
SleepPos App: An Automated Smartphone Application for Angle Based High Resolution Sleep Position Monitoring and Treatment

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. ‘SleepPos’ App: Design and Specifications
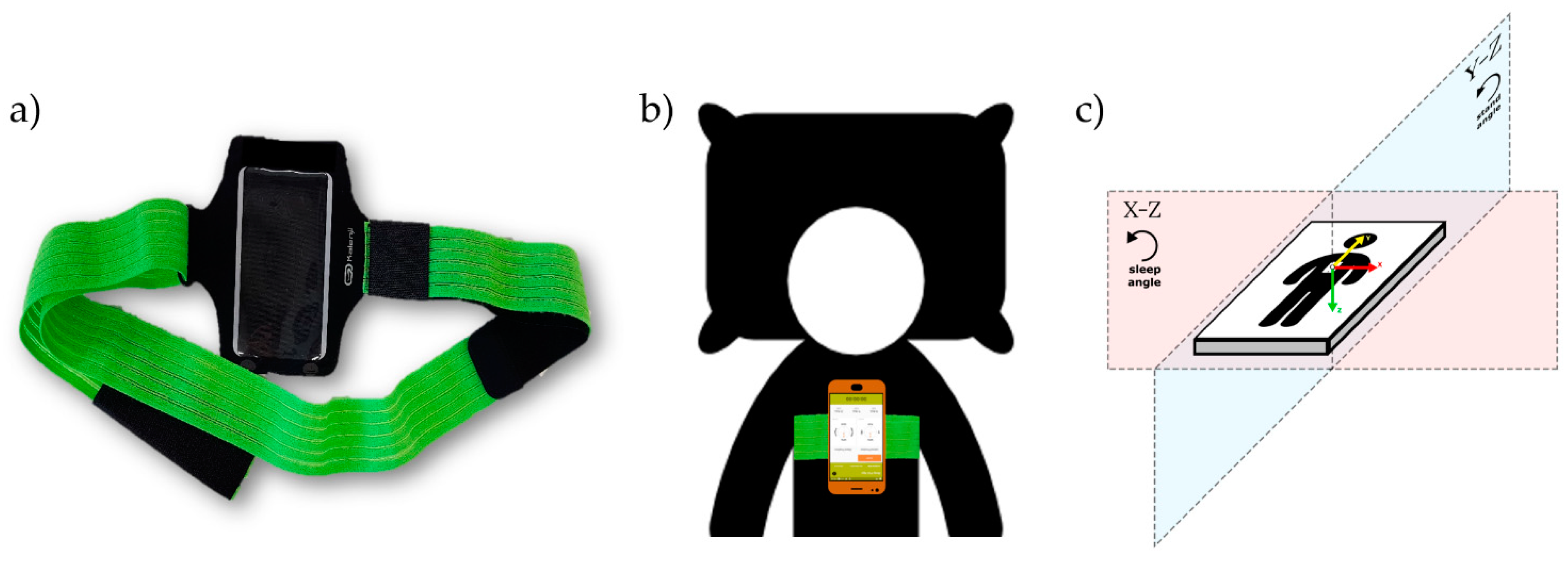
2.1.1. Hardware
- An Android smartphone containing an accelerometry sensor.
2.1.2. Software
- 1
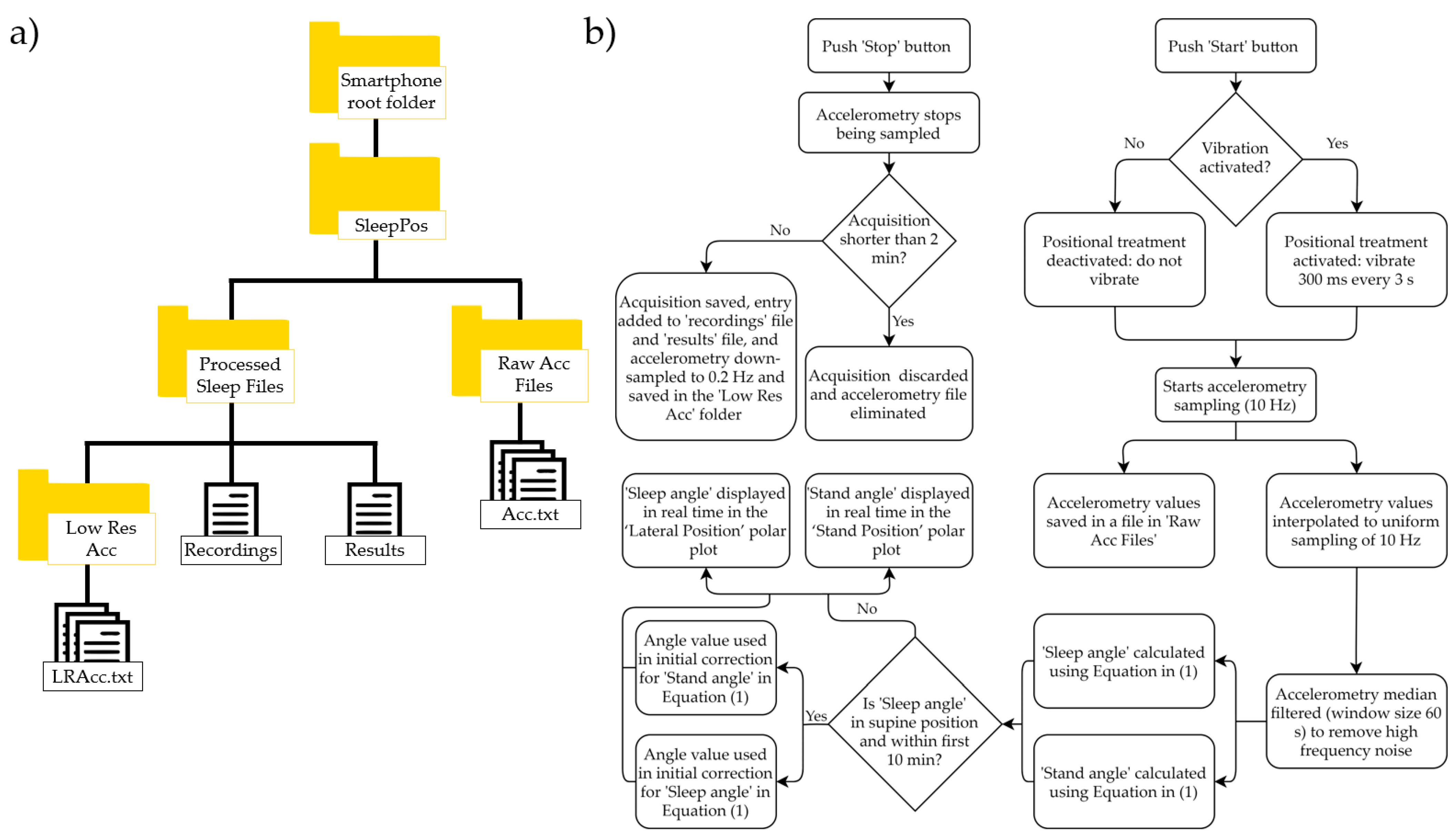
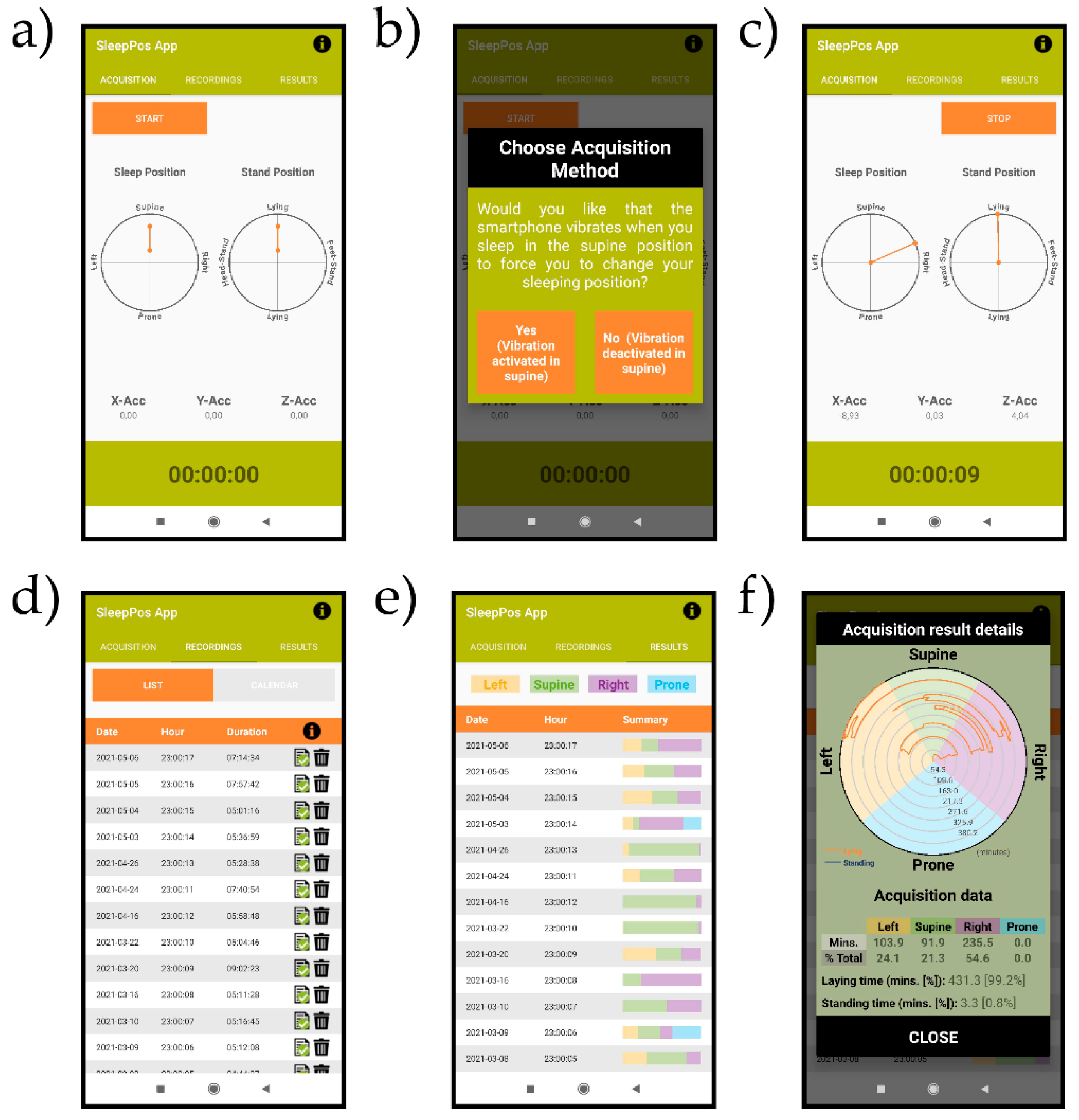
- ‘Acquisition’ tab: this tab allows to start the sleep position acquisition by clicking the ‘Start’ button and stop it by clicking the ‘Stop’ button. Once the ‘Start’ button is clicked, a dialog prompts asking if you would like the smartphone to vibrate when sleeping in a supine-like sleep position, to force the user to change the sleep position. If vibration is selected, when sleeping in a supine-like sleep position, the smartphone will vibrate for 300 ms every 3 s. After the user’s decision upon the vibration option, accelerometry starts being sampled at a non-uniform sample rate of around 10 Hz. The acquired accelerometry data are saved in a separate file in the ‘Raw Acc Files’ folder seen in Figure 2a, and a new registry is entered in the ‘Recordings’ file. Then, it is simultaneously processed to extract information of interest and it is interpolated to a uniform sampling rate of 10 Hz. Afterwards, each sampled accelerometry value is median filtered, with a window of 60 s around each sample, to remove the high frequency noise from the accelerometry. In addition, the sleep angle and stand angles are calculated and displayed on the polar plots from the tab using the following formula:where, for the sleep angle, with and being the values of the X and Z axis of the triaxial accelerometry at each specific timestamp; , which is a static reference aligned with the left sleep position; and , to be able to differentiate supine and prone positions. For the stand angle, , with and being the values of the Y and Z axis of the triaxial accelerometry at each specific timestamp; , which is a static reference aligned with the stand position; and , to be able to differentiate stand and headstand positions. The is an angle used to correct the differences in anatomy between patients when placing the phone over the sternum. It is automatically determined from the sleep and stand angles when sleeping in a supine position during the first 10 min of acquisition [38]. It can be different for the sleep and stand angles and it is used to ensure that the smartphone returns 90° for both the sleep and stand angles when being in a pure supine position, which are the values expected for this position. The algorithm described in this section has successfully been tested and validated in a previous work of our group compared to the video-validated position from the PSG [38].Then, the sleep angle is used to display the high-resolution sleep position in real time in the ‘Sleep Position’ polar plot, which shows the smartphone angular orientation between the four classic sleep positions (supine, left, right and prone). The stand angle can also be observed in real time to determine if the subject is laying on the bed or standing, by looking at the ‘Stand Position’ polar plot, which shows the angular orientation between the standing and laying positions. The acceleration values and time spent on the acquisition can also be seen in this Table Finally, accelerometry is down-sampled to 0.2 Hz and saved also in the ‘Low Res Acc’ folder for its visualization in the results Table Acquisitions shorter than 2 min are discarded. The logical scheme applied in this tab can be seen in Figure 2b.
- 2
- ‘Recordings’ tab: this tab displays all the sleep position acquisitions performed. For each acquisition, the date, start time, and duration are shown. It is also possible to switch to a calendar view, where the number of acquisitions per day are shown. Finally, in this menu it is possible to observe whether the accelerometry file is still saved in the smartphone memory and it gives you the option to delete the file and/or the results linked to the acquisition.
- 3
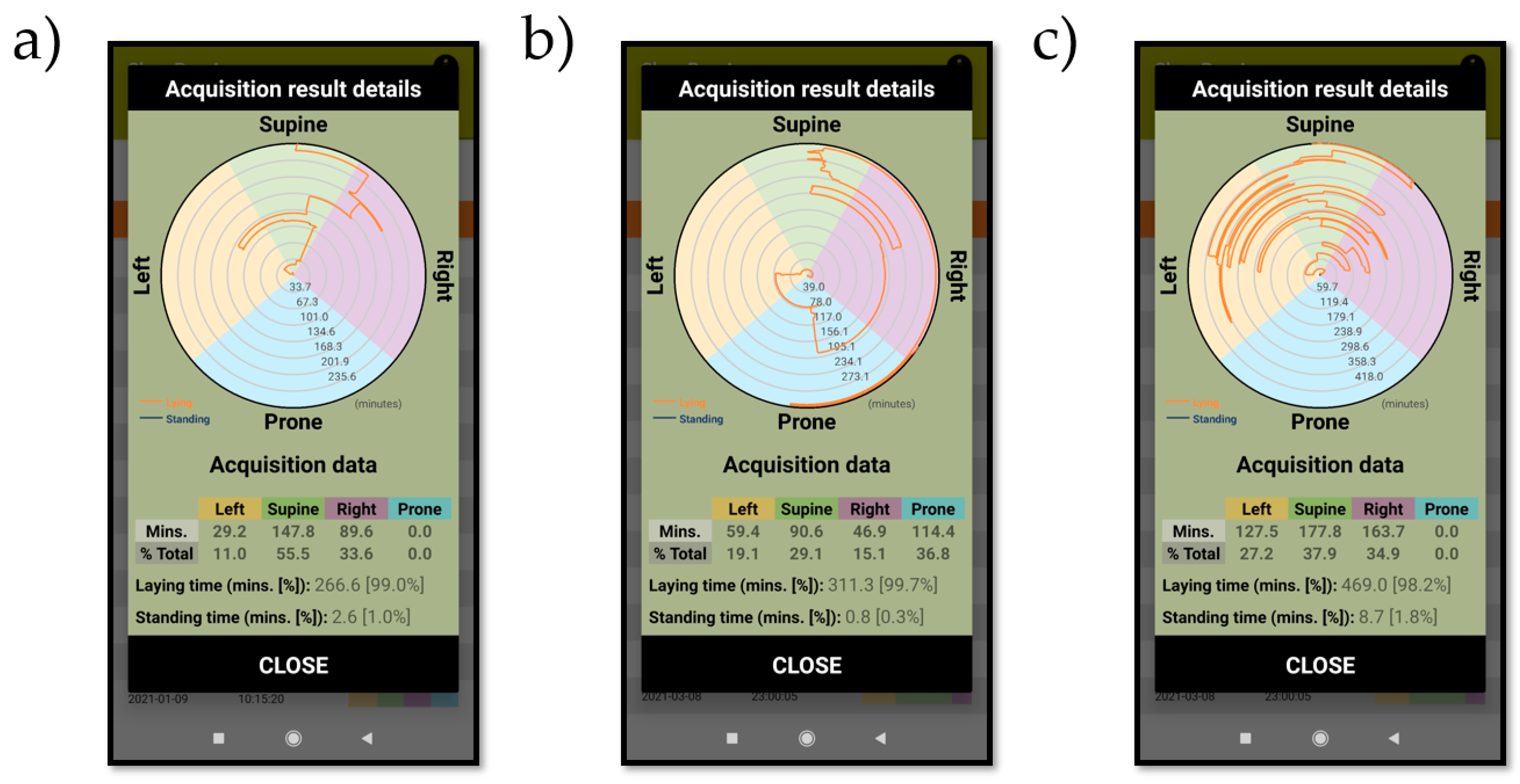
- ‘Results’ tab: this tab shows the sleep position results for each of the acquisitions, including the acquisition date, start time, and a summary of the discrete sleep position performance. When clicking on each of the sleep position summary boxes, a dialog box appears showing the details of the acquisition. The details of the sleep position include a polar plot showing the evolution in time of the sleep position as well as a summary table with the minutes and percentage of minutes spent at each sleep position. In the detailed polar plot, the standing position, if present, appears in blue, and the laying position in orange. The high-resolution sleep position orientation is also shown, allowing to determine the exact angular orientation at each specific time of the night.
2.2. ‘SleepPos’ App: Position Monitoring during the Night
2.3. ‘SleepPos’ App: Combination with Oximetry
2.4. ‘SleepPos’ App: Positional Treatment
3. Results
3.1. ‘SleepPos’ App: Design and Specifications
 is used to provide the information that the raw accelerometry is still saved in the ‘Raw Acc Files’ folder, whereas the
is used to provide the information that the raw accelerometry is still saved in the ‘Raw Acc Files’ folder, whereas the  icon is used to provide the information that the raw accelerometry has been removed. The icon
icon is used to provide the information that the raw accelerometry has been removed. The icon  opens a window which let the users decide whether to remove the raw accelerometry file to reduce the smartphone’s memory used, or to remove this acquisition and its results from the app. Each acquisition is estimated to occupy at maximum 20 Mb.
opens a window which let the users decide whether to remove the raw accelerometry file to reduce the smartphone’s memory used, or to remove this acquisition and its results from the app. Each acquisition is estimated to occupy at maximum 20 Mb.3.2. ‘SleepPos’ App: Position Monitoring during the Night
3.3. ‘SleepPos’ App: Combination with Pulse Oximetry
3.4. ‘SleepPos’ App: Positional Treatment
4. Discussion
4.1. High-Resolution Sleep Position Monitoring and Treatment Relevance
4.2. Sleep Position and Oximetry
4.3. Smartphones and Their Role as Portable mHealth Tools
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lee, K.A. An overview of sleep and common sleep problems. ANNA J. 1997, 24, 614–623. [Google Scholar]
- Aminoff, M.J.; Boller, F.; Swaab, D.F. We spend about one-third of our life either sleeping or attempting to do so. Handb. Clin. Neurol. 2011, 98, vii. [Google Scholar] [CrossRef]
- Koo, D.L.; Kim, J. The Physiology of Normal Sleep. Hanyang Med. Rev. 2013, 33, 190. [Google Scholar] [CrossRef] [Green Version]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Bishop, T.M.; Walsh, P.G.; Ashrafioun, L.; Lavigne, J.E.; Pigeon, W.R. Sleep, suicide behaviors, and the protective role of sleep medicine. Sleep Med. 2020, 66, 264–270. [Google Scholar] [CrossRef]
- Stowkowy, J.; Brummitt, K.; Bonneville, D.; Goldstein, B.I.; Wang, J.; Kennedy, S.H.; Bray, S.; Lebel, C.; MacQueen, G.; Addington, J. Sleep disturbances in youth at-risk for serious mental illness. Early Interv. Psychiatry 2020, 14, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Augner, C. Associations of Subjective Sleep Quality with Depression Score, Anxiety, Physical Symptoms and Sleep Onset Latency in Young Students. Cent. Eur. J. Public Health 2011, 19, 115–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartlett, D.J.; Marshall, N.S.; Williams, A.; Grunstein, R.R. Sleep health New South Wales: Chronic sleep restriction and daytime sleepiness. Intern. Med. J. 2007. [Google Scholar] [CrossRef]
- Yoshihisa, A.; Takeishi, Y. Sleep Disordered Breathing and Cardiovascular Diseases. J. Atheroscler. Thromb. 2019, 26, 315–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durgan, D.J.; Bryan, R.M. Cerebrovascular Consequences of Obstructive Sleep Apnea. J. Am. Heart Assoc. 2012, 1. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, F.B.; Anderson, R.N. The Leading Causes of Death in the US for 2020. JAMA 2021, 325, 1829. [Google Scholar] [CrossRef]
- Organization World Health. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 15 May 2021).
- Kaplowitz, K.; Blizzard, S.; Blizzard, D.J.; Nwogu, E.; Hamill, C.E.; Weinreb, R.N.; Mohsenin, V.; Loewen, N.A. Time Spent in Lateral Sleep Position and Asymmetry in Glaucoma. Investig. Opthalmol. Vis. Sci. 2015, 56, 3869. [Google Scholar] [CrossRef] [Green Version]
- Alevi, D.; Perry, H.D.; Wedel, A.; Rosenberg, E.; Alevi, L.; Donnenfeld, E.D. Effect of Sleep Position on the Ocular Surface. Cornea 2017, 36, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Kaplowitz, K.; Dredge, J.; Honkanen, R. Relationship between sleep position and glaucoma progression. Curr. Opin. Ophthalmol. 2019, 30, 484–490. [Google Scholar] [CrossRef]
- Kerr, M.G.; Scott, D.B.; Samuel, E. Studies of the Inferior Vena Cava in Late Pregnancy. Br. Med. J. 1964, 1, 522-4, 532–533. [Google Scholar] [CrossRef] [Green Version]
- Jeffreys, R.; Stepanchak, W.; Lopez, B.; Hardis, J.; Clapp, J. Uterine blood flow during supine rest and exercise after 28 weeks of gestation. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Warland, J.; Dorrian, J.; Morrison, J.L.; O’Brien, L.M. Maternal sleep during pregnancy and poor fetal outcomes: A scoping review of the literature with meta-analysis. Sleep Med. Rev. 2018, 41, 197–219. [Google Scholar] [CrossRef] [PubMed]
- Robertson, N.T.; Turner, J.M.; Kumar, S. Pathophysiological changes associated with sleep disordered breathing and supine sleep position in pregnancy. Sleep Med. Rev. 2019, 46, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Oksenberg, A.; Arons, E.; Radwan, H.; Silverberg, D.S. Positional vs Nonpositional Obstructive Sleep Apnea Patients. Chest 1997, 112, 629–639. [Google Scholar] [CrossRef] [Green Version]
- Yalciner, G.; Babademez, M.A.; Gul, F. Association of sleep time in supine position with apnea-hypopnea index as evidenced by successive polysomnography. Sleep Breath. 2017, 21, 289–294. [Google Scholar] [CrossRef]
- Eckert, D.J.; Malhotra, A. Pathophysiology of Adult Obstructive Sleep Apnea. Proc. Am. Thorac. Soc. 2008, 5, 144–153. [Google Scholar] [CrossRef]
- Patil, S.P.; Schneider, H.; Schwartz, A.R.; Smith, P.L. Adult Obstructive Sleep Apnea. Chest 2007, 132, 325–337. [Google Scholar] [CrossRef] [Green Version]
- Osman, A.M.; Carter, S.G.; Carberry, J.C.; Eckert, D.J. Obstructive sleep apnea: Current perspectives. Nat. Sci. Sleep 2018, 10, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Rundo, J.V. Obstructive sleep apnea basics. Cleve. Clin. J. Med. 2019, 86, 2–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. STOP Questionnaire. Anesthesiology 2008, 108, 812–821. [Google Scholar] [CrossRef] [Green Version]
- Netzer, N.C.; Stoohs, R.A.; Netzer, C.M.; Clark, K.; Strohl, K.P. Using the Berlin Questionnaire To Identify Patients at Risk for the Sleep Apnea Syndrome. Ann. Intern. Med. 1999, 131, 485. [Google Scholar] [CrossRef] [PubMed]
- Lomeli, H.A.; Pérez-Olmos, I.; Talero-Gutiérrez, C.; Moreno, C.B.; González-Reyes, R.; Palacios, L.; de la Peña, F.; Muñoz-Delgado, J. Sleep evaluation scales and questionaries: A review. Actas Esp. Psiquiatr. 2008, 36, 50–59. [Google Scholar]
- Russo, K.; Bianchi, M.T. How Reliable Is Self-Reported Body Position during Sleep? J. Clin. Sleep Med. 2016, 12, 127–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warland, J.; Dorrian, J. Accuracy of Self-Reported Sleep Position in Late Pregnancy. PLoS ONE 2014, 9, e115760. [Google Scholar] [CrossRef] [PubMed]
- Kai-Ching Yu, C. Why is Self-Report of Sleep Position Sometimes Unreliable? Sleep Hypn. Int. J. 2017. [Google Scholar] [CrossRef] [Green Version]
- Vonk, P.E.; de Vries, N.; Ravesloot, M.J.L. Polysomnography and sleep position, a Heisenberg phenomenon? HNO 2019, 67, 679–684. [Google Scholar] [CrossRef]
- Metersky, M.L.; Castriotta, R.J. The Effect of Polysomnography on Sleep Position: Possible Implications on the Diagnosis of Positional Obstructive Sleep Apnea. Respiration 1996, 63, 283–287. [Google Scholar] [CrossRef]
- Wang, Y.-K.; Chen, H.-Y.; Chen, J.-R. Unobtrusive Sleep Monitoring Using Movement Activity by Video Analysis. Electronics 2019, 8, 812. [Google Scholar] [CrossRef] [Green Version]
- Cary, D.; Collinson, R.; Sterling, M.; Briffa, K. Examining the Relationship between Sleep Posture and Morning Spinal Symptoms in the Habitual Environment Using Infrared Cameras. J. Sleep Disord. Treat. Care 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Akbarian, S.; Delfi, G.; Zhu, K.; Yadollahi, A.; Taati, B. Automated Non-Contact Detection of Head and Body Positions During Sleep. IEEE Access 2019, 7, 72826–72834. [Google Scholar] [CrossRef]
- Tate, A.; Walsh, J.; Kurup, V.; Shenoy, B.; Mann, D.; Freakley, C.; Eastwood, P.; Terrill, P. An emerging technology for the identification and characterization of postural-dependent obstructive sleep apnea. J. Clin. Sleep Med. 2020, 16, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Lluis, I.; Castillo-Escario, Y.; Montserrat, J.M.; Jané, R. Enhanced Monitoring of Sleep Position in Sleep Apnea Patients: Smartphone Triaxial Accelerometry Compared with Video-Validated Position from Polysomnography. Sensors 2021, 21, 3689. [Google Scholar] [CrossRef]
- Xia, F.; Sawan, M. Clinical and Research Solutions to Manage Obstructive Sleep Apnea: A Review. Sensors 2021, 21, 1784. [Google Scholar] [CrossRef]
- Bloomfield, R.; Noble, D.W.; Sudlow, A. Prone position for acute respiratory failure in adults. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Gattinoni, L.; Busana, M.; Giosa, L.; Macrì, M.; Quintel, M. Prone Positioning in Acute Respiratory Distress Syndrome. Semin. Respir. Crit. Care Med. 2019, 40, 094–100. [Google Scholar] [CrossRef] [Green Version]
- Epstein, L.J.; Kristo, D.; Strollo, P.J.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar]
- Ravesloot, M.J.L.; van Maanen, J.P.; Dun, L.; de Vries, N. The undervalued potential of positional therapy in position-dependent snoring and obstructive sleep apnea—a review of the literature. Sleep Breath. 2013, 17, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Oksenberg, A.; Silverberg, D.; Offenbach, D.; Arons, E. Positional Therapy for Obstructive Sleep Apnea Patients: A 6-Month Follow-Up Study. Laryngoscope 2006, 116, 1995–2000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skinner, M.A.; Kingshott, R.N.; Filsell, S.; Taylor, D.R. Efficacy of the “tennis ball technique” versus nCPAP in the management of position-dependent obstructive sleep apnoea syndrome. Respirology 2008, 13, 708–715. [Google Scholar] [CrossRef]
- van Maanen, J.P.; Richard, W.; Van Kesteren, E.R.; Ravesloot, M.J.L.; Laman, D.M.; Hilgevoord, A.A.J.; de Vries, N. Evaluation of a new simple treatment for positional sleep apnoea patients. J. Sleep Res. 2012, 21, 322–329. [Google Scholar] [CrossRef]
- Laub, R.R.; Tønnesen, P.; Jennum, P.J. A Sleep Position Trainer for positional sleep apnea: A randomized, controlled trial. J. Sleep Res. 2017, 26, 641–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinzer, R. ‘Good vibrations’: Positional treatments for obstructive sleep apnoea. Thorax 2020, 75, 296. [Google Scholar] [CrossRef] [PubMed]
- Eijsvogel, M.M.; Ubbink, R.; Dekker, J.; Oppersma, E.; de Jongh, F.H.; van der Palen, J.; Brusse-Keizer, M.G. Sleep Position Trainer versus Tennis Ball Technique in Positional Obstructive Sleep Apnea Syndrome. J. Clin. Sleep Med. 2015, 11, 139–147. [Google Scholar] [CrossRef]
- Bignold, J.J.; Deans-Costi, G.; Goldsworthy, M.R.; Robertson, C.A.; McEvoy, D.; Catcheside, P.G.; Mercer, J.D. Poor long-term patient compliance with the tennis ball technique for treating positional obstructive sleep apnea. J. Clin. Sleep Med. 2009, 5, 428–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fino, E.; Mazzetti, M. Monitoring healthy and disturbed sleep through smartphone applications: A review of experimental evidence. Sleep Breath. 2019, 23, 13–24. [Google Scholar] [CrossRef]
- Behar, J.; Roebuck, A.; Domingos, J.S.; Gederi, E.; Clifford, G.D. A review of current sleep screening applications for smartphones. Physiol. Meas. 2013, 34, R29–R46. [Google Scholar] [CrossRef]
- Nakano, H.; Hirayama, K.; Sadamitsu, Y.; Toshimitsu, A.; Fujita, H.; Shin, S.; Tanigawa, T. Monitoring Sound To Quantify Snoring and Sleep Apnea Severity Using a Smartphone: Proof of Concept. J. Clin. Sleep Med. 2014, 10, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Escario, Y.; Ferrer-Lluis, I.; Montserrat, J.M.; Jane, R. Automatic Silence Events Detector from Smartphone Audio Signals: A Pilot mHealth System for Sleep Apnea Monitoring at Home. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4982–4985. [Google Scholar]
- Castillo-Escario, Y.; Ferrer-Lluis, I.; Montserrat, J.M.; Jane, R. Entropy Analysis of Acoustic Signals Recorded With a Smartphone for Detecting Apneas and Hypopneas: A Comparison With a Commercial System for Home Sleep Apnea Diagnosis. IEEE Access 2019, 7, 128224–128241. [Google Scholar] [CrossRef]
- Behar, J.; Roebuck, A.; Shahid, M.; Daly, J.; Hallack, A.; Palmius, N.; Stradling, J.; Clifford, G.D. SleepAp: An Automated Obstructive Sleep Apnoea Screening Application for Smartphones. IEEE J. Biomed. Health Inform. 2015, 19, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, A.; Ling, M.J.; Mann, J.; Arvind, D.K. Respiratory rate and flow waveform estimation from tri-axial accelerometer data. In Proceedings of the 2010 International Conference on Body Sensor Networks, Singapore, 7–9 June 2010; pp. 144–150. [Google Scholar]
- Ferrer-Lluis, I.; Castillo-Escario, Y.; Montserrat, J.M.; Jane, R. Automatic Event Detector from Smartphone Accelerometry: Pilot mHealth Study for Obstructive Sleep Apnea Monitoring at Home. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4990–4993. [Google Scholar]
- Ferrer-Lluis, I.; Castillo-Escario, Y.; Montserrat, J.M.; Jane, R. Analysis of Smartphone Triaxial Accelerometry for Monitoring Sleep-Disordered Breathing and Sleep Position at Home. IEEE Access 2020, 8, 71231–71244. [Google Scholar] [CrossRef]
- Liu, G.-Z.; Guo, Y.-W.; Zhu, Q.-S.; Huang, B.-Y.; Wang, L. Estimation of Respiration Rate from Three-Dimensional Acceleration Data Based on Body Sensor Network. Telemed. e-Health 2011, 17, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Haas, D.; Birk, R.; Maurer, J.T.; Hörmann, K.; Stuck, B.A.; Sommer, J.U. Therapie rückenlagebezogener obstruktiver Schlafapnoe mittels Smartphone-App. HNO 2017, 65, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. J. Clin. Sleep Med. 2012, 08, 597–619. [Google Scholar] [CrossRef] [Green Version]
- Temirbekoy, D.; Gunes, S.; Yazici, Z.M.; Sayin, İ. The Ignored Parameter in the Diagnosis of Obstructive Sleep Apnea Syndrome The Oxygen Desaturation Index. Turk Otolarengoloji Arsivi Turkish Arch. Otolaryngol. 2018, 1–6. [Google Scholar] [CrossRef]
- Fietze, I.; Dingli, K.; Diefenbach, K.; Douglas, N.J.; Glos, M.; Tallafuss, M.; Terhalle, W.; Witt, C. Night-to-night variation of the oxygen desaturation index in sleep apnoea syndrome. Eur. Respir. J. 2004, 24, 987–993. [Google Scholar] [CrossRef]
- Skarpsno, E.S.; Mork, P.J.; Nilsen, T.I.L.; Holtermann, A. Sleep positions and nocturnal body movements based on free-living accelerometer recordings: Association with demographics, lifestyle, and insomnia symptoms. Nat. Sci. Sleep 2017. [Google Scholar] [CrossRef] [Green Version]
- Freed, J.; Lowe, C.; Flodgren, G.; Binks, R.; Doughty, K.; Kolsi, J. Telemedicine: Is it really worth it? A perspective from evidence and experience. BMJ Health Care Inform. 2018, 25, 14–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekeland, A.G.; Bowes, A.; Flottorp, S. Effectiveness of telemedicine: A systematic review of reviews. Int. J. Med. Inform. 2010, 79, 736–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects | Left | Supine | Right | Prone | Laying | Standing | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Min | % | Min | % | Min | % | Min | % | Min | % | Min | % | |||||||||
| 1 | 16.0 | 4.3 | 56.2 | 1.1 | 210.5 | 56.7 | 94.6 | 9.2 | 142.4 | 38.4 | 157.1 | 4.3 | 2.3 | 0.6 | −85.6 | 1.3 | 371.2 | 94.1 | 23.3 | 5.9 |
| 2 | 29.2 | 11.0 | 31.0 | 2.9 | 147.8 | 55.5 | 105.7 | 8.8 | 89.6 | 33.6 | 129.6 | 4.4 | - | - | - | - | 266.6 | 99.0 | 2.6 | 1.0 |
| 3 | 159.2 | 47.7 | 22.1 | 11.6 | 152.4 | 45.7 | 98.0 | 12.2 | 22.0 | 6.6 | −173.1 | 16.1 | - | - | - | - | 333.6 | 100.0 | - | 0.0 |
| 4 | - | - | - | - | 114.5 | 36.1 | 112.4 | 1.6 | 202.6 | 63.9 | 161.4 | 6.2 | - | - | - | - | 317.1 | 100.0 | - | 0.0 |
| 5 | 87.3 | 30.7 | 59.2 | 1.2 | 145.4 | 51.1 | 85.7 | 18.2 | 51.9 | 18.2 | 157.9 | 2.4 | - | - | - | - | 284.6 | 100.0 | - | 0.0 |
| 6 | 59.4 | 19.1 | 5.6 | 5.0 | 90.6 | 29.1 | 97.4 | 4.2 | 46.9 | 15.1 | 175.5 | 20.7 | 114.4 | 36.8 | −97.8 | 3.1 | 311.3 | 99.7 | 0.8 | 0.3 |
| 7 | - | - | - | - | 177.1 | 56.1 | 99.0 | 8.7 | 138.7 | 43.9 | 170.2 | 9.1 | - | - | - | - | 315.8 | 99.7 | 0.9 | 0.3 |
| 8 | - | - | - | - | 72.8 | 23.4 | 102.7 | 2.1 | 238.6 | 76.6 | 161.3 | 7.4 | - | - | - | - | 311.4 | 100.0 | - | 0.0 |
| 9 | 227.8 | 42.3 | 40.7 | 10.5 | 176.0 | 32.7 | 98.8 | 14.6 | 134.1 | 24.9 | 173.8 | 13.3 | - | - | - | - | 537.9 | 99.2 | 4.5 | 0.8 |
| 10 | 3.5 | 1.1 | 52.7 | 8.0 | 290.0 | 95.2 | 86.2 | 7.3 | 11.2 | 3.7 | 162.0 | 27.3 | - | - | - | - | 304.7 | 100.0 | - | 0.0 |
| 11 | 97.8 | 21.6 | 33.7 | 4.2 | 198.5 | 43.9 | 98.2 | 7.9 | 155.8 | 34.5 | 172.0 | 7.5 | - | - | - | - | 452.1 | 98.1 | 8.8 | 1.9 |
| 12 | - | - | - | - | 335.7 | 94.4 | 95.1 | 4.1 | 19.9 | 5.6 | 125.5 | 2.6 | - | - | - | - | 355.6 | 99.1 | 3.3 | 0.9 |
| 13 | 24.4 | 7.5 | 58.8 | 0.8 | 293.3 | 90.1 | 85.2 | 13.6 | 7.7 | 2.4 | 128.3 | 0.3 | - | - | - | - | 325.4 | 99.0 | 3.2 | 1.0 |
| 14 | 42.8 | 12.9 | -22.1 | 14.5 | 29.0 | 8.7 | 86.5 | 5.0 | 185.6 | 55.8 | 174.2 | 22.2 | 75.4 | 22.7 | −115.0 | 21.4 | 332.8 | 98.7 | 4.3 | 1.3 |
| 15 | 113.3 | 37.6 | 18.5 | 12.1 | 98.1 | 32.6 | 91.9 | 9.8 | 89.8 | 29.8 | 129.2 | 0.8 | - | - | - | - | 301.2 | 100.0 | 0.0 | 0.0 |
| 16 | 127.5 | 27.2 | 6.6 | 8.4 | 177.8 | 37.9 | 86.4 | 8.1 | 163.7 | 34.9 | 147.9 | 15.6 | - | - | - | - | 469.0 | 98.2 | 8.7 | 1.8 |
| 17 | 103.9 | 24.1 | 20.5 | 5.4 | 91.9 | 21.3 | 87.2 | 7.4 | 235.5 | 54.6 | 161.8 | 5.1 | - | - | - | - | 431.3 | 99.2 | 3.3 | 0.8 |
| Total | 1092.1 | 18.1 | 26.6 | 20.7 | 2801.4 | 46.5 | 94.0 | 12.2 | 1936.0 | 32.2 | 160.6 | 17.5 | 192.1 | 3.2 | −104.4 | 16.1 | 6021.6 | 99.0 | 63.7 | 1.0 |
| Subjects | Desaturation Events (Number) | Sleep Time (Hours) | ODI (h−1) | ODI Severity |
|---|---|---|---|---|
| 1 | 92 | 6.2 | 14.9 | Mild |
| 2 | 107 | 4.4 | 24.1 | Moderate |
| 3 | 43 | 5.6 | 7.7 | Mild |
| 4 | 136 | 5.3 | 25.7 | Moderate |
| 5 | 4 | 4.7 | 0.8 | Healthy |
| 6 | 6 | 5.2 | 1.2 | Healthy |
| 7 | 138 | 5.3 | 26.2 | Moderate |
| 8 | 108 | 5.2 | 20.8 | Moderate |
| 9 | 42 | 9.0 | 4.7 | Healthy |
| 10 | 20 | 5.1 | 3.9 | Healthy |
| 11 | 295 | 7.5 | 39.2 | Severe |
| 12 | 342 | 5.9 | 57.7 | Severe |
| 13 | 83 | 5.4 | 15.3 | Moderate |
| 14 | 40 | 5.5 | 7.2 | Mild |
| 15 | 78 | 5.0 | 15.5 | Moderate |
| 16 | 230 | 7.8 | 29.4 | Moderate |
| 17 | 203 | 7.2 | 28.2 | Moderate |
| Total/Mean | 1967 | 100.3 | 19.6 | Moderate |
| Subjects | Left | Supine | Right | Prone | Desaturation Events (Number) | Sleep Time (Hours) | ODI (h−1) | ODI Severity | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Min | % | Min | % | Min | % | Min | % | |||||
| 1 | 165.9 | 34.6 | 29.7 | 6.2 | 283.9 | 59.2 | - | - | 74 | 8.0 | 9.3 | Mild |
| 2 | 264.4 | 55.3 | 3.6 | 0.8 | 210.4 | 44.0 | - | - | 246 | 8.0 | 30.9 | Severe |
| 3 | 183.9 | 40.4 | 19.9 | 4.4 | 251.4 | 55.2 | - | - | 89 | 7.6 | 11.7 | Mild |
| 4 | 156.9 | 45.6 | 4.0 | 1.2 | 177.7 | 51.6 | 5.5 | 1.6 | 72 | 5.7 | 12.6 | Mild |
| 5 | 73.9 | 16.1 | 6.1 | 1.3 | 204.6 | 44.6 | 173.7 | 37.9 | 17 | 7.6 | 2.2 | Healthy |
| 6 | 80.5 | 15.2 | 2.4 | 0.4 | 189.2 | 35.6 | 258.8 | 48.8 | 18 | 8.8 | 2.0 | Healthy |
| 7 | 185.4 | 44.5 | 0.4 | 0.1 | 230.7 | 55.4 | - | - | 48 | 6.9 | 6.9 | Mild |
| 10 | 59.7 | 19.7 | 9.8 | 3.2 | 143.3 | 47.7 | 89.6 | 29.6 | 36 | 5.0 | 7.1 | Mild |
| 13 | 195.1 | 59.5 | 0.8 | 0.2 | 121.0 | 36.9 | 10.9 | 3.3 | 91 | 5.5 | 16.7 | Moderate |
| Total | 1365.7 | 36.0 | 76.7 | 2.0 | 1812.2 | 47.8 | 538.5 | 14.2 | 691 | 63.2 | 10.9 | Mild |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrer-Lluis, I.; Castillo-Escario, Y.; Montserrat, J.M.; Jané, R. SleepPos App: An Automated Smartphone Application for Angle Based High Resolution Sleep Position Monitoring and Treatment. Sensors 2021, 21, 4531. https://doi.org/10.3390/s21134531
Ferrer-Lluis I, Castillo-Escario Y, Montserrat JM, Jané R. SleepPos App: An Automated Smartphone Application for Angle Based High Resolution Sleep Position Monitoring and Treatment. Sensors. 2021; 21(13):4531. https://doi.org/10.3390/s21134531
Chicago/Turabian StyleFerrer-Lluis, Ignasi, Yolanda Castillo-Escario, Josep Maria Montserrat, and Raimon Jané. 2021. "SleepPos App: An Automated Smartphone Application for Angle Based High Resolution Sleep Position Monitoring and Treatment" Sensors 21, no. 13: 4531. https://doi.org/10.3390/s21134531