Whole-Body Vibration as Antihypertensive Non-Pharmacological Treatment in Hypertensive Individuals with Knee Osteoarthritis: Randomized Cross-Over Trial


 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
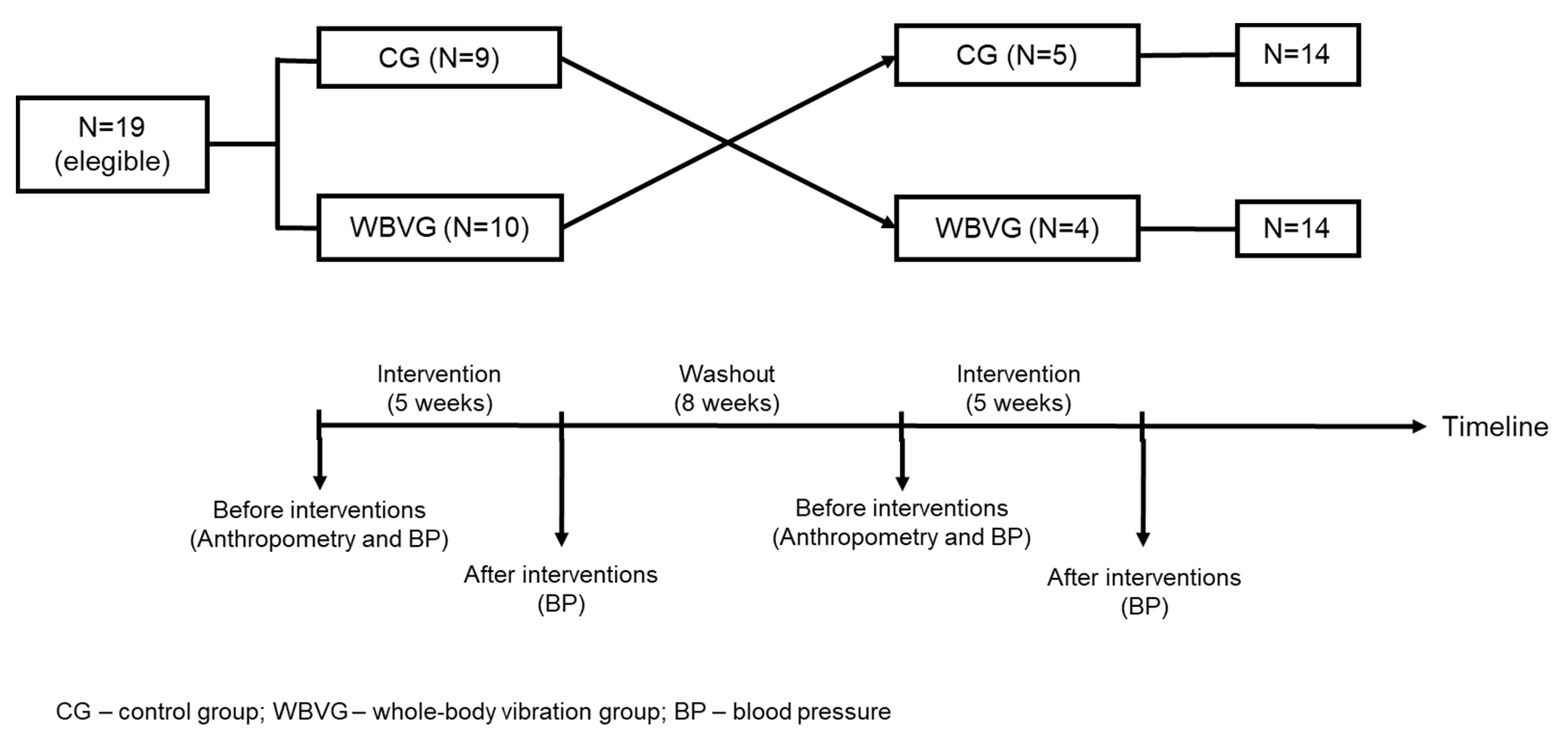
2.2. Study Design
2.3. Anthropometry and BP
2.4. Whole-Body Vibration Intervention
2.5. Statistical Analysis
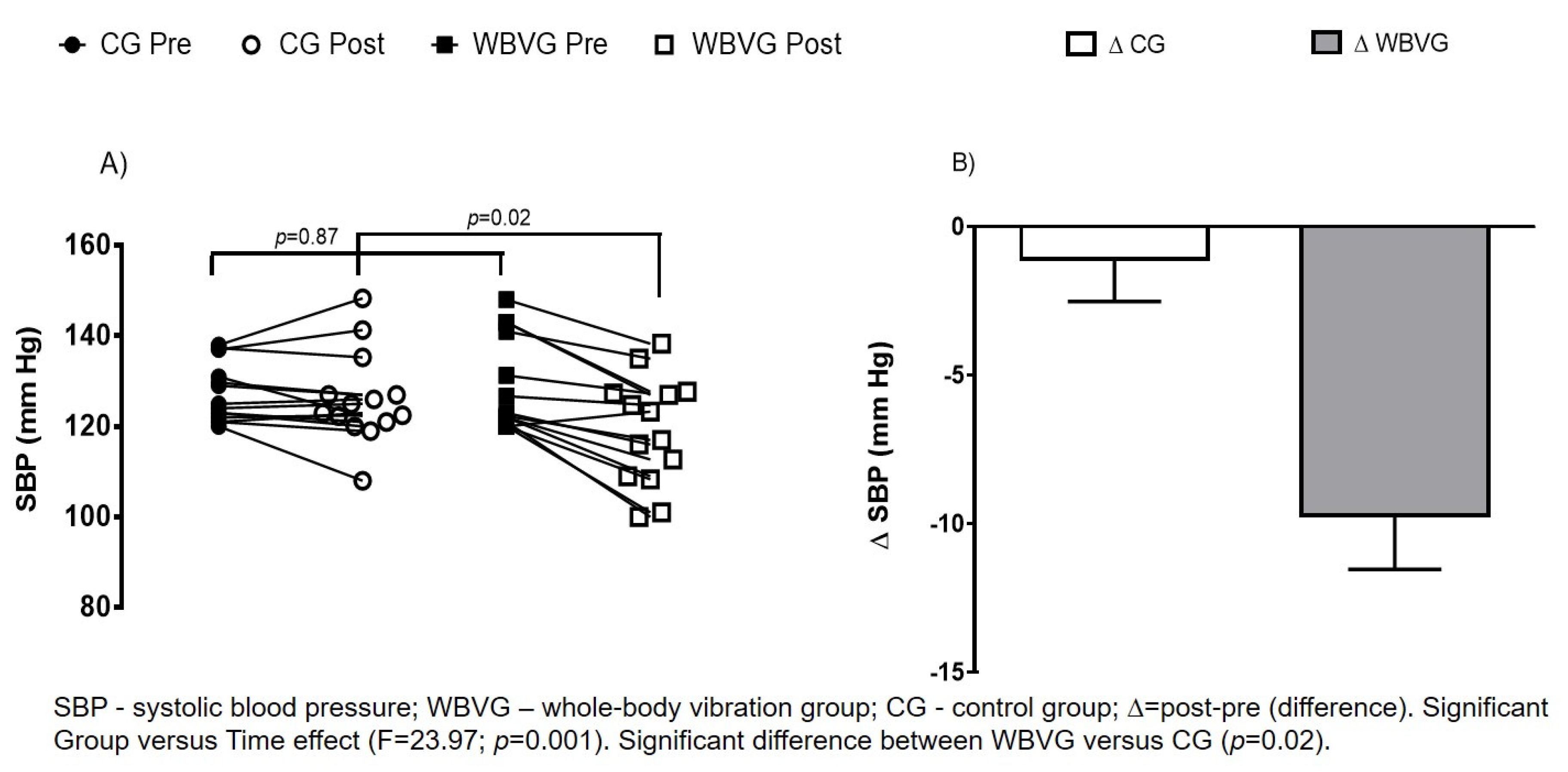
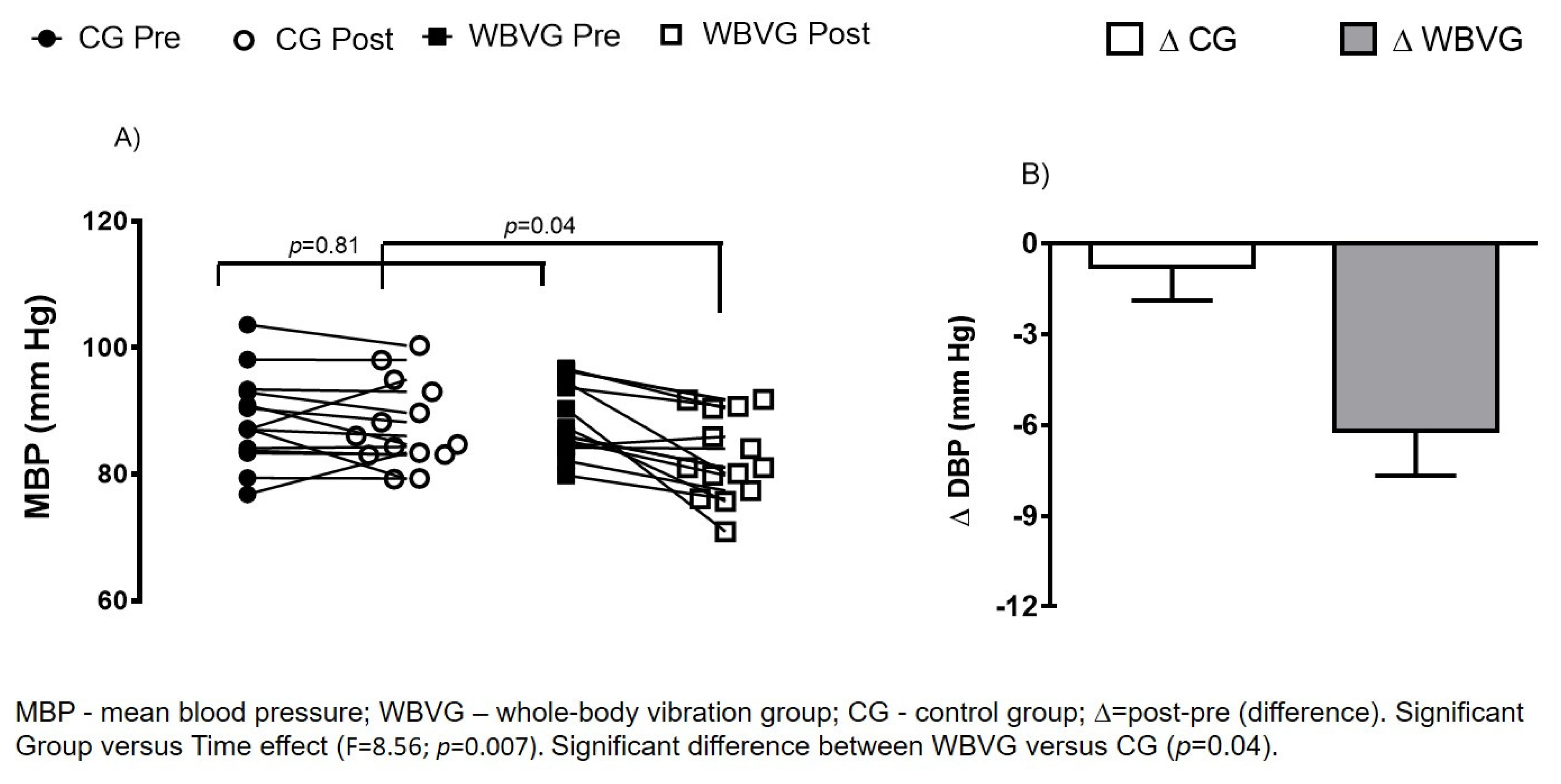
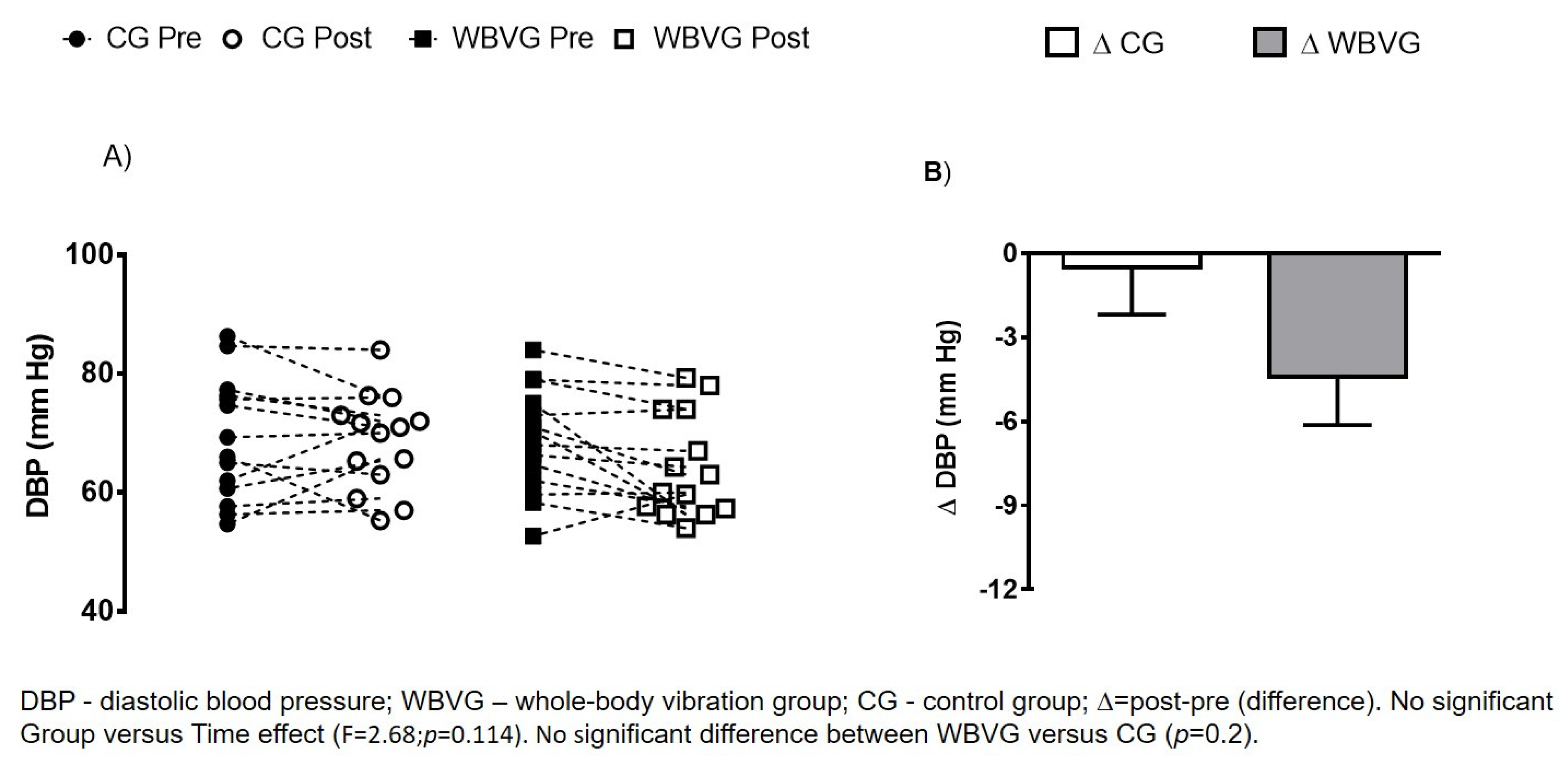
3. Results
4. Discussion
4.1. Blood Pressure and Whole-Body Vibration
4.2. Association between Hypertension and Knee Osteoarthritis
4.3. Possible Mechanisms of the Whole-Body Vibration to Reduce Blood Pressure
4.4. Limitations of Study
4.5. Strength of Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organisation (WHO) Hypertension. Available online: https://www.who.int/health-topics/hypertension/#tab=tab_1 (accessed on 17 April 2020).
- Veronese, N.; Stubbs, B.; Solmi, M.; Smith, T.O.; Noale, M.; Schofield, P.; Maggi, S. Knee Osteoarthritis and Risk of Hypertension: A Longitudinal Cohort Study. Rejuvenation Res. 2018, 21, 15–21. [Google Scholar] [CrossRef]
- Cheung, B.M.Y.; Li, C. Diabetes and Hypertension: Is There a Common Metabolic Pathway? Curr. Atheroscler. Rep. 2012, 14, 160–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulè, G. Metabolic syndrome in hypertensive patients: An unholy alliance. World J. Cardiol. 2014, 6, 890. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.-Z.; Lu, W.; Zong, X.-F.; Ruan, H.-Y.; Liu, Y. Obesity and hypertension. Exp. Ther. Med. 2016, 12, 2395–2399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, W.H.; Lepus, C.M.; Wang, Q.; Raghu, H.; Mao, R.; Lindstrom, T.M.; Sokolove, J. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 580–592. [Google Scholar] [CrossRef]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.; Yang, S.; Kwon, S.; Choi, K.; Kim, W. Association between metabolic syndrome and knee osteoarthritis: A cross-sectional Nationwide survey study. J. Rehabil. Med. 2019, 51, 464–470. [Google Scholar] [CrossRef]
- Khan, B.; Khan, O.Y.; Zehra, S.; Azhar, A.; Fatima, S. Association between obesity and risk of knee osteoarthritis. Pak. J. Pharm. Sci. 2020, 33, 295–298. [Google Scholar]
- Kim, H.S.; Shin, J.-S.; Lee, J.; Lee, Y.J.; Kim, M.; Bae, Y.-H.; Park, K.B.; Lee, E.-J.; Kim, J.-H.; Ha, I.-H. Association between Knee Osteoarthritis, Cardiovascular Risk Factors, and the Framingham Risk Score in South Koreans: A Cross-Sectional Study. PLoS ONE 2016, 11, e0165325. [Google Scholar] [CrossRef]
- Liu, Q.; Niu, J.; Huang, J.; Ke, Y.; Tang, X.; Wu, X.; Li, R.; Li, H.; Zhi, X.; Wang, K.; et al. Knee osteoarthritis and all-cause mortality: The Wuchuan Osteoarthritis Study. Osteoarthr. Cartil. 2015, 23, 1154–1157. [Google Scholar] [CrossRef] [Green Version]
- DongXing, X.; Jie, W.; Chao, Z.; Tuo, Y.; Hui, L.; YiLun, W.; HuiZhong, L.; ZiYing, W.; YuXuan, Q.; KangHua, L.; et al. Association between metabolic syndrome and knee osteoarthritis: A cross-sectional study. BMC Musculoskelet. Disord. 2017, 18. [Google Scholar] [CrossRef] [Green Version]
- Nielen, M.M.J.; Van Sijl, A.M.; Peters, M.J.L.; Verheij, R.A.; Schellevis, F.G.; Nurmohamed, M.T. Cardiovascular disease prevalence in patients with inflammatory arthritis, diabetes mellitus and osteoarthritis: A cross-sectional study in primary care. BMC Musculoskelet. Disord. 2012, 13, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawker, G.A.; Croxford, R.; Bierman, A.S.; Harvey, P.; Ravi, B.; Kendzerska, T.; Stanaitis, I.; King, L.K.; Lipscombe, L. Osteoarthritis-related difficulty walking and risk for diabetes complications. Osteoarthr. Cartil. 2017, 25, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohn, M.W.; Manheim, L.M.; Chang, R.W.; Greenland, P.; Hochberg, M.C.; Nevitt, M.C.; Semanik, P.A.; Dunlop, D.D. Sedentary behavior and blood pressure control among osteoarthritis initiative participants. Osteoarthr. Cartil. 2014, 22, 1234–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, S.-M.; Hadadi, E.; Dang, T.-M.; Yeap, W.-H.; Tan, C.T.-Y.; Ng, T.-P.; Larbi, A.; Wong, S.-C. The pro-inflammatory phenotype of the human non-classical monocyte subset is attributed to senescence. Cell Death Dis. 2018, 9, 266. [Google Scholar] [CrossRef]
- Nakayama, H.; Otsu, K. Mitochondrial DNA as an inflammatory mediator in cardiovascular diseases. Biochem. J. 2018, 475, 839–852. [Google Scholar] [CrossRef]
- Radojčić, M.R.; Thudium, C.S.; Henriksen, K.; Tan, K.; Karlsten, R.; Dudley, A.; Chessell, I.; Karsdal, M.A.; Bay-Jensen, A.-C.; Crema, M.D.; et al. Biomarker of extracellular matrix remodelling C1M and proinflammatory cytokine interleukin 6 are related to synovitis and pain in end-stage knee osteoarthritis patients. Pain 2017, 158, 1254–1263. [Google Scholar] [CrossRef] [Green Version]
- Lacolley, P.; Regnault, V.; Avolio, A.P. Smooth muscle cell and arterial aging: Basic and clinical aspects. Cardiovasc. Res. 2018, 114, 513–528. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Binnekade, T.T.; Soundy, A.; Schofield, P.; Huijnen, I.P.J.; Eggermont, L.H.P. Are Older Adults with Chronic Musculoskeletal Pain Less Active than Older Adults Without Pain? A Systematic Review and Meta-Analysis. Pain Med. 2013, 14, 1316–1331. [Google Scholar] [CrossRef] [Green Version]
- Bergler-Klein, J. What’s new in the ESC 2018 guidelines for arterial hypertension. Wien. Klin. Wochenschr. 2019, 131, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Crawford, S.E.; Hartung, T.; Hollert, H.; Mathes, B.; van Ravenzwaay, B.; Steger-Hartmann, T.; Studer, C.; Krug, H.F. Green Toxicology: A strategy for sustainable chemical and material development. Environ. Sci. Eur. 2017, 29, 16. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, N.; Sapienza, D.; Guerrero, R.; Aekplakorn, W.; Naghavi, M.; Mokdad, A.H.; Lozano, R.; Murray, C.J.; Lim, S.S. Control of hypertension with medication: A comparative analysis of national surveys in 20 countries. Bull. World Health Organ. 2014, 92, 10–19C. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S. Prescription of exercise training for hypertensives. Hypertens. Res. 2020, 43, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Gil, R.; Wong, A.; Hooshmand, S.; Park, S.Y.; Vicil, F.; Sanchez-Gonzalez, M.A. Whole-body vibration training reduces arterial stiffness, blood pressure and sympathovagal balance in young overweight/obese women. Hypertens. Res. 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, Z.; Wang, X.; Lee, S.; Hou, X.; Wang, L. Effects of whole body vibration exercise on neuromuscular function for individuals with knee osteoarthritis: Study protocol for a randomized controlled trial. Trials 2017, 18, 437. [Google Scholar] [CrossRef] [Green Version]
- Newberry, S.J.; FitzGerald, J.; SooHoo, N.F. Treatment of Osteoarthritis of the Knee: An Update Review. Comp. Eff. Rev. 2017, 190. [Google Scholar] [CrossRef]
- Wang, P.; Yang, L.; Li, H.; Lei, Z.; Yang, X.; Liu, C.; Jiang, H.; Zhang, L.; Zhou, Z.; Reinhardt, J.D.; et al. Effects of whole-body vibration training with quadriceps strengthening exercise on functioning and gait parameters in patients with medial compartment knee osteoarthritis: A randomised controlled preliminary study. Physiotherapy 2016, 102, 86–92. [Google Scholar] [CrossRef]
- Beck, B.R.; Norling, T.L. The Effect of 8 Mos of Twice-Weekly Low- or Higher Intensity Whole Body Vibration on Risk Factors for Postmenopausal Hip Fracture. Am. J. Phys. Med. Rehabil. 2010. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, A.; Kalfon, R.; Wong, A. Whole-body vibration training decreases ankle systolic blood pressure and leg arterial stiffness in obese postmenopausal women with high blood pressure. Menopause 2015. [Google Scholar] [CrossRef]
- Alvarez-Alvarado, S.; Jaime, S.J.; Ormsbee, M.J.; Campbell, J.C.; Post, J.; Pacilio, J.; Figueroa, A. Benefits of whole-body vibration training on arterial function and muscle strength in young overweight/obese women. Hypertens. Res. 2017, 40, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Lage, V.K.S.; Lacerda, A.C.R.; Neves, C.D.C.; Chaves, M.G.A.; Soares, A.A.; Lima, L.P.; Matos, M.A.; Leite, H.R.; Fernandes, J.S.C.; Oliveira, V.C.; et al. Cardiorespiratory responses in different types of squats and frequencies of whole body vibration in patients with chronic obstructive pulmonary disease. J. Appl. Physiol. 2018, 126, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Ahlback, S. Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol Diagn 1968, 77, 7–72. [Google Scholar] [CrossRef] [Green Version]
- Silva Júnior, O.D.M.; Ohashi, B.D.N.; De Almeida, M.O.; Gonçalves, M.R. Resultado funcional relacionado ao posicionamento do enxerto na reconstrução do ligamento cruzado anterior. Rev. Bras. Ortop. 2015, 50, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Dwan, K.; Li, T.; Altman, D.G.; Elbourne, D. CONSORT 2010 statement: Extension to randomised crossover trials. BMJ 2019, l4378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiroshige, K.; Mahbub, M.H.; Harada, N. Effects of whole-body vibration on postural balance and proprioception in healthy young and elderly subjects: A randomized cross-over study. J. Sports Med. Phys. Fitness 2014, 54, 216–224. [Google Scholar]
- Brzezinski, W. Blood Pressure. In Clinical Methods: The History, Physical, and Laboratory Examinations.; Walkr, H., Hall, W., Hurst, J., Eds.; Butterworths: Boston, MA, USA, 1990. [Google Scholar]
- Neto, S.B.; Marconi, E.M.; Kutter, C.R.; Frederico, E.H.; de Paiva, P.D.; Meyer, P.F.; Chang, S.; Sá-Caputo, D.; Bernardo-Filho, M. Beneficial effects of whole body mechanical vibration alone or combined with auriculotherapy in the pain and in flexion of knee of individuals with knee osteoarthritis. Acupunct. Electrother. Res. 2017, 42, 185–201. [Google Scholar] [CrossRef]
- Ribeiro Kütter, C.; Moreira-Marconi, E.; Teixeira-Silva, Y.; Cristina Moura-Fernandes, M.; Gonçalves de Meirelles, A.; José dos Santos Pereira, M.; Chang, S.; Alexandre Bachur, J.; Liane Paineiras-Domingos, L.; Taiar, R.; et al. Effects of the whole-body vibration and auriculotherapy on the functionality of knee osteoarthritis individuals. Appl. Sci. 2019, 9, 5194. [Google Scholar] [CrossRef] [Green Version]
- Moura-Fernandes, M.C.; Moreira-Marconi, E.; Gonçalves de Meirelles, A.; Paula Ferreira de Oliveira, A.; Silva, A.R.; Felipe Ferreira de Souza, L.; Lírio Pereira da Silva, A.; dos Santos-Fernandes, C.; Bessa Monteiro de Oliveira, B.; Antonio de Souza Gama, M.; et al. Effect of the Combined Intervention with Passive Whole-Body Vibration and Auriculotherapy on the Quality of Life of Individuals with Knee Osteoarthritis Assessed by the WHOQOL-Bref: A Multi-Arm Clinical Trial. Appl. Sci. 2020, 10, 1956. [Google Scholar] [CrossRef] [Green Version]
- Moreira-marconi, E.; Dionello, C.F.; Morel, D.S.; Sá-caputo, D.C.; Sousa-gonçalves, C.R.; José, M.; Bernardo-filho, M. Whole body vibration and auriculotherapy improve handgrip strength in individuals with knee osteoarthritis. J. Tradit. Chin. Med. 2019, 39, 707–715. [Google Scholar]
- Figueroa, A.; Kalfon, R.; Madzima, T.A.; Wong, A. Effects of whole-body vibration exercise training on aortic wave reflection and muscle strength in postmenopausal women with prehypertension and hypertension. J. Hum. Hypertens. 2013, 28, 118. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Kalfon, R.; Madzima, T.A.; Wong, A. Whole-body vibration exercise training reduces arterial stiffness in postmenopausal women with prehypertension and hypertension. Menopause 2014, 21, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Malachias, M.; Souza, W.; Plavnik, F.; Rodrigues, C.; Brandão, A.; Neves, M.; Bortolotto, L.; Franco, R.; Figueiredo, C.; Jardim, P.; et al. 7th Brazilian Guideline of arterial hypertension. Arq. Bras. Cardiol. 2016, 107, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Alvarez-Alvarado, S.; Jaime, S.J.; Kinsey, A.W.; Spicer, M.T.; Madzima, T.A.; Figueroa, A. Combined whole-body vibration training and l-citrulline supplementation improves pressure wave reflection in obese postmenopausal women. Appl. Physiol. Nutr. Metab. 2015, 41, 292–297. [Google Scholar] [CrossRef]
- Wong, A.; Alvarez-Alvarado, S.; Kinsey, A.W.; Figueroa, A. Whole-Body Vibration Exercise Therapy Improves Cardiac Autonomic Function and Blood Pressure in Obese Pre- and Stage 1 Hypertensive Postmenopausal Women. J. Altern. Complement. Med. 2016, 22, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Clifford, P.S.; Hellsten, Y. Vasodilatory mechanisms in contracting skeletal muscle. J. Appl. Physiol. 2004, 97, 393–403. [Google Scholar] [CrossRef]
- Manimmanakorn, N.; Manimmanakorn, A.; Phuttharak, W.; Hamlin, M.J. Effects of Whole Body Vibration on Glycemic Indices and Peripheral Blood Flow in Type II Diabetic Patients. Malaysian J. Med. Sci. 2017, 24, 55–63. [Google Scholar] [CrossRef]
- Beijer, Å.; Rosenberger, A.; Weber, T.; Zange, J.; May, F.; Schoenau, E.; Mester, J.; Bloch, W.; Rittweger, J. Randomized controlled study on resistive vibration exercise (EVE study): Protocol, implementation and feasibility. J. Musculoskelet. Neuronal Interact. 2013, 13, 147–156. [Google Scholar]
- Saccò, M.; Meschi, M.; Regolisti, G.; Detrenis, S.; Bianchi, L.; Bertorelli, M.; Pioli, S.; Magnano, A.; Spagnoli, F.; Giuri, P.G.; et al. The relationship between blood pressure and pain. J. Clin. Hypertens. 2013, 15, 600–605. [Google Scholar] [CrossRef]
- Bruehl, S.; Olsen, R.B.; Tronstad, C.; Sevre, K.; Burns, J.W.; Schirmer, H.; Nielsen, C.S.; Stubhaug, A.; Rosseland, L.A. Chronic pain-related changes in cardiovascular regulation and impact on comorbid hypertension in a general population: The Tromsø study. Pain 2018, 159, 119–127. [Google Scholar] [CrossRef]
- Rissardi, G.D.; Cipullo, J.P.; Moreira, G.C.; Ciorlia, L.A.; Cesarino, C.B.; Giollo Junior, L.T.; Zanesco, A.; Vilela-Martin, J.F. Prevalence of Physical Inactivity and its Effects on Blood Pressure and Metabolic Parameters in a Brazilian Urban Population. Int. J. Cardiovasc. Sci. 2018, 31, 594–602. [Google Scholar] [CrossRef]
- De Miguel, C.; Rudemiller, N.P.; Abais, J.M.; Mattson, D.L. Inflammation and Hypertension: New Understandings and Potential Therapeutic Targets. Curr. Hypertens. Rep. 2014, 17, 507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartoloni, E.; Alunno, A.; Valentini, V.; Luccioli, F.; Valentini, E.; La Paglia, G.; Bistoni, O.; Gerli, R. Role of Inflammatory Diseases in Hypertension. High Blood Press. Cardiovasc. Prev. 2017, 24, 353–361. [Google Scholar] [CrossRef]
- Aljadhey, H.; Tu, W.; Hansen, R.A.; Blalock, S.J.; Brater, D.C.; Murray, M.D. Comparative effects of non-steroidal anti-inflammatory drugs (NSAIDs) on blood pressure in patients with hypertension. BMC Cardiovasc. Disord. 2012, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zafar, H.; Alghadir, A.; Anwer, S.; Al-Eisa, E. Therapeutic Effects of Whole-Body Vibration Training in Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehab 2015, 96, 1525–1532. [Google Scholar] [CrossRef] [PubMed]
- Simão, A.P.; Avelar, N.C.; Tossige-Gomes, R.; Neves, C.D.; Mendonça, V.A.; Miranda, A.S.; Teixeira, M.M.; Teixeira, A.L.; Andrade, A.P.; Coimbra, C.C.; et al. Functional performance and inflammatory cytokines after squat exercises and whole-body vibration in elderly individuals with knee osteoarthritis. Arch. Phys. Med. Rehabil. 2012, 93, 1692–1700. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Yang, X.; Yang, Y.; Yang, L.; Zhou, Y.; Liu, C.; Reinhardt, J.D.; He, C. Effects of whole body vibration on pain, stiffness and physical functions in patients with knee osteoarthritis: A systematic review and meta-analysis. Clin. Rehabil. 2015, 29, 939–951. [Google Scholar] [CrossRef]
- Wong, A.; Sanchez-Gonzalez, M.A.; Gil, R.; Vicil, F.; Park, S.Y.; Figueroa, A. Passive vibration on the legs reduces peripheral and systemic arterial stiffness. Hypertens. Res. 2012, 35, 126–127. [Google Scholar] [CrossRef]
- Lohman, E.B.; Petrofsky, J.S.; Maloney-Hinds, C.; Betts-Schwab, H.; Thorpe, D. The effect of whole body vibration on lower extremity skin blood flow in normal subjects. Med. Sci. Monit. 2007, 13, CR71–CR76. [Google Scholar] [CrossRef]
- Sanchez-Gonzalez, M.A.; Wong, A.; Vicil, F.; Gil, R.; Park, S.Y.; Figueroa, A. Impact of passive vibration on pressure pulse wave characteristics. J. Hum. Hypertens. 2012, 26, 610–615. [Google Scholar] [CrossRef] [Green Version]
- Maloney-Hinds, C.; Petrofsky, J.S.; Zimmerman, G.; Hessinger, D.A. The Role of Nitric Oxide in Skin Blood Flow Increases Due to Vibration in Healthy Adults and Adults with Type 2 Diabetes. Diabetes Technol. Ther. 2009, 11, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Okazawa, T.; Nagase, H.; Yoshida, M.; Arüzumi, M.; Okada, A. Change in digital blood flow with simultaneous reduction in plasma endothelin induced by hand-arm vibration. Int. Arch. Occup. Environ. Health 1996, 68, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Charkoudian, N.; Wallin, B.G. Sympathetic Nervous System and Blood Pressure in Humans. Hypertension 2010, 56, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, G.K.; Pal, P.; Nanda, N.; Lalitha, V.; Dutta, T.K.; Adithan, C. Sympathovagal Imbalance in Prehypertensive Offspring of Two Parents versus One Parent Hypertensive. Int. J. Hypertens. 2011, 2011, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control Group (CG) n = 14 (2 M and 12 F) | Vibration Group (WBVG) n = 14 (2 M and 12 F) | Independent T-Test |
|---|---|---|---|
| Age (year) | 64.1 ± 3.3 | 67.1 ± 2.8 | 0.518 |
| Body mass (kg) | 82.8 ± 2.8 | 86.8 ± 3.8 | 0.642 |
| Stature (cm) | 160.8 ± 0.1 | 160.8 ± 0.2 | 0.431 |
| BMI (kg/m2) | 33.2 ± 1.6 | 35.2 ± 2.0 | 0.428 |
| IKDC score | 26.14 ± 2.36 | 29.45 ± 2.51 | 0.349 |
| SBP (mmHg) | 127.2 ± 1.7 | 128.3 ± 2.7 | 0.871 |
| DBP (mmHg) | 69.0 ± 2.7 | 68.7 ± 2.3 | 0.881 |
| MBP (mmHg) | 88.4 ± 1.9 | 88.7 ± 1.5 | 0.943 |
| Medications | Chi-Square Test | ||
| Diuretic + AT1 blocker or ACE inhibitor | 3 | 5 | 0.50 |
| AT1 blocker | 6 | 6 | 0.64 |
| ACE inhibitor | 2 | 1 | 0.54 |
| Beta-1 blocker | 2 | 1 | 0.54 |
| Calcium blocker | 2 | 2 | 0.70 |
| Metformin | 2 | 1 | 0.54 |
| Statins | 3 | 4 | 0.66 |
| SAIDs | 2 | 3 | 0.62 |
| Chondroitin sulphate | 1 | 1 | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira-Marconi, E.; Caiado, V.d.S.; Teixeira-Silva, Y.; Meirelles, A.G.d.; Moura-Fernandes, M.C.; Lopes-Souza, P.; Reis-Silva, A.; Sá-Caputo, D.C.; Paineiras-Domingos, L.L.; Lacerda, A.C.R.; et al. Whole-Body Vibration as Antihypertensive Non-Pharmacological Treatment in Hypertensive Individuals with Knee Osteoarthritis: Randomized Cross-Over Trial. Sustainability 2020, 12, 8944. https://doi.org/10.3390/su12218944
Moreira-Marconi E, Caiado VdS, Teixeira-Silva Y, Meirelles AGd, Moura-Fernandes MC, Lopes-Souza P, Reis-Silva A, Sá-Caputo DC, Paineiras-Domingos LL, Lacerda ACR, et al. Whole-Body Vibration as Antihypertensive Non-Pharmacological Treatment in Hypertensive Individuals with Knee Osteoarthritis: Randomized Cross-Over Trial. Sustainability. 2020; 12(21):8944. https://doi.org/10.3390/su12218944
Chicago/Turabian StyleMoreira-Marconi, Eloá, Vanessa da Silva Caiado, Ygor Teixeira-Silva, Alexandre Gonçalves de Meirelles, Marcia Cristina Moura-Fernandes, Patrícia Lopes-Souza, Aline Reis-Silva, Danúbia C. Sá-Caputo, Laisa L. Paineiras-Domingos, Ana Cristina Rodrigues Lacerda, and et al. 2020. "Whole-Body Vibration as Antihypertensive Non-Pharmacological Treatment in Hypertensive Individuals with Knee Osteoarthritis: Randomized Cross-Over Trial" Sustainability 12, no. 21: 8944. https://doi.org/10.3390/su12218944