
Automated Coronary Optical Coherence Tomography Feature Extraction with Application to Three-Dimensional Reconstruction

 ,
,
Abstract
:1. Introduction
2. Coronary Lumen
3. Artery Layers
4. Plaque Characteristics and Subtypes
5. Stents
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Glossary of Performance Metrics
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author [Ref] | Aim | Dataset | Morphological/Filtering Operations | Feature Detection/Classification | Outcome | Comparison * |
|---|---|---|---|---|---|---|
| Akbar et al. [65] | Automated lumen extraction and 3D FFR modelling | 5931 images (40 patients) | Polar transform, Bilateral smoothing filter, dilation, erosion | L- & C-mode interpolation and Sobel edge detection | R: 0.99 FFR R: 0.98 | Manual segmentation and individual L- and C-mode interpolation |
| Athanasiou et al. [91] | Lumen detection through optimized segmentation and 3D WSS modelling | 11 patients, 613 annotated images | Polar transform, Bilateral smoothing filter | B-spline curve fit, K-means | 3D HD: 0.05 mm (±0.19) R: 0.98 R2: 0.96 WSS R2: 0.95 | Expert annotation and WSS results between expert annotated reconstruction |
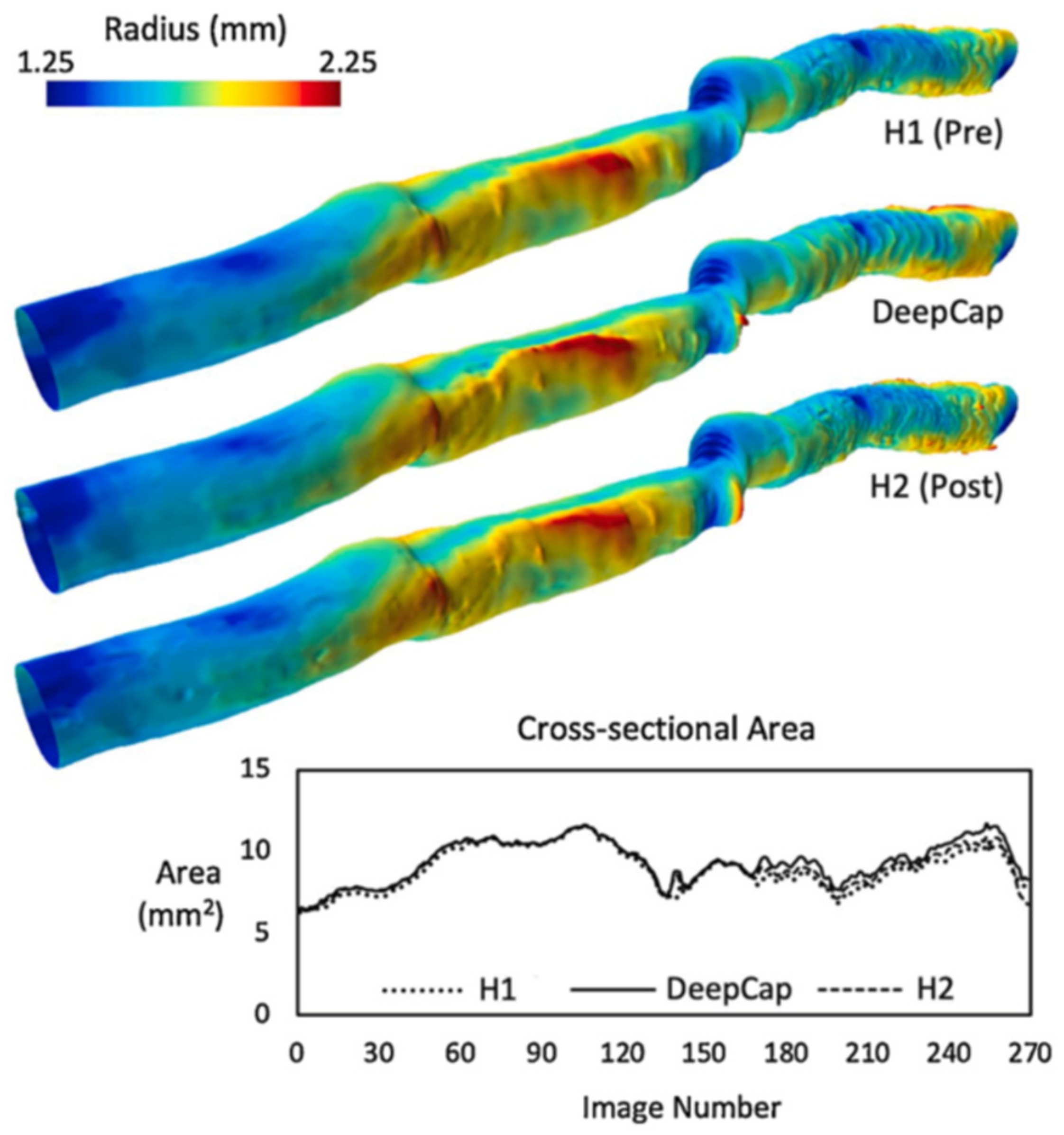
| Balaji et al. [93] | Efficient and low memory automated lumen segmentation for clinical application | 12,011 images (22 patients) | Gaussian derivative | PyTorch based deep capsules with ADAM optimizer | DICE: 0.97 ± 0.06 HD: 3.30 ±1.51 µm SEN: 93.00 ± 8.00% SPE: 99.00 ± 1.00% | Expert annotation, UNet-ResNet18, FCNResNet50 and DeepLabV3-ResNet50 |
| Cao et al. [74] | Automated lumen segmentation in challenging geometries | 880 images (five patients) | Polar transform, Narrow image smoothing filter (Gaussian) | Distance regularized level set | DICE: 0.98 ± 0.01 | Manual segmentation |
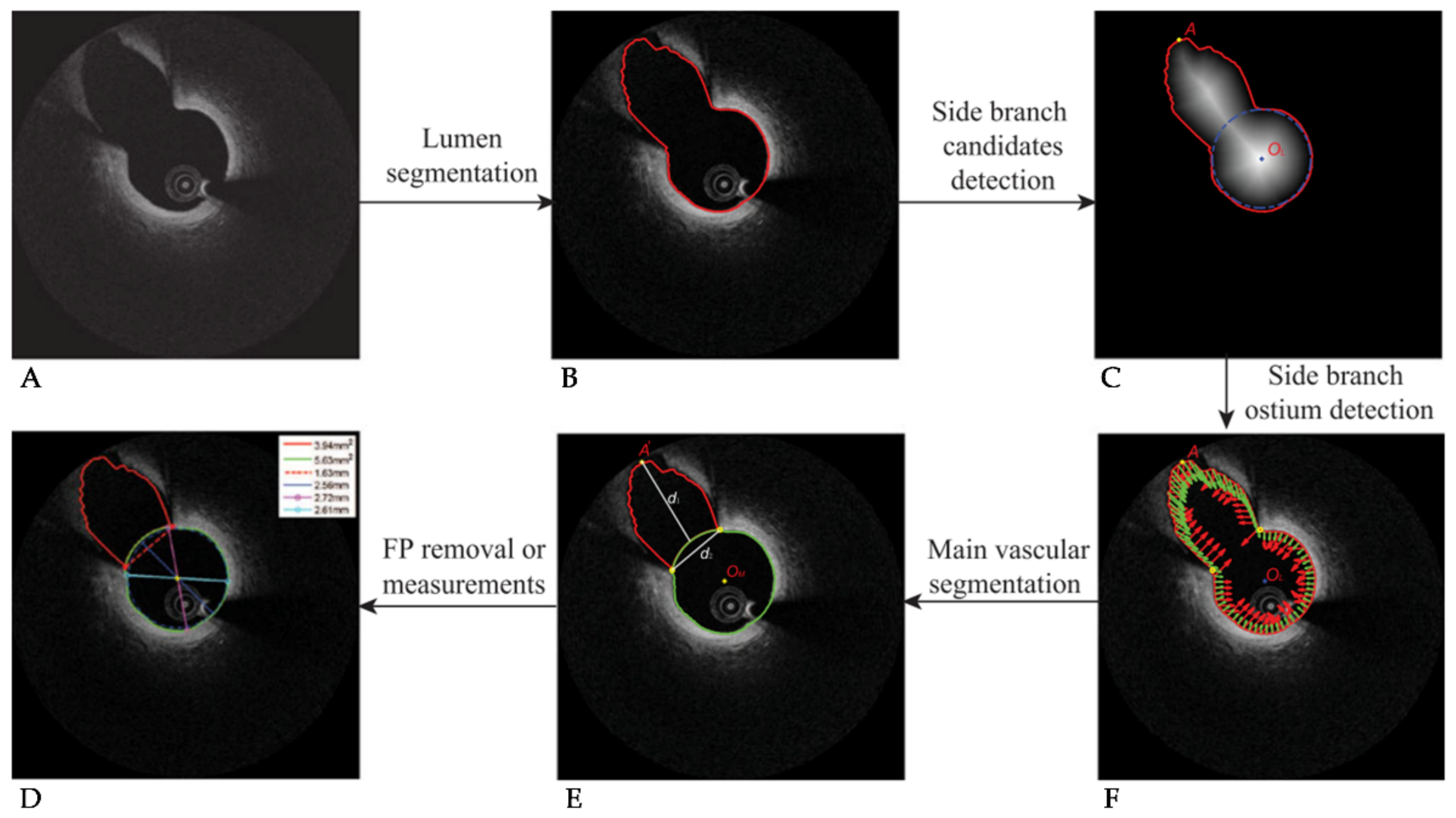
| Cao et al. [76] | Automatic side branch ostium and lumen detection | 4618 images (22 pullbacks) | Dynamic programming distance transform, differential filter | MV DICE: 0.96 BR DICE: 0.78 TPR: 0.83 TNR: 0.99 PPV: 87.00% NPV: 98.00% | Manual segmentation | |
| Cheimariotis et al. [63] | Automated lumen segmentation in all image types (bifurcation, blood artefacts) | 1812 images (20 patients, 308 stented, 1504 native) | Polar transform, Median filtering, Gaussian filtering, opening, Otsu binarization, low-pass filtering | Gradient window enhancement | Stented: DICE: 0.94 R2: 0.97 Non-stented: DICE: 0.93 R: 0.99 R2: 0.92 | Expert annotation (area, perimeter, radius, diameter, centroid) |
| Essa at al. [70] | Automatic lumen detection in OCT (and tissue characterization in IVUS) | 2303 images (13 pullbacks: Column-wise labelling 457, training 457, testing 1389) | Polar transform, A-line based dynamic tissue classification | Kalman filter based spatio-temporal segmentation method, RF | ACC: 96.27% HD: 11.01 ± 11.93 µm JS: 0.95 ± 0.03 SEN: 95.55 ± 3.19% SPE: 99.84 ± 0.29% | Expert annotation |
| Joseph et al. [68] | Automated lumen contours using local transmittance-based enhancement | 8100 images (30 pullbacks, 270 images per pullback) | Polar transform, transmissivity-based mapping | Region-based level set active contour method | BR DICE: 0.78 ± 0.20 | Expert annotation |
| Macedo et al. [62] | Automated lumen segmentation by morphological operations in plaque and bifurcation regions. | 1328 images (nine pullbacks, 141 BR, 1188 NBR) | Polar transform, Bilateral filtering, Otsu thresholding, Erosion/dilation | Sobel edge detection, Distance transform based automatic contour correction | NBR MADA: 0.19 ± 0.13 mm2 NBR DICE: 0.97 ± 0.02 BR MADA: 0.52 ± 0.81 mm2 BR DICE: 0.91 ± 0.09 | Manual segmentation |
| Miyagawa et al. [77] | Automated detection and outline of bifurcation regions | 2460 images (Nine patients, 157 BR, 1204 NBR, 1099 DA) | Global thresholding, closing, Hough transform | Four CNNs, three with transfer learning from lumen detection | ACC: 98.00 ± 1.00% SPE: 98.00 ± 1.00% AUC: 0.99 ± 0.00 | Expert annotation |
| Pociask et al. [66] | Automated lumen segmentation | 667 images | Polar transform, Gaussian & Savitzky–Golay filtering, opening/closing | Linear interpolation | Relative difference in lumen area: 1.12% (1.55–0.68%) | Manual segmentation |
| Roy et al. [69] | Random walks automatic segmentation of the lumen | Patients: six in vivo, 15 in vitro. 150–300 frames per patient | Polar transform, | Random walks based on edge weights and backscattering tracking | CK: 0.98 ± 0.01 KL: 5.17 ± 2.39 BHAT: 0.56 ± 0.28 | Expert annotation |
| Tang et al. [87] | Automated lumen extraction using N-Net CNN | 20,000 images (400 for training from manual annotation) | N-Net CNN with cross entropy loss function | ACC: 98.00 ± 0.00% DICE: 0.93 ± 0.00 JS: 0.88 ± 0.00 SPE: 99.00 ± 0.00% | Expert annotation of 400 images | |
| Yang et al. [84] | Automated lumen extraction in abnormal lumen geometries | 14,207 images (54 patients) | Polar transform, Gaussian filtering | Active contour model, Gray-level co-occurrence matrix, SVM, AdaBoost, J48, RF, NB, Bagging | DICE: 0.98 ± 0.01 JS: 0.95 ± 0.02 MADA: 0.27 ± 0.19 mm2 ASSD: 0.03 ± 0.01 mm RMSD: 0.04 ± 0.01 mm ACC: 99.00 ± 1.00% | Expert annotation on 1541 images |
| Yong et al. [85] | Automated lumen extraction using linear regression CNN | 19,027 images (64 pullbacks, 28 patients) | Polar transform, | Linear regression CNN | Location accuracy: 22 µm DICE 0.99 JS: 0.97 | Expert annotation on 19 pullbacks (5685 images) |
| Zhao et al. [61] | Automated lumen extraction using morphological operations | 268 images | Polar transform, Median filtering, Otsu binarization, closing/opening | DICE: 0.99 JS: 0.99 ACC: 99.00% HD: 0.01 mm | Expert annotation | |
| Zhu et al. [59] | Automated lumen segmentation to overcome blood artefacts | 216 images with blood artefacts (from 1436 images, 6 patients) | Polar transform, Gaussian filtering, adaptive block binarization, erosion/area opening | Connected A-line region filtering with bicubic interpolation and quadratic regression smoothing | DICE: 0.95 JS: 0.90 ACC: 98.00% | Morphological only, dynamic programming, manual segmentation |
| First Author [Ref] | Aim | Dataset | Morphological Operations | Feature Detection/Classification | Outcome | Comparison |
|---|---|---|---|---|---|---|
| Abdolmanafi et al. [101] | Automated intima and media classification in pediatric patients | 4800 regions of interest (26 patients) | CNN (AlexNet), RF, SVM | CNN ACC: 97.00 ± 4.00% RF ACC: 96.00 ± 6.00% SVM ACC: 90.00 ± 10.00% | Manual segmentation | |
| Chen et al. [102] | Automated wall morphology change analyses in heart transplant patients | 43,873 images (100 pullbacks, 50 patients) | Caffe framework, LOGISMOS, Sobel edge detector | R2: 0.96 Intima error: 4.98 ± 31.24 µm Media error: 5.38 ± 28.54 µm | Expert annotation | |
| Haft-Javaherian et al. [110] | Automated lumen, intima and media classification in polarization-sensitive OCT | 984 images (57 patients) | CNN based on U-Net and deep residual learning model, combination of five loss functions | DICE *: 0.99 ACC *: 99.30% SEN *: 99.50% SPE *: 99.00% | Expert annotation and traditional OCT. | |
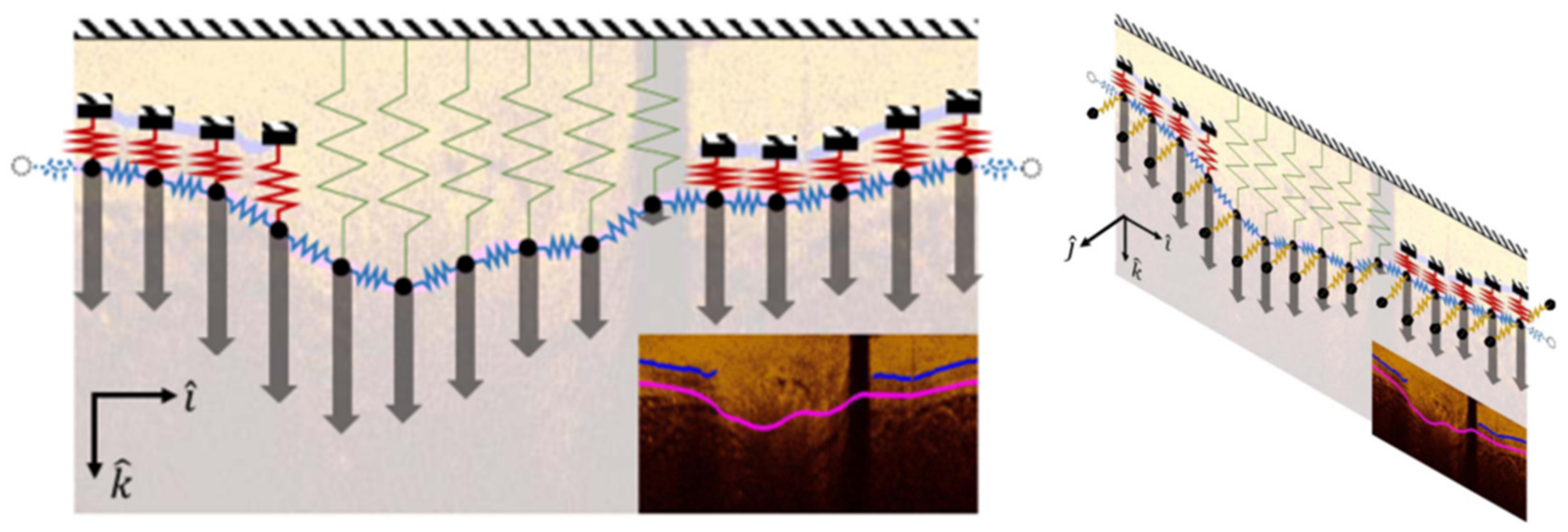
| Olender et al. [113] | Automated delineation of outer elastic membrane using mechanical approach | 724 images (seven patients) | Contrast enhancement, image compensation, median filtering | Sobel-Feldman edge detection, anisotropic linear elastic mesh force balance | MADA: 0.93 mm2 (±0.84) DICE: 0.91 JS: 0.84 SEN: 90.79% SPE: 99.00% | Expert annotation and IVUS |
| Pazdernik et al. [103] | Automated wall morphology change analyses in heart transplant patients | 50 patients (~25,000 co-registered images) | LOGISMOS | R2: 0.99 Intima error: 0.4 ± 27.1 µm Media error: 8.1 ± 12.2 µm | Expert annotation | |
| Zahnd et al. [100] | Automatically segment three layers of healthy coronary artery wall | 40 patients (400 classified images, 140 training, 260 validation) | Erosion, dilation | AdaBoost, front propagation scheme with cumulative cost function, Boruta algorithm (RF based) | DICE: 0.93 ACC: 91.00% SEN: 92.00% SPE: 100.00% IMe: 29 ± 46 µm MAe: 30 ± 50 µm APe: 50 ± 64 µm | Expert annotation |
| First Author [Ref] | Aim | Dataset | Morphological Operations | Feature Detection/Classification | Outcome | Comparison |
|---|---|---|---|---|---|---|
| Abdolmanafi et al. [132] | Tissue characterization in Kawasaki disease | 8910 images (33 pullbacks) | Polar transform | RF (AlexNet, VGG-19 & Inception-V3) & majority voting | ACC ^^: 99.00 ± 1.00% SEN: 98.00 ± 2.00% SPE: 100.00 ± 0.00% | Expert annotation |
| Abdolmanafi et al. [133] | Tissue characterization in Kawasaki disease | 5040 images (45 pullbacks) | Polar transform | FCN, RF (VGG-19) | ACC ^^: 96.00 ± 4.00% SPE: 95.00 ± 5.00% SEN: 97.00 ± 3.00% F1: 0.96 ± 0.04 | Expert annotation |
| Abdolmanafi et al. [134] | Automatic plaque tissue classification | 41 pullbacks (~200 images per pullback) | FCN (ResNet), ADAM optimizer | ACC: 93.00 ± 10.00% SEN: 90.00 13.00% SPE: 95.00 ± 5.00% F1: 0.84 ± 0.18 | Manual segmentation | |
| Avital et al. [168] | Deep learning-based calcification classification | 8000 images (540 frames for training) | U-Net | ACC: 99.03 ± 9.00% DICE: 0.71 ± 0.26 | Manual segmentation | |
| Cheimariotis et al. [161] | Four-way plaque type classification | 183 images (33 patients) | Polar transform, Median filtering, Gaussian filtering, opening, Otsu binarization, low-pass filtering (ARC-OCT) | CNN (AlexNet), ADAM optimizer with attenuation coefficient | A-line transformed ACC: 83.47% Plaque: ACC: 74.73% SEN: 87.78% SPE: 61.45% | Manual segmentation |
| Gerbaud et al. [151] | Plaque burden measurement with enhancement algorithm | 42 patients (96 pullbacks) 200 IVUS-OCT matched images | Adaptive attenuation compensation, frame averaging | Mean difference. EEL: 0.27 ± 3.31 mm2 PB: −0.5 ± 7.0% | Expert annotation and IVUS | |
| Gessert et al. [130] | Plaque detection and segmentation with multi-path architecture | 4000 images (49 patients) | Polar & cartesian | CNN (ResNet50-V2 & DenseNet-121) | ACC: 91.70% SEN: 90.90% SPE: 92.40% F1: 0.91 | Expert annotation |
| Gharaibeh et al. [170] | Classification and segmentation of lumen and calcification | 2640 images (34 pullbacks) | Polar transform, log-transform, Gaussian filtering | CNN (SegNet) & CRF | Calcific: DICE: 0.76 ± 0.03 SEN: 85.00 ± 4.00% Lumen: DICE: 0.98 ± 0.01 SEN: 99.00 ± 1.00% | Manual segmentation |
| He et al. [167] | Automatic classification of calcification | 4860 images (18 pullbacks) | Polar transform | CNN (ResNet-3D & 2D), cross-entropy loss, ADAM optimizer | PRE: 96.90 ± 1.30% REC: 97.70 ± 3.40% F1: 96.10 ± 3.40% | Manual segmentation |
| Huang et al. [136] | Fibrous, calcific and lipidic tissue classification | 28 images (11 patients] | Polar transform, Otsu thresholding, | SVM (RF feature selection) | ACC: 83.00% Fibrous ACC: 89.00% Lipidic ACC: 86.50% Calcific ACC: 79.30% | Manual segmentation |
| Isidori et al. [152] | Automated lipid core burden index assessment | Training: 23 patients. Testing: 40 patients, | CNN | SEN: 90.50% SPE: 84.20% | Expert annotation and NIRS-IVUS | |
| Kolluru et al. [155] | CNN classification of plaque types (fibro-calcific and fibro-lipidic) | 4469 images (48 pullbacks) | Log transform, Gaussian filtering | CNN and ANN | ACC: 77.7% ± 4.1% for fibro-calcific, 86.5% ± 2.3% for fibro-lipid and 85.3% ± 2.5% for others | Expert annotation and ANN |
| Kolluru et al. [172] | Reduce number of training images needed for deep learning | 3741 images (60 VOIs from 41 pullbacks) | Log transform, Gaussian filtering | U-Net, Image subset selection through deep-feature clustering and k-medoids algorithm | Clustering outperforms equal spacing methods for sparse annotations (F1: 0.63 vs. 0.52, AP: 66% vs. 50%) | Expert annotation |
| Lee et al. [156] | Hybrid learning approach to classify fibro-lipidic and fibro-calcific tissue | 6556 images | Polar transform, Gaussian filtering | CNN (ADAM optimizer) & RF with hybrid learning approach, CRF & dynamic programming | Fibro-lipidic: SEN: 84.80 ± 8.20% SPE: 97.80 ± 1.60% F1: 0.89 ± 0.04 Fibro-calcific: SEN: 91.20 ± 6.40% SPE: 96.20 ± 1.60% F1: 0.72 ± 0.07 | Manual segmentation, pre & post noise cleaning and active learning |
| Lee et al. [157] | Automatic lipid/calcium characterization comparison | 4892 images (57 pullbacks, 55 patients) | Polar transform, non-local mean filtering | CNN (SegNet VGG16), Deeplab 3+, dynamic programming | Manual segmentation, pixel-wise vs. A-line | |
| Lee et al. [169] | Fully automated 3D calcium segmentation and reconstruction | 8231 images (68 patients) 4320 ex vivo images (four cadavers) | Polar transform, Gaussian filtering, opening & closing | 3D CNN & SegNet with Tversky loss function, CRF & dynamic programming | SEN: 97.70% SPE: 87.70% F1: 0.92 | Manual segmentation, one-step approach |
| Li et al. [135] | Segmentation of vulnerable plaque regions | 2000 images (50% vulnerable plaque) | Polar transform | Deep Residual U-Net (ResNet101) & combined cross-entropy and dice loss | ACC: 93.31% MIoU: 0.85 FIoU: 0.86 PRE: 94.33% REC: 91.35% | Manual segmentation, prototype U-Net; VGG16, ResNet50, ResNet101 |
| Liu et al. [144] | Automated fibrous plaque detection | 1000 images | Polar & Hough transform | CNN (VGG16) | ACC ^: 94.12% REC: 94.12% | Expert annotation, SSD, YOLO-V3 |
| Liu et al. [150] | Vulnerable plaque detection | 2000 training images, 300 testing images, data augmentation | Polar transform, erosion/dilation, de-noising | Deep CNN (Adaboost, YOLO, SSD, Faster R-CNN) | PRE: 88.84% REC: 95.02% | Manual segmentation |
| Liu et al. [162] | Classification of six tissue types: mixed, calcification, fibrous, lipid-rich, macrophages, necrotic core | 135 images (ex vivo) | Polar transform, median filtering | Attenuation, backscatter, intensity | Attenuation and backscatter can differentiate six tissue types | Expert annotation & histology |
| Prabhu et al. [115] | Detection of fibro-lipidic and fibro-calcific A-lines | 6556 in vivo images (49 pullbacks), 440 ex vivo images (10 pullbacks) | Polar transform, texture features from Leung–Malik filter bank | RF, SVM, DB, mRMR, binary Wilcoxon & CRF | ACC: 81.58% Fibro-lipidic: SEN: 94.48% SPE: 87.32% Fibro-calcific: SEN: 74.82% SPE: 95.28% | Expert annotation |
| Rico-Jimenez et al. [129] | Automated tissue characterization with A-line features | 513 images | Polar transform, entropy & frost filter | Linear Discriminant Analysis | ACC: 88.20% | Manual segmentation |
| Rico-Jimenez et al. [153] | Macrophage infiltration detection | 28 ex vivo coronary segments | Normalized-intensity standard deviation ratio | ACC: 87.45% SEN: 85.57% SPE: 88.03% | Manual segmentation and histological evaluation | |
| Shibutani et al. [154] | Automated plaque characterization in ex vivo sections | 1103 histological cross sections (45 autopsied hearts) | CNN (ResNet50), scene parsing network (PSPNet) | FC AUC: 0.91 PIT AUC: 0.85 TCFA AUC: 0.86 HER AUC: 0.86 | Expert annotation and histological evaluation | |
| Wang et al. [128] | Fibrotic plaque area segmentation | 20 images (nine patients) | Adaptive diffusivity | Log-likelihood function of Gaussian mixture model (GMM) | MCR **: 0.65 ± 0.66 PRI: 0.99 ± 0.01 | Manual segmentation, GMM, FCM, SMM, FRSCGMM, AFPDEFCM, GMM-SMSI |
| Yang et al. [127] | Automatic classification of plaque (fibrous, calcific and lipid-rich) | 1700 images (20 pullbacks, nine patients) | Mean filtering, graph-cut method | SVM (C-SVC) with HEM training, K-means, radial basis function | ACC: 96.80 ± 0.02% | Manual segmentation |
| Zhang et al. [120] | Automated fibrous cap thickness quantification and plaque classification | 18 images (two patients, 1008 images after DA) | CNN (U-Net), CNN (FC-DenseNet), SVM | U-Net ACC *: 95.40% FC-DenseNet ACC: 91.14% SVM ACC: 81.84% | Manual segmentation guided by VH-IVUS | |
| Zhang et al. [126] | Comparison of automated lipid, fibrous and background tissue segmentation | 77 images (five patients) | CNN (U-Net based architecture) and SVM Focal loss function, local binary patterns, gray level co-occurrence matrices | CNN ACC *: 94.29% SVM ACC: 69.46% | Manual segmentation guided by VH-IVUS |
| First Author [Ref] | Aim | Dataset | Morphological Operations | Feature Detection/Classification | Outcome | Comparison |
|---|---|---|---|---|---|---|
| Bologna et al. [64] | Automated lumen contour and stent strut selection for 3D reconstruction | 1150 images (23 pullbacks) | Thresholding, opening, closing, nonlinear filtering | Sobel edge detection | Lumen: SPE: 97.00% SEN: 99.00% Stent: SPE: 63.00% SEN: 83.00% | Manual segmentation |
| Cao et al. [176] | Automatic stent segmentation and malapposition evaluation | 4065 images (12,550 struts, 15 pullbacks) | Cascade AdaBoost classifier, dynamic programming | DICE: 0.81 TPR: 90.50% FPR: 12.10% F1: 0.90 | Expert annotation | |
| Chiastra et al. [187] | Stent strut and lumen contour detection through OCT and micro-CT | Eight stented bifurcation phantom arteries (in vitro), four in vivo patients | Polar transform, opening, thresholding | Sobel edge detection | Stent *: DICE: 0.93 ± 0.06 JS: 0.87 ± 0.10 SPE: 94.75 ± 7.60% SEN: 90.87 ± 9.44% | Manual segmentation |
| Elliot et al. [190] | Automated 3D stent reconstruction through OCT and micro-CT | 2156 images, four stented phantom arteries (in vitro) | Polar transform | A-line intensity profile, peak intensity, number of peaks | ASSD: 184 ± 96 µm | Manual segmentation |
| Jiang et al. [178] | Automatic segmentation of metallic stent struts | 165 images, 1200 post DA on (10 pullbacks) | YOLOv3 (binary cross-entropy loss) and region-based fully-convolutional network (R-FCN), Darknet53 | YOLOv3 vs. R-FCN PRE: 97.20% vs. 99.80% REC: 96.50% vs. 96.20% AP: 96.00% vs. 96.20% | Manual segmentation and between two classifiers | |
| Junedh et al. [179] | Automation of polymeric stent strut segmentation | 1140 images (15 patients) | Polar transform, bilateral filter | K-means | R2: 0.88 PPV: 93.00% TPR: 90.00% | Expert annotation |
| Lau et al. [180] | Segmentation of metallic and bioresorbable vascular scaffolds | 51 pullbacks (27 patients), 13,890 training images, 3909 test images | U-Net with combined MobileNetV2 and DenseNet121 | DICE *: 0.86 PRE *: 92.00% REC *: 92.00% | Manual segmentation | |
| Lu et al. [182] | Automatic classification of covered/uncovered stents | 7125 images (39,000 covered struts, 16,500 uncovered struts, 80 pullbacks) | Polar transform | SVM (LIBSVM), bagged decision trees classifier, pixel patch method, mesh growing, active learning relabeling | SPE: 94.00 ± 3.00% SEN: 90.00 ± 4.00% AUC: 0.97 | Expert annotation |
| Lu et al. [184] | Development of automated OCT image visualization and analysis toolkit for stents (OCTivat-stent) | (292 pullbacks) | Polar transform | SVM (LIBSVM), bagged decision trees classifier, pixel patch method, mesh growing, active learning relabeling | Lumen CCC: 0.99 Stent CCC: 0.97 | Expert annotation |
| Migliori et al. [189] | Framework for automated stent segmentation and lumen reconstruction for CFD simulation | 540 images, 0ne phantom (in vitro) | Polar transform, intensity/area thresholding | Fuzzy logic, Sobel edge detection and linear interpolation | Stent *: DICE: 0.87 ± 0.13 JS: 0.78 ± 0.18% SPE: 77.8 ± 28.20% SEN: 91.7 ± 13.20% | Manual segmentation of 95 images |
| Nam et al. [174] | Automatic stent apposition and neointimal coverage analysis | 5420 images (20 pullbacks) | Polar transform, Gaussian smoothing | ANN, image gradient and intensity | PPV: 95.60% TPR: 92.90% | Manual segmentation on 800 images |
| O’Brien et al. [186] | Enhanced stent and lumen 3D reconstruction for CFD simulation | Four swine pullbacks | Decision tree, ramp edge detection | Lumen (62 frames) MADA: 0.42 ± 0.13 mm2 Stent (57 frames) MADA: 0.20 ± 0.17 mm2 | Manual segmentation | |
| Wu et al. [175] | Automated stent strut detection in multiple stent designs | Training: 10,417 images (60 pullbacks) Testing: 21,363 images (170 pullbacks) | Polar transform, Manual training mask | U-Net based deep convolutional model (ADAM optimizer, binary cross-entropy and Tversky loss functions) | DICE: 0.91 ± 0.04 JS: 0.84 ± 0.06 PRE: 94.30 ± 3.60% REC: 94.00 ± 3.90% F1: 0.94 ± 0.04 | Expert annotation and QIvus v3.1 (Medis Medical Imaging System BV, Leiden, The Netherlands) |
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N. Heart disease and stroke statistics—2021 update: A report from the American Heart Association. Circulation 2021, 143, 254–743. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, A.; Griffiths, U.; Murphy, A.; Legido-Quigley, H.; Lamptey, P.; Perel, P. The economic burden of cardiovascular disease and hypertension in low-and middle-income countries: A systematic review. BMC Public Health 2018, 18, 975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jernberg, T.; Hasvold, P.; Henriksson, M.; Hjelm, H.; Thuresson, M.; Janzon, M. Cardiovascular risk in post-myocardial infarction patients: Nationwide real world data demonstrate the importance of a long-term perspective. Eur. Heart J. 2015, 36, 1163–1170. [Google Scholar] [CrossRef] [Green Version]
- Baumann, A.A.W.; Mishra, A.; Worthley, M.I.; Nelson, A.J.; Psaltis, P.J. Management of multivessel coronary artery disease in patients with non-ST-elevation myocardial infarction: A complex path to precision medicine. Ther. Adv. Chronic Dis. 2020, 11, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Kim, W.Y.; Danias, P.G.; Stuber, M.; Flamm, S.D.; Plein, S.; Nagel, E.; Langerak, S.E.; Weber, O.M.; Pedersen, E.M.; Schmidt, M. Coronary magnetic resonance angiography for the detection of coronary stenoses. N. Engl. J. Med. 2001, 345, 1863–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narula, J.; Nakano, M.; Virmani, R.; Kolodgie, F.D.; Petersen, R.; Newcomb, R.; Malik, S.; Fuster, V.; Finn, A.V. Histopathologic characteristics of atherosclerotic coronary disease and implications of the findings for the invasive and noninvasive detection of vulnerable plaques. J. Am. Coll. Cardiol. 2013, 61, 1041–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Z.; Tian, J.; Ma, L.; Du, H.; Dong, N.; Hou, J.; He, J.; Dai, J.; Liu, X.; Pan, H.; et al. Comparison of optical coherence tomography and intravascular ultrasound for evaluation of coronary lipid-rich atherosclerotic plaque progression and regression. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1374–1380. [Google Scholar] [CrossRef] [Green Version]
- Tearney, G.J.; Waxman, S.; Shishkov, M.; Vakoc, B.J.; Suter, M.J.; Freilich, M.I.; Desjardins, A.E.; Oh, W.-Y.; Bartlett, L.A.; Rosenberg, M. Three-dimensional coronary artery microscopy by intracoronary optical frequency domain imaging. JACC Cardiovasc. Imaging 2008, 1, 752–761. [Google Scholar] [CrossRef] [Green Version]
- Prati, F.; Romagnoli, E.; Gatto, L.; La Manna, A.; Burzotta, F.; Ozaki, Y.; Marco, V.; Boi, A.; Fineschi, M.; Fabbiocchi, F.; et al. Relationship between coronary plaque morphology of the left anterior descending artery and 12 months clinical outcome: The CLIMA study. Eur. Heart J. 2019, 41, 383–391. [Google Scholar] [CrossRef]
- Montarello, N.J.; Nelson, A.J.; Verjans, J.; Nicholls, S.J.; Psaltis, P.J. The role of intracoronary imaging in translational research. Cardiovasc. Diagn. Ther. 2020, 10, 1480–1507. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, H.J.; Gholipour, A.; Ghayesh, M.H.; Zander, A.C.; Psaltis, P.J. A review on the biomechanics of coronary arteries. Int. J. Eng. Sci. 2020, 147, 1–62. [Google Scholar] [CrossRef]
- Shishikura, D.; Sidharta, S.L.; Honda, S.; Takata, K.; Kim, S.W.; Andrews, J.; Montarello, N.; Delacroix, S.; Baillie, T.; Worthley, M.I.; et al. The relationship between segmental wall shear stress and lipid core plaque derived from near-infrared spectroscopy. Atherosclerosis 2018, 275, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Giannoglou, G.D.; Soulis, J.V.; Farmakis, T.M.; Farmakis, D.M.; Louridas, G.E. Haemodynamic factors and the important role of local low static pressure in coronary wall thickening. Int. J. Cardiol. 2002, 86, 27–40. [Google Scholar] [CrossRef]
- Bourantas Christos, V.; Räber, L.; Sakellarios, A.; Ueki, Y.; Zanchin, T.; Koskinas Konstantinos, C.; Yamaji, K.; Taniwaki, M.; Heg, D.; Radu Maria, D.; et al. Utility of multimodality intravascular imaging and the local hemodynamic forces to predict atherosclerotic disease progression. JACC Cardiovasc. Imaging 2020, 13, 1021–1032. [Google Scholar] [CrossRef]
- Soulis, J.V.; Fytanidis, D.K.; Papaioannou, V.C.; Giannoglou, G.D. Wall shear stress on LDL accumulation in human RCAs. Med. Eng. Phys. 2010, 32, 867–877. [Google Scholar] [CrossRef]
- Bourantas Christos, V.; Zanchin, T.; Torii, R.; Serruys Patrick, W.; Karagiannis, A.; Ramasamy, A.; Safi, H.; Coskun Ahmet, U.; Koning, G.; Onuma, Y.; et al. Shear stress estimated by quantitative coronary angiography predicts plaques prone to progress and cause events. JACC Cardiovasc. Imaging 2020, 13, 2206–2219. [Google Scholar] [CrossRef]
- Stone, P.H.; Maehara, A.; Coskun, A.U.; Maynard, C.C.; Zaromytidou, M.; Siasos, G.; Andreou, I.; Fotiadis, D.; Stefanou, K.; Papafaklis, M.; et al. Role of low endothelial shear stress and plaque characteristics in the prediction of nonculprit major adverse cardiac events: The PROSPECT study. JACC Cardiovasc. Imaging 2018, 11, 462–471. [Google Scholar] [CrossRef]
- Gholipour, A.; Ghayesh, M.H.; Zander, A.; Mahajan, R. Three-dimensional biomechanics of coronary arteries. Int. J. Eng. Sci. 2018, 130, 93–114. [Google Scholar] [CrossRef]
- Pei, X.; Wu, B.; Li, Z.-Y. Fatigue crack propagation analysis of plaque rupture. J. Biomech. Eng. 2013, 135, 1–9. [Google Scholar] [CrossRef]
- Cardoso, L.; Weinbaum, S. Changing views of the biomechanics of vulnerable plaque rupture: A review. Ann. Biomed. Eng. 2014, 42, 415–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Wu, Z.; Yang, C.; Zheng, J.; Bach, R.; Muccigrosso, D.; Billiar, K.; Maehara, A.; Mintz, G.S.; Tang, D. IVUS-based FSI models for human coronary plaque progression study: Components, correlation and predictive analysis. Ann. Biomed. Eng. 2015, 43, 107–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, H.; Gholipour, A.; Ghayesh, M.; Zander, A.C.; Psaltis, P. In vivo based fluid-structure interaction biomechanics of the left anterior descending coronary artery. J. Biomech. Eng. 2021, 143, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Tang, D.; Wang, L.; Meahara, A.; Molony, D.; Samady, H.; Zheng, J.; Mintz, G.S.; Stone, G.W.; Giddens, D.P. Multi-patient study for coronary vulnerable plaque model comparisons: 2D/3D and fluid–structure interaction simulations. Biomech. Model. Mechanobiol. 2021, 20, 1383–1397. [Google Scholar] [CrossRef]
- Tang, D.; Yang, C.; Kobayashi, S.; Zheng, J.; Woodard, P.K.; Teng, Z.; Billiar, K.; Bach, R.; Ku, D.N. 3D MRI-based anisotropic FSI models with cyclic bending for human coronary atherosclerotic plaque mechanical analysis. J. Biomech. Eng. 2009, 131, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Costopoulos, C.; Brown, A.J.; Teng, Z.; Hoole, S.P.; West, N.E.J.; Samady, H.; Bennett, M.R. Intravascular ultrasound and optical coherence tomography imaging of coronary atherosclerosis. Int. J. Cardiovasc. Imaging 2016, 32, 189–200. [Google Scholar] [CrossRef]
- Fujimoto, J.G. Optical coherence tomography for ultrahigh resolution in vivo imaging. Nat. Biotechnol. 2003, 21, 1361–1367. [Google Scholar] [CrossRef]
- Bezerra Hiram, G.; Costa Marco, A.; Guagliumi, G.; Rollins Andrew, M.; Simon Daniel, I. Intracoronary optical coherence tomography: A comprehensive review. JACC Cardiovasc. Interv. 2009, 2, 1035–1046. [Google Scholar] [CrossRef] [Green Version]
- Prati, F.; Regar, E.; Mintz, G.S.; Arbustini, E.; Di Mario, C.; Jang, I.-K.; Akasaka, T.; Costa, M.; Guagliumi, G.; Grube, E. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: Physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis. Eur. Heart J. 2010, 31, 401–415. [Google Scholar] [CrossRef]
- Jang, I.-K.; Bouma, B.E.; Kang, D.-H.; Park, S.-J.; Park, S.-W.; Seung, K.-B.; Choi, K.-B.; Shishkov, M.; Schlendorf, K.; Pomerantsev, E. Visualization of coronary atherosclerotic plaques in patients using optical coherence tomography: Comparison with intravascular ultrasound. J. Am. Coll. Cardiol. 2002, 39, 604–609. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-J.; Lee, H.; Kato, K.; Yonetsu, T.; Xing, L.; Zhang, S.; Jang, I.-K. Reproducibility of in vivo measurements for fibrous cap thickness and lipid arc by OCT. JACC Cardiovasc. Imaging 2012, 5, 1072–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koskinas, K.C.; Ughi, G.J.; Windecker, S.; Tearney, G.J.; Räber, L. Intracoronary imaging of coronary atherosclerosis: Validation for diagnosis, prognosis and treatment. Eur. Heart J. 2016, 37, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, A.; Araki, M.; Minami, Y.; Soeda, T.; Yonetsu, T.; McNulty, I.; Lee, H.; Nakamura, S.; Jang, I.-K. Layered plaque characteristics and layer burden in acute coronary syndromes. Am. J. Cardiol. 2021, 164, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Araki, M.; Yonetsu, T.; Kurihara, O.; Nakajima, A.; Lee, H.; Soeda, T.; Minami, Y.; McNulty, I.; Uemura, S.; Kakuta, T.; et al. Predictors of rapid plaque progression: An optical coherence tomography study. JACC Cardiovasc. Imaging 2021, 14, 1628–1638. [Google Scholar] [CrossRef]
- Araki, M.; Park, S.-J.; Dauerman, H.L.; Uemura, S.; Kim, J.-S.; Di Mario, C.; Johnson, T.W.; Guagliumi, G.; Kastrati, A.; Joner, M.; et al. Optical coherence tomography in coronary atherosclerosis assessment and intervention. Nat. Rev. Cardiol. 2022. [Google Scholar] [CrossRef]
- Montarello, N.J.; Singh, K.; Sinhal, A.; Wong, D.T.L.; Alcock, R.; Rajendran, S.; Dautov, R.; Barlis, P.; Patel, S.; Nidorf, S.M.; et al. Assessing the impact of colchicine on coronary plaque phenotype after myocardial infarction with optical coherence tomography: Rationale and design of the COCOMO-ACS study. Cardiovasc. Drugs Ther. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Nissen, S.E.; Prati, F.; Windecker, S.; Kataoka, Y.; Puri, R.; Hucko, T.; Kassahun, H.; Liao, J.; Somaratne, R. Assessing the impact of PCSK9 inhibition on coronary plaque phenotype with optical coherence tomography: Rationale and design of the randomized, placebo-controlled HUYGENS study. Cardiovasc. Diagn. Ther. 2021, 11, 120. [Google Scholar] [CrossRef]
- Habara, M.; Nasu, K.; Terashima, M.; Ko, E.; Yokota, D.; Ito, T.; Kurita, T.; Teramoto, T.; Kimura, M.; Kinoshita, Y. Impact on optical coherence tomographic coronary findings of fluvastatin alone versus fluvastatin+ ezetimibe. Am. J. Cardiol. 2014, 113, 580–587. [Google Scholar] [CrossRef]
- Komukai, K.; Kubo, T.; Kitabata, H.; Matsuo, Y.; Ozaki, Y.; Takarada, S.; Okumoto, Y.; Shiono, Y.; Orii, M.; Shimamura, K. Effect of atorvastatin therapy on fibrous cap thickness in coronary atherosclerotic plaque as assessed by optical coherence tomography: The EASY-FIT study. J. Am. Coll. Cardiol. 2014, 64, 2207–2217. [Google Scholar] [CrossRef]
- Gholipour, A.; Ghayesh, M.H.; Zander, A.C.; Psaltis, P.J. In vivo based biomechanics of right and left coronary arteries. Int. J. Eng. Sci. 2020, 154, 103281. [Google Scholar] [CrossRef]
- Toutouzas, K.; Chatzizisis, Y.S.; Riga, M.; Giannopoulos, A.; Antoniadis, A.P.; Tu, S.; Fujino, Y.; Mitsouras, D.; Doulaverakis, C.; Tsampoulatidis, I.; et al. Accurate and reproducible reconstruction of coronary arteries and endothelial shear stress calculation using 3D OCT: Comparative study to 3D IVUS and 3D QCA. Atherosclerosis 2015, 240, 510–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migliori, S.; Chiastra, C.; Bologna, M.; Montin, E.; Dubini, G.; Genuardi, L.; Aurigemma, C.; Mainardi, L.; Burzotta, F.; Migliavacca, F. Application of an OCT-based 3D reconstruction framework to the hemodynamic assessment of an ulcerated coronary artery plaque. Med. Eng. Phys. 2020, 78, 74–81. [Google Scholar] [CrossRef]
- Wang, L.; He, L.; Jia, H.; Lv, R.; Guo, X.; Yang, C.; Giddens, D.P.; Samady, H.; Maehara, A.; Mintz, G.; et al. Optical coherence tomography-based patient-specific residual multi-thrombus coronary plaque models with fluid-structure interaction for better treatment decisions: A biomechanical modeling case study. J. Biomech. Eng. 2021, 143, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, H.J.; Ghayesh, M.H.; Zander, A.C.; Ottaway, J.L.; Di Giovanni, G.; Nicholls, S.J.; Psaltis, P.J. Optical coherence tomography based biomechanical fluid-structure interaction analysis of coronary atherosclerosis progression. J. Vis. Exp. JoVE 2022, 179, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Tearney, G.J.; Regar, E.; Akasaka, T.; Adriaenssens, T.; Barlis, P.; Bezerra, H.G.; Bouma, B.; Bruining, N.; Cho, J.-M.; Chowdhary, S. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: A report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J. Am. Coll. Cardiol. 2012, 59, 1058–1072. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- De Boer, P.-T.; Kroese, D.P.; Mannor, S.; Rubinstein, R.Y. A tutorial on the cross-entropy method. Ann. Oper. Res. 2005, 134, 19–67. [Google Scholar] [CrossRef]
- Sudre, C.H.; Li, W.; Vercauteren, T.; Ourselin, S.; Jorge Cardoso, M. Generalised Dice Overlap as a Deep Learning Loss Function for Highly Unbalanced Segmentations. In Proceedings of the Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support, Cham, Switzerland, 14 September 2017; Cardoso, M.J., Arbel, T., Carneiro, G., Syeda-Mahmood, T., Tavares, J.M.R.S., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 240–248. [Google Scholar]
- Salehi, S.S.M.; Erdogmus, D.; Gholipour, A. Tversky Loss Function for Image Segmentation Using 3D Fully Convolutional Deep Networks. In Proceedings of the Machine Learning in Medical Imaging, Cham, Switzerland, 14 September 2017; Wang, Q., Shi, Y., Suk, H.-I., Suzuki, K., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 379–387. [Google Scholar]
- Sony, S.; Dunphy, K.; Sadhu, A.; Capretz, M. A systematic review of convolutional neural network-based structural condition assessment techniques. Eng. Struct. 2021, 226, 1–16. [Google Scholar] [CrossRef]
- Hassoun, M.H. Fundamentals of Artificial Neural Networks; MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Chen, L.-C.; Papandreou, G.; Kokkinos, I.; Murphy, K.; Yuille, A.L. Semantic image segmentation with deep convolutional nets and fully connected crfs. arXiv 2014, arXiv:1412.7062. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015, Munich, Germany, 5–9 October 2015; Navab, N., Hornegger, J., Wells, W.M., Frangi, A.F., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Litjens, G.; Ciompi, F.; Wolterink Jelmer, M.; de Vos Bob, D.; Leiner, T.; Teuwen, J.; Išgum, I. State-of-the-art deep learning in cardiovascular image analysis. JACC Cardiovasc. Imaging 2019, 12, 1549–1565. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Jeyaseelan, L.; Li, Q.; Chiang, J.N.; Wu, Z.; Ding, X. Embracing imperfect datasets: A review of deep learning solutions for medical image segmentation. Med. Image Anal. 2020, 63, 1–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gudigar, A.; Nayak, S.; Samanth, J.; Raghavendra, U.; AJ, A.; Barua, P.D.; Hasan, M.N.; Ciaccio, E.J.; Tan, R.-S.; Rajendra Acharya, U. Recent trends in artificial intelligence-assisted coronary atherosclerotic plaque characterization. Int. J. Environ. Res. Public Health 2021, 18, 1–27. [Google Scholar]
- Boi, A.; Jamthikar, A.D.; Saba, L.; Gupta, D.; Sharma, A.; Loi, B.; Laird, J.R.; Khanna, N.N.; Suri, J.S. A survey on coronary atherosclerotic plaque tissue characterization in intravascular optical coherence tomography. Curr. Atheroscler. Rep. 2018, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Johnson Kipp, W.; Torres Soto, J.; Glicksberg Benjamin, S.; Shameer, K.; Miotto, R.; Ali, M.; Ashley, E.; Dudley Joel, T. Artificial intelligence in cardiology. J. Am. Coll. Cardiol. 2018, 71, 2668–2679. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Ding, Z.; Tao, K.; Li, Q.; Kuang, H.; Tian, F.; Zhou, S.; Hua, P.; Hu, J.; Shang, M.; et al. Automatic lumen segmentation using uniqueness of vascular connected region for intravascular optical coherence tomography. J. Biophotonics 2021, 14, e202100124. [Google Scholar] [CrossRef] [PubMed]
- Otsu, N. A threshold selection method from gray-level histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; He, B.; Ding, Z.; Tao, K.; Lai, T.; Kuang, H.; Liu, R.; Zhang, X.; Zheng, Y.; Zheng, J. Automatic lumen segmentation in intravascular optical coherence tomography using morphological features. IEEE Access 2019, 7, 88859–88869. [Google Scholar] [CrossRef]
- Macedo, M.M.G.D.; Takimura, C.K.; Lemos, P.A.; Gutierrez, M.A. A robust fully automatic lumen segmentation method for in vivo intracoronary optical coherence tomography. Res. Biomed. Eng. 2016, 32, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Cheimariotis, G.-A.; Chatzizisis, Y.S.; Koutkias, V.G.; Toutouzas, K.; Giannopoulos, A.; Riga, M.; Chouvarda, I.; Antoniadis, A.P.; Doulaverakis, C.; Tsamboulatidis, I.; et al. ARCOCT: Automatic detection of lumen border in intravascular OCT images. Comput. Methods Programs Biomed. 2017, 151, 21–32. [Google Scholar] [CrossRef]
- Bologna, M.; Migliori, S.; Montin, E.; Rampat, R.; Dubini, G.; Migliavacca, F.; Mainardi, L.; Chiastra, C. Automatic segmentation of optical coherence tomography pullbacks of coronary arteries treated with bioresorbable vascular scaffolds: Application to hemodynamics modeling. PLoS ONE 2019, 14, e0213603. [Google Scholar] [CrossRef]
- Akbar, A.; Khwaja, T.S.; Javaid, A.; Kim, J.-S.; Ha, J. Automated accurate lumen segmentation using L-mode interpolation for three-dimensional intravascular optical coherence tomography. Biomed. Opt. Express 2019, 10, 5325–5336. [Google Scholar] [CrossRef] [PubMed]
- Pociask, E.; Malinowski, K.P.; Ślęzak, M.; Jaworek-Korjakowska, J.; Wojakowski, W.; Roleder, T. Fully automated lumen segmentation method for intracoronary optical coherence tomography. J. Healthc. Eng. 2018, 2018, 1414076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moraes, M.C.; Cardenas, D.A.C.; Furuie, S.S. Automatic lumen segmentation in IVOCT images using binary morphological reconstruction. BioMed. Eng. OnLine 2013, 12, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, S.; Adnan, A.; Adlam, D. Automatic segmentation of coronary morphology using transmittance-based lumen intensity-enhanced intravascular optical coherence tomography images and applying a localized level-set-based active contour method. J. Med. Imaging 2016, 3, 044001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, A.G.; Conjeti, S.; Carlier, S.G.; Dutta, P.K.; Kastrati, A.; Laine, A.F.; Navab, N.; Katouzian, A.; Sheet, D. Lumen segmentation in intravascular optical coherence tomography using backscattering tracked and initialized random walks. IEEE J. Biomed. Health Inform. 2016, 20, 606–614. [Google Scholar]
- Essa, E.; Xie, X. Automatic segmentation of cross-sectional coronary arterial images. Comput. Vis. Image Underst. 2017, 165, 97–110. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.M.; Iverson, L.R.; Liaw, A. Newer classification and regression tree techniques: Bagging and random forests for ecological prediction. Ecosystems 2006, 9, 181–199. [Google Scholar] [CrossRef]
- Li, K.; Wu, X.; Chen, D.Z.; Sonka, M. Optimal surface segmentation in volumetric images-a graph-theoretic approach. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 28, 119–134. [Google Scholar]
- Cao, Y.; Cheng, K.; Qin, X.; Yin, Q.; Li, J.; Zhu, R.; Zhao, W. Automatic lumen segmentation in intravascular optical coherence tomography images using level set. Comput. Math. Methods Med. 2017, 2017, 4710305. [Google Scholar] [CrossRef]
- Macedo, M.M.G.; Guimarães, W.V.N.; Galon, M.Z.; Takimura, C.K.; Lemos, P.A.; Gutierrez, M.A. A bifurcation identifier for IV-OCT using orthogonal least squares and supervised machine learning. Comput. Med. Imaging Graph. 2015, 46, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Jin, Q.; Chen, Y.; Yin, Q.; Qin, X.; Li, J.; Zhu, R.; Zhao, W. Automatic side branch ostium detection and main vascular segmentation in intravascular optical coherence tomography images. IEEE J. Biomed. Health Inform. 2018, 22, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, M.; Costa, M.G.F.; Gutierrez, M.A.; Costa, J.P.G.F.; Filho, C.F.F.C. Detecting vascular bifurcation in IVOCT images using convolutional neural networks with transfer learning. IEEE Access 2019, 7, 66167–66175. [Google Scholar] [CrossRef]
- Miyagawa, M.; Costa, M.G.F.; Gutierrez, M.A.; Costa, J.P.G.F.; Costa Filho, C.F. Lumen Segmentation in Optical Coherence Tomography Images Using Convolutional Neural Network. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; pp. 600–603. [Google Scholar]
- Porto, C.; Costa Filho, C.F.; Macedo, M.M.; Gutierrez, M.A.; Costa, M.G.F. Classification of Bifurcations Regions in IVOCT Images Using Support Vector Machine and Artificial Neural Network Models. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 13–16 February 2017. [Google Scholar]
- Wang, A.; Eggermont, J.; Reiber, J.H.; Dijkstra, J. Fully automated side branch detection in intravascular optical coherence tomography pullback runs. Biomed. Opt. Express 2014, 5, 3160–3173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinlan, J.R. Bagging, boosting, and C4. 5. In Proceedings of the Aaai/iaai, Portland, OR, USA, 4–8 August 1996; Volume 1, pp. 725–730. [Google Scholar]
- Freund, Y.; Schapire, R.E. A decision-theoretic generalization of on-line learning and an application to boosting. J. Comput. Syst. Sci. 1997, 55, 119–139. [Google Scholar] [CrossRef] [Green Version]
- Quinlan, J.R. C4. 5: Programs for Machine Learning; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Yang, S.; Yoon, H.-J.; Yazdi, S.J.M.; Lee, J.-H. A novel automated lumen segmentation and classification algorithm for detection of irregular protrusion after stents deployment. Int. J. Med. Robot. Comput. Assist. Surg. 2020, 16, e2033. [Google Scholar] [CrossRef]
- Yong, Y.L.; Tan, L.K.; McLaughlin, R.; Chee, K.H.; Liew, Y.M. Linear-regression convolutional neural network for fully automated coronary lumen segmentation in intravascular optical coherence tomography. J. Biomed. Opt. 2017, 22, 126005. [Google Scholar] [CrossRef] [Green Version]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Tang, J.; Lan, Y.; Chen, S.; Zhong, Y.; Huang, C.; Peng, Y.; Liu, Q.; Cheng, Y.; Chen, F.; Che, W. Lumen contour segmentation in IVOCT based on N-type CNN. IEEE Access 2019, 7, 135573–135581. [Google Scholar] [CrossRef]
- Pyxaras, S.A.; Tu, S.; Barbato, E.; Barbati, G.; Di Serafino, L.; De Vroey, F.; Toth, G.; Mangiacapra, F.; Sinagra, G.; De Bruyne, B.; et al. Quantitative angiography and optical coherence tomography for the functional assessment of nonobstructive coronary stenoses: Comparison with fractional flow reserve. Am. Heart J. 2013, 166, 1010–1018. [Google Scholar] [CrossRef]
- Westra, J.; Andersen Birgitte, K.; Campo, G.; Matsuo, H.; Koltowski, L.; Eftekhari, A.; Liu, T.; Di Serafino, L.; Di Girolamo, D.; Escaned, J.; et al. Diagnostic performance of in-procedure angiography-derived quantitative flow reserve compared to pressure-derived fractional flow feserve: The FAVOR II Europe-Japan study. J. Am. Heart Assoc. 2018, 7, e009603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, P.H.; Saito, S.; Takahashi, S.; Makita, Y.; Nakamura, S.; Kawasaki, T.; Takahashi, A.; Katsuki, T.; Nakamura, S.; Namiki, A. Prediction of progression of coronary artery disease and clinical outcomes using vascular profiling of endothelial shear stress and arterial plaque characteristics: The PREDICTION Study. Circulation 2012, 126, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, L.; Nezami, F.R.; Galon, M.Z.; Lopes, A.C.; Lemos, P.A.; Hernandez, J.M.d.l.T.; Ben-Assa, E.; Edelman, E.R. Optimized computer-aided segmentation and three-dimensional reconstruction using intracoronary optical coherence tomography. IEEE J. Biomed. Health Inform. 2018, 22, 1168–1176. [Google Scholar] [CrossRef]
- Athanasiou, L.; Bourantas, C.; Rigas, G.; Sakellarios, A.; Exarchos, T.; Siogkas, P.; Ricciardi, A.; Naka, K.; Papafaklis, M.; Michalis, L.; et al. Methodology for fully automated segmentation and plaque characterization in intracoronary optical coherence tomography images. J. Biomed. Opt. 2014, 19, 026009. [Google Scholar] [CrossRef] [PubMed]
- Balaji, A.; Kelsey, L.J.; Majeed, K.; Schultz, C.J.; Doyle, B.J. Coronary artery segmentation from intravascular optical coherence tomography using deep capsules. Artif. Intell. Med. 2021, 116, 102072. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Proceedings of the European Conference on Computer Vision, Amsterdam, The Netherlands, 8–16 October 2016; pp. 630–645. [Google Scholar]
- LaLonde, R.; Bagci, U. Capsules for object segmentation. arXiv 2018, arXiv:1804.04241. [Google Scholar]
- Sabour, S.; Frosst, N.; Hinton, G.E. Dynamic routing between capsules. arXiv 2017, arXiv:1710.09829. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Amsterdam, The Netherlands, 8–16 October 2016; pp. 770–778. [Google Scholar]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar]
- Chen, L.-C.; Papandreou, G.; Schroff, F.; Adam, H. Rethinking atrous convolution for semantic image segmentation. arXiv 2017, arXiv:1706.05587. [Google Scholar]
- Zahnd, G.; Hoogendoorn, A.; Combaret, N.; Karanasos, A.; Péry, E.; Sarry, L.; Motreff, P.; Niessen, W.; Regar, E.; van Soest, G.; et al. Contour segmentation of the intima, media, and adventitia layers in intracoronary OCT images: Application to fully automatic detection of healthy wall regions. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 1923–1936. [Google Scholar] [CrossRef] [Green Version]
- Abdolmanafi, A.; Duong, L.; Dahdah, N.; Cheriet, F. Deep feature learning for automatic tissue classification of coronary artery using optical coherence tomography. Biomed. Opt. Express 2017, 8, 1203–1220. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Pazdernik, M.; Zhang, H.; Wahle, A.; Guo, Z.; Bedanova, H.; Kautzner, J.; Melenovsky, V.; Kovarnik, T.; Sonka, M. Quantitative 3D analysis of coronary wall morphology in heart transplant patients: OCT-assessed cardiac allograft vasculopathy progression. Med. Image Anal. 2018, 50, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Pazdernik, M.; Chen, Z.; Bedanova, H.; Kautzner, J.; Melenovsky, V.; Karmazin, V.; Malek, I.; Tomasek, A.; Ozabalova, E.; Krejci, J.; et al. Early detection of cardiac allograft vasculopathy using highly automated 3-dimensional optical coherence tomography analysis. J. Heart Lung Transplant. 2018, 37, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Zhang, X.; Williams, R.; Wu, X.; Anderson, D.D.; Sonka, M. LOGISMOS—Layered optimal graph image segmentation of multiple objects and surfaces: Cartilage segmentation in the knee joint. IEEE Trans. Med. Imaging 2010, 29, 2023–2037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Lee, K.; Chen, Z.; Kashyap, S.; Sonka, M. Chapter 11—LOGISMOS-JEI: Segmentation Using Optimal Graph Search and Just-Enough Interaction. In Handbook of Medical Image Computing and Computer Assisted Intervention; Zhou, S.K., Rueckert, D., Fichtinger, G., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 249–272. [Google Scholar]
- Jia, Y.; Shelhamer, E.; Donahue, J.; Karayev, S.; Long, J.; Girshick, R.; Guadarrama, S.; Darrell, T. Caffe: Convolutional architecture for fast feature embedding. In Proceedings of the 22nd ACM International Conference on Multimedia, Orlando, FL, USA, 3–7 November 2014; pp. 675–678. [Google Scholar]
- Otsuka, K.; Villiger, M.; Nadkarni, S.K.; Bouma, B.E. Intravascular polarimetry for tissue characterization of coronary atherosclerosis. Circ. Rep. 2019, 1, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Otsuka, K.; Villiger, M.; Nadkarni, S.K.; Bouma, B.E. Intravascular polarimetry: Clinical translation and future applications of catheter-based polarization sensitive optical frequency domain imaging. Front. Cardiovasc. Med. 2020, 7, 146. [Google Scholar] [CrossRef]
- Villiger, M.; Otsuka, K.; Karanasos, A.; Doradla, P.; Ren, J.; Lippok, N.; Shishkov, M.; Daemen, J.; Diletti, R.; van Geuns, R.-J. Coronary plaque microstructure and composition modify optical polarization: A new endogenous contrast mechanism for optical frequency domain imaging. JACC Cardiovasc. Imaging 2018, 11, 1666–1676. [Google Scholar] [CrossRef] [Green Version]
- Haft-Javaherian, M.; Villiger, M.; Otsuka, K.; Daemen, J.; Libby, P.; Golland, P.; Bouma, B.E. Segmentation of anatomical layers and artifacts in intravascular polarization sensitive optical coherence tomography using attending physician and boundary cardinality lost terms. arXiv 2021, arXiv:2105.05137. [Google Scholar]
- Xu, B.; Wang, N.; Chen, T.; Li, M. Empirical evaluation of rectified activations in convolutional network. arXiv 2015, arXiv:1505.00853. [Google Scholar]
- Li, J.; Montarello, N.J.; Hoogendoorn, A.; Verjans, J.W.; Bursill, C.A.; Peter, K.; Nicholls, S.J.; McLaughlin, R.A.; Psaltis, P.J. Multimodality intravascular imaging of high-risk coronary plaque. JACC Cardiovasc. Imaging 2021, 15, 145–159. [Google Scholar] [CrossRef]
- Olender, M.L.; Athanasiou, L.S.; Hernández, J.M.d.l.T.; Ben-Assa, E.; Nezami, F.R.; Edelman, E.R. A Mechanical Approach for Smooth Surface Fitting to Delineate Vessel Walls in Optical Coherence Tomography Images. IEEE Trans. Med. Imaging 2019, 38, 1384–1397. [Google Scholar] [CrossRef]
- Olender, M.L.; Athanasiou, L.S.; José, M.; Camarero, T.G.; Cascón, J.D.; Consuegra-Sanchez, L.; Edelman, E.R. Estimating the internal elastic membrane cross-sectional area of coronary arteries autonomously using optical coherence tomography images. In Proceedings of the 2017 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Orlando, FL, USA, 16–19 February 2017; pp. 109–112. [Google Scholar]
- Prabhu, D.S.; Bezerra, H.G.; Kolluru, C.; Gharaibeh, Y.; Mehanna, E.; Wu, H.; Wilson, D.L. Automated A-line coronary plaque classification of intravascular optical coherence tomography images using handcrafted features and large datasets. J. Biomed. Opt. 2019, 24, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Long, F.; Ding, C. Feature selection based on mutual information criteria of max-dependency, max-relevance, and min-redundancy. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 27, 1226–1238. [Google Scholar] [CrossRef] [PubMed]
- Parmar, C.; Grossmann, P.; Bussink, J.; Lambin, P.; Aerts, H.J. Machine learning methods for quantitative radiomic biomarkers. Sci. Rep. 2015, 5, 13087. [Google Scholar] [CrossRef] [PubMed]
- Krähenbühl, P.; Koltun, V. Efficient inference in fully connected crfs with gaussian edge potentials. Adv. Neural Inf. Process. Syst. 2011, 24, 109–117. [Google Scholar]
- Leung, T.; Malik, J. Representing and recognizing the visual appearance of materials using three-dimensional textons. Int. J. Comput. Vis. 2001, 43, 29–44. [Google Scholar] [CrossRef]
- Zhang, C.; Guo, X.; Guo, X.; Molony, D.; Li, H.; Samady, H.; Giddens, D.P.; Athanasiou, L.; Tang, D.; Nie, R.; et al. Machine learning model comparison for automatic segmentation of intracoronary optical coherence tomography and plaque cap thickness quantification. Comput. Model. Eng. Sci. 2020, 123, 631–646. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Jégou, S.; Drozdzal, M.; Vazquez, D.; Romero, A.; Bengio, Y. The one hundred layers tiramisu: Fully convolutional densenets for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 11–19. [Google Scholar]
- Lv, R.; Maehara, A.; Matsumura, M.; Wang, L.; Wang, Q.; Zhang, C.; Guo, X.; Samady, H.; Giddens, D.P.; Zheng, J.; et al. Using optical coherence tomography and intravascular ultrasound imaging to quantify coronary plaque cap thickness and vulnerability: A pilot study. BioMed. Eng. OnLine 2020, 19, 90. [Google Scholar] [CrossRef]
- Zahnd, G.; Karanasos, A.; van Soest, G.; Regar, E.; Niessen, W.; Gijsen, F.; van Walsum, T. Quantification of fibrous cap thickness in intracoronary optical coherence tomography with a contour segmentation method based on dynamic programming. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 1383–1394. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Chamie, D.; Bezerra, H.G.; Yamamoto, H.; Kanovsky, J.; Wilson, D.L.; Costa, M.A.; Rollins, A.M. Volumetric quantification of fibrous caps using intravascular optical coherence tomography. Biomed. Opt. Express 2012, 3, 1413–1426. [Google Scholar] [CrossRef]
- Zhang, C.; Li, H.; Guo, X.; Molony, D.; Guo, X.; Samady, H.; Giddens, D.P.; Athanasiou, L.; Nie, R.; Cao, J.; et al. Convolution neural networks and support vector machines for automatic segmentation of intracoronary optical coherence tomography. Mol. Cell. Biomech. 2019, 16, 153–161. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, B.; Wang, H.; Lin, F.; Han, Y.; Liu, X. Automated characterization and classification of coronary atherosclerotic plaques for intravascular optical coherence tomography. Biocybern. Biomed. Eng. 2019, 39, 719–727. [Google Scholar] [CrossRef]
- Wang, P.; Zhu, H.; Ling, X. Intravascular optical coherence tomography image segmentation based on Gaussian mixture model and adaptive fourth-order PDE. Signal Image Video Process. 2020, 14, 29–37. [Google Scholar] [CrossRef]
- Rico-Jimenez, J.J.; Campos-Delgado, D.U.; Villiger, M.; Otsuka, K.; Bouma, B.E.; Jo, J.A. Automatic classification of atherosclerotic plaques imaged with intravascular OCT. Biomed. Opt. Express 2016, 7, 4069–4085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gessert, N.; Lutz, M.; Heyder, M.; Latus, S.; Leistner, D.M.; Abdelwahed, Y.S.; Schlaefer, A. Automatic plaque detection in IVOCT pullbacks using convolutional neural networks. IEEE Trans. Med. Imaging 2019, 38, 426–434. [Google Scholar] [CrossRef] [Green Version]
- Athanasiou, L.S.; Olender, M.L.; José, M.; Ben-Assa, E.; Edelman, E.R. A deep learning approach to classify atherosclerosis using intracoronary optical coherence tomography. In Proceedings of the Medical Imaging 2019: Computer-Aided Diagnosis, San Diego, CA, USA, 17–20 February 2019; pp. 163–170. [Google Scholar]
- Abdolmanafi, A.; Duong, L.; Dahdah, N.; Adib, I.R.; Cheriet, F. Characterization of coronary artery pathological formations from OCT imaging using deep learning. Biomed. Opt. Express 2018, 9, 4936–4960. [Google Scholar] [CrossRef]
- Abdolmanafi, A.; Cheriet, F.; Duong, L.; Ibrahim, R.; Dahdah, N. An automatic diagnostic system of coronary artery lesions in Kawasaki disease using intravascular optical coherence tomography imaging. J. Biophotonics 2019, 13, e201900112. [Google Scholar] [CrossRef]
- Abdolmanafi, A.; Duong, L.; Ibrahim, R.; Dahdah, N. A deep learning-based model for characterization of atherosclerotic plaque in coronary arteries using optical coherence tomography images. Med. Phys. 2021, 48, 3511–3524. [Google Scholar] [CrossRef]
- Li, L.; Jia, T. Optical coherence tomography vulnerable plaque segmentation based on deep residual U-net. Rev. Cardiovasc. Med. 2019, 20, 171–177. [Google Scholar]
- Huang, Y.; He, C.; Wang, J.; Miao, Y.; Zhu, T.; Zhou, P.; Li, Z. Intravascular optical coherence tomography image segmentation based on support vector machine algorithm. MCB Mol. Cell. Biomech. 2018, 15, 117–125. [Google Scholar]
- You, Y.-L.; Kaveh, M. Fourth-order partial differential equations for noise removal. IEEE Trans. Image Process. 2000, 9, 1723–1730. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.M.; Wu, Q.J. Fast and robust spatially constrained Gaussian mixture model for image segmentation. IEEE Trans. Circuits Syst. Video Technol. 2012, 23, 621–635. [Google Scholar] [CrossRef]
- Kumar, R.; Srivastava, S.; Srivastava, R. A fourth order PDE based fuzzy c-means approach for segmentation of microscopic biopsy images in presence of Poisson noise for cancer detection. Comput. Methods Programs Biomed. 2017, 146, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, M.M.; Bezdek, J.C. Low-level segmentation of aerial images with fuzzy clustering. IEEE Trans. Syst. Man Cybern. 1986, 16, 589–598. [Google Scholar] [CrossRef]
- Sfikas, G.; Nikou, C.; Galatsanos, N. Robust image segmentation with mixtures of Student’s t-distributions. In Proceedings of the 2007 IEEE International Conference on Image Processing, San Antonio, TX, USA, 16–19 September 2007; pp. 273–276. [Google Scholar]
- Titterington, D.M.; Afm, S.; Smith, A.F.; Makov, U. Statistical Analysis of Finite Mixture Distributions; John Wiley & Sons Incorporated: Hoboken, NJ, USA, 1985; Volume 198. [Google Scholar]
- Bi, H.; Tang, H.; Yang, G.; Shu, H.; Dillenseger, J.-L. Accurate image segmentation using Gaussian mixture model with saliency map. Pattern Anal. Appl. 2018, 21, 869–878. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Du, J.; Yang, J.; Xiong, P.; Liu, J.; Lin, F. Coronary artery fibrous plaque detection based on multi-scale convolutional neural networks. J. Signal Process. Syst. 2020, 92, 325–333. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Liu, W.; Anguelov, D.; Erhan, D.; Szegedy, C.; Reed, S.; Fu, C.-Y.; Berg, A.C. SSD: Single shot multibox detector. In Proceedings of the European Conference on Computer Vision, Amsterdam, The Netherlands, 8–16 October 2016; pp. 21–37. [Google Scholar]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You only look once: Unified, real-time object detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 779–788. [Google Scholar]
- Redmon, J.; Farhadi, A. YOLO9000: Better, faster, stronger. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 7263–7271. [Google Scholar]
- Redmon, J.; Farhadi, A. Yolov3: An incremental improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar]
- Liu, R.; Zhang, Y.; Zheng, Y.; Liu, Y.; Zhao, Y.; Yi, L. Automated detection of vulnerable plaque for intravascular optical coherence tomography images. Cardiovasc. Eng. Technol. 2019, 10, 590–603. [Google Scholar] [CrossRef]
- Gerbaud, E.; Weisz, G.; Tanaka, A.; Luu, R.; Osman, H.A.S.H.; Baldwin, G.; Coste, P.; Cognet, L.; Waxman, S.; Zheng, H.; et al. Plaque burden can be assessed using intravascular optical coherence tomography and a dedicated automated processing algorithm: A comparison study with intravascular ultrasound. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 640–652. [Google Scholar] [CrossRef]
- Isidori, F.; Lella, E.; Marco, V.; Albertucci, M.; Ozaki, Y.; La Manna, A.; Biccirè, F.G.; Romagnoli, E.; Bourantas, C.V.; Paoletti, G.; et al. Adoption of a new automated optical coherence tomography software to obtain a lipid plaque spread-out plot. Int. J. Cardiovasc. Imaging 2021, 37, 3129–3135. [Google Scholar] [CrossRef]
- Rico-Jimenez, J.J.; Campos-Delgado, D.U.; Buja, L.M.; Vela, D.; Jo, J.A. Intravascular optical coherence tomography method for automated detection of macrophage infiltration within atherosclerotic coronary plaques. Atherosclerosis 2019, 290, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Shibutani, H.; Fujii, K.; Ueda, D.; Kawakami, R.; Imanaka, T.; Kawai, K.; Matsumura, K.; Hashimoto, K.; Yamamoto, A.; Hao, H.; et al. Automated classification of coronary atherosclerotic plaque in optical frequency domain imaging based on deep learning. Atherosclerosis 2021, 328, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Kolluru, C.; Prabhu, D.; Gharaibeh, Y.; Bezerra, H.; Guagliumi, G.; Wilson, D. Deep neural networks for A-line-based plaque classification in coronary intravascular optical coherence tomography images. J. Med. Imaging 2018, 5, 044504. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Prabhu, D.; Kolluru, C.; Gharaibeh, Y.; Zimin, V.N.; Dallan, L.A.P.; Bezerra, H.G.; Wilson, D.L. Fully automated plaque characterization in intravascular OCT images using hybrid convolutional and lumen morphology features. Sci. Rep. 2020, 10, 2596. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Prabhu, D.; Kolluru, C.; Gharaibeh, Y.; Zimin, V.N.; Bezerra, H.G.; Wilson, D.L. Automated plaque characterization using deep learning on coronary intravascular optical coherence tomographic images. Biomed. Opt. Express 2019, 10, 6497–6515. [Google Scholar] [CrossRef] [PubMed]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef]
- Chen, L.-C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-decoder with atrous separable convolution for semantic image segmentation. In Proceedings of the European Conference on Computer Vision (ECCV), Glasgow, UK, 23–28 August 2018; pp. 801–818. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Cheimariotis, G.-A.; Riga, M.; Haris, K.; Toutouzas, K.; Katsaggelos, A.K.; Maglaveras, N. Automatic classification of A-lines in intravascular OCT images using deep learning and estimation of attenuation coefficients. Appl. Sci. 2021, 11, 7412. [Google Scholar] [CrossRef]
- Liu, S.; Sotomi, Y.; Eggermont, J.; Nakazawa, G.; Torii, S.; Ijichi, T.; Onuma, Y.; Serruys, P.W.; Lelieveldt, B.P.; Dijkstra, J. Tissue characterization with depth-resolved attenuation coefficient and backscatter term in intravascular optical coherence tomography images. J. Biomed. Opt. 2017, 22, 096004. [Google Scholar] [CrossRef] [Green Version]
- Ughi, G.J.; Adriaenssens, T.; Sinnaeve, P.; Desmet, W.; D’hooge, J. Automated tissue characterization of in vivo atherosclerotic plaques by intravascular optical coherence tomography images. Biomed. Opt. Express 2013, 4, 1014–1030. [Google Scholar] [CrossRef] [Green Version]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Zhang, Z. Improved adam optimizer for deep neural networks. In Proceedings of the 2018 IEEE/ACM 26th International Symposium on Quality of Service (IWQoS), Banff, AB, Canada, 4–6 June 2018; pp. 1–2. [Google Scholar]
- He, C.; Wang, J.; Yin, Y.; Li, Z. Automated classification of coronary plaque calcification in OCT pullbacks with 3D deep neural networks. J. Biomed. Opt. 2020, 25, 095003. [Google Scholar] [CrossRef] [PubMed]
- Avital, Y.; Madar, A.; Arnon, S.; Koifman, E. Identification of coronary calcifications in optical coherence tomography imaging using deep learning. Sci. Rep. 2021, 11, 11269. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Gharaibeh, Y.; Kolluru, C.; Zimin, V.N.; Dallan, L.A.P.; Kim, J.N.; Bezerra, H.G.; Wilson, D.L. Segmentation of coronary calcified plaque in intravascular OCT images using a two-step deep learning approach. IEEE Access 2020, 8, 225581–225593. [Google Scholar] [CrossRef] [PubMed]
- Gharaibeh, Y.; Prabhu, D.; Kolluru, C.; Lee, J.; Zimin, V.; Bezerra, H.; Wilson, D. Coronary calcification segmentation in intravascular OCT images using deep learning: Application to calcification scoring. J. Med. Imaging 2019, 6, 045002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordts, M.; Omran, M.; Ramos, S.; Rehfeld, T.; Enzweiler, M.; Benenson, R.; Franke, U.; Roth, S.; Schiele, B. The cityscapes dataset for semantic urban scene understanding. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 3213–3223. [Google Scholar]
- Kolluru, C.; Lee, J.; Gharaibeh, Y.; Bezerra, H.G.; Wilson, D.L. Learning with fewer images via image clustering: Application to intravascular OCT image segmentation. IEEE Access 2021, 9, 37273–37280. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Iantorno, M.; Waksman, R. Restenosis of drug-eluting stents. Circ. Cardiovasc. Interv. 2019, 12, e007023. [Google Scholar] [CrossRef]
- Nam, H.S.; Kim, C.-S.; Lee, J.J.; Song, J.W.; Kim, J.W.; Yoo, H. Automated detection of vessel lumen and stent struts in intravascular optical coherence tomography to evaluate stent apposition and neointimal coverage. Med. Phys. 2016, 43, 1662–1675. [Google Scholar] [CrossRef]
- Wu, P.; Gutiérrez-Chico, J.L.; Tauzin, H.; Yang, W.; Li, Y.; Yu, W.; Chu, M.; Guillon, B.; Bai, J.; Meneveau, N. Automatic stent reconstruction in optical coherence tomography based on a deep convolutional model. Biomed. Opt. Express 2020, 11, 3374–3394. [Google Scholar] [CrossRef]
- Cao, Y.; Jin, Q.; Lu, Y.; Jing, J.; Chen, Y.; Yin, Q.; Qin, X.; Li, J.; Zhu, R.; Zhao, W. Automatic analysis of bioresorbable vascular scaffolds in intravascular optical coherence tomography images. Biomed. Opt. Express 2018, 9, 2495–2510. [Google Scholar] [CrossRef]
- Zysk, A.M.; Nguyen, F.T.; Oldenburg, A.L.; Marks, D.L.; Boppart, S.A. Optical coherence tomography: A review of clinical development from bench to bedside. J. Biomed. Opt. 2007, 12, 051403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Zeng, Y.; Xiao, S.; He, S.; Ye, C.; Qi, Y.; Zhao, J.; Wei, D.; Hu, M.; Chen, F. Automatic detection of coronary metallic stent struts based on YOLOv3 and R-FCN. Comput. Math. Methods Med. 2020, 2020, 1793517. [Google Scholar] [CrossRef] [PubMed]
- Amrute, J.M.; Athanasiou, L.S.; Rikhtegar, F.; de la Torre Hernández, J.M.; Camarero, T.G.; Edelman, E.R. Polymeric endovascular strut and lumen detection algorithm for intracoronary optical coherence tomography images. J. Biomed. Opt. 2018, 23, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Lau, Y.S.; Tan, L.K.; Chan, C.K.; Chee, K.H.; Liew, Y.M. Automated segmentation of metal stent and bioresorbable vascular scaffold in intravascular optical coherence tomography images using deep learning architectures. Phys. Med. Biol. 2021, 66, 245026. [Google Scholar] [CrossRef]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.-C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]
- Lu, H.; Lee, J.; Ray, S.; Tanaka, K.; Bezerra, H.G.; Rollins, A.M.; Wilson, D.L. Automated stent coverage analysis in intravascular OCT (IVOCT) image volumes using a support vector machine and mesh growing. Biomed. Opt. Express 2019, 10, 2809–2828. [Google Scholar] [CrossRef]
- Chang, C.-C.; Lin, C.-J. LIBSVM: A library for support vector machines. ACM Trans. Intell. Syst. Technol. 2011, 2, 1–27. [Google Scholar] [CrossRef]
- Lu, H.; Lee, J.; Jakl, M.; Wang, Z.; Cervinka, P.; Bezerra, H.G.; Wilson, D.L. Application and evaluation of highly automated software for comprehensive stent analysis in intravascular optical coherence tomography. Sci. Rep. 2020, 10, 2150. [Google Scholar] [CrossRef] [Green Version]
- Lin, G.; Milan, A.; Shen, C.; Reid, I. Refinenet: Multi-path refinement networks for high-resolution semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1925–1934. [Google Scholar]
- O’Brien, C.C.; Kolandaivelu, K.; Brown, J.; Lopes, A.C.; Kunio, M.; Kolachalama, V.B.; Edelman, E.R. Constraining OCT with Knowledge of Device Design Enables High Accuracy Hemodynamic Assessment of Endovascular Implants. PLoS ONE 2016, 11, e0149178. [Google Scholar] [CrossRef]
- Chiastra, C.; Montin, E.; Bologna, M.; Migliori, S.; Aurigemma, C.; Burzotta, F.; Celi, S.; Dubini, G.; Migliavacca, F.; Mainardi, L. Reconstruction of stented coronary arteries from optical coherence tomography images: Feasibility, validation, and repeatability of a segmentation method. PLoS ONE 2017, 12, e0177495. [Google Scholar] [CrossRef]
- Wang, A.; Eggermont, J.; Dekker, N.; Garcia-Garcia, H.M.; Pawar, R.; Reiber, J.H.; Dijkstra, J. Automatic stent strut detection in intravascular optical coherence tomographic pullback runs. Int. J. Cardiovasc. Imaging 2013, 29, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Migliori, S.; Chiastra, C.; Bologna, M.; Montin, E.; Dubini, G.; Aurigemma, C.; Fedele, R.; Burzotta, F.; Mainardi, L.; Migliavacca, F. A framework for computational fluid dynamic analyses of patient-specific stented coronary arteries from optical coherence tomography images. Med. Eng. Phys. 2017, 47, 105–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, M.R.; Kim, D.; Molony, D.S.; Morris, L.; Samady, H.; Joshi, S.; Timmins, L.H. Establishment of an automated algorithm utilizing optical coherence tomography and micro-computed tomography imaging to reconstruct the 3-D deformed stent geometry. IEEE Trans. Med. Imaging 2019, 38, 710–720. [Google Scholar] [CrossRef] [PubMed]
- Tsantis, S.; Kagadis, G.C.; Katsanos, K.; Karnabatidis, D.; Bourantas, G.; Nikiforidis, G.C. Automatic vessel lumen segmentation and stent strut detection in intravascular optical coherence tomography. Med. Phys. 2012, 39, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Ughi, G.J.; Adriaenssens, T.; Onsea, K.; Kayaert, P.; Dubois, C.; Sinnaeve, P.; Coosemans, M.; Desmet, W.; D’hooge, J. Automatic segmentation of in-vivo intra-coronary optical coherence tomography images to assess stent strut apposition and coverage. Int. J. Cardiovasc. Imaging 2012, 28, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, X.; Mohar, D.; Raney, A.; Jing, J.; Zhang, J.; Johnston, A.; Liang, S.; Ma, T.; Shung, K.K.; et al. Integrated IVUS-OCT for real-time imaging of coronary atherosclerosis. JACC Cardiovasc. Imaging 2014, 7, 101–103. [Google Scholar] [CrossRef] [Green Version]
- Cha, S.-H. Comprehensive survey on distance/similarity measures between probability density functions. City 2007, 1, 300–307. [Google Scholar]
- Yeghiazaryan, V.; Voiculescu, I. Family of boundary overlap metrics for the evaluation of medical image segmentation. J. Med. Imaging 2018, 5, 015006. [Google Scholar] [CrossRef]
- Baxter, J.S.H.; Jannin, P. Bias in machine learning for computer-assisted surgery and medical image processing. Comput. Assist. Surg. 2022, 27, 1–3. [Google Scholar] [CrossRef]
- Sengupta Partho, P.; Shrestha, S.; Berthon, B.; Messas, E.; Donal, E.; Tison Geoffrey, H.; Min James, K.; D’hooge, J.; Voigt, J.-U.; Dudley, J.; et al. Proposed requirements for cardiovascular imaging-related machine learning evaluation (PRIME): A checklist. JACC Cardiovasc. Imaging 2020, 13, 2017–2035. [Google Scholar] [CrossRef]
- Cao, Y.; Fang, Z.; Wu, Y.; Zhou, D.-X.; Gu, Q. Towards understanding the spectral bias of deep learning. arXiv 2019, arXiv:1912.01198. [Google Scholar]
- Statnikov, A.; Wang, L.; Aliferis, C.F. A comprehensive comparison of random forests and support vector machines for microarray-based cancer classification. BMC Bioinform. 2008, 9, 319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vokinger, K.N.; Feuerriegel, S.; Kesselheim, A.S. Mitigating bias in machine learning for medicine. Commun. Med. 2021, 1, 25. [Google Scholar] [CrossRef] [PubMed]
- Bernard, O.; Lalande, A.; Zotti, C.; Cervenansky, F.; Yang, X.; Heng, P.A.; Cetin, I.; Lekadir, K.; Camara, O.; Ballester, M.A.G.; et al. Deep learning techniques for automatic MRI cardiac multi-structures segmentation and diagnosis: Is the problem solved? IEEE Trans. Med. Imaging 2018, 37, 2514–2525. [Google Scholar] [CrossRef] [PubMed]
- MONAI Medical Open Network for Artificial Intelligence. Available online: https://monai.io/index.html (accessed on 5 January 2022).
- Yi, X.; Walia, E.; Babyn, P. Generative adversarial network in medical imaging: A review. Med. Image Anal. 2019, 58, 101552. [Google Scholar] [CrossRef] [Green Version]
- Kazeminia, S.; Baur, C.; Kuijper, A.; van Ginneken, B.; Navab, N.; Albarqouni, S.; Mukhopadhyay, A. GANs for medical image analysis. Artif. Intell. Med. 2020, 109, 101938. [Google Scholar] [CrossRef]
- Chen, M.; Shi, X.; Zhang, Y.; Wu, D.; Guizani, M. Deep feature learning for medical image analysis with convolutional autoencoder neural network. IEEE Trans. Big Data 2021, 7, 750–758. [Google Scholar] [CrossRef]
- Kadry, K.; Olender, M.L.; Marlevi, D.; Edelman, E.R.; Nezami, F.R. A platform for high-fidelity patient-specific structural modelling of atherosclerotic arteries: From intravascular imaging to three-dimensional stress distributions. J. R. Soc. Interface 2021, 18, 20210436. [Google Scholar] [CrossRef]
- Griese, F.; Latus, S.; Schlüter, M.; Graeser, M.; Lutz, M.; Schlaefer, A.; Knopp, T. In-Vitro MPI-guided IVOCT catheter tracking in real time for motion artifact compensation. PLoS ONE 2020, 15, e0230821. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Samant, S.; de Zwart, G.; Zhao, S.; Khan, B.; Ahmad, M.; Bologna, M.; Watanabe, Y.; Murasato, Y.; Burzotta, F.; et al. 3D reconstruction of coronary artery bifurcations from coronary angiography and optical coherence tomography: Feasibility, validation, and reproducibility. Sci. Rep. 2020, 10, 18049. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhu, F.; Ding, Z.; Tao, K.; Lai, T.; Kuang, H.; Hua, P.; Shang, M.; Hu, J.; Yu, Y.; et al. Three-dimensional spatial reconstruction of coronary arteries based on fusion of intravascular optical coherence tomography and coronary angiography. J. Biophotonics 2021, 14, e202000370. [Google Scholar] [CrossRef]
- Wang, J.; Paritala, P.K.; Mendieta, J.B.; Komori, Y.; Raffel, O.C.; Gu, Y.; Li, Z. Optical coherence tomography-based patient-specific coronary artery reconstruction and fluid–structure interaction simulation. Biomech. Model. Mechanobiol. 2020, 19, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Schaap, M.; Metz, C.T.; van Walsum, T.; van der Giessen, A.G.; Weustink, A.C.; Mollet, N.R.; Bauer, C.; Bogunović, H.; Castro, C.; Deng, X. Standardized evaluation methodology and reference database for evaluating coronary artery centerline extraction algorithms. Med. Image Anal. 2009, 13, 701–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajhosseiny, R.; Munoz, C.; Cruz, G.; Khamis, R.; Kim, W.Y.; Prieto, C.; Botnar, R.M. Coronary magnetic resonance angiography in chronic coronary syndromes. Front. Cardiovasc. Med. 2021, 8, PMC8416045. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, H. Coronary CT versus MR angiography: The role of MR angiography. Radiology 2011, 258, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ma, T.; Zhou, Q.; Chen, Z. The integration of IVUS and OCT. In Multimodality Imaging: For Intravascular Application; Zhou, Q., Chen, Z., Eds.; Springer: Singapore, 2020; pp. 57–79. [Google Scholar]
- Fujii, K.; Hao, H.; Shibuya, M.; Imanaka, T.; Fukunaga, M.; Miki, K.; Tamaru, H.; Sawada, H.; Naito, Y.; Ohyanagi, M.; et al. Accuracy of OCT, grayscale IVUS, and their combination for the diagnosis of coronary TCFA. JACC Cardiovasc. Imaging 2015, 8, 451–460. [Google Scholar] [CrossRef] [Green Version]
- Fracassi, F.; Crea, F.; Sugiyama, T.; Yamamoto, E.; Uemura, S.; Vergallo, R.; Porto, I.; Lee, H.; Fujimoto, J.; Fuster, V.; et al. Healed culprit plaques in patients with acute coronary syndromes. J. Am. Coll. Cardiol. 2019, 73, 2253–2263. [Google Scholar] [CrossRef]
- Nadkarni, S.K.; Pierce, M.C.; Park, B.H.; de Boer, J.F.; Whittaker, P.; Bouma, B.E.; Bressner, J.E.; Halpern, E.; Houser, S.L.; Tearney, G.J. Measurement of collagen and smooth muscle cell content in atherosclerotic plaques using polarization-sensitive optical coherence tomography. J. Am. Coll. Cardiol. 2007, 49, 1474–1481. [Google Scholar] [CrossRef] [Green Version]
- MacRitchie, N.; Grassia, G.; Noonan, J.; Garside, P.; Graham, D.; Maffia, P. Molecular imaging of atherosclerosis: Spotlight on Raman spectroscopy and surface-enhanced Raman scattering. Heart 2018, 104, 460–467. [Google Scholar] [CrossRef]
- Osborn, E.A.; Jaffer, F.A. The advancing clinical impact of molecular imaging in CVD. JACC Cardiovasc. Imaging 2013, 6, 1327–1341. [Google Scholar] [CrossRef] [Green Version]
- Tarkin, J.M.; Joshi, F.R.; Rudd, J.H. PET imaging of inflammation in atherosclerosis. Nat. Rev. Cardiol. 2014, 11, 443–457. [Google Scholar] [CrossRef]
- Ughi, G.J.; Wang, H.; Gerbaud, E.; Gardecki, J.A.; Fard, A.M.; Hamidi, E.; Vacas-Jacques, P.; Rosenberg, M.; Jaffer, F.A.; Tearney, G.J. Clinical characterization of coronary atherosclerosis with dual-modality OCT and near-infrared autofluorescence imaging. JACC Cardiovasc. Imaging 2016, 9, 1304–1314. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Karimi Galougahi, K.; Maehara, A.; Shlofmitz, R.A.; Ben-Yehuda, O.; Mintz, G.S.; Stone, G.W. Intracoronary optical coherence tomography 2018: Current status and future directions. JACC Cardiovasc. Interv. 2017, 10, 2473–2487. [Google Scholar] [CrossRef] [PubMed]
- Calvert Patrick, A.; Obaid Daniel, R.; O’Sullivan, M.; Shapiro Leonard, M.; McNab, D.; Densem Cameron, G.; Schofield Peter, M.; Braganza, D.; Clarke Sarah, C.; Ray Kausik, K.; et al. Association between IVUS findings and adverse outcomes in patients with coronary artery disease. JACC Cardiovasc. Imaging 2011, 4, 894–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baruah, V.; Zahedivash, A.; Hoyt, T.; McElroy, A.; Vela, D.; Buja, L.M.; Cabe, A.; Oglesby, M.; Estrada, A.; Antonik, P.; et al. Automated coronary plaque characterization with intravascular optical coherence tomography and smart-algorithm approach. JACC Cardiovasc. Imaging 2020, 13, 1848–1850. [Google Scholar] [CrossRef]
- Holzapfel, G.A. Biomechanics of soft tissue. Handb. Mater. Behav. Models 2001, 3, 1049–1063. [Google Scholar]
- Hollander, Y.; Durban, D.; Lu, X.; Kassab, G.S.; Lanir, Y. Constitutive modeling of coronary arterial media—Comparison of three model classes. J. Biomech. Eng. 2011, 133, 061008. [Google Scholar] [CrossRef]
- Holzapfel, G.A.; Gasser, T.C.; Ogden, R.W. A new constitutive framework for arterial wall mechanics and a comparative study of material models. J. Elast. Phys. Sci. Solids 2000, 61, 1–48. [Google Scholar]
- Holzapfel, G.A.; Gasser, T.C.; Stadler, M. A structural model for the viscoelastic behavior of arterial walls: Continuum formulation and finite element analysis. Eur. J. Mech. A/Solids 2002, 21, 441–463. [Google Scholar] [CrossRef]
- Khaniki, H.B.; Ghayesh, M.H.; Chin, R.; Amabili, M. Large amplitude vibrations of imperfect porous-hyperelastic beams via a modified strain energy. J. Sound Vib. 2021, 513, 116416. [Google Scholar] [CrossRef]
- Rivlin, R.S. Large elastic deformations of isotropic materials IV. Further developments of the general theory. Philos. Trans. R. Soc. Lond. Ser. A Math. Phys. Sci. 1948, 241, 379–397. [Google Scholar]
- Narayanan, B.; Olender, M.L.; Marlevi, D.; Edelman, E.R.; Nezami, F.R. An inverse method for mechanical characterization of heterogeneous diseased arteries using intravascular imaging. Sci. Rep. 2021, 11, 22540. [Google Scholar] [CrossRef] [PubMed]
- Baldewsing, R.A.; Schaar, J.A.; Mastik, F.; Oomens, C.W.; van der Steen, A.F. Assessment of vulnerable plaque composition by matching the deformation of a parametric plaque model to measured plaque deformation. IEEE Trans. Med. Imaging 2005, 24, 514–528. [Google Scholar] [CrossRef] [PubMed]
- Baldewsing, R.A.; Danilouchkine, M.G.; Mastik, F.; Schaar, J.A.; Serruys, P.W.; van der Steen, A.F. An inverse method for imaging the local elasticity of atherosclerotic coronary plaques. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Le Floc’h, S.; Ohayon, J.; Tracqui, P.; Finet, G.; Gharib, A.M.; Maurice, R.L.; Cloutier, G.; Pettigrew, R.I. Vulnerable atherosclerotic plaque elasticity reconstruction based on a segmentation-driven optimization procedure using strain measurements: Theoretical framework. IEEE Trans. Med. Imaging 2009, 28, 1126–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, J.; Fenner, J. The challenge of clinical adoption—The insurmountable obstacle that will stop machine learning? BJR|Open 2019, 1, 20180017. [Google Scholar] [CrossRef]
- Bhattacharyya, A. On a measure of divergence between two statistical populations defined by their probability distributions. Bull. Calcutta Math. Soc. 1943, 35, 99–109. [Google Scholar]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Lawrence, I.; Lin, K. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar]
- Dice, L.R. Measures of the amount of ecologic association between species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Jaccard, P. The distribution of the flora in the alpine zone. 1. New Phytol. 1912, 11, 37–50. [Google Scholar] [CrossRef]
- Kullback, S.; Leibler, R.A. On information and sufficiency. Ann. Math. Stat. 1951, 22, 79–86. [Google Scholar] [CrossRef]














Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carpenter, H.J.; Ghayesh, M.H.; Zander, A.C.; Li, J.; Di Giovanni, G.; Psaltis, P.J. Automated Coronary Optical Coherence Tomography Feature Extraction with Application to Three-Dimensional Reconstruction. Tomography 2022, 8, 1307-1349. https://doi.org/10.3390/tomography8030108
Carpenter HJ, Ghayesh MH, Zander AC, Li J, Di Giovanni G, Psaltis PJ. Automated Coronary Optical Coherence Tomography Feature Extraction with Application to Three-Dimensional Reconstruction. Tomography. 2022; 8(3):1307-1349. https://doi.org/10.3390/tomography8030108
Chicago/Turabian StyleCarpenter, Harry J., Mergen H. Ghayesh, Anthony C. Zander, Jiawen Li, Giuseppe Di Giovanni, and Peter J. Psaltis. 2022. "Automated Coronary Optical Coherence Tomography Feature Extraction with Application to Three-Dimensional Reconstruction" Tomography 8, no. 3: 1307-1349. https://doi.org/10.3390/tomography8030108