
Quantitative Analysis of Real-Time Infrared Thermography for the Assessment of Lumbar Sympathetic Blocks: A Preliminary Study


 ,
,  , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Study
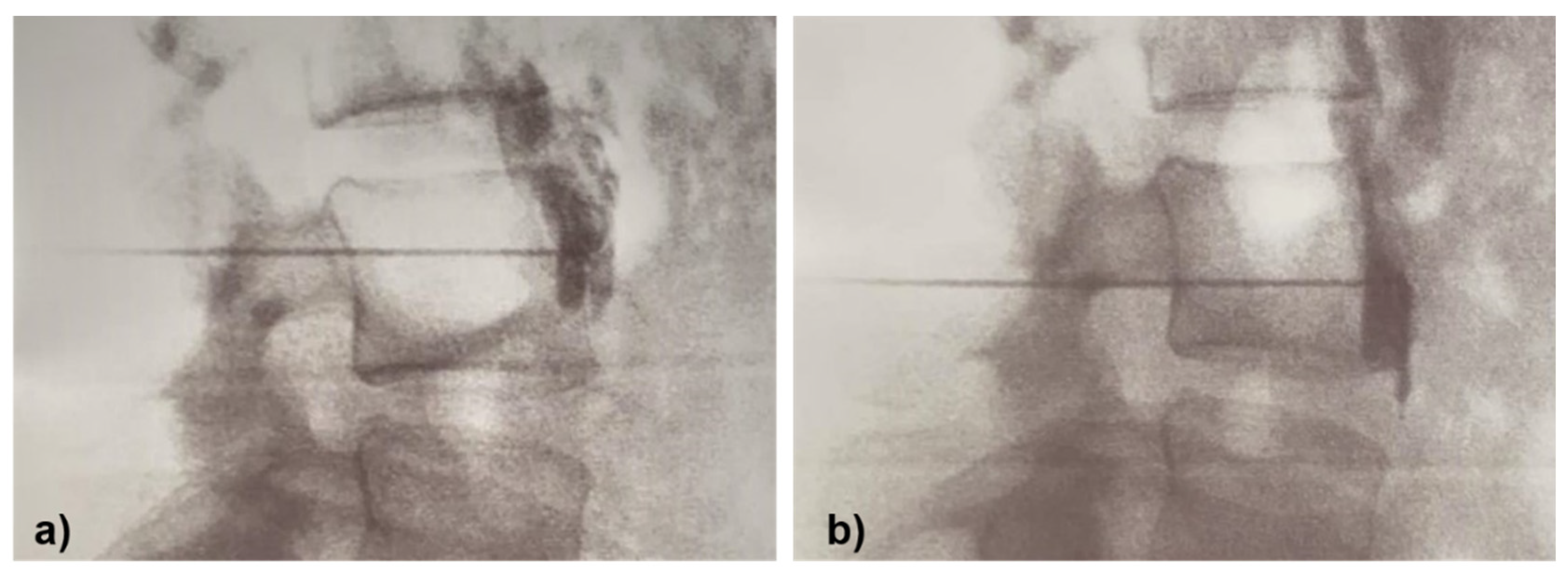
2.2. Lumbar Sympathetic Block Procedure
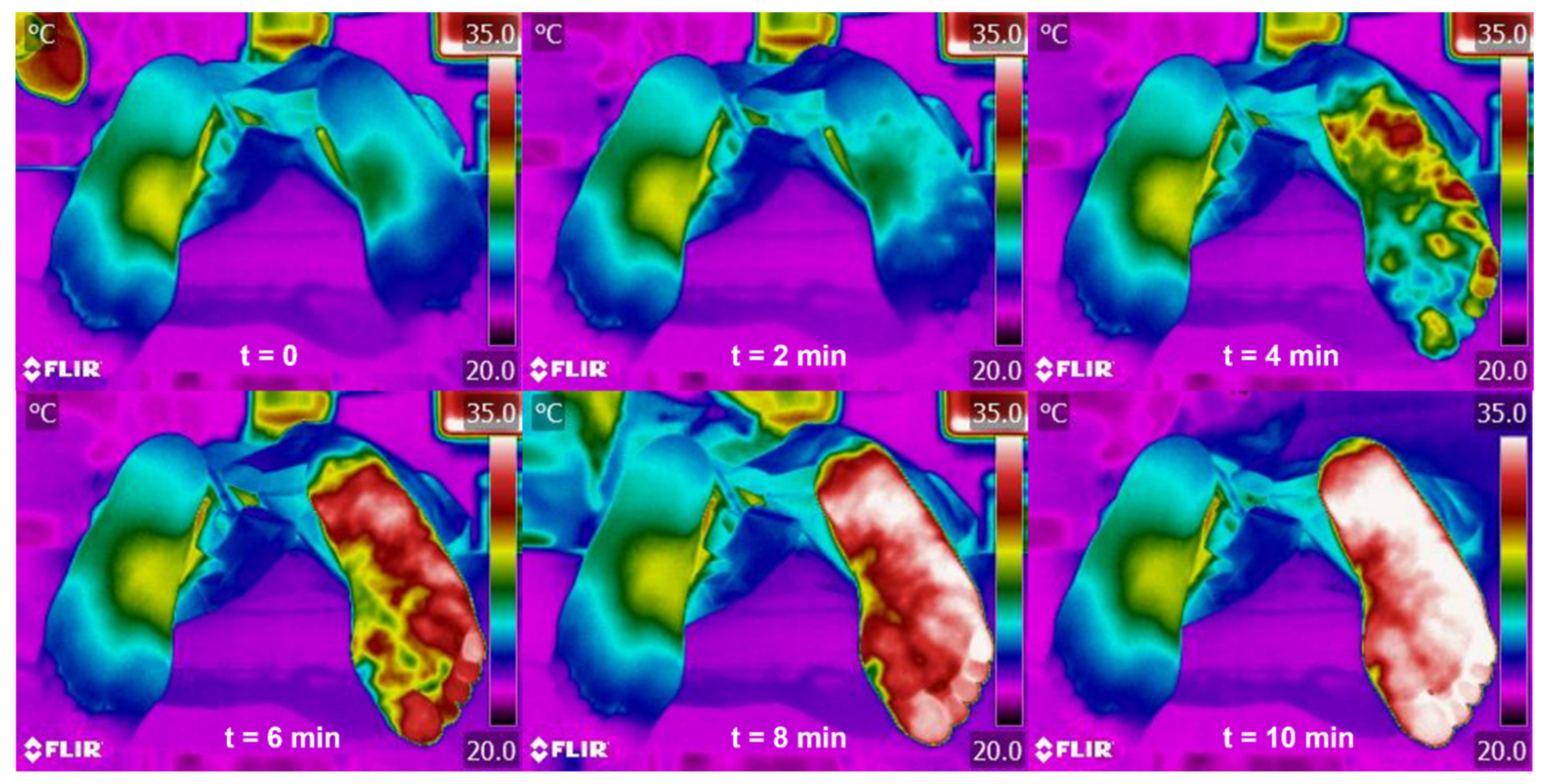
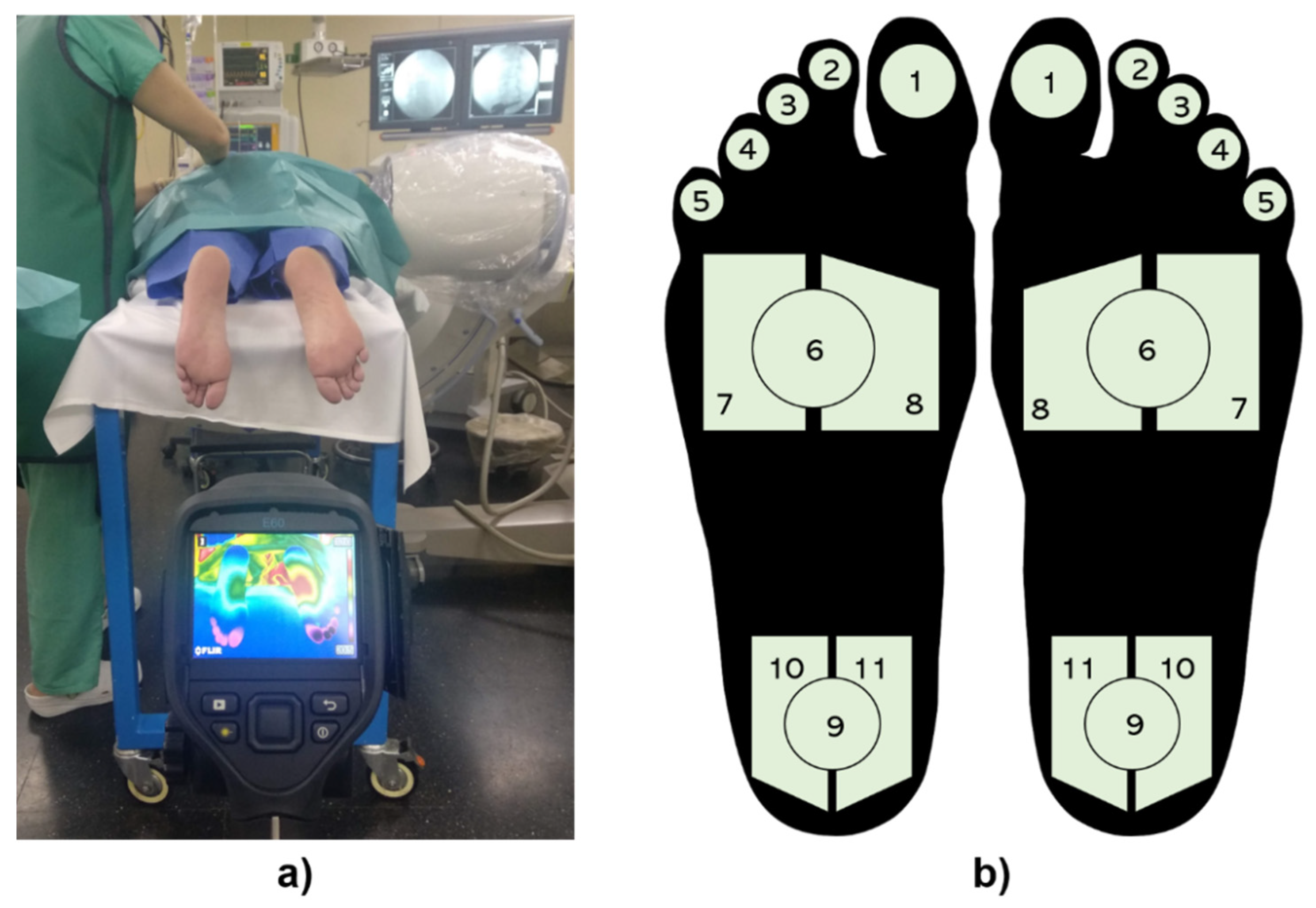
2.3. Thermal Data Acquisition
2.4. Regions of Interest
2.5. Statistical Analysis
3. Results
3.1. Medical Classification in Real Time Using Infrared Thermography
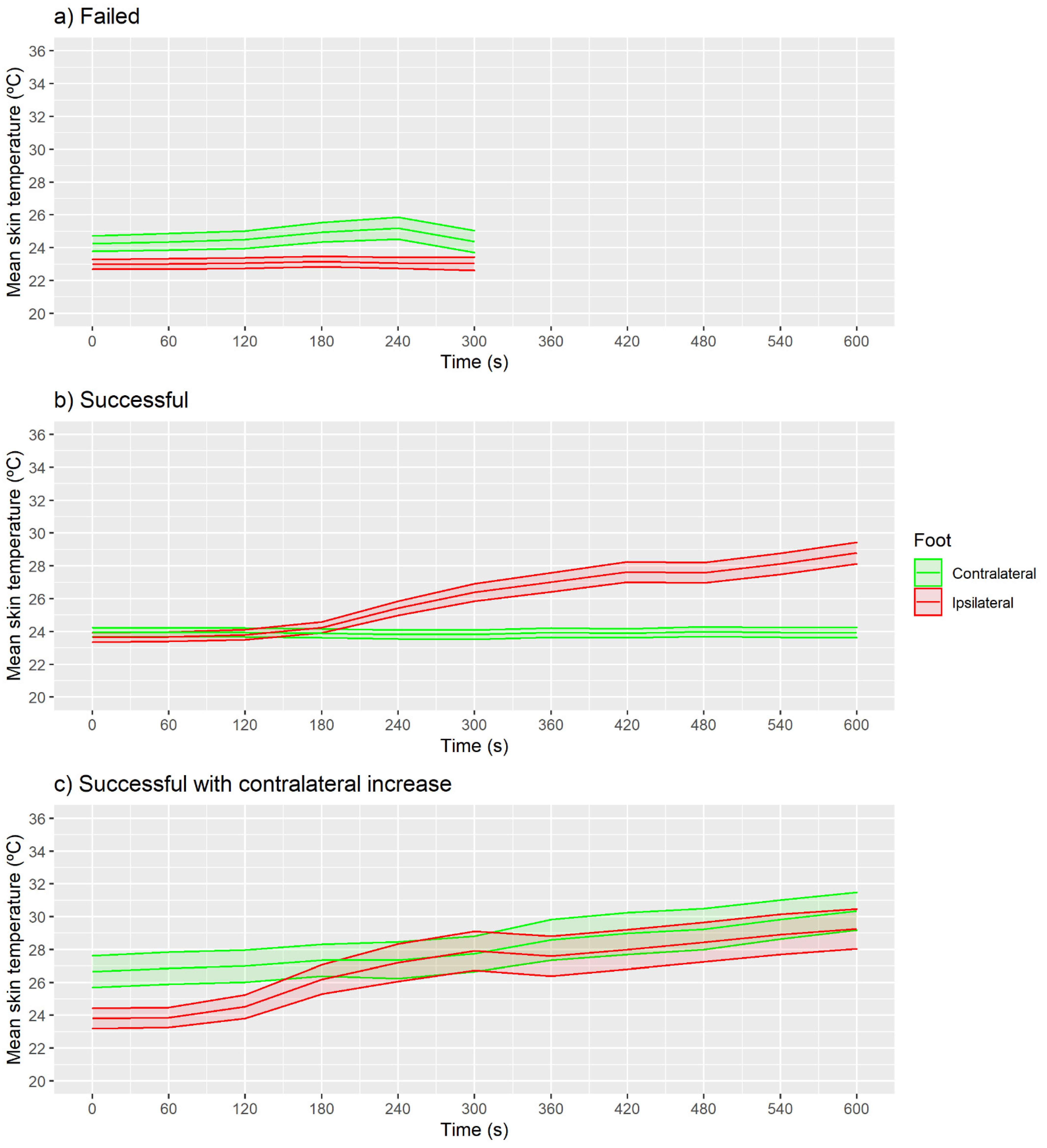
3.2. Quantification of Mean Skin Temperature
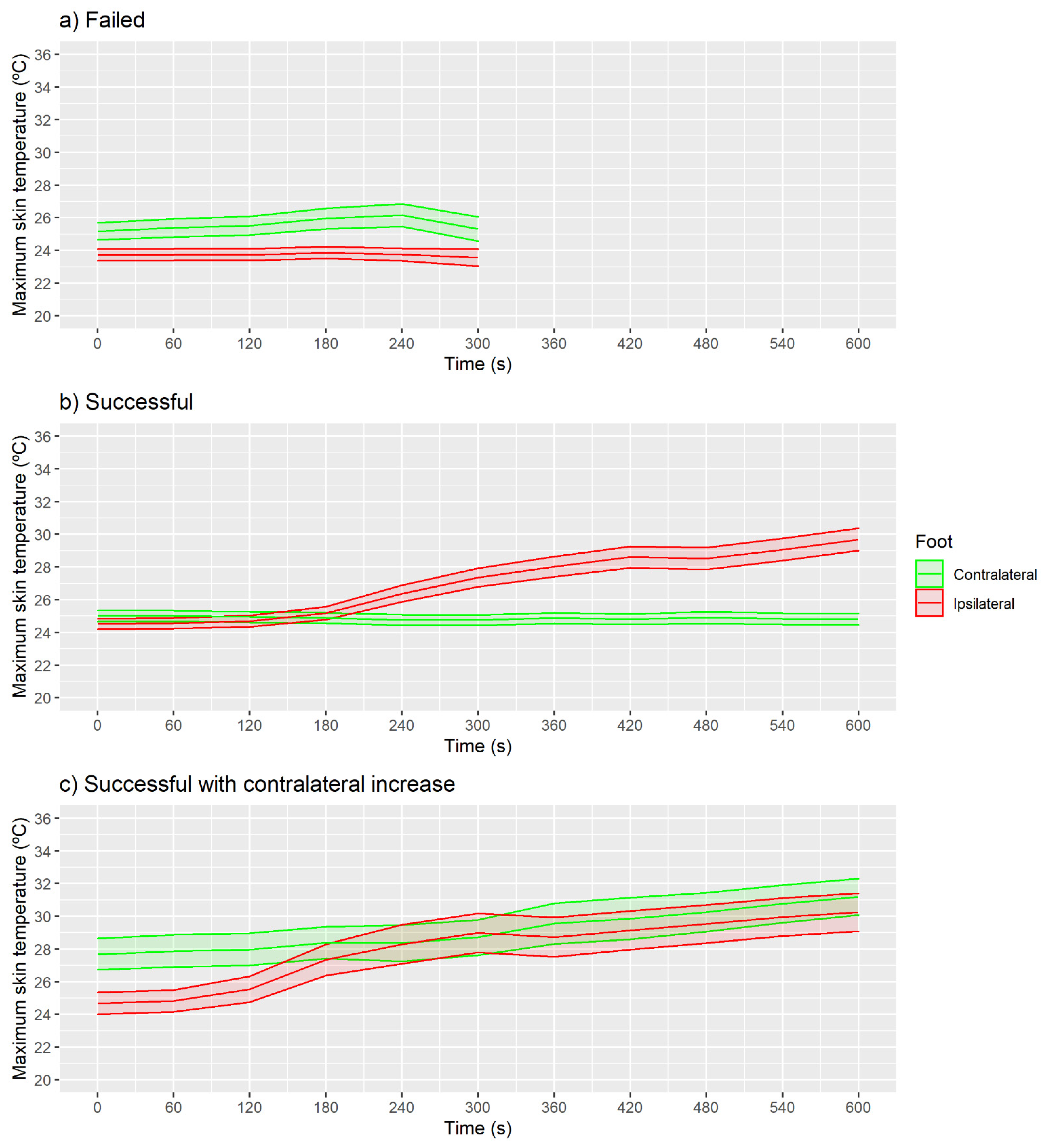
3.3. Quantification of Maximum Skin Temperature
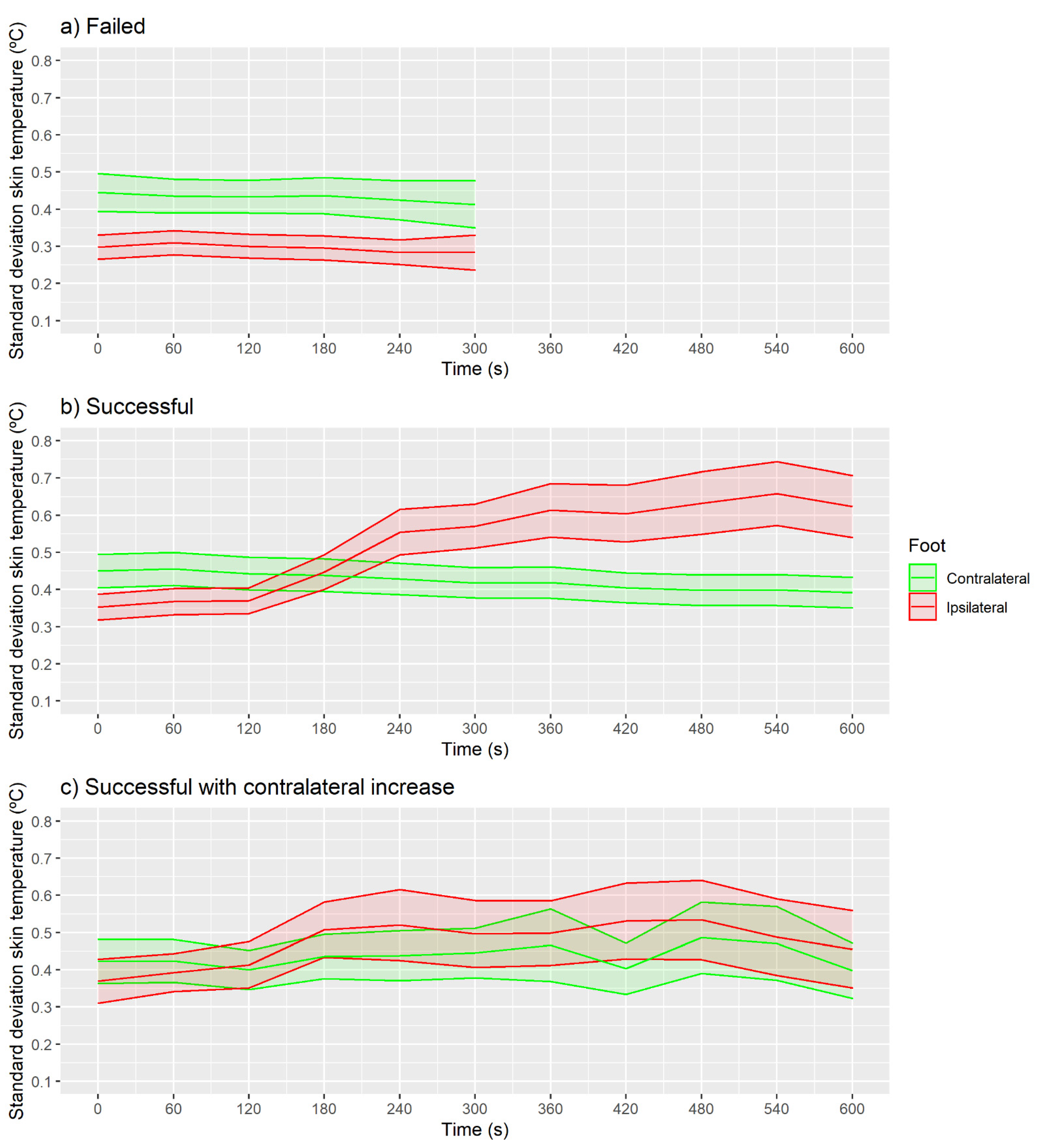
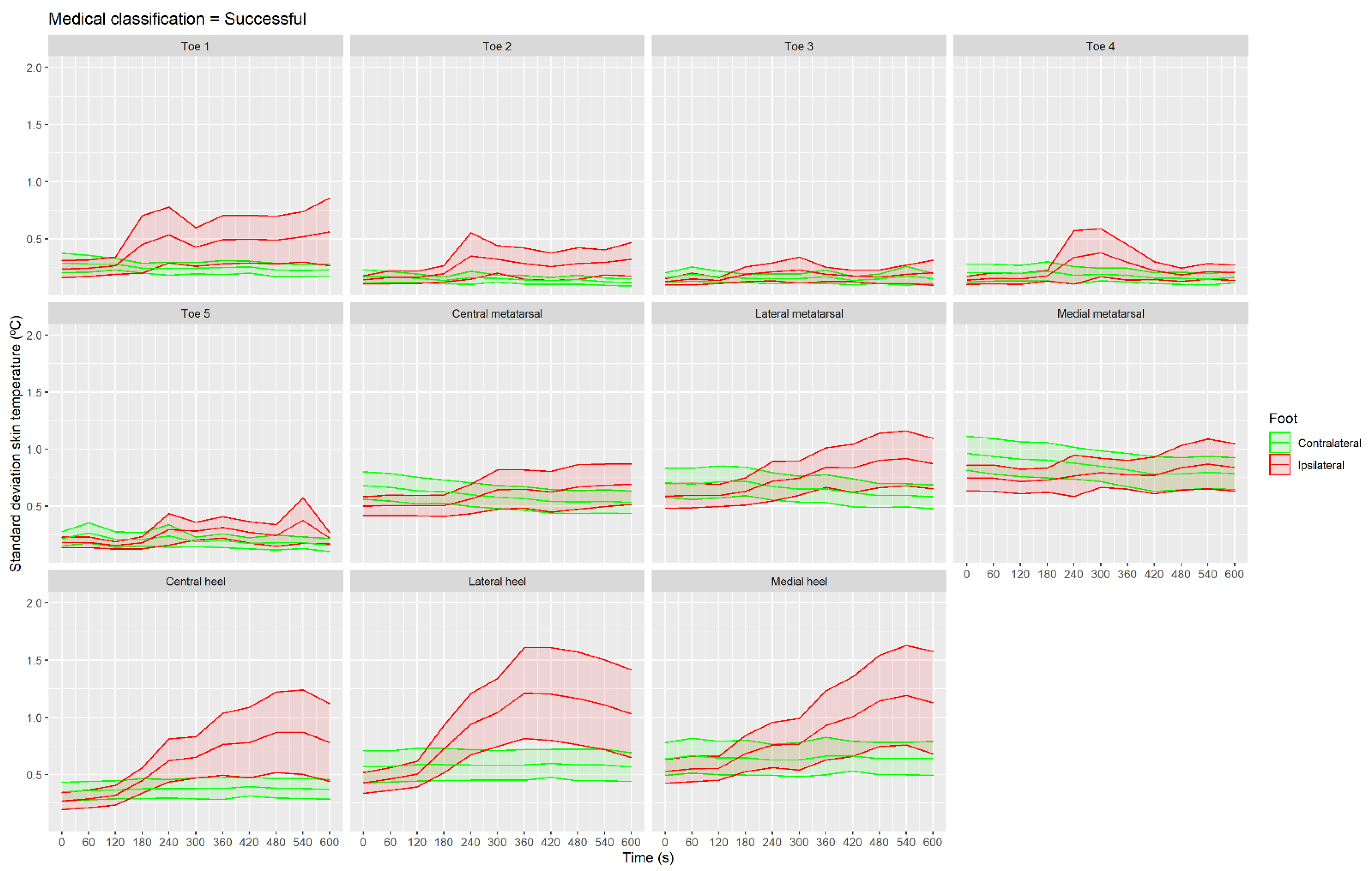
3.4. Quantification of Standard Deviation Skin Temperature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harden, R.N.; Oaklander, A.L.; Burton, A.W.; Perez, R.S.G.M.; Richardson, K.; Swan, M.; Barthel, J.; Costa, B.; Graciosa, J.R.; Bruehl, S. Complex regional pain syndrome: Practical diagnostic and treatment guidelines, 4th edition. Pain Med. 2013, 14, 180–229. [Google Scholar] [CrossRef] [Green Version]
- Shim, H.; Rose, J.; Halle, S.; Shekane, P. Complex regional pain syndrome: A narrative review for the practising clinician. Br. J. Anaesth. 2019, 123, e424–e433. [Google Scholar] [CrossRef]
- Gierthmühlen, J.; Maier, C.; Baron, R.; Tölle, T.; Treede, R.D.; Birbaumer, N.; Huge, V.; Koroschetz, J.; Krumova, E.K.; Lauchart, M.; et al. Sensory signs in complex regional pain syndrome and peripheral nerve injury. Pain 2012, 153, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Marinus, J.; Moseley, G.L.; Birklein, F.; Baron, R.; Maihöfner, C.; Kingery, W.S.; van Hilten, J.J. Clinical features and pathophysiology of complex regional pain syndrome. Lancet Neurol. 2011, 10, 637–648. [Google Scholar] [CrossRef] [Green Version]
- Borchers, A.T.; Gershwin, M.E. Complex regional pain syndrome: A comprehensive and critical review. Autoimmun. Rev. 2014, 13, 242–265. [Google Scholar] [CrossRef] [PubMed]
- Allen, G.; Galer, B.S.; Schwartz, L. Epidemiology of complex regional pain syndrome: A retrospective chart review of 134 patients. Pain 1999, 80, 539–544. [Google Scholar] [CrossRef]
- Sandroni, P.; Benrud-Larson, L.M.; McClelland, R.L.; Low, P.A. Complex regional pain syndrome type I: Incidence and prevalence in Olmsted county, a population-based study. Pain 2003, 103, 199–207. [Google Scholar] [CrossRef]
- De Mos, M.; de Bruijn, A.G.J.; Huygen, F.J.P.M.; Dieleman, J.P.; Stricker, B.H.C.; Sturkenboom, M.C.J.M. The incidence of complex regional pain syndrome: A population-based study. Pain 2007, 129, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Ott, S.; Maihöfner, C. Signs and Symptoms in 1043 Patients with Complex Regional Pain Syndrome. J. Pain 2018, 19, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Mouraux, D.; Lenoir, C.; Tuna, T.; Brassinne, E. The long-term effect of complex regional pain syndrome type 1 on disability and quality of life after foot injury. Disabil. Rehabil. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Van Velzen, G.A.; Perez, R.S.; van Gestel, M.A.; Huygen, F.J.; van Kleef, M.; van Eijs, F.; Dahan, A.; van Hilten, J.J.; Marinus, J. Health-related quality of life in 975 patients with complex regional pain syndrome type 1. Pain 2014, 155, 629–634. [Google Scholar] [CrossRef]
- Rand, S.E.; Basu, S.; Khalid, S. Complex Regional Pain Syndrome: Current Diagnostic and Treatment Considerations. Curr. Sports Med. Rep. 2019, 18, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Bruehl, S. An update on the pathophysiology of complex regional pain syndrome. Anesthesiology 2010, 113, 713–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knudsen, L.F.; Terkelsen, A.J.; Drummond, P.D.; Birklein, F. Complex regional pain syndrome: A focus on the autonomic nervous system. Clin. Auton. Res. 2019, 29, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Birklen, F.; Dimova, V. Complex regional pain syndrome up-to-date. Pain Rep. 2017, 624, 1–8. [Google Scholar] [CrossRef]
- Cutts, S.; Gangoo, S.; Srinivasan, S.H.; Pasapula, C.; Power, D.; Modi, N. Complex regional pain syndrome: An evolving perspective. Postgrad. Med. J. 2020, 97, 250–255. [Google Scholar] [CrossRef]
- Money, S. Pathophysiology of Complex Regional Pain Syndrome and Treatment: Recent Advancements. Curr. Emerg. Hosp. Med. Rep. 2019, 7, 203–207. [Google Scholar] [CrossRef]
- Mesa, J.M.G.; Granados, E.O.; Del Valle Hoyos, M.; Rivera, M. Bloqueo simpático lumbar. Rev. Soc. Esp. Dolor 2013, 20, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Day, M. Sympathetic Blocks: The Evidence. Pain Pract. 2008, 8, 98–109. [Google Scholar] [CrossRef]
- Varrassi, G.; Paladini, A.; Marinangeli, F.; Racz, G. Neural Modulation by Blocks and Infusions. Pain Pract. 2006, 6, 34–38. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, N.E.; Wand, B.M.; Gibson, W.; Carr, D.B.; Birklein, F.; Stanton, T.R. Local anaesthetic sympathetic blockade for complex regional pain syndrome. Cochrane Database Syst. Rev. 2016, 7, 1–54. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Salmasi, V.; You, J.; Grille, M.; Yang, D.; Mascha, E.J.; Cheng, O.T.; Zhao, F.; Rosenquist, R.W. Outcomes of Sympathetic Blocks in the Management of Complex Regional Pain Syndrome: A Retrospective Cohort Study. Anesthesiology 2019, 131, 883–893. [Google Scholar] [CrossRef] [Green Version]
- An, J.W.; Koh, J.C.; Sun, J.M.; Park, J.Y.; Choi, J.B.; Shin, M.J.; Lee, Y.W. Clinical Identification of the Vertebral Level at Which the Lumbar Sympathetic Ganglia Aggregate. Korean J. Pain 2016, 29, 103–109. [Google Scholar] [CrossRef]
- Qian, S.; Sengupta, V.; Urbiztondo, N.; Haider, N. Lumbar Sympathetic Block. In Deer’s Treatment of Pain: An Illustrated Guide for Practitioners; Deer, T.R., Pope, J.E., Lamer, T.J., Provenzano, D., Eds.; Springer International Publishing: Cham, Switerland, 2019; pp. 467–475. ISBN 978-3-030-12281-2. [Google Scholar]
- Gofeld, M.; Shankar, H.; Benzon, H.T. Fluoroscopy and ultrasound-guided sympathetic blocks: Stellate ganglion, lumbar sympathetic blocks, and visceral sympathetic blocks. In Essentials of Pain Medicine; Benzon, H.T., Raja, S.N., Liu, S.S., Fishman, S.M., Cohen, S.P., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 789–804.e2. [Google Scholar]
- Zhu, X.; Kohan, L.R.; Morris, J.D.; Hamill-Ruth, R.J. Sympathetic blocks for complex regional pain syndrome: A survey of pain physicians. Reg. Anesth. Pain Med. 2019, 44, 736–741. [Google Scholar] [CrossRef]
- Żyluk, A.; Puchalski, P. Effectiveness of complex regional pain syndrome treatment: A systematic review. Neurol. Neurochir. Pol. 2018, 52, 326–333. [Google Scholar] [CrossRef]
- Abramov, R. Lumbar Sympathetic Treatment in the Management of Lower Limb Pain. Curr. Pain Headache Rep. 2014, 18. [Google Scholar] [CrossRef]
- Kim, W.O.; Yoon, K.B.; Kil, H.K.; Yoon, D.M. Chemical lumbar sympathetic block in the treatment of plantar hyperhidrosis: A study of 69 patients. Dermatol. Surg. Off. Publ. Am. Soc. 2008, 34, 1340–1345. [Google Scholar] [CrossRef]
- Yoshida, W.B.; Cataneo, D.C.; Bomfim, G.A.Z.; Hasimoto, E.; Cataneo, A.J.M. Chemical lumbar sympathectomy in plantar hyperhidrosis. Clin. Auton. Res. Off. J. Clin. Auton. Res. Soc. 2010, 20, 113–115. [Google Scholar] [CrossRef]
- Wu, C.L.; Marsh, A.; Dworkin, R.H. The role of sympathetic nerve blocks in herpes zoster and postherpetic neuralgia. Pain 2000, 87, 121–129. [Google Scholar] [CrossRef]
- Cheng, J.; Daftari, A.; Zhou, L. Sympathetic blocks provided sustained pain relief in a patient with refractory painful diabetic neuropathy. Case Rep. Anesthesiol. 2012, 2012, 285328. [Google Scholar] [CrossRef] [Green Version]
- Gunduz, O.H.; Kenis-Coskun, O. Ganglion blocks as a treatment of pain: Current perspectives. J. Pain Res. 2017, 10, 2815–2826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, P.M.; Zurakowsi, D.; Berde, C.B.; Sethna, N.F. Lumbar sympathetic blockade in children with complex regional pain syndromes: A double blind placebo-controlled crossover trial. Anesthesiology 2010, 111, 372–380. [Google Scholar] [CrossRef] [Green Version]
- Rocco, A.G.; Kaul, A.F.; Reisman, R.M.; Gallo, J.P.; Lief, P.A. A comparison of regional intravenous guanethidine and reserpine in reflex sympathetic dystrophy a controlled, randomized, double-blind crossover study. Clin. J. Pain 1989, 5, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, K.R.; Verma, V.K.; Chavan, S.K.; Joshi, S.D.; Joshi, S.S. The morphology of lumbar sympathetic trunk in humans: A cadaveric study. Folia Morphol. 2013, 72, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Park, S.Y.; Nahm, F.S.; Kim, Y.C.; Lee, S.C.; Sim, S.E.; Lee, S.J. The cut-off rate of skin temperature change to confirm successful lumbar sympathetic block. J. Int. Med. Res. 2010, 38, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.; Lee, C.; Kim, Y.; Lee, S.; Shankar, H.; Moon, J. Ultrasound-Assisted Versus Fluoroscopic-Guided Lumbar Sympathetic Ganglion Block: A Prospective and Randomized Study. Chronic Pain Med. 2018, 126, 1362–1368. [Google Scholar] [CrossRef]
- Schmid, M.R.; Kissling, R.O.; Curt, A.; Jaschko, G. Sympathetic Skin Response: Monitoring of CT-guided Lumbar Sympathetic Blocks. Vasc. Interv. Radiol. 2006, 241, 595–602. [Google Scholar] [CrossRef]
- Sze, D.Y.; Mackey, S.C. MR Guidance of Sympathetic Nerve Blockade: Measurement of Vasomotor Response Initial Experience in Seven Patients. Radiology 2002, 223, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Punj, J.; Marada, S. Ultrasound lymbar sympathetic block: Out of plane approach with insulated stimulation needle. Case series of three patients. Indian J. Anaesth. 2020, 64, 148–150. [Google Scholar] [CrossRef]
- Lee, Y.; Lee, C.J.; Choi, E.; Lee, P.B.; Lee, H.J.; Nahm, F.S. Lumbar sympathetic block with botulinum toxin type A and type B for the complex regional pain syndrome. Toxins 2018, 10, 164. [Google Scholar] [CrossRef] [Green Version]
- Marhofer, D.; Marhofer, P.; Kettner, S.C.; Fleischmann, E.; Prayer, D.; Schernthaner, M.; Lackner, E.; Willschke, H.; Schwetz, P.; Zeitlinger, M. Magnetic resonance imaging analysis of the spread of local anesthetic solution after ultrasound-guided lateral thoracic paravertebral blockade: A volunteer study. Anesthesiology 2013, 118, 1106–1112. [Google Scholar] [CrossRef]
- Gungor, S.; Rana, B.; Fields, K.; Bae, J.J.; Mount, L.; Buschiazzo, V. Changes in the Skin Conductance Monitor as an End Point for Sympathetic Nerve Blocks. Pain Med. 2017, 18, 2187–2197. [Google Scholar] [CrossRef] [PubMed]
- Wasner, G.; Schattschneider, J.; Heckmann, K.; Maier, C.; Baron, R. Vascular abnormalities in reflex sympathetic dystrophy (CRPS I): Mechanisms and diagnostic value. Brain 2001, 124, 587–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joo, E.Y.; Kong, Y.G.; Lee, J.; Cho, H.S.; Kim, S.H.; Suh, J.H. Change in pulse transit time in the lower extremity after lumbar sympathetic ganglion block: An early indicator of successful block. J. Int. Med. Res. 2017, 45, 203–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.Y.; Baek, H.J.; Park, K.S.; Kim, Y.C. Photoplethysmographic signals to predict the success of lumbar sympathetic blockade for lower extremity pain. J. Int. Med. Res. 2014, 42, 938–948. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Sim, W.S.; Lee, D.W.; Lee, J.Y. Correlation between paravertebral spread of injectate and clinical efficacy in lumbar transforaminal block. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef]
- Breivik, H.; Cousins, M.J. Sympathetic Neural Blockade of Upper and Lower Extremity. Anesthesya Key [internet]. 2012. Available online: https://aneskey.com/sympathetic-neural-blockade-of-upper-and-lower-extremity/ (accessed on 13 April 2021).
- Hermanns, H.; Werdehausen, R.; Hollmann, M.; Stevens, M.F. Assessment of skin temperature during regional anaesthesia—What the anaesthesiologist should know. Acta Anaesthesiol. Scand. 2018, 62, 1280–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lossius, B.Y.K.; Eriksen, M.; Walle, L. Fluctuations in blood flow to acral skin in humans: Connection with heart rate and blood pressure variability. J. Physiol. 1993, 460, 641–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cousins, M.J.; Bridenbaugh, P.O. Cousins and Bridenbaugh’s Neural blockade in Clinical Anesthesia and Pain Medicine; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; ISBN 9780781773881. [Google Scholar]
- Medel Rebollo, J.; Ribera Canudas, M.V.; Mesas Idáñez, A.; Márquez Martínez, E.; Martínez Ripol, P.; Candela Custardoy, A.; Paños Gozalo, M.; Gili Grahit, S. Técnicas mínimamente invasivas en el tratamiento del dolor crónico. Semin. Fund. Española Reumatol. 2013, 14, 135–141. [Google Scholar] [CrossRef]
- Borchers, A.T.; Gershwin, M.E. The clinical relevance of complex regional pain syndrome type I: The Emperor’s New Clothes. Autoimmun. Rev. 2017, 16, 22–33. [Google Scholar] [CrossRef]
- Gatt, A.; Formosa, C.; Cassar, K.; Camilleri, K.P.; De Raffaele, C.; Mizzi, A.; Azzopardi, C.; Mizzi, S.; Falzon, O.; Cristina, S.; et al. Thermographic Patterns of the Upper and Lower Limbs: Baseline Data. Int. J. Vasc. Med. 2015, 2015, 831369. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.C.M.; Castro, H.A.; Carvalho, L.C.; Chaves, É.C.L.; Ruela, L.O.; Iunes, D.H. Reliability of Infrared Thermography Images in the Analysis of the Plantar Surface Temperature in Diabetes Mellitus. J. Chiropr. Med. 2018, 17, 30–35. [Google Scholar] [CrossRef]
- Quesada, J.I.P. Application of Infrared Thermography in Sports Science; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; ISBN 9783319474090. [Google Scholar]
- MacRae, B.A.; Annaheim, S.; Spengler, C.M.; Rossi, R.M. Skin Temperature Measurement Using Contact Thermometry: A systematic review of setup variables and their effects on measured values. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammer, K.; Ring, E.F.J. The Thermal Human Body. A Practical Guide to Thermal Imaging; CRC Press: Boca Raton, FL, USA, 2019; ISBN 978-0-429-01998-2/978-981-4745-82-6. [Google Scholar]
- Priego Quesada, J.I.; Martínez Guillamón, N.; Cibrián Ortiz de Anda, R.M.; Psikuta, A.; Annaheim, S.; Rossi, R.M.; Corberán Salvador, J.M.; Pérez-Soriano, P.; Salvador Palmer, R. Effect of perspiration on skin temperature measurements by infrared thermography and contact thermometry during aerobic cycling. Infrared Phys. Technol. 2015, 72, 68–76. [Google Scholar] [CrossRef]
- Lahiri, B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef]
- Kirimtat, A.; Krejcar, O.; Selamat, A. A Mini-review of Biomedical Infrared Thermography (B-IRT). In Proceedings of the Bioinformatics and Biomedical Engineering, IWBBIO 2019, Granada, Spain, 8–10 May 2019; Lecture Notes in Computer Science. Rojas, I., Valenzuela, O., Rojas, F., Ortuño, F., Eds.; Springer International Publishing: Cham, Switerland, 2019; pp. 514–523. [Google Scholar]
- Haren, F.G.A.M.; Van Kadic, L.; Driessen, J.J. Skin temperature measured by infrared thermography after ultrasound-guided blockade of the sciatic nerve. Acta Anaesthesiol. Scand. 2013, 57, 1111–1117. [Google Scholar] [CrossRef]
- Bouvet, L.; Roukhomovsky, M.; Desgranges, F.; Allaouchiche, B. Infrared thermography to assess dermatomal levels of labor epidural analgesia with 1 mg/mL ropivacaine plus 0.5 µg/mL sufentanil: A prospective cohort study. Int. J. Obstet. Anesth. 2019, 8–13. [Google Scholar] [CrossRef]
- Werdehausen, R.; Braun, S.; Hermanns, H.; Freynhagen, R.; Lipfert, P.; Ph, D.; Stevens, M.F. Uniform Distribution of Skin-Temperature Increase After Different Regional-Anesthesia Techniques of the Lower Extremity. Reg. Anesth. Pain Med. 2007, 32, 73–78. [Google Scholar] [CrossRef]
- Kim, Y.C.; Bahk, J.; Lee, S.C.; Lee, Y. Infrared Thermographic Imaging in the assessment of successful block on lumbar sympathetic ganglion. Yonsei Med. J. 2003, 44, 119–124. [Google Scholar] [CrossRef]
- Fernández-cuevas, I.; Carlos, J.; Marins, B.; Arnáiz, J.; María, P.; Carmona, G.; Piñonosa, S.; García-concepción, M.Á.; Sillero-quintana, M. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Phys. Technol. 2015, 71, 28–55. [Google Scholar] [CrossRef]
- Marins, J.C.B.; Moreira, D.G.; Cano, S.P.; Quintana, M.S.; Soares, D.D.; De Andrade Fernandes, A.; Da Silva, F.S.; Costa, C.M.A.; Dos Santos Amorim, P.R. Time required to stabilize thermographic images at rest. Infrared Phys. Technol. 2014, 65, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Vollmer, M.; Möllmann, K. Infrared Thermal Imaging: Fundamentals, Research and Applications; Wiley-VCH: Weinheim, Germany, 2010; ISBN 9783527403820. [Google Scholar]
- Steketee, J. Spectral emissivity of skin and pericardium, Physics in Medicine and Biology. Phys. Med. Biol. 1973, 18, 686–694. [Google Scholar] [CrossRef]
- Gauci, J.; Falzon, O.; Formosa, C.; Gatt, A.; Ellul, C.; Mizzi, S.; Mizzi, A.; Sturgeon Delia, C.; Cassar, K.; Chockalingam, N.; et al. Automated Region Extraction from Thermal Images for Peripheral Vascular Disease Monitoring. J. Healthc. Eng. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Priego Quesada, J.I.; Kunzler, M.R.; Carpes, F.P. Methodological Aspects of Infrared Thermography in Human Assessment. In Application of Infrared Thermography in Sports Science; Priego Quesada, J.I., Ed.; Springer International Publishing: Cham, Switerland, 2017; pp. 49–79. ISBN 978-3-319-47410-6. [Google Scholar]
- Sun, P.; Jao, S.-H.E.; Cheng, C.-K. Assessing foot temperature using infrared thermography. Foot Ankle Int. 2005, 26. [Google Scholar] [CrossRef]
- Formenti, D.; Ludwig, N.; Rossi, A.; Trecroci, A.; Alberti, G.; Gargano, M.; Merla, A.; Ammer, K.; Caumo, A. Is the maximum value in the region of interest a reliable indicator of skin temperature? Infrared Phys. Technol. 2018, 94, 299–304. [Google Scholar] [CrossRef]
- Requena-Bueno, L.; Priego-Quesada, J.I.; Jimenez-Perez, I.; Gil-Calvo, M.; Pérez-Soriano, P. Validation of ThermoHuman automatic thermographic software for assessing foot temperature before and after running. J. Therm. Biol. 2020, 92. [Google Scholar] [CrossRef]
- Gauci, J.; Falzon, O.; Camilleri, K.; Formosa, C.; Gatt, A.; Ellul, C.; Mizzi, S.; Mizzi, A.; Cassar, K.; Chockalingam, N. Automated Segmentation and Temperature Extraction from Thermal Images of Human Hands, Shins and Feet. IFMBE Proc. 2016, 57, 275–280. [Google Scholar] [CrossRef]
- Silbergleit, R.; Mehta, B.A.; Sanders, W.P.; Talati, S.J. Imaging-guided injection techniques with fluoroscopy and CT for spinal pain management. Radiographics 2001, 21, 922–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, K.M.; Frank, S.M.; Raja, S.N.; El-Rahmany, H.K.; Kim, L.J.; Vu, B. Lumbar sympathetic block for sympathetically maintained pain: Changes in cutaneous temperatures and pain perception. Anesth. Analg. 2000, 90, 1396–1401. [Google Scholar] [CrossRef]
- Snell, R.S. Clinical Anatomy; Snell Clinical Anatomy; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004; ISBN 9780781743150. [Google Scholar]
- Niu, H.H.; Lui, P.W.; Hu, J.S.; Ting, C.K.; Yin, Y.C.; Lo, Y.L.; Liu, L.; Lee, T.Y. Thermal symmetry of skin temperature: Normative data of normal subjects in Taiwan. Zhonghua Yi Xue Za Zhi (Taipei) 2001, 64, 459–468. [Google Scholar]
- Hildebrandt, C.; Raschner, C.; Ammer, K. An overview of recent application of medical infrared thermography in sports medicine in Austria. Sensors 2010, 10, 4700–4715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardasca, R.; Ring, F.; Plassmann, P.; Jones, C. Thermal symmetry of the upper and lower extremities in healthy subjects. Thermol. Int. 2012, 22, 53–60. [Google Scholar]
- Saxena, A.; Raman, V.; Ng, E.Y.K. Study on methods to extract high contrast image in active dynamic thermography. Quant. Infrared Thermogr. J. 2019, 16, 243–259. [Google Scholar] [CrossRef]
- Saxena, A.; Ng, E.Y.K.; Canchi, T.; Lim, J.L.; Beruvar, A.S. A method to produce high contrast vein visualization in active dynamic thermography (ADT). Comput. Biol. Med. 2021, 132, 104309. [Google Scholar] [CrossRef] [PubMed]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cañada-Soriano, M.; Priego-Quesada, J.I.; Bovaira, M.; García-Vitoria, C.; Salvador Palmer, R.; Cibrián Ortiz de Anda, R.; Moratal, D. Quantitative Analysis of Real-Time Infrared Thermography for the Assessment of Lumbar Sympathetic Blocks: A Preliminary Study. Sensors 2021, 21, 3573. https://doi.org/10.3390/s21113573
Cañada-Soriano M, Priego-Quesada JI, Bovaira M, García-Vitoria C, Salvador Palmer R, Cibrián Ortiz de Anda R, Moratal D. Quantitative Analysis of Real-Time Infrared Thermography for the Assessment of Lumbar Sympathetic Blocks: A Preliminary Study. Sensors. 2021; 21(11):3573. https://doi.org/10.3390/s21113573
Chicago/Turabian StyleCañada-Soriano, Mar, José Ignacio Priego-Quesada, Maite Bovaira, Carles García-Vitoria, Rosario Salvador Palmer, Rosa Cibrián Ortiz de Anda, and David Moratal. 2021. "Quantitative Analysis of Real-Time Infrared Thermography for the Assessment of Lumbar Sympathetic Blocks: A Preliminary Study" Sensors 21, no. 11: 3573. https://doi.org/10.3390/s21113573