and 25 mg/kg demeclocycline 7 and 3 days before sacrifice, respectively. At sacrifice, the left tibia was isolated and fixed overnight in 70% ethanol. After dehydration and embedding in 100% methyl methacrylate (Merck, Hohenbrunn, Germany), 5 µm thick sections were stained by the method of Goldner for quantitative histology to determine static bone parameters using Axiovision image analysis software (Release 4.5, Carl Zeiss, Oberkochen, Germany). Total bone area, mineralized bone area, osteoid width and area, osteoblast perimeter, eroded perimeter, osteoclast perimeter, and trabecular number were measured using this software platform. Unstained sections of the tibia (10 µm thick) were mounted in 100% glycerol for fluorescence microscopy and visualization of tetracycline and demeclocycline labels. Based on the length and distance between double tetracycline/demeclocycline labels, dynamic bone parameters, including bone formation rate and mineral apposition rate, were measured.
4.10. Identification of Vascular Sclerostin mRNA
Total mRNA was extracted from the distal part of the abdominal aorta using the RNeasy Fibrous Tissue Mini Kit (Qiagen, Hilden, Germany) and complementary DNA was generated with the High-Capacity cDNA Archive Kit (Applied Biosystems, Foster City, CA, USA). Real-time PCR amplification was performed based on the TaqMan fluorescence methodology (ABI Prism® 7000 Sequence Detection System, Applied Biosystems). TaqMan probes and primers for glyceraldehyde 3-phosphate dehydrogenase (GAPDH) (Rn99999916_s1) and sclerostin (SOST) (Rn00577971_m1) were purchased from Applied Biosystems as a Taqman® gene expression assay on demand. For each sample, the expression of the tested transcripts was analyzed in triplicate and normalized to the expression of GAPDH, the housekeeping gene. The comparative CT method, using aortas of control rats as calibrator samples, was used to calculate the gene expression levels.
4.11. Immunohistochemical Sclerostin/LRP4 Staining on Rat and Human Arterial Sections
Immunohistochemical staining was performed on neutral buffered formalin-fixed, deparaffinized arterial sections of warfarin-exposed and control rats sacrificed at week 10, as well as on calcified human arterial sections. The excised tissue sections were blocked with normal goat serum (20% in PBS) for 20 min and incubated overnight with polyclonal rabbit antisclerostin (1:500, ab-63097, Abcam, Cambridge, UK) or LRP4 (1:75, sc-98775, Santa Cruz, TX, USA). Biotinylated goat anti-rabbit (Vector Laboratories, Burlingame, CA, USA) was used as a secondary antibody. Avidin/biotinylated peroxidase complex (VECTASTAIN ABC kit, Vector Laboratories) was added as a signal amplifier and 3-amino-9-ethylcarbazole (AEC, Sigma-Aldrich, St. Louis, MO, USA) was used as a substrate. The sections were counterstained with hematoxylin. Sections in which the primary antibody was omitted were used as negative controls.
4.12. Immunohistochemical Staining on Rat Bone Sections
Sclerostin expression was also investigated on tibia sections in order to compare the absolute sclerostin expression per bone area as the percentage of sclerostin-positive osteocytes (lacunae) between control and warfarin-exposed rats. After deacrylation and decalcification of the tibia sections, the same protocol for immunohistochemistry on the arterial sections was used as described above. The antisclerostin primary antibody (ab-63097, Abcam) was used in a 1:750 concentration.
4.13. Evaluation of Serum Sclerostin Levels
The sclerostin concentration in the serum was determined using an antisclerostin ELISA kit (Quantikine® Elisa, R&D Systems, Minneapolis, MN, USA), following the appropriate procedures.
4.14. Statistical Analysis
All statistical analyses were performed using PRISM software (GraphPad Prism 6.0, San Diego, CA, USA). Data are presented as the mean ± standard error of mean (SEM). Statistical differences between groups were investigated by a two-tailed Mann–Whitney U test. Bonferroni correction was applied when appropriate. p-Values < 0.05 were considered statistically significant.

 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}