
Does the Score on the MRC Strength Scale Reflect Instrumented Measures of Maximal Torque and Muscle Activity in Post-Stroke Survivors?

 , , ,
, , , 
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
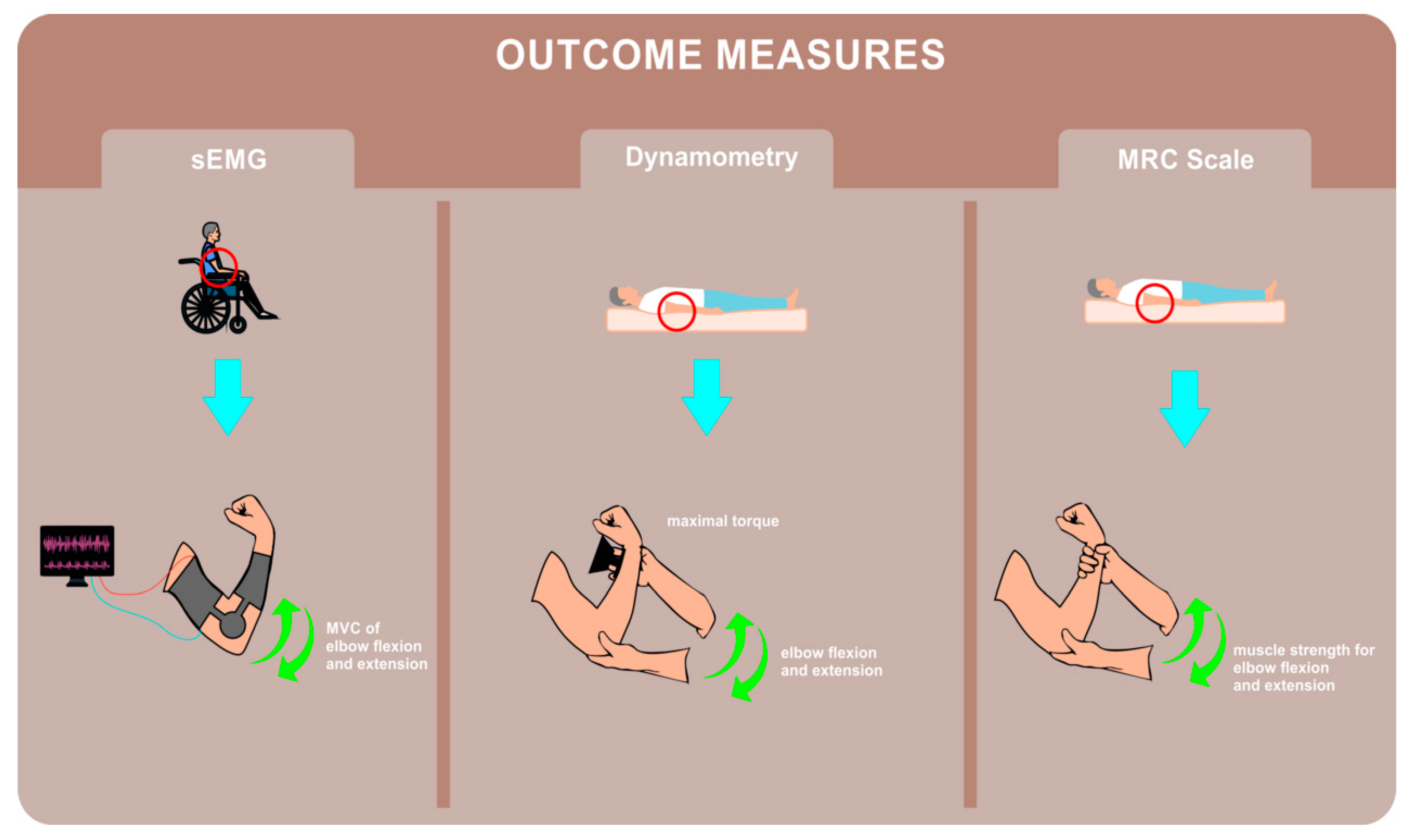
2.2. Outcome Measures
2.2.1. MRC Scale for Muscle Strength
2.2.2. Dynamometry
2.2.3. Surface Electromyography
2.3. Intervention
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lui, S.K.; Nguyen, M.H. Elderly Stroke Rehabilitation: Overcoming the Complications and Its Associated Challenges. Curr. Gerontol. Geriatr. Res. 2018, 2018, 9853837. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, X.; Gong, Y.; Cheng, Y.; Gao, X.; Chen, X. Motor Function Evaluation of Hemiplegic Upper-Extremities Using Data Fusion from Wearable Inertial and Surface EMG Sensors. Sensors 2017, 17, 582. [Google Scholar] [CrossRef] [Green Version]
- Kiper, P.; Szczudlik, A.; Mirek, E.; Nowobilski, R.; Opara, J.; Agostini, M.; Tonin, P.; Turolla, A. The application of virtual reality in neuro-rehabilitation: Motor re-learning supported by innovative technologies. Med. Rehabil. 2013, 17, 29–36. [Google Scholar] [CrossRef]
- Kuo, I.Y.; Ehrlich, B.E. Signaling in muscle contraction. Cold Spring Harb. Perspect. Biol. 2015, 7, a006023. [Google Scholar] [CrossRef]
- James, M.A. Use of the Medical Research Council muscle strength grading system in the upper extremity. J. Hand Surg. Am. 2007, 32, 154–156. [Google Scholar] [CrossRef]
- Medical Research Council. Aids to the Examination of the Peripheral Nervous System; Pengragon House: London, UK, 1975. [Google Scholar]
- Gregson, J.M.; Leathley, M.J.; Moore, A.P.; Smith, T.L.; Sharma, A.K.; Watkins, C.L. Reliability of measurements of muscle tone and muscle power in stroke patients. Age Ageing 2000, 29, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paternostro-Sluga, T.; Grim-Stieger, M.; Posch, M.; Schuhfried, O.; Vacariu, G.; Mittermaier, C.; Bittner, C.; Fialka-Moser, V. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J. Rehabil. Med. 2008, 40, 665–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jepsen, J.; Laursen, L.; Larsen, A.; Hagert, C.G. Manual strength testing in 14 upper limb muscles: A study of inter-rater reliability. Acta Orthop. Scand. 2004, 75, 442–448. [Google Scholar] [CrossRef] [Green Version]
- Dyck, P.J.; Boes, C.J.; Mulder, D.; Millikan, C.; Windebank, A.J.; Dyck, P.J.B.; Espinosa, R. History of standard scoring, notation, and summation of neuromuscular signs. A current survey and recommendation. J. Peripher. Nerv. Syst. 2005, 10, 158–173. [Google Scholar] [CrossRef]
- Hermans, G.; Clerckx, B.; Vanhullebusch, T.; Segers, J.; Vanpee, G.; Robbeets, C.; Casaer, M.P.; Wouters, P.; Gosselink, R.; Van den Berghe, G. Interobserver agreement of medical research council sum-score and handgrip strength in the intensive care unit. Muscle Nerve 2012, 45, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Dupépé, E.B.; Davis, M.; Elsayed, G.A.; Agee, B.; Kirksey, K.; Gordon, A.; Pritchard, P.R. Inter-rater reliability of the modified Medical Research Council scale in patients with chronic incomplete spinal cord injury. J. Neurosurg. Spine 2019, 18, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Samosawala, N.R.; Vaishali, K.; Kalyana, B.C. Measurement of muscle strength with handheld dynamometer in Intensive Care Unit. Indian J. Crit. Care Med. 2016, 20, 21–26. [Google Scholar] [CrossRef]
- Nitschke, J.E. Reliability of isokinetic torque measurements: A review of the literature. Aust. J. Physiother. 1992, 38, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Baschung Pfister, P.; de Bruin, E.D.; Sterkele, I.; Maurer, B.; de Bie, R.A.; Knols, R.H. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra- and interrater reliability and validity study. PLoS ONE 2018, 13, e0194531. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, L.T.; Martins, J.C.; Lara, E.M.; Albuquerque, J.A.; Teixeira-Salmela, L.F.; Faria, C.D. Dynamometry for the measurement of grip, pinch, and trunk muscles strength in subjects with subacute stroke: Reliability and different number of trials. Braz. J. Phys. Ther. 2016, 20, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karthikbabu, S.; Chakrapani, M. Hand-Held Dynamometer is a Reliable Tool to Measure Trunk Muscle Strength in Chronic Stroke. J. Clin. Diagn. Res. 2017, 11, YC09–YC12. [Google Scholar] [CrossRef]
- Kushner, J. Encyclopedia of the Neurological Sciences; Choice: Current Reviews for Academic Libraries; Academic Press: Cleveland, OH, USA, 2003; Volume 41, p. 687. [Google Scholar]
- Merletti, R.; Parker, P. Electromyography: Physiology, Engineering, and Noninvasive Applications; IEEE Press/J Wiley: Hoboken, NJ, USA, 2004. [Google Scholar]
- Gilmore, K.L.; Meyers, J.E. Using Surface Electromyography in Physiotherapy Research. Aust. J. Physiother. 1983, 29, 3–9. [Google Scholar] [CrossRef]
- Rong, W.; Tong, K.Y.; Hu, X.L.; Ho, S.K. Effects of electromyography-driven robot-aided hand training with neuromuscular electrical stimulation on hand control performance after chronic stroke. Disabil. Rehabil. Assist. Technol. 2015, 10, 149–159. [Google Scholar] [CrossRef]
- Cesqui, B.; Tropea, P.; Micera, S.; Krebs, H.I. EMG-based pattern recognition approach in post stroke robot-aided rehabilitation: A feasibility study. J. Neuroeng. Rehabil. 2013, 10, 75. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Luo, Z.; Jin, Y.; Xi, X. Gesture Recognition Based on Multiscale Singular Value Entropy and Deep Belief Network. Sensors 2020, 21, 119. [Google Scholar] [CrossRef]
- Gonzalez, S.; Stegall, P.; Edwards, H.; Stirling, L.; Siu, H.C. Ablation Analysis to Select Wearable Sensors for Classifying Standing, Walking, and Running. Sensors 2020, 21, 194. [Google Scholar] [CrossRef] [PubMed]
- Diez, J.A.; Santamaria, V.; Khan, M.I.; Catalan, J.M.; Garcia-Aracil, N.; Agrawal, S.K. Exploring New Potential Applications for Hand Exoskeletons: Power Grip to Assist Human Standing. Sensors 2020, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, G.; Sylos-Labini, F.; Assenza, C.; Libernini, L.; Morelli, D.; Lacquaniti, F.; Ivanenko, Y. Clinical Relevance of State-of-the-Art Analysis of Surface Electromyography in Cerebral Palsy. Front. Neurol. 2020, 11, 583296. [Google Scholar] [CrossRef] [PubMed]
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef] [Green Version]
- Merletti, R.; Farina, D. Surface Electromyography: Physiology, Engineering, and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016. [Google Scholar]
- Zhang, Z.; Yang, K.; Qian, J.; Zhang, L. Real-Time Surface EMG Pattern Recognition for Hand Gestures Based on an Artificial Neural Network. Sensors 2019, 19, 3170. [Google Scholar] [CrossRef] [Green Version]
- Vasanthi, S.M.; Jayasree, T. Performance evaluation of pattern recognition networks using electromyography signal and time-domain features for the classification of hand gestures. Proc. Inst. Mech. Eng. H 2020, 234, 639–648. [Google Scholar] [CrossRef]
- Tsinganos, P.; Cornelis, B.; Cornelis, J.; Jansen, B.; Skodras, A. Data Augmentation of Surface Electromyography for Hand Gesture Recognition. Sensors 2020, 20, 4892. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Slater, L.V.; Corbett, R.O.; Hart, J.M.; Hertel, J. Muscle activation patterns of the lumbo-pelvic-hip complex during walking gait before and after exercise. Gait Posture 2017, 52, 15–21. [Google Scholar] [CrossRef]
- Lu, Z.; Tong, K.Y.; Zhang, X.; Li, S.; Zhou, P. Myoelectric Pattern Recognition for Controlling a Robotic Hand: A Feasibility Study in Stroke. IEEE Trans. Biomed. Eng. 2019, 66, 365–372. [Google Scholar] [CrossRef]
- Resnik, L.; Huang, H.H.; Winslow, A.; Crouch, D.L.; Zhang, F.; Wolk, N. Evaluation of EMG pattern recognition for upper limb prosthesis control: A case study in comparison with direct myoelectric control. J. Neuroeng. Rehabil. 2018, 15, 23. [Google Scholar] [CrossRef]
- Parajuli, N.; Sreenivasan, N.; Bifulco, P.; Cesarelli, M.; Savino, S.; Niola, V.; Esposito, D.; Hamilton, T.J.; Naik, G.R.; Gunawardana, U.; et al. Real-Time EMG Based Pattern Recognition Control for Hand Prostheses: A Review on Existing Methods, Challenges and Future Implementation. Sensors 2019, 19, 4596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, C.; He, B.; Wang, Y.; Cao, J.; Gao, S. EMG-Centered Multisensory Based Technologies for Pattern Recognition in Rehabilitation: State of the Art and Challenges. Biosensors 2020, 10, 85. [Google Scholar] [CrossRef] [PubMed]
- Kuriki, H.U.; Mícolis de Azevedo, F.; Takahashi, L.S.O.; Mello, E.M.; Filho, R.d.F.N.; Alves, N. The Relationship Between Electromyography and Muscle Force. In EMG Methods for Evaluating Muscle and Nerve Function; Schwartz, M., Ed.; InTech: Sao Paulo, Brasil, 2012; p. 532. [Google Scholar]
- Petersen, E.; Rostalski, P. A Comprehensive Mathematical Model of Motor Unit Pool Organization, Surface Electromyography, and Force Generation. Front. Physiol. 2019, 10, 176. [Google Scholar] [CrossRef] [Green Version]
- Disselhorst-Klug, C.; Schmitz-Rode, T.; Rau, G. Surface electromyography and muscle force: Limits in sEMG-force relationship and new approaches for applications. Clin. Biomech. 2009, 24, 225–235. [Google Scholar] [CrossRef]
- Zhou, P.; Rymer, W.Z. Factors governing the form of the relation between muscle force and the EMG: A simulation study. J. Neurophysiol. 2004, 92, 2878–2886. [Google Scholar] [CrossRef] [Green Version]
- Kiper, P.; Baba, A.; Agostini, M.; Turolla, A. Proprioceptive based training for stroke recovery. Proposal of new treatment modality for rehabilitation of upper limb in neurological diseases. Arch. Physiother. 2015, 5, 6. [Google Scholar] [CrossRef]
- Hislop, H.J.; Avers, D.; Brown, M.; Daniels, L. Daniels and Worthingham’s Muscle Testing: Techniques of Manual Examination and Performance Testing, 9th ed.; Elsevier: St. Louis, MO, USA, 2014; 514p. [Google Scholar]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst, C.; Hagg, G. SENIAM Raccomandazioni Europee per l’Elettromiografia di Superficie; CLUT: Torino, Italy, 2000; p. 138. [Google Scholar]
- Deroide, N.; Bousson, V.; Mambre, L.; Vicaut, E.; Laredo, J.D.; Kubis, N. Muscle MRI STIR signal intensity and atrophy are correlated to focal lower limb neuropathy severity. Eur. Radiol. 2015, 25, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Chia, D.S.Y.; Doi, K.; Hattori, Y.; Sakamoto, S. Elbow flexion strength and contractile activity after partial ulnar nerve or intercostal nerve transfers for brachial plexus injuries. J. Hand Surg. Eur. Vol. 2020, 45, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Bilodeau, M.; Schindler-Ivens, S.; Williams, D.M.; Chandran, R.; Sharma, S.S. EMG frequency content changes with increasing force and during fatigue in the quadriceps femoris muscle of men and women. J. Electromyogr. Kinesiol. 2003, 13, 83–92. [Google Scholar] [CrossRef]
- Madeleine, P.; Bajaj, P.; Sogaard, K.; Arendt-Nielsen, L. Mechanomyography and electromyography force relationships during concentric, isometric and eccentric contractions. J. Electromyogr. Kinesiol. 2001, 11, 113–121. [Google Scholar] [CrossRef]
- Doud, J.R.; Walsh, J.M. Muscle fatigue and muscle length interaction: Effect on the EMG frequency components. Electromyogr. Clin. Neurophysiol. 1995, 35, 331–339. [Google Scholar] [PubMed]
- Woods, J.J.; Bigland-Ritchie, B. Linear and non-linear surface EMG/force relationships in human muscles. An anatomical/functional argument for the existence of both. Am. J. Phys. Med. 1983, 62, 287–299. [Google Scholar] [PubMed]
- Cuthbert, S.C.; Goodheart, G.J., Jr. On the reliability and validity of manual muscle testing: A literature review. Chiropr. Osteopathy 2007, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Parameters | Before Mean ± SD (95% CI) | After Mean ± SD (95% CI) |
|---|---|---|
| MRC (No) (biceps brachii) | 0.42 ± 0.51 (0.18–0.67) | 2.37 ± 0.96 (1.91–2.83) |
| MRC (No) (triceps brachii) | 0.21 ± 0.42 (0.01–0.41) | 2.16 ± 0.90 (1.73–2.59) |
| Dynamometry (N) (biceps brachii) | 4.11 ± 6.04 (1.19–7.02) | 23.00 ± 15.89 (15.34–30.66) |
| Dynamometry (N) (triceps brachii) | 2.05 ± 5.45 (−0.58–4.68) | 23.68 ± 18.93 (14.56–2.81) |
| sEMG (mV) (biceps brachii) | 7.15 ± 8.89 (2.42–11.88) | 40.04 ± 41.43 (17.09–62.98) |
| sEMG (mV) (triceps brachii) | 2.04 ± 2.4 (0.71–3.37) | 34.5 ± 43.16 (10.59–58.41) |
| Clinical Parameters | Before | After | ∆ | |||
|---|---|---|---|---|---|---|
| ρ | p-Value | ρ | p-Value | ρ | p-Value | |
| sEMG (Biceps Brachii) | 0.342 A | 0.1953 | 0.601 A | 0.0177 * | 0.453 | 0.0898 |
| Dynamometry (Biceps Brachii) | 0.954 A | 0.0000 * | 0.867 A | 0.0001 * | 0.795 | 0.0000 * |
| sEMG (Triceps Brachii) | 0.178 B | 0.5267 | 0.717 B | 0.0026 * | 0.677 | 0.0079 * |
| Dynamometry (Triceps Brachii) | 0.749 B | 0.0002 * | 0.873 B | 0.0001 * | 0.795 | 0.0000 * |
| Regression Model | % Variance Explained | p-Value of Residuals |
|---|---|---|
| MRC (biceps brachii) = 0.017 · sEMG (biceps brachii) | 0.50 | p = 0.766 |
| MRC (biceps brachii) = 0.050 · Dynamometry (biceps brachii) | 0.70 | p = 0.165 |
| MRC (triceps brachii) = 0.012 · sEMG (triceps brachii) | 0.31 | p = 0.009 * |
| MRC (triceps brachii) = 0.041 · Dynamometry (triceps brachii) | 0.76 | p = 0.033 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiper, P.; Rimini, D.; Falla, D.; Baba, A.; Rutkowski, S.; Maistrello, L.; Turolla, A. Does the Score on the MRC Strength Scale Reflect Instrumented Measures of Maximal Torque and Muscle Activity in Post-Stroke Survivors? Sensors 2021, 21, 8175. https://doi.org/10.3390/s21248175
Kiper P, Rimini D, Falla D, Baba A, Rutkowski S, Maistrello L, Turolla A. Does the Score on the MRC Strength Scale Reflect Instrumented Measures of Maximal Torque and Muscle Activity in Post-Stroke Survivors? Sensors. 2021; 21(24):8175. https://doi.org/10.3390/s21248175
Chicago/Turabian StyleKiper, Pawel, Daniele Rimini, Deborah Falla, Alfonc Baba, Sebastian Rutkowski, Lorenza Maistrello, and Andrea Turolla. 2021. "Does the Score on the MRC Strength Scale Reflect Instrumented Measures of Maximal Torque and Muscle Activity in Post-Stroke Survivors?" Sensors 21, no. 24: 8175. https://doi.org/10.3390/s21248175