
Preservation of the Posterior Interspinous Ligamentary Complex in Posterior and Transforaminal Lumbar Interbody Fusion
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Study Selection
2.2. Risk of Bias and Quality of Study
2.3. Data Collection
2.4. Statistical Analysis
3. Results
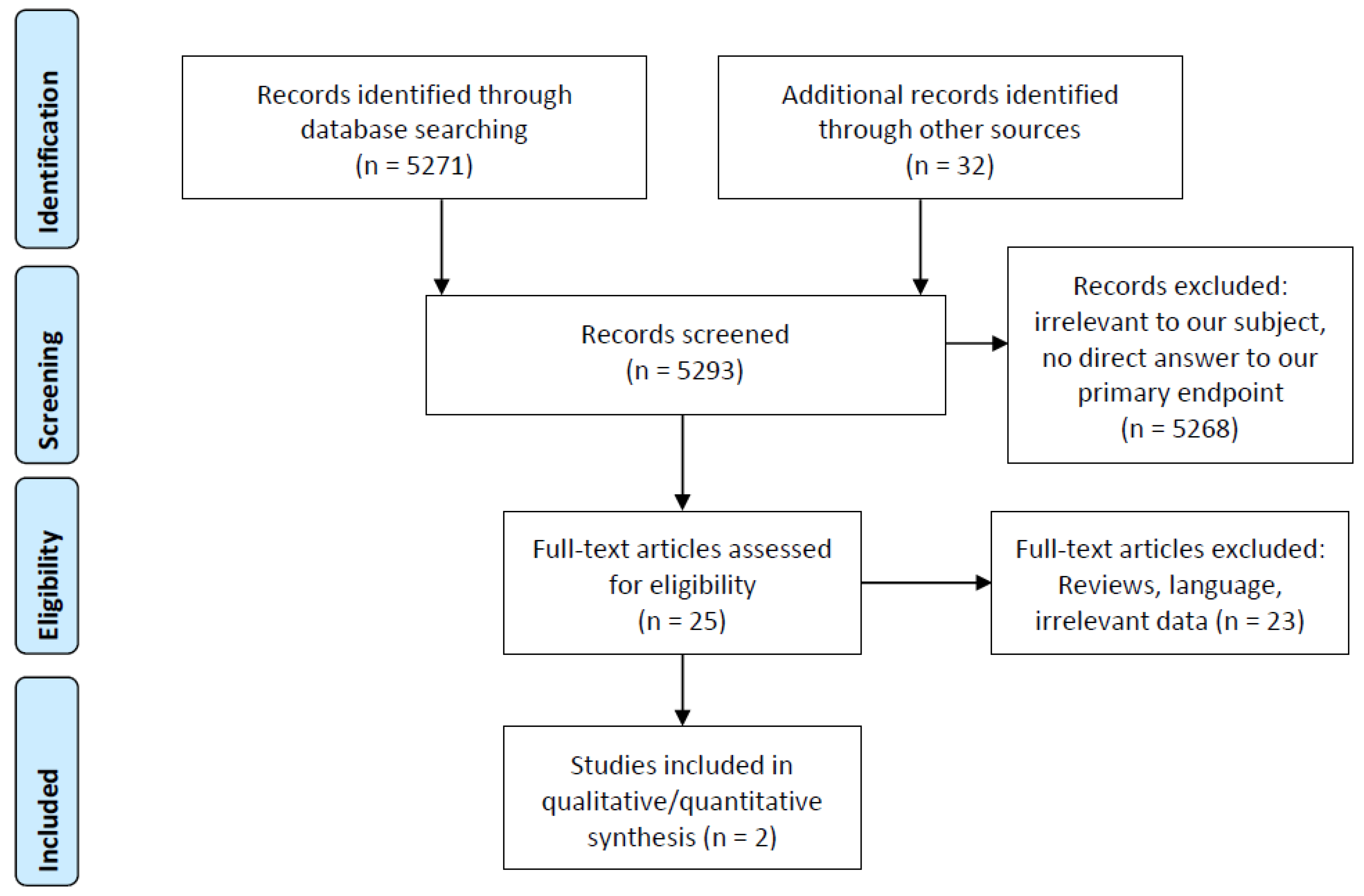
3.1. Search Results and Relevant Data Reported in Included Articles
3.2. Demographic Results
3.3. Surgical Parameters and Complications
3.4. Clinical and Radiological Outcomes
4. Discussion
4.1. Summary of Evidence
4.2. Biomechanical Considerations and Future Perspectives on ASD Pathophysiology
4.3. Limitations
5. Conclusions and Recommendations for Future Research
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Briggs, H.; Milligan, P.R. Chip fusion of the low back following exploration of the spinal canal. J. Bone Jt. Surg. Am. 1944, 26, 125–130. [Google Scholar]
- Cloward, R.B. The treatment of ruptured lumbar intervertebral discs by vertebral body fusion. I. Indications, operative technique, after care. J. Neurosurg. 1953, 10, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Harms, J.G.; Jeszenszky, D. Die posteriore, lumbale, interkorporelle Fusion in unilateraler transforaminaler Technik. Orthop. Traumatol. 1998, 10, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Fritzell, P.; Hägg, O.; Wessberg, P.; Nordwall, A.; Swedish Lumbar Spine Study Group. 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001, 26, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 2015, 1, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Karikari, I.O.; Isaacs, R.E. Minimally invasive transforaminal lumbar interbody fusion: A review of techniques and outcomes. Spine 2010, 35 (Suppl. S26), S294–S301. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.L.; Chen, L.H.; Niu, C.C.; Fu, T.S.; Chen, W.J. Relation between laminectomy and development of adjacent segment instability after lumbar fusion with pedicle fixation. Spine 2004, 29, 2527–2532. [Google Scholar] [CrossRef]
- Ekman, P.; Moller, H.; Shalabi, A.; Yu, Y.X.; Hedlund, R. A prospective randomised study on the long-term effect of lumbar fusion on adjacent disc degeneration. Eur. Spine J. 2009, 18, 1175–1186. [Google Scholar] [CrossRef]
- Wai, E.K.; Santos, E.R.; Morcom, R.A.; Fraser, R.D. Magnetic resonance imaging 20 years after anterior lumbar interbody fusion. Spine 2006, 31, 1952–1956. [Google Scholar] [CrossRef]
- Xia, X.P.; Chen, H.L.; Cheng, H.B. Prevalence of adjacent segment degeneration after spine surgery: A systematic review and meta-analysis. Spine 2013, 38, 597–608. [Google Scholar] [CrossRef]
- Nakashima, H.; Kawakami, N.; Tsuji, T.; Ohara, T.; Suzuki, Y.; Saito, T.; Nohara, A.; Tauchi, R.; Ohta, K.; Hamajima, N.; et al. Adjacent segment disease after posterior lumbar interbody fusion: Based on cases with a minimum of 10 years of follow-up. Spine 2015, 40, E831–E841. [Google Scholar] [CrossRef]
- Hilibrand, A.S.; Robbins, M. Adjacent segment degeneration and adjacent segment disease: The consequences of spinal fusion? Spine J. 2004, 4, 190S–194S. [Google Scholar] [CrossRef] [PubMed]
- Sears, W.R.; Sergides, I.G.; Kazemi, N.; Smith, M.; White, G.J.; Osburg, B. Incidence and prevalence of surgery at segments adjacent to a previous posterior lumbar arthrodesis. Spine J. 2011, 11, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Fassett, D.R.; Clark, R.; Brockmeyer, D.L.; Schmidt, M.H. Cervical spine deformity associated with resection of spinal cord tumors. Neurosurg. Focus 2006, 20, E2. [Google Scholar] [CrossRef] [PubMed]
- Albert, T.J.; Vacarro, A. Postlaminectomy kyphosis. Spine 1998, 23, 2738–2745. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.K.; Kim, Y.E.; Lim, T.H.; Weinstein, J.N. An analytical investigation of the mechanics of spinal instrumentation. Spine 1988, 13, 1003–1011. [Google Scholar] [CrossRef]
- Umehara, S.; Zindrick, M.R.; Patwardhan, A.G.; Havey, R.M.; Vrbos, L.A.; Knight, G.W.; Miyano, S.; Kirincic, M.; Kaneda, K.; Lorenz, M.A. The biomechanical effect of postoperative hypolordosis in instrumented lumbar fusion on instrumented and adjacent spinal segments. Spine 2000, 25, 1617–1624. [Google Scholar] [CrossRef]
- Chen, C.-S.; Feng, C.-K.; Cheng, C.-K.; Tzeng, M.-J.; Liu, C.-L.; Chen, W.-J. Biomechanical analysis of the disc adjacent to posterolateral fusion with laminectomy in lumbar spine. J. Spinal Disord. Tech. 2005, 18, 58–65. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials. 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S.; Ben Van Den, A. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2009. [Google Scholar]
- CEBM (Centre for Evidence-Based Medicine). Oxford Centre for Evidence-based Medicine—Levels of Evidence (March 2009). 2009. Available online: http://www.cebm.net/index.aspx?o=1025 (accessed on 28 December 2019).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wu, W.; Li, Y.; Liu, J.; Yang, K.; Chen, Y. Protective effects of preserving the posterior complex on the development of adjacent-segment degeneration after lumbar fusion. J. Neurosurg. Spine 2013, 19, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Huang, S.; Sun, J.; Li, F.; Sun, J.; Pi, G. Risk factors for upper adjacent segment degeneration after multi-level posterior lumbar spinal fusion surgery. J. Orthop. Surg. Res. 2019, 14, 89. [Google Scholar] [CrossRef]
- Kato, S.; Ganau, M.; Fehlings, M. Surgical decision-making in degenerative cervical myelopathy—Anterior versus posterior approach. J. Clin. Neurosci. 2018, 58, 7–12. [Google Scholar] [CrossRef]
- Lawrence, B.D.; Wang, J.; Arnold, P.M.; Hermsmeyer, J.; Norvell, D.C.; Brodke, D.S. Predicting the risk of adjacent segment pathology after lumbar fusion: A systematic review. Spine 2012, 37 (Suppl. S22), S123–S132. [Google Scholar] [CrossRef]
- Cheh, G.; Bridwell, K.H.; Lenke, L.G.; Buchowski, J.M.; Daubs, M.D.; Kim, Y.; Baldus, C. Adjacent segment disease following lumbar/thoracolumbar fusion with pedicle screw instrumentation: A minimum 5-year follow-up. Spine 2007, 32, 2253–2257. [Google Scholar] [CrossRef] [PubMed]
- Gillet, P. The fate of the adjacent motion segments after lumbar fusion. J. Spinal. Disord Tech. 2003, 16, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Bransford, R.J.; Bellabarba, C.; Chapman, J.R.; Cohen, A.M.; Harrington, R.M.; Ching, R.P. The effect of bilateral laminotomy versus laminectomy on the motion and stiffness of the human lumbar spine. Spine 2010, 35, 1789–1793. [Google Scholar] [CrossRef]
- Rao, R.D.; Wang, M.; Singhal, P.; McGrady, L.M.; Rao, S. Intradiscal pressure and kinematic behavior of lumbar spine after bilateral laminotomy and laminectomy. Spine J. 2002, 2, 320–326. [Google Scholar] [CrossRef]
- Huang, Y.-P.; Du, C.-F.; Cheng, C.-K.; Zhong, Z.-C.; Chen, X.-W.; Wu, G.; Li, Z.-C.; Ye, J.-D.; Lin, J.-H.; Wang, L.Z. Preserving posterior complex can prevent adjacent segment disease following posterior lumbar interbody fusion surgeries: A finite element analysis. PLoS ONE 2016, 11, e0166452. [Google Scholar] [CrossRef]
- Rothenfluh, D.A.; Mueller, D.A.; Rothenfluh, E.; Min, K. Pelvic incidence-lumbar lordosis mismatch predisposes to adjacent segment disease after lumbar spinal fusion. Eur. Spine J. 2015, 24, 1251. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, A.; Quattrocchi, C.C.; Scarciolla, L.; Papapietro, N.; Zobel, B.B.; Denaro, V. Estimating the risk for symptomatic adjacent segment degeneration after lumbar fusion: Analysis from a cohort of patients undergoing revision surgery. Eur. Spine J. 2014, 23, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Sim, H.B.; Murovic, J.A.; Cho, B.Y.; Lim, T.J.; Park, J. Biomechanical comparison of single-level posterior versus transforaminal lumbar interbody fusions with bilateral pedicle screw fixation: Segmental stability and the effects on adjacent motion segments. J. Neurosurg. Spine. 2010, 12, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Du, C.; Mo, Z.; Tian, S.; Wang, L.; Fan, J.; Liu, S.; Fan, Y. Biomechanical investigation of thoracolumbar spine in different postures during ejection using a combined finite element and multi-body approach. Int. J. Numer. Method Biomed. Eng. 2014, 30, 1121–1131. [Google Scholar] [CrossRef]
- Chen, L.-H.; Lai, P.-L.; Tai, C.-L.; Niu, C.-C.; Fu, T.-S.; Chen, W.-J. The effect of interspinous ligament integrity on adjacent segment instability after lumbar instrumentation and laminectomy—An experimental study in porcine model. Biomed. Mater. Eng. 2006, 16, 261–267. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Design Type | Number of Patients | Mean Age (Years) | Fusion Levels (Range/Mean) | Intervention | Follow-Up Time (Years) | ASDG (A vs. B) | Other Sagittal Parameters | ||
|---|---|---|---|---|---|---|---|---|---|---|
| No injury to PILC (A) | Injured PILC (B) | |||||||||
| Liu, 2013 [24] | Prospective RCT | 80 | 40 | 58 | L4–L5/1 | TLIF with PLF | 6 | 7 vs. 17 (p < 0.01) | >Loss of LL in group B (p < 0.05) | |
| Ma, 2019 [25] | Retrospective observational | 22 | 49 | 62 | T11–S1/1.8 | PLIF with PLF | 3 | 5 vs. 24 (p = 0.042) | >PI in group B (p = 0.042) | |
| Characteristic | TLIF Group (PILC Preserved) | L+TLIF Group (PILC Preserved) | CL+TLIF Group (PILC Injured) | p Value |
|---|---|---|---|---|
| Surgical technique | TLIF with PLF | TLIF with PLF | TLIF with PLF | |
| Number of patients | 40 | 40 | 40 | |
| Mean age of patients (y) | 58 | 58 | 58 | |
| Women:men ratio | 3 | 3 | 3 | |
| Fusion level | L4-L5 | L4-L5 | L4-L5 | |
| Follow-up (y) | 6 | 6 | 6 | |
| Number of patients with ASDG | 3 | 4 | 17 | 0.01 |
| Characteristic | PLIF Group (PILC Preserved) | L+PLIF Group (PILC Pesected) | p Value |
|---|---|---|---|
| Surgical technique | PLIF with PLF | PLIF with PLF | |
| Number of patients | 22 | 49 | |
| Mean age of patients (y) | 60.6 ± 9.0 | 63.0 ± 8.6 | 0.294 |
| Women:men ratio | 11:11 | 26:23 | 0.811 |
| Fusion levels | T11-S1 | T12-S1 | |
| Follow-up (y) | 3 | 3 | |
| Number of patients with ASDG | 5 | 24 | 0.042 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gondar, R.; Jesse, C.M.; Schär, R.T.; Fichtner, J.; Fung, C.; Raabe, A.; Ulrich, C.T. Preservation of the Posterior Interspinous Ligamentary Complex in Posterior and Transforaminal Lumbar Interbody Fusion. Surgeries 2023, 4, 600-610. https://doi.org/10.3390/surgeries4040058
Gondar R, Jesse CM, Schär RT, Fichtner J, Fung C, Raabe A, Ulrich CT. Preservation of the Posterior Interspinous Ligamentary Complex in Posterior and Transforaminal Lumbar Interbody Fusion. Surgeries. 2023; 4(4):600-610. https://doi.org/10.3390/surgeries4040058
Chicago/Turabian StyleGondar, Renato, Christopher Marvin Jesse, Ralph T. Schär, Jens Fichtner, Christian Fung, Andreas Raabe, and Christian T. Ulrich. 2023. "Preservation of the Posterior Interspinous Ligamentary Complex in Posterior and Transforaminal Lumbar Interbody Fusion" Surgeries 4, no. 4: 600-610. https://doi.org/10.3390/surgeries4040058