
Spatiotemporal Accessibility of COVID-19 Healthcare Facilities in Jakarta, Indonesia

 , , , , , ,
, , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
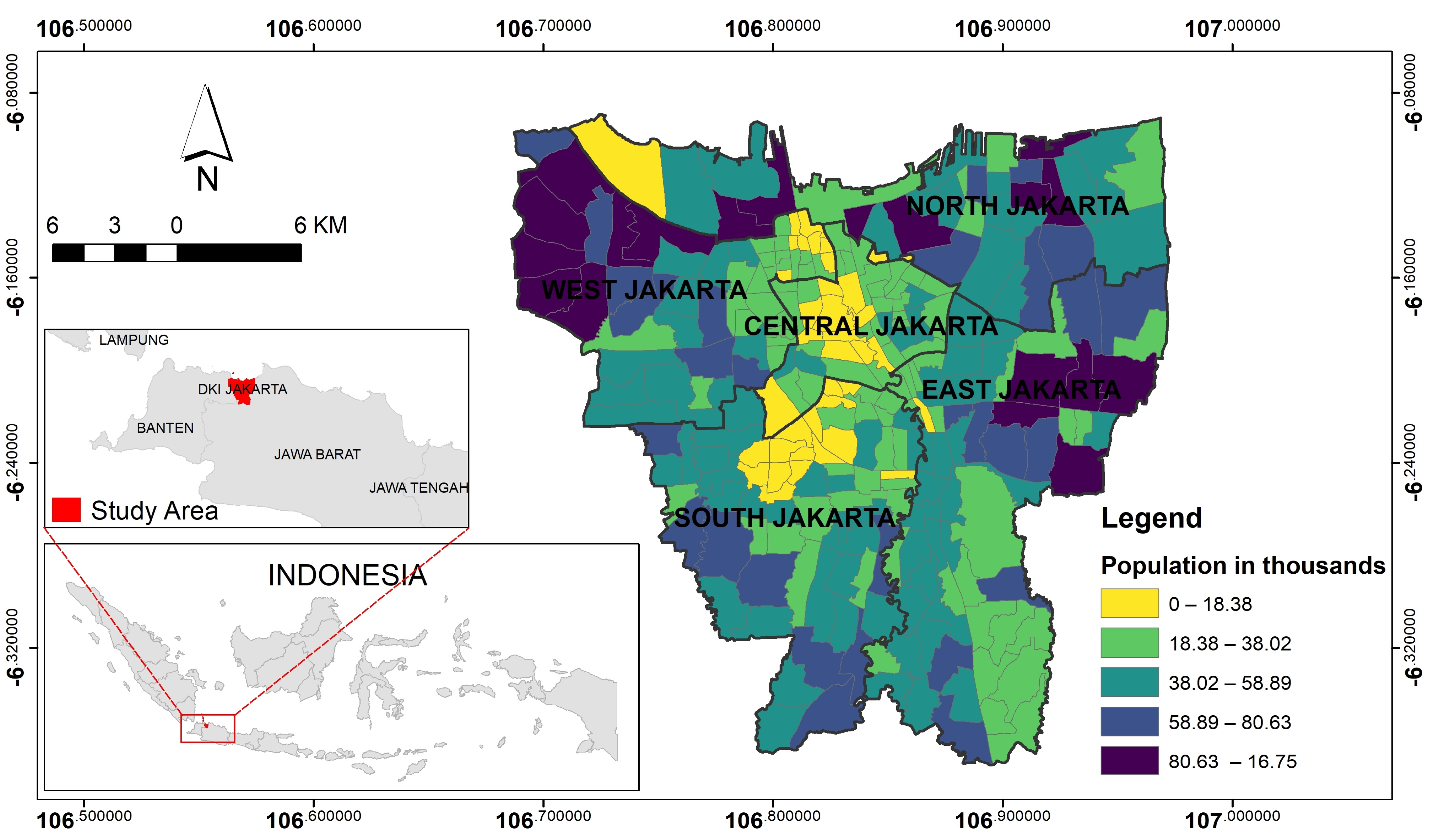
2.1. Study Area
2.2. Research Framework
2.2.1. Data Preparation
2.2.2. SFCA Analysis
2.2.3. Zonation of Accessibility and Spatial Disparity Analysis
3. Results
3.1. The First Year Period of COVID-19 Pandemic in Jakarta
3.2. COVID-19 Healthcare Services Dynamic
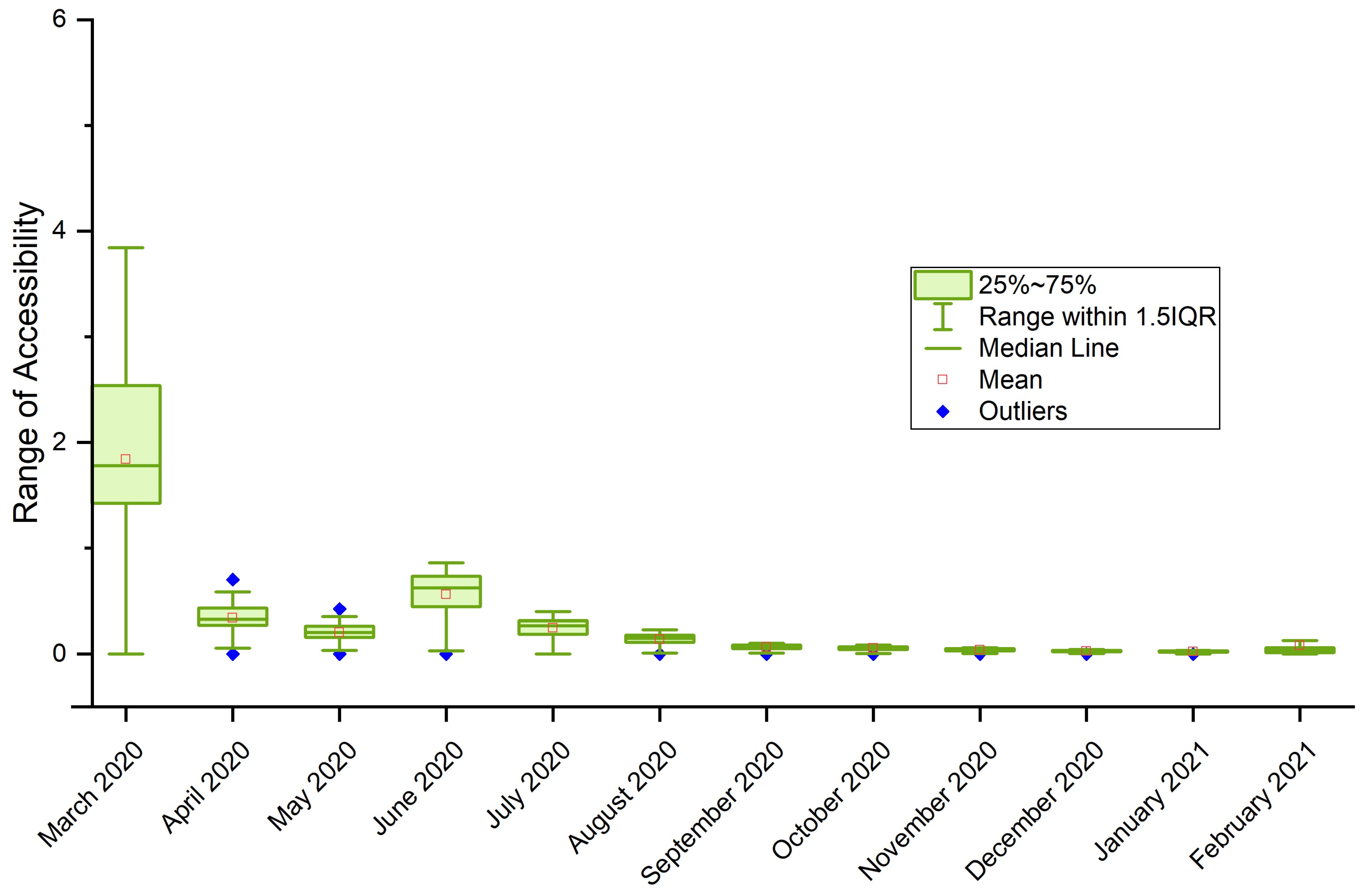
Spatiotemporal Dynamics of COVID-19 Healthcare Service Accessibility
3.3. Accessibility Clusters
4. Discussion and Future Works
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ciotti, M.; Angeletti, S.; Minieri, M.; Giovannetti, M.; Benvenuto, D.; Pascarella, S.; Sagnelli, C.; Bianchi, M.; Bernardini, S.; Ciccozzi, M. COVID-19 Outbreak: An Overview. CHE 2019, 64, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Hadibasyir, H.Z.; Rijal, S.S.; Sari, D.R. Comparison of Land Surface Temperature During and Before the Emergence of COVID-19 Using Modis Imagery in Wuhan City, China. Forum Geogr. 2020, 34, 1–15. [Google Scholar] [CrossRef]
- Permatasari, A.L.; Suherningtyas, I.A.; Febriarta, E.; Wiguna, P.P.K. Analysis of Vulnerability to Transmission of the COVID-19 Based on Building Function at Padukuhan Mancasan Kleben, Pandowoharjo, Sleman, Yogyakarta. Forum Geogr. 2022, 35, 169–178. [Google Scholar] [CrossRef]
- Hamzah, F.B.; Lau, C.; Nazri, H.; Ligot, D.V.; Lee, G.; Tan, C.L.; Shaib, M.; Zaidon, U.H.B.; Abdullah, A.B.; Chung, M.H. CoronaTracker: Worldwide COVID-19 Outbreak Data Analysis and Prediction. Bull. World Health Organ. 2020, 1, 1–32. [Google Scholar]
- WHO. COVID 19 Public Health Emergency of International Concern (PHEIC). Global Research and Innovation Forum: Towards a Research Roadmap; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The Positive Impact of Lockdown in Wuhan on Containing the COVID-19 Outbreak in China. J. Travel Med. 2020, 27, taaa037. [Google Scholar] [CrossRef] [Green Version]
- The Lancet. India under COVID-19 Lockdown. Lancet 2020, 395, 1315. [Google Scholar] [CrossRef]
- Pepe, E.; Bajardi, P.; Gauvin, L.; Privitera, F.; Lake, B.; Cattuto, C.; Tizzoni, M. COVID-19 Outbreak Response, a Dataset to Assess Mobility Changes in Italy Following National Lockdown. Sci. Data 2020, 7, 230. [Google Scholar] [CrossRef]
- Ghazali, M.F.; Tridawati, A.; Sugandi, M.; Anesta, A.F.; Wikantika, K. Spatial Analysis to Mitigate the Spread of COVID-19 Based on Regional Demographic Characteristics. Forum Geogr. 2021, 35, 57–73. [Google Scholar] [CrossRef]
- Grauer, J.; Löwen, H.; Liebchen, B. Strategic Spatiotemporal Vaccine Distribution Increases the Survival Rate in an Infectious Disease like COVID-19. Sci. Rep. 2020, 10, 21594. [Google Scholar] [CrossRef]
- Haque, A.; Pant, A.B. Efforts at COVID-19 Vaccine Development: Challenges and Successes. Vaccines 2020, 8, 739. [Google Scholar] [CrossRef] [PubMed]
- Qian, M.; Jiang, J. COVID-19 and Social Distancing. J. Public Health 2022, 30, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Tang, B.; Bragazzi, N.L.; Nah, K.; McCarthy, Z. Quantifying the Role of Social Distancing, Personal Protection and Case Detection in Mitigating COVID-19 Outbreak in Ontario, Canada. J. Math. Ind. 2020, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Amin, C.; Priyono, P.; Umrotun, U.; Fatkhiyah, M.; Sufahani, S.F. Exploring the Prevalence of Protective Measure Adoption in Mosques during the COVID-19 Pandemic in Indonesia. Sustainability 2021, 13, 13927. [Google Scholar] [CrossRef]
- Bahagia, B.; Hudayana, B.; Wibowo, R.; Anna, Z. Local Wisdom to Overcome COVID-19 Pandemic of Urug and Cipatat Kolot Societies in Bogor, West Java, Indonesia. Forum Geogr. 2020, 34, 146–160. [Google Scholar] [CrossRef]
- Nzediegwu, C.; Chang, S.X. Improper Solid Waste Management Increases Potential for COVID-19 Spread in Developing Countries. Resour. Conserv. Recycl. 2020, 161, 104947. [Google Scholar] [CrossRef]
- Purwanto, P.; Utaya, S.; Handoyo, B.; Bachri, S.; Astuti, I.S.; Utomo, K.S.B.; Aldianto, Y.E. Spatiotemporal Analysis of COVID-19 Spread with Emerging Hotspot Analysis and Space–Time Cube Models in East Java, Indonesia. ISPRS Int. J. Geo-Inf. 2021, 10, 133. [Google Scholar] [CrossRef]
- Saputra, A.; Setiawan, W.; Arif, M.; Sriyono; Nurmalasari, I.R.; Dijaya, R.; Ulinuha, A.; Hermawan, S. Non-Medical risk assessment of COVID-19 in parts of Central and East Java, Indonesia. Quaest. Geogr. 2022, 41, 147–169. [Google Scholar] [CrossRef]
- Jumadi, J.; Fikriyah, V.; Hadibasyir, H.; Priyono, K.; Musiyam, M.; Mardiah, A.; Rohman, A.; Hasyim, H. A Year Spatiotemporal Clusters of Covid-19 in Indonesia. Quaest. Geogr. 2022, 41, 139–151. [Google Scholar] [CrossRef]
- BPS Provinsi DKI Jakarta Dalam Angka 2021. Available online: https://jakarta.bps.go.id/publication/2021/02/26/bb7fa6dd5e90b534e3fa6984/provinsi-dki-jakarta-dalam-angka-2021.html (accessed on 30 March 2020).
- Ministry of Health Republic of Indonesia Media Informasi Resmi Terkini Penyakit Infeksi Emerging. Available online: https://infeksiemerging.kemkes.go.id/document/download/cover (accessed on 30 March 2020).
- Hierink, F.; Okiro, E.A.; Flahault, A.; Ray, N. The Winding Road to Health: A Systematic Scoping Review on the Effect of Geographical Accessibility to Health Care on Infectious Diseases in Low- and Middle-Income Countries. PLoS ONE 2021, 16, e0244921. [Google Scholar] [CrossRef]
- Ji, Y.; Ma, Z.; Peppelenbosch, M.P.; Pan, Q. Potential Association between COVID-19 Mortality and Health-Care Resource Availability. Lancet Glob. Health 2020, 8, e480. [Google Scholar] [CrossRef]
- Sun, Y.; Hu, X.; Xie, J. Spatial Inequalities of COVID-19 Mortality Rate in Relation to Socioeconomic and Environmental Factors across England. Sci. Total Environ. 2021, 758, 143595. [Google Scholar] [CrossRef] [PubMed]
- Nugraha, B.; Wahyuni, L.K.; Laswati, H.; Kusumastuti, P.; Tulaar, A.B.; Gutenbrunner, C. COVID-19 Pandemic in Indonesia: Situation and Challenges of Rehabilitation Medicine in Indonesia. Acta Med. Indones. 2020, 52, 299–305. [Google Scholar] [PubMed]
- Silalahi, F.E.S.; Hidayat, F.; Dewi, R.S.; Purwono, N.; Oktaviani, N. GIS-Based Approaches on the Accessibility of Referral Hospital Using Network Analysis and the Spatial Distribution Model of the Spreading Case of COVID-19 in Jakarta, Indonesia. BMC Health Serv. Res. 2020, 20, 1053. [Google Scholar] [CrossRef]
- Ghorbanzadeh, M.; Kim, K.; Erman Ozguven, E.; Horner, M.W. Spatial Accessibility Assessment of COVID-19 Patients to Healthcare Facilities: A Case Study of Florida. Travel Behav. Soc. 2021, 24, 95–101. [Google Scholar] [CrossRef]
- Kim, K.; Ghorbanzadeh, M.; Horner, M.W.; Ozguven, E.E. Identifying Areas of Potential Critical Healthcare Shortages: A Case Study of Spatial Accessibility to ICU Beds during the COVID-19 Pandemic in Florida. Transp. Policy 2021, 110, 478–486. [Google Scholar] [CrossRef]
- Kang, J.-Y.; Michels, A.; Lyu, F.; Wang, S.; Agbodo, N.; Freeman, V.L.; Wang, S. Rapidly Measuring Spatial Accessibility of COVID-19 Healthcare Resources: A Case Study of Illinois, USA. Int. J. Health Geogr. 2020, 19, 36. [Google Scholar] [CrossRef]
- Pereira, R.H.M.; Braga, C.K.V.; Servo, L.M.; Serra, B.; Amaral, P.; Gouveia, N.; Paez, A. Geographic Access to COVID-19 Healthcare in Brazil Using a Balanced Float Catchment Area Approach. Soc. Sci. Med. 2021, 273, 113773. [Google Scholar] [CrossRef]
- Zhou, Z.; Xu, Z.; Liu, A.; Zhou, S.; Mu, L.; Zhang, X. Mapping the Accessibility of Medical Facilities of Wuhan during the COVID-19 Pandemic. ISPRS Int. J. Geo-Inf. 2021, 10, 318. [Google Scholar] [CrossRef]
- Zheng, L.; Li, J.; Hu, W.; Duan, P. Analysis of the Spatial Range of Service and Accessibility of Hospitals Designated for Coronavirus Disease 2019 in Yunnan Province, China. Geocarto Int. 2022, 37, 6519–6537. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Yu, P.; Chen, Y.; Jing, Y.; Zeng, F. Accessibility of Park Green Space in Wuhan, China: Implications for Spatial Equity in the Post-COVID-19 Era. Int. J. Environ. Res. Public Health 2022, 19, 5440. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Luo, W. Supply-Demand Adjusted Two-Steps Floating Catchment Area (SDA-2SFCA) Model for Measuring Spatial Access to Health Care. Soc. Sci. Med. 2022, 296, 114727. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Fu, J.; Wang, H.; Zhao, Y.; Yi, T. Identifying Spatial Matching between the Supply and Demand of Medical Resource and Accessing Carrying Capacity: A Case Study of Shenzhen, China. Int. J. Environ. Res. Public Health 2022, 19, 2354. [Google Scholar] [CrossRef]
- Lotfata, A.; Tao, R.; Su, Y. Evaluating the Walking Accessibility of Cook County’s Public Schools to Use as Open Space. Int. J. Urban Sci. 2022, 1–18. [Google Scholar] [CrossRef]
- Radke, J.; Mu, L. Spatial Decompositions, Modeling and Mapping Service Regions to Predict Access to Social Programs. Geogr. Inf. Sci. 2000, 6, 105–112. [Google Scholar] [CrossRef]
- Pemerintah Provinsi DKI Jakarta. Open Data COVID-19 Provinsi DKI Jakarta. Available online: https://riwayat-file-covid-19-dki-jakarta-jakartagis.hub.arcgis.com (accessed on 30 March 2020).
- Daftar Rumah Sakit Rujukan. Available online: https://covid19.go.id/daftar-rumah-sakit-rujukan (accessed on 30 March 2020).
- Joseph, A.E.; Bantock, P.R. Measuring Potential Physical Accessibility to General Practitioners in Rural Areas: A Method and Case Study. Soc. Sci. Med. 1982, 16, 85–90. [Google Scholar] [CrossRef]
- Chen, X.; Jia, P. A Comparative Analysis of Accessibility Measures by the Two-Step Floating Catchment Area (2SFCA) Method. Int. J. Geogr. Inf. Sci. 2019, 33, 1739–1758. [Google Scholar] [CrossRef]
- Lee, R.C. Current Approaches to Shortage Area Designation. J. Rural. Health 1991, 7, 437–450. [Google Scholar]
- Multivariate Clustering (Spatial Statistics)—ArcGIS Pro | Documentation. Available online: https://pro.arcgis.com/en/pro-app/2.8/tool-reference/spatial-statistics/multivariate-clustering.htm (accessed on 2 September 2022).
- How Multivariate Clustering Works—ArcGIS Pro | Documentation. Available online: https://pro.arcgis.com/en/pro-app/2.8/tool-reference/spatial-statistics/how-multivariate-clustering-works.htm (accessed on 2 September 2022).
- STP COVID-19. Analisis Data COVID-19 Indonesia Update Per 3 Januari 2021. 2021. Available online: https://covid19.go.id/v/analisis-data-covid-19-indonesia-update-3-januari-2021 (accessed on 2 September 2022).
- KEPGUB NO. 1421/2021 PENETAPAN RUMAH SAKIT RUJUKAN PENANGGULANGAN PENYAKIT CORONAVIRUS DISEASE (COVID-19). Available online: https://jdih.jakarta.go.id/himpunan/produkhukum_detail/11255 (accessed on 29 May 2022).
- KEPGUB NO. 987/2021 PENETAPAN RUMAH SAKIT RUJUKAN PENANGGULANGAN PENYAKIT CORONAVIRUS DISEASE (COVID-19). Available online: https://jdih.jakarta.go.id/himpunan/produkhukum_detail/11070 (accessed on 29 May 2022).
- KEPGUB NO. 494/2020 PENETAPAN RUMAH SAKIT RUJUKAN PENANGGULANGAN PENYAKIT CORONAVIRUS DISEASE (COVID-19). Available online: https://jdih.jakarta.go.id/himpunan/produkhukum_detail/10199 (accessed on 29 May 2022).
- KEPGUB NO. 378/2020 PENETAPAN RUMAH SAKIT RUJUKAN PENANGGULANGAN PENYAKIT CORONAVIRUS DISEASE (COVID-19). Available online: https://jdih.jakarta.go.id/himpunan/produkhukum_detail/10200 (accessed on 29 May 2022).
- Sirkeci, I.; Yucesahin, M.M. Coronavirus and Migration: Analysis of Human Mobility and the Spread of COVID-19. Migr. Lett. 2020, 17, 379–398. [Google Scholar] [CrossRef] [Green Version]
- Gorbiano, M. BREAKING: Jokowi Announces Indonesia’s First Two Confirmed COVID-19 Cases—National—The Jakarta Post. Available online: https://www.thejakartapost.com/news/2020/03/02/breaking-jokowi-announces-indonesias-first-two-confirmed-covid-19-cases.html (accessed on 31 July 2021).
- Singh, L.K.; Tikka, S.K. Nondisrupted, Safety Ensured, Opioid Substitution Clinic in a COVID-19 Designated Hospital of a Resource-Limited State in India. Asia-Pac. Psychiatry 2021, 13, e12428. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Chen, H.; Zuo, C.; Zhang, N. The Impact of Traffic on Equality of Urban Healthcare Service Accessibility: A Case Study in Wuhan, China. Sustain. Cities Soc. 2022, 86, 104130. [Google Scholar] [CrossRef]
- Ni, J.; Liang, M.; Lin, Y.; Wu, Y.; Wang, C. Multi-Mode Two-Step Floating Catchment Area (2SFCA) Method to Measure the Potential Spatial Accessibility of Healthcare Services. ISPRS Int. J. Geo-Inf. 2019, 8, 236. [Google Scholar] [CrossRef] [Green Version]
- Gong, S.; Gao, Y.; Zhang, F.; Mu, L.; Kang, C.; Liu, Y. Evaluating Healthcare Resource Inequality in Beijing, China Based on an Improved Spatial Accessibility Measurement. Trans. GIS 2021, 25, 1504–1521. [Google Scholar] [CrossRef]
- Kim, Y.; Byon, Y.-J.; Yeo, H. Enhancing Healthcare Accessibility Measurements Using GIS: A Case Study in Seoul, Korea. PLoS ONE 2018, 13, e0193013. [Google Scholar] [CrossRef]
- Giarchi, G.G. Distance Decay and Information Deprivation: Health Implications for People in Rural Isolation. In New Directions in the Sociology of Health; Routledge: London, UK, 1990; ISBN 978-1-351-14172-7. [Google Scholar]
- Angka Testing Indonesia Per Juli 2021 Sudah 4 Kali Melampaui Standar WHO—Berita Terkini. Available online: https://covid19.go.id/p/berita/angka-testing-indonesia-juli-2021-sudah-4-kali-melampaui-standar-who (accessed on 4 September 2022).
- Sandi, F. Testing COVID-19 Turun & Tak Capai Target, Ini Kata Airlangga. Available online: https://www.cnbcindonesia.com/news/20210721203728-4-262616/testing-covid-19-turun-tak-capai-target-ini-kata-airlangga (accessed on 4 September 2022).
- Sehat Negeriku. Lonjakan Kasus COVID di Indonesia, Disebabkan Peningkatan Testing dan Tracing. 2022. Available online: https://sehatnegeriku.kemkes.go.id/baca/rilis-media/20220131/0639241/lonjakan-kasus-covid-di-indonesia-disebabkan-peningkatan-testing-dan-tracing/ (accessed on 4 September 2022).
- The Jakarta Post. Indonesia Ranks among World’s Worst in Coronavirus Testing Rate. Available online: https://www.thejakartapost.com/news/2020/04/07/indonesia-ranks-among-worlds-worst-in-coronavirus-testing-rate.html (accessed on 4 September 2022).









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jumadi, J.; Fikriyah, V.N.; Hadibasyir, H.Z.; Sunariya, M.I.T.; Priyono, K.D.; Setiyadi, N.A.; Carver, S.J.; Norman, P.D.; Malleson, N.S.; Rohman, A.; et al. Spatiotemporal Accessibility of COVID-19 Healthcare Facilities in Jakarta, Indonesia. Sustainability 2022, 14, 14478. https://doi.org/10.3390/su142114478
Jumadi J, Fikriyah VN, Hadibasyir HZ, Sunariya MIT, Priyono KD, Setiyadi NA, Carver SJ, Norman PD, Malleson NS, Rohman A, et al. Spatiotemporal Accessibility of COVID-19 Healthcare Facilities in Jakarta, Indonesia. Sustainability. 2022; 14(21):14478. https://doi.org/10.3390/su142114478
Chicago/Turabian StyleJumadi, Jumadi, Vidya N. Fikriyah, Hamim Z. Hadibasyir, Muhammad I. T. Sunariya, Kuswaji D. Priyono, Noor A. Setiyadi, Steve J. Carver, Paul D. Norman, Nick S. Malleson, Arif Rohman, and et al. 2022. "Spatiotemporal Accessibility of COVID-19 Healthcare Facilities in Jakarta, Indonesia" Sustainability 14, no. 21: 14478. https://doi.org/10.3390/su142114478