
Unobtrusive Health Monitoring in Private Spaces: The Smart Home
by
 , , , , and
, , , , and
Ju Wang
1,* ,
,
Nicolai Spicher
1 ,
,
Joana M. Warnecke
1 ,
,
Mostafa Haghi
1 ,
,
Jonas Schwartze
1,2 and
Thomas M. Deserno
1 1
Peter L. Reichertz Institute for Medical Informatics of TU Braunschweig and Hannover Medical School, Muehlenpfordtstr. 23, D-38106 Braunschweig, Lower Saxony, Germany
2
Wohnungsentwicklung und Forschung, Nibelungen-Wohnbau-GmbH, Freyastr. 10, D-38106 Braunschweig, Lower Saxony, Germany
*
Author to whom correspondence should be addressed.
Sensors 2021, 21(3), 864; https://doi.org/10.3390/s21030864
Submission received: 2 December 2020
/
Revised: 8 January 2021
/
Accepted: 23 January 2021
/
Published: 28 January 2021
(This article belongs to the Special Issue Simplified Sensing for Ambient Assisted Living in Smart Homes)
Abstract
:With the advances in sensor technology, big data, and artificial intelligence, unobtrusive in-home health monitoring has been a research focus for decades. Following up our research on smart vehicles, within the framework of unobtrusive health monitoring in private spaces, this work attempts to provide a guide to current sensor technology for unobtrusive in-home monitoring by a literature review of the state of the art and to answer, in particular, the questions: (1) What types of sensors can be used for unobtrusive in-home health data acquisition? (2) Where should the sensors be placed? (3) What data can be monitored in a smart home? (4) How can the obtained data support the monitoring functions? We conducted a retrospective literature review and summarized the state-of-the-art research on leveraging sensor technology for unobtrusive in-home health monitoring. For structured analysis, we developed a four-category terminology (location, unobtrusive sensor, data, and monitoring functions). We acquired 912 unique articles from four relevant databases (ACM Digital Lib, IEEE Xplore, PubMed, and Scopus) and screened them for relevance, resulting in papers analyzed in a structured manner using the terminology. The results delivered 25 types of sensors (motion sensor, contact sensor, pressure sensor, electrical current sensor, etc.) that can be deployed within rooms, static facilities, or electric appliances in an ambient way. While behavioral data (e.g., presence (), time spent on activities ()) can be acquired effortlessly, physiological parameters (e.g., heart rate, respiratory rate) are measurable on a limited scale (). Behavioral data contribute to functional monitoring. Emergency monitoring can be built up on behavioral and environmental data. Acquired physiological parameters allow reasonable monitoring of physiological functions to a limited extent. Environmental data and behavioral data also detect safety and security abnormalities. Social interaction monitoring relies mainly on direct monitoring of tools of communication (smartphone; computer). In summary, convincing proof of a clear effect of these monitoring functions on clinical outcome with a large sample size and long-term monitoring is still lacking.
1. Introduction
Living environments with limited public access, such as a home or a privately-owned car, form private spaces where people spend much time on daily activities [1]. In many cases, private spaces imply far more than ordinary living. For patients with chronic diseases or patients post-operationally discharged, their homes are places for not only living but also rehabilitation, and—in the future—could also facilitate medical diagnosis and therapy [2,3,4]. Health monitoring in private spaces will benefit the subjects who require assistance, such as the elderly, patients, and disabled persons.
The Internet of things (IoT) and ambient assisted living (AAL) enable the sensing of many aspects of our life, particularly including health-relevant information [5]. A sensor-enhanced private space can provide unobtrusive health monitoring. We defined unobtrusive health monitoring as ambient using sensor technology to collect human health-related data without introducing any inconveniences to everyday life [6]. Given this definition, wearable devices are not considered unobtrusive, as the adherence to wearing them introduces an additional burden to the users. Even in the case of a user-friendly integration of the sensors into a smart watch or wristband, they still need to be recharged or configured. Within the framework of unobtrusive health monitoring in private spaces, our previous work investigated the up-to-date research on leveraging sensor technology in smart vehicles [7]. In this work, we extend this thematic series in the framework of unobtrusive health monitoring by focusing on the sensor-enhanced private spaces, namely, smart homes.
A pivotal feature of unobtrusive health monitoring is continuity. Conventional approaches collect health information (e.g., morphological and functional performance assessments) at the point-of-care over time intervals ranging from months to years. In contrast, a smart home can continuously or over shorter time intervals monitor its resident’s health status while the resident is doing daily activities, unaffected by the measurements. This monitoring may capture a comprehensive picture of a person’s health and functional status and critical changes or events [8]. As is known, the activities of daily living (ADLs) reflect the behavioral routines. However, a human may not be able to pay close attention to how well an individual performs the ADLs and therefore spot subtle changes that may signal a pattern of decline [9]. Continuous health monitoring could ensure that subtle changes are not overlooked. Besides, studies have shown that the ambient in-home health monitoring technologies are feasible and well-accepted [10,11].
Smart home research and relevant topics have been reviewed from different perspectives in the past. Demiris et al. categorized health-related smart home technologies into physiological monitoring, functional monitoring or emergency detection and response, safety monitoring and assistance, security monitoring and assistance, social interaction monitoring and assistance, and cognitive and sensory assistance [12]. Majumder et al. analyzed the smart home monitoring technologies for the elderly and summarized the monitoring of resident activity, the home environment, resident health, and home appliances [13]. Liu et al. assessed the level of evidence in using smart home technology to support different health concerns, such as ADL monitoring, chronic obstructive pulmonary disease (COPD), cognitive decline and mental health struggles, fall prevention, and monitoring heart conditions; and concluded that the technology readiness for smart home and health monitoring is still low [14]. Cedillo et al. explored the relation between health concerns and different AAL technology [15]. Rashidi et al. summarized the AAL tools (smart homes, wearable sensors, and robotics) for older adults [16]. Recently, Rodrigues et al. addressed the requirements for the development of smart healthcare environments for physiological and behavior monitoring [17]. Stavropoulos et al. examined IoT wearable sensors and some smart home devices in elderly care, and categorized the sensing approaches according to healthcare aspects, ranging from specific ailments to general eldercare [18]. In addition, the authors proposed a case study classification taxonomy, which can be a reference for similar work.
The concept of unobtrusive health monitoring aims at measuring health parameters without interfering with the subject. However, this concept is not on the focus of existing reviews. A review of the current sensor technology for unobtrusive in-home monitoring is yet in demand. Therefore, this literature review aims to provide a snapshot of the state-of-the-art sensor technology in unobtrusive health monitoring. We focus on the subject groups of the elderly, patients, and disabled individuals, who need to be paid close attention in their everyday lives. In particular, the following questions will be answered: (1) What types of sensors can be used for unobtrusive in-home health data acquisition? (2) Where should the sensors be placed? (3) Which data can be monitored in the smart home? (4) How can the obtained data support the monitoring functions?
2. Methods
2.1. Terminology of Unobtrusive In-Home Health Monitoring
The term ADLs is defined as the self-care activities that are necessary for health maintenance and independent living [19]. Basic and instrumental ADLs (BADLs and IADLs) are the typical classes. The BADLs refer to life-sustaining self-care activities (e.g., feeding, grooming, bathing, dressing, toileting, and ambulation); the IADLs are more complex activities necessary for independent living (e.g., using telephones, preparing meals, shopping, managing finances, taking medications, and driving) [19]. ADLs indicate an individual’s health status, as the performance of ADLs depends on cognitive (e.g., reasoning and planning), motor (e.g., balance and dexterity), and perceptual abilities (e.g., hearing and seeing) [20].
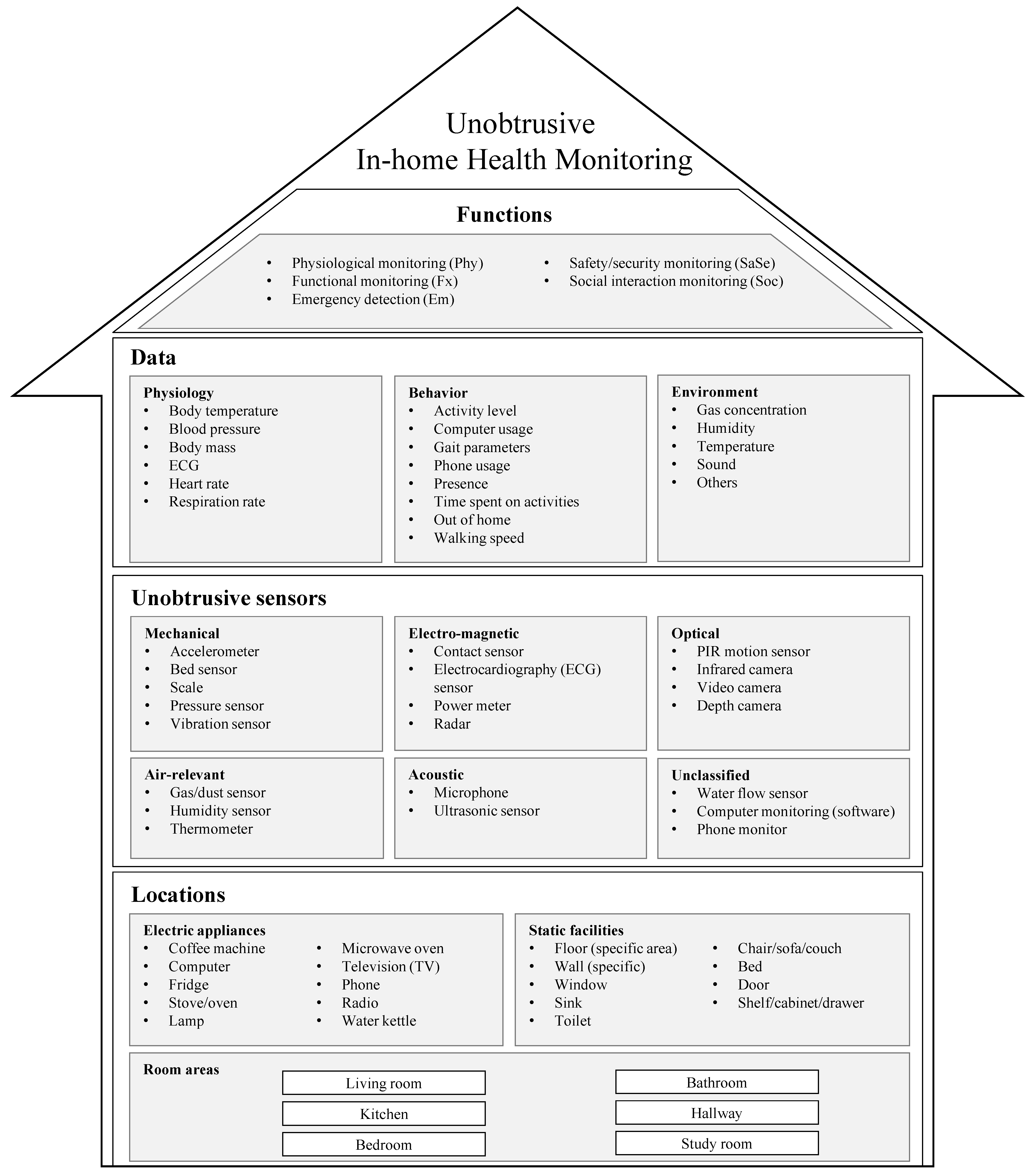
Conventionally, we assess the ability to perform ADLs with clinical instruments, such as the Barthel index or the Lawton IADL scale [21,22]. Interactions with many in-home objects (e.g., toilet, oven, bed, or telephone) are unavoidable while performing ADLs. Thereby, we believe that sensors attached/integrated to these objects can enable automatic assessments of ADLs to a certain extent. To comprehensively understand different approaches, we have to consider the monitoring context, including sensor placement and data sources [23]. Accordingly, we propose a terminology that covers unobtrusive sensors, their locations, the data that can be obtained, and the potential monitoring functions (Figure 1). Hereby the term unobtrusive is regarded as unnoticed—i.e., the acquiring of health data is accomplished while the monitored individual is doing everyday activities as usual. For instance, heart rate can be measured without notice when a person is watching TV while sitting on a sofa integrating capacitive electrocardiography (ECG) electrodes.
- Location refers to the objects where the sensors can be unobtrusively deployed or integrated. It can be broken down into:
- -
- Room areas, which denotes rooms and other large spaces such as a hallway;
- -
- Static facilities, which consist of objects with fixed locations but usually without any electrical supply—e.g., furniture, windows, toilets, and sink;
- -
- Electric appliances have electricity, but may be fixed (e.g, oven) or unfixed (e.g., phone).
- Unobtrusive sensors refer to the sensing devices that can be unobtrusively deployed in the locations introduced above, consisting of mechanical, electro-magnetic, optical, acoustic, and air sensors [13].
- Data are the outputs directly from the sensors or derived values from data processing or analysis. Physiological, behavioral, and environmental data can be acquired from the sensors.
- Functions refer to the possible services that can be delivered through the monitoring system. We formalized the functions based on Demiris’ definitions [12].
- -
- Physiological monitoring (Phy) refers to the data collection and analysis of physiological measurements (e.g., heart rate, respiration rate, and body temperature).
- -
- Functional monitoring (Fx) refers to the data collection and analysis on functional measurements of BADLs and IADLs (e.g., activity level, motion, gait, and meal intake).
- -
- Emergency detection (Em) refers to detecting abnormal or critical situations that need immediate intervention (e.g., falls).
- -
- Safety and security detection (SaSe) refers to the detection of environmental hazards (e.g., fire and gas leak) and human threats (e.g., intruders).
- -
- Social interaction monitoring (Soc) refers to social interactions (e.g., phone calls, visitors, and social activities).
2.2. Literature Retrieval
The search string we developed reflects two aspects (Appendix A):
Unobtrusive monitoring technologies consist of terms on the technologies applied for unobtrusive sensor monitoring, such as “smart home”; “in-home monitoring”; “home-based monitoring”; “continuous assessment”; “ambient assisted living”; “intelligent monitoring.”
People that are monitored consist of the terms on the target groups who need healthcare support in their everyday life, such as “patient”; “disability”; “disabled”; “elderly”; “older people.”
We constructed the search term by connecting the terms within and across each aspect with logic operators OR and AND, respectively. We applied the search string to four databases, i.e., ACM Digital Lib, IEEE Xplore, PubMed, and Scopus. To reflect only up-to-date research, we defined the publishing date span as the last decade (May 2010–April 2020). We restricted the query to results written in English. Subsequently, we combined all returned records, removed duplicates, and screened the titles and abstracts according to the Review Criteria and excluded irrelevant records. Afterward, we analyzed the full texts with the Terminology of Unobtrusive In-Home Health Monitoring.
2.3. Review Criteria
As several persons performed a two-stage review, we defined the following criteria to maintain consistency:
- Inclusion
- -
- Unobtrusive sensors were part of the method;
- -
- The sensors were used to collect either behavioral, physiological, or environmental health-relevant data;
- -
- The monitoring method was implemented in a smart home, either a smart home laboratory or a real living home.
- Exclusion
- -
- No sensor technology was applied;
- -
- Only wearable/implanted sensors were applied;
- -
- Sensor data were not used for health monitoring;
- -
- The work only focused on human–computer interaction;
- -
- The work presented a design/idea only, but no implementation, test, or evaluation;
- -
- Research was not on humans;
- -
- Review/survey/vision papers.
When analyzing the full texts, we focused on extracting three sorts of information, i.e., the types of sensors used in the research and their placement (location), the sensor outputs, including physiological signals/parameters, behavioral and environmental information (data), and the main monitoring functions. Besides, we investigated (i) whether a sensor network was formed and what the communication channel was; (ii) the number of subjects participating in the test/evaluation; (iii) whether the experiment was conducted in a real living environment or a smart home laboratory; and (iv) whether privacy issues were taken into account.
3. Results
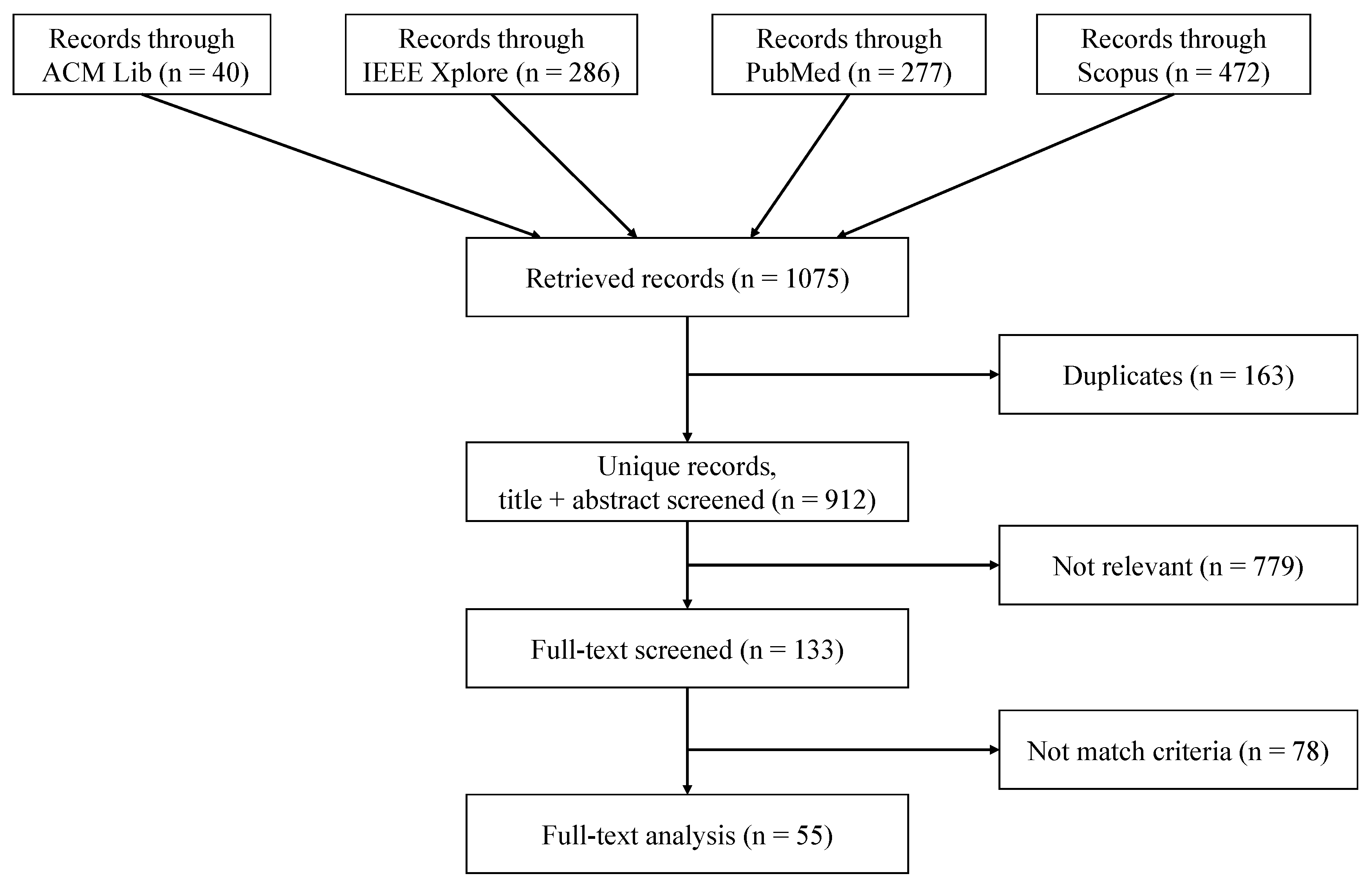
The search string on the four databases resulted in 912 records after removing 163 duplicates, of which 133 papers remained after screening titles and abstracts (Figure 2). After reviewing the full texts, we excluded 78 papers as they did not match the criteria, and finally included 55 papers for in-depth text analysis.
Results of the text analysis are given in Table 1 and Table 2. The included papers are sorted by ascending publish year. With the terminology (Figure 1), we extracted the sensors and their deployed locations (represented with the syntax sensor [location]), the acquired data, and the functions of the monitoring system. Additionally, we also examined the type of sensor network, the subject information, and experiment settings, if the information is available.
3.1. Sensors and Locations
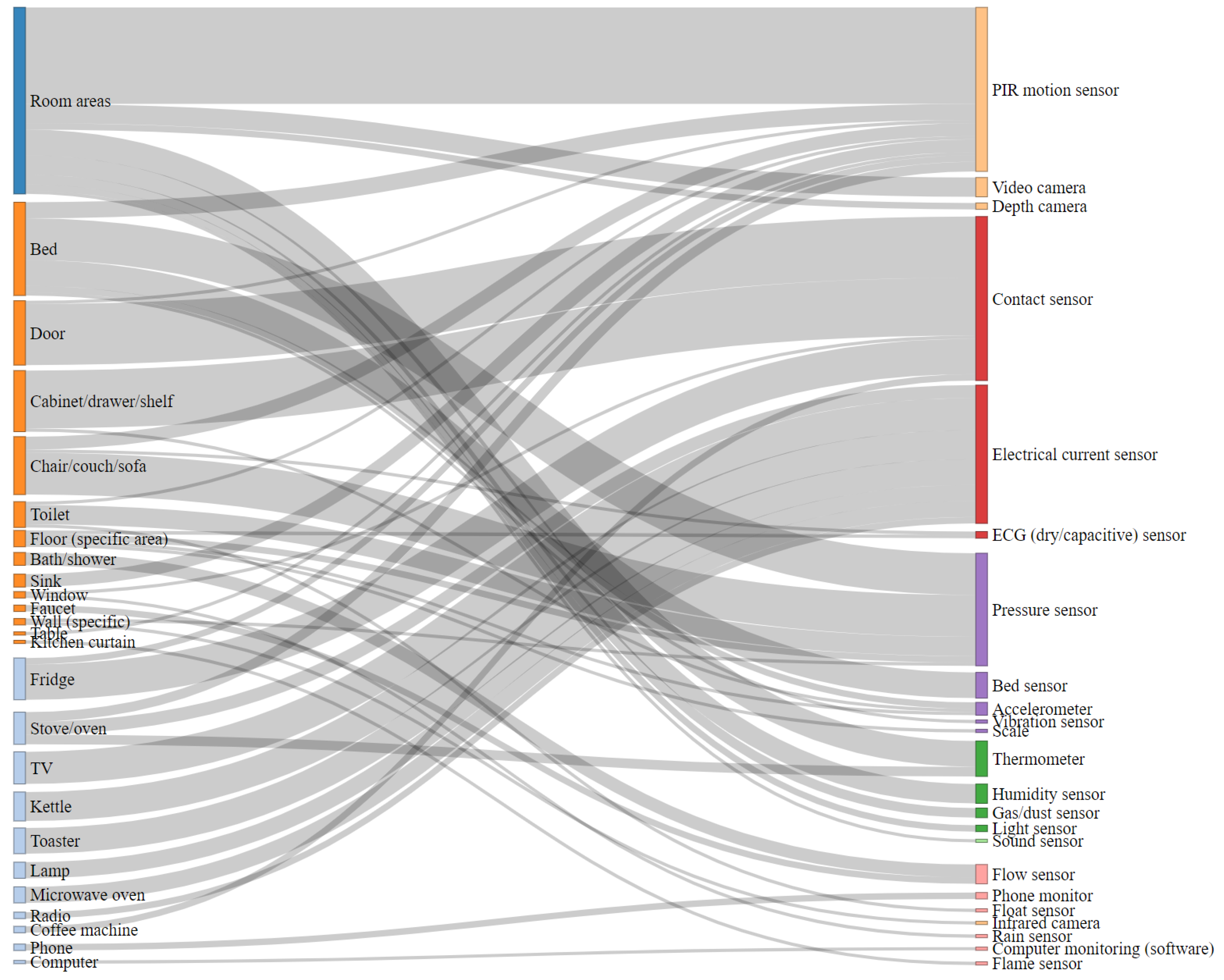
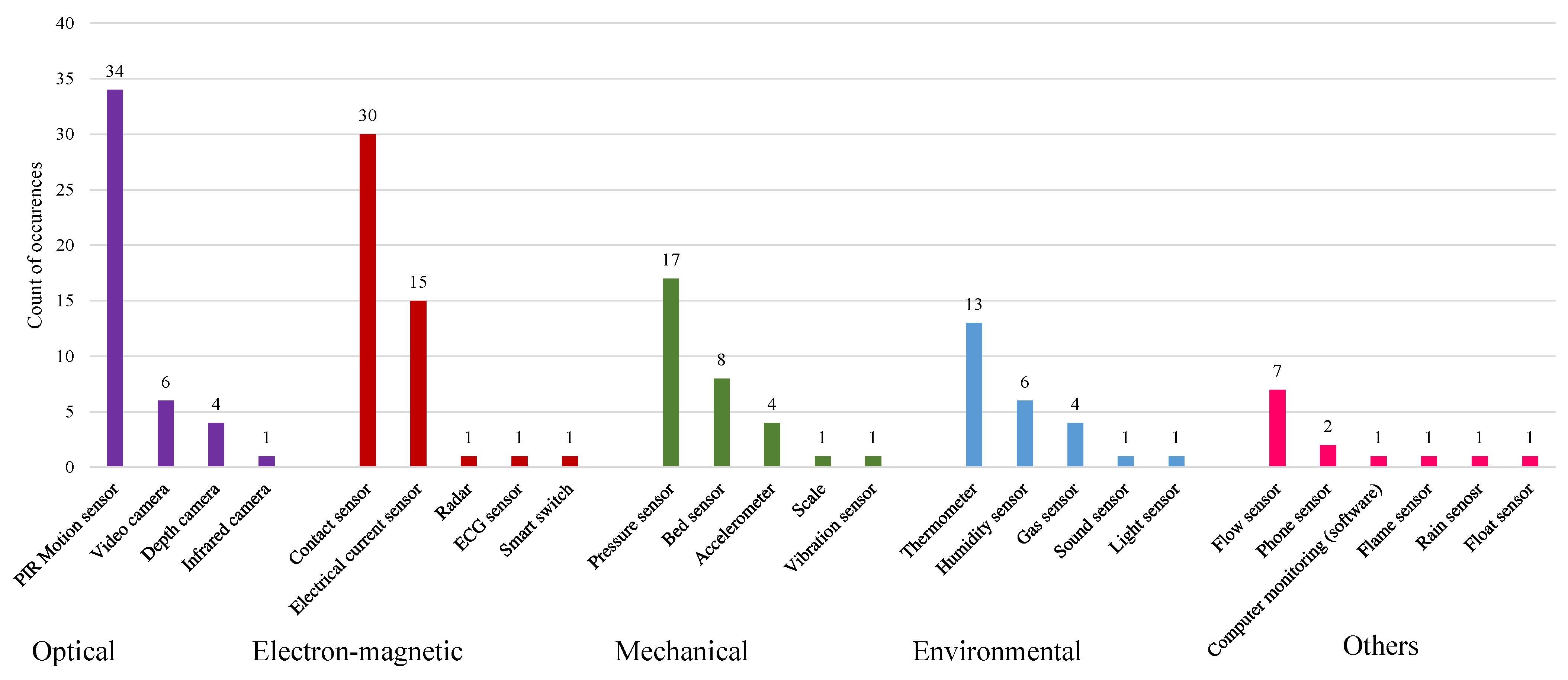
A Sankey diagram [79] provides an overview of the connections between sensors and their locations (Figure 3). We found a total of 25 types of sensors in the 55 included papers. Passive infrared (PIR) motion sensors, contact sensors, pressure sensors, and electrical current sensors were the most popularly reported sensing devices, which can be found in 34, 30, 17 and 15 papers, respectively (Figure 4). Many studies used these sensors to monitor human behavior, such as presence and time spent on activities (time on) [26,37,50,60,62,64,76,77,78]. For instance, PIR motion sensors frequently monitored presence in certain room areas. In some cases, however, the motion sensors also detected presence at some specific locations, e.g., stove/oven, toilet, sink, and table/desk [27,60,64,78]. In line with their working principle, contact sensors mostly detected the operations on facilities with doors, such as fridges, shelves, cabinets, and windows [24,51]. Pressure sensors were usually attached to the objects that can undergo pressure due to human’s standing, sitting, or lying. Furniture such as a chair/couch/sofa and bed are the common locations for this kind of sensor [26,41,43,71,76]. As an electrical current sensor detects electric current, we could monitor any electric appliance in theory. In the included work, stoves/ovens and water kettles, which can indicate nutrition activities, were of particular interest [33,47,62,73]. Besides PIR motion sensors, video cameras and air-relevant sensors also monitored room areas [34,35,48,56]. Some research designed customized sensors to monitor the operations of some specific objects. For instance, water flow sensors monitored the use of water supply facilities, a phone integrated with a monitor component monitored its usage, and similarly, monitoring software recorded the computer users’ activities [25,45,50,51]. In addition, we also observed that wearable sensors were also in use in combination with ambient sensors in 10 included papers. The wearable devices are frequently embedded with accelerometers [69,75,76] and radio-frequency identification (RFID) tags [44].
3.2. Data
We obtained 20 data types through the introduced combinations of sensors and locations. In line with the sensor occurrence distribution (Figure 4), behavioral data were the most common outputs, with the presence being the most frequent data type (). As the sensors that can detect human–object contact shall deliver presence information, the setups for detecting presence typically included optical sensors, such as PIR motion sensors; contact sensors; and mechanical sensors, such as pressure sensors, accelerometers, and bed sensors. Based on presence data, the time spent on activities was also frequently derived in behavior monitoring (). Besides, a customized placement design of PIR motion sensors estimated the specific metric, the walking speed [27]. Surprisingly, we found rare research on unobtrusively collecting physiological data collection (). Dry or capacitive electrodes appeared to be an alternative solution for capturing ECG signals, from which the heart rate was derived [53]. The body weight (body mass) can be easily measured through a pressure sensor [26]. Besides, research has also derived the blood pressure from the ballistocardiograph (BCG) signal through a pressure sensor [53]. A bed sensor, as an integrated sensor system, successfully delivered heart rate and respiration rate [52]. In room areas, environmental sensors and microphones measured environmental parameters such as gas concentration and sound level, which were used for in-door positioning [48,56].
3.3. Monitoring Functions
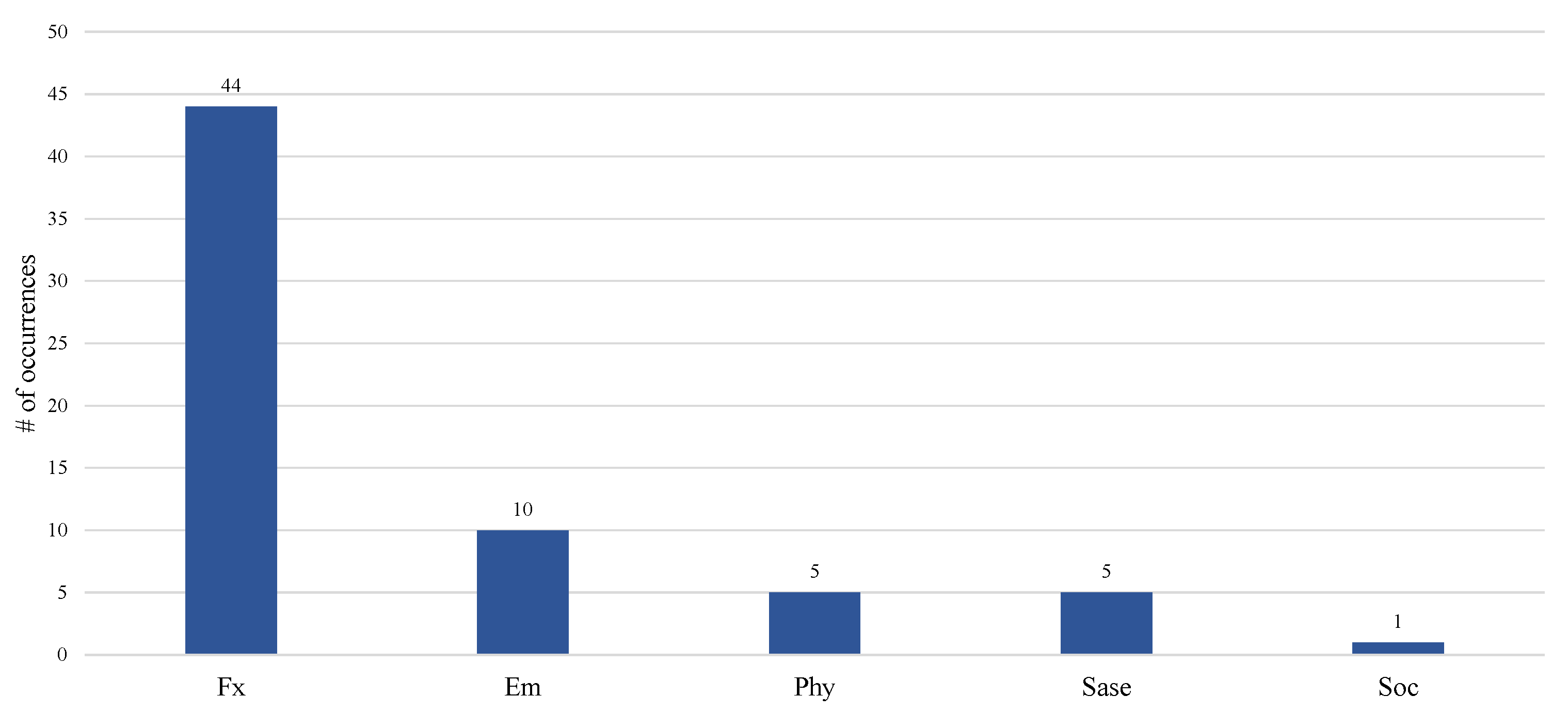
Most included work focused on functional monitoring (). Only a few covered emergency monitoring (), physiological monitoring (), safety and security monitoring (), and social interaction monitoring () (Figure 5). Intuitively, functional monitoring needed behavioral data, including presence, time spent on activities, walking speed, gait parameters, and time spent out of home. Emergency monitoring relied on video/images, presence detection, and abnormal detection of harmful gas concentrations [29,34,35,61]. Safety and security monitoring used environmental data and presence at the entry door [38,43,48,70]. Only one paper covers the social interaction, in which the phone and computer usage was monitored as the indicator [50].
3.4. Sensor Network
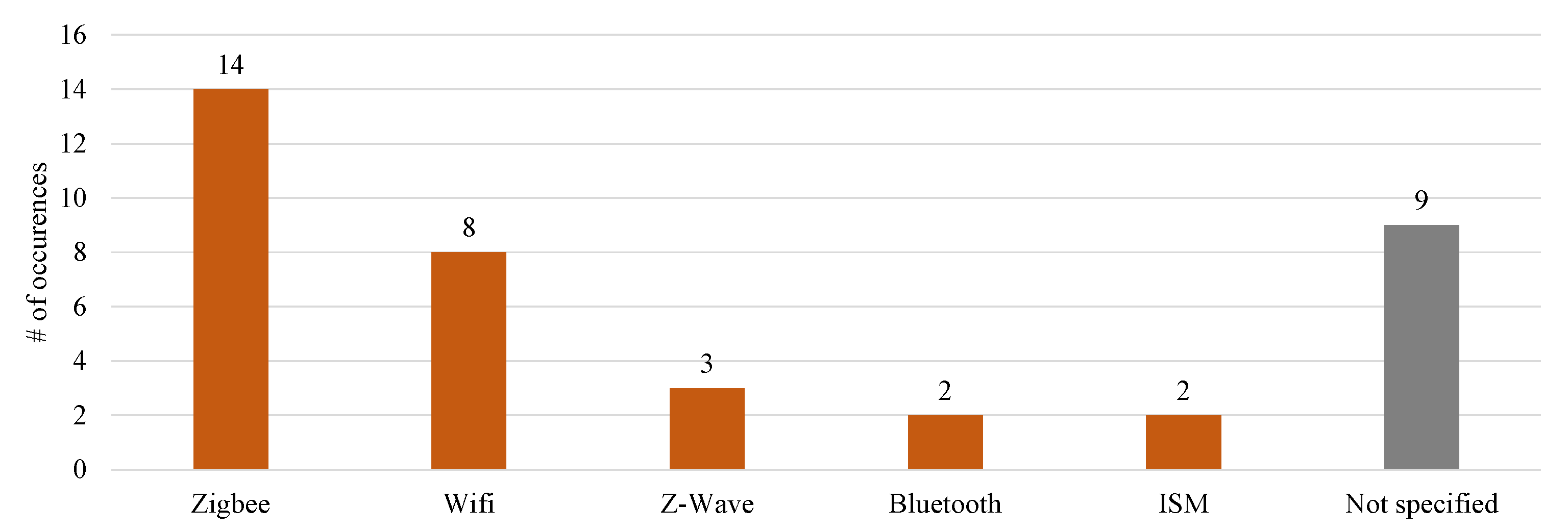
As multiple sensors were used, most works set up a sensor network () for data transmission, for which 37 papers applied wireless communication. The presented wireless communication protocols include Zigbee, WiFi, Z-Wave, Bluetooth, and ISM bands, found in 14, 8, 3, 2, and 2 papers, respectively (Figure 6).
3.5. Subjects and Experimental Settings
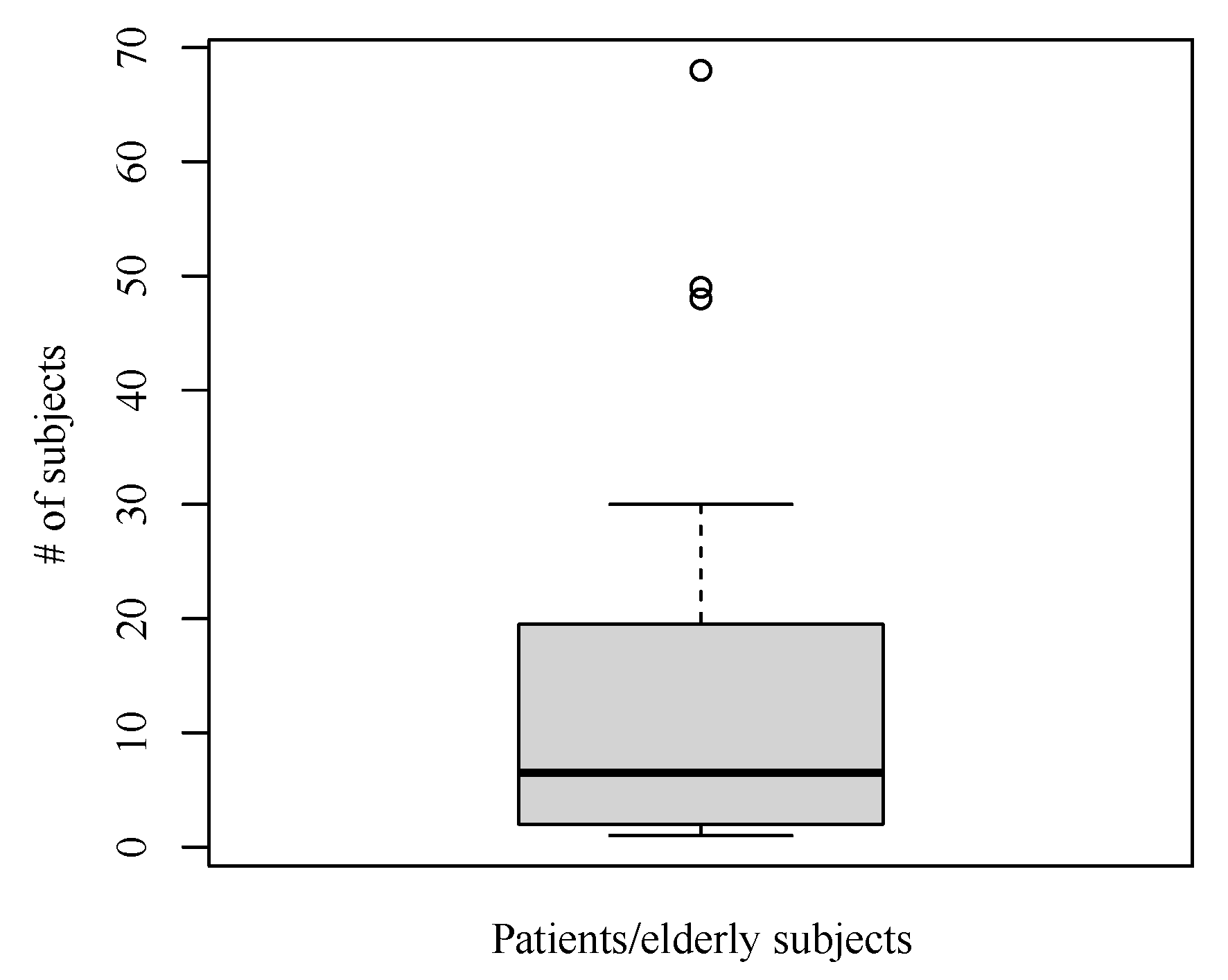
The majority of studies () recruited patients or elderly, whereas some only tested their system with healthy volunteers, e.g., students or developers themselves. Among the research with patients or elderly adults, the number of subjects ranged from one to 265 [27]. The average number was 13.64 without considering the outlier 265 (Figure 7). The 25% and 75% quantiles were 2.0 and 19.25, respectively. Most of the research with patient or elderly adults deployed the monitoring systems in real homes. Only three were used in smart home laboratories. Besides general aging issues, the diseases involved in the included papers were dementia, heart disease, and stroke [26,52,53,60,73,77].
Overall, most research adopted real home settings (), either with real patients/elderly adults or healthy volunteers. The monitoring duration in real homes was much longer than in smart home laboratories. In real home settings, some papers () reported that the monitoring duration was between one month and one year, while several lasted longer than one year (). In contrast, for the research conducted in smart home laboratories, only one exceeded one month, and the rest were up to one week.
3.6. Privacy Issues
Only less than half () of the included papers mentioned privacy issues. Cameras were referred to in several papers as invasive monitoring [37,38,40,54]. Due to the intruding of privacy, some actions were taken regarding sensor selection and sensor placement. Some cases did not take cameras or vision sensors into account [30,31,33,38]. Due to privacy, the toilet could be sensor-free [72]. For data security, some research has adopted different solutions: raw data were not transmitted [35,76], a sensor network was isolated [42], data transmission was encrypted [50], and data access was authorized [40,43].
3.7. Data Sources
Despite most research collecting data using their own monitoring systems, a few () applied their algorithms on existing datasets [24,30,36,41,55,64,68,74]. The reused external datasets are (i) MavHome and CASAS dataset [80,81] (), (ii) the MIT dataset [82] (), (iii) ORCATECH dataset [27] (), and (iv) TigerPlace dataset [83] ().
4. Discussion
To sample relevant literature, in this work, we performed a search with a limited search space on four databases, namely, ACM Digital Lib, IEEE Xplore, PubMed, and Scopus, for acquiring the work in the field of in-home health monitoring published in the past decade. This search strategy might not be able to provide an exhaustive and comprehensive literature coverage; however, we assume that the sampled literature adequately reflects the current state of the research on the topic of unobtrusive health monitoring in smart homes. The high sensitivity of this retrieval strategy is indicated by the fact that approximately 6% of the initially returned records were included for in-depth text analysis (55/912 = 6.03%). We developed a structured terminology for unobtrusive in-home health monitoring (Figure 1). Based on the terminology, we reviewed the included literature in a structured manner. Returning to the initial questions proposed at the beginning (Section 1), we answer them as follows:
- What types of sensors can be used for unobtrusive in-home health data acquisition? To unobtrusively monitor behavior, we can use PIR motion sensors, contact sensors, pressure sensors, and electrical current sensors. Bed sensor systems (respiration rate and heart rate) and dry or capacitive electrodes (ECG, heart rate) are the alternatives to unobtrusively deliver physiological parameters. Apart from that, force-based sensors cal also acquire physiological parameters such as heart rate or blood pressure that can be derived from BCG. Gas sensors, humidity sensors, thermometers, and microphones can be easily unobtrusively deployed for environment monitoring.
- Where should the sensors be placed? Electric appliances and static facilities are the positions for unobtrusively placing the sensors. When monitoring room areas, PIR motion sensors or other optical sensors, and environmental sensors should be placed at appropriate locations according to the sensor fact data. To monitor the presence at a specific location, (i) the facilities with doors are the locations best used to attach contact sensors; (ii) the power supply (e.g., plugin) of a monitored appliance must be able to sustain an electrical current sensor; (iii) a pressure sensor must be beneath the area where force is applied when standing, sitting, walking, or lying; (iv) a position from which a PIR motion sensor can point at the monitored location must be determined to place the sensor according to its fact data. To monitor certain physiological parameters such as heart rate or respiration rate, the positions (e.g., chair and bed) where a person maintains stable contact with the body are appropriate for attaching dry or capacitive electrodes. In this case, acceptable textile layers are the precondition. These locations also qualify for BCG sensors.
- What data can be monitored in the smart home? Behavioral data (presence, time spent on activities, activity level) can be easily acquired through the ambient, sensors such as motion, contact, and pressure sensors. Human functional data such as gait velocity and step time can be derived from depth videos. By customizing the placement of PIR motion sensor, the walking speed can also be estimated. Even though physiological parameters cannot be unobtrusively obtained as easily as behavioral data, heart rate can be derived from BCG (pressure sensor, bed sensor) or ECG (dry or capacitive ECG electrodes), respiration rate can be delivered by bed sensors, and body temperature from an infrared thermometer. Air-relevant and sound sensors can offer environmental data, such as gas concentrations, humidity, and sound level.
- How can the obtained data support the monitoring functions? All five functional categories can be supported by the data from unobtrusive in-home health monitoring systems. Functional monitoring is the easiest one to implement as the variety and the readiness of sensor technology for behavioral monitoring. Emergency monitoring can be built up on behavioral data (e.g., in-door positioning, time-spent on activities, and activity level) and environmental data (e.g., gas level). The physiological data (BCG or ECG) collected from the objects with stable contact (e.g., bed and chair) can deliver heart rate and respiratory rate, leading to partly physiological monitoring. Besides contributing to functional and emergency monitoring, environmental data and behavioral data detect safety and security abnormalities. Social interaction monitoring relies mainly on monitoring social interaction tools, such as phones and computers.
4.1. Implications of In-Home Health Monitoring Terminology
The developed terminology of unobtrusive in-home health monitoring (Figure 1) was applied to the structured text analysis in the current work. We expect to generalize the text analysis mechanism to future relevant work. It may serve as a basis for developing a guideline for sensor deployment in this context. Furthermore, it may assist in designing a monitoring system and analyzing it comprehensively. As technology is continuously being developed in sensors and computing, the terminology remains open, and new entries can be added to any dimension.
4.2. The Demand for Customized and Hybrid Sensor Technology
Even though many efforts have explored different sensors for in-home health monitoring, many sensors in use, however, are not originally designed for health monitoring. For example, PIR motion sensors are designed initially for presence detection [84], and basic home automation functions like switching on/off lights according to the presence. They may have either blind spots or overlaps in the sensing areas when used for behavioral monitoring, downgrading their value for health monitoring. The sensor systems dedicated designed for unobtrusive health monitoring such as the EarlySense bed sensor [52] are still in demand. Mature products are very likely to improve user experience and enable reliable outputs. Smart building developments will enrich the variety of such simple and non-health-focused sensors, which can yet be used to extract health-related data by sensor fusion. In addition to the static objects that were on the focus of this work, ambient sensors may also be embedded in the mobile objects on which some special groups continuously rely in daily life, for instance, the wheelchairs and crutches for disabled individuals [85,86]. Hence, the monitoring might be extended to other private spaces, such as a smart vehicle [7], and beyond private spaces.
4.3. Wearables as Complements to Ambient Sensors
We focused on ambient (non-wearable) sensors that can collect data in an unnoticeable way in this work. Some cases, however, involved wearable sensors as well. For instance, activity monitoring task frequently adopts wearable accelerometers, which can deliver more precise results (e.g., activity level) than ambient sensors [69,75,76]. RFID tag may address the issue of distinguishing multiple individuals under monitoring [44], especially when cameras are absent. Although the ambient sensors have certain advantages, they are also more sensitive to external noise [87]. Given the limited scale of research on physiological monitoring, wearable sensors are advantaging in doing the task. For instance, the commercially available smart watches, smart wristbands (e.g., Jawbone and Fitbit), and smart rings (e.g., Aura) integrated with a photoplethysmogram (PPG) sensor can deliver heart rate, heart rate variability (HRV), respiratory rate, and body temperature [18,88]. Therefore, in current stage, a combination of both types of sensors would be logical if the effort to use wearable sensors can be kept at a minimal level.
4.4. The Demand for Appropriate Data Interpretation and Medical Value
In-home health monitoring involves a variety of sensors (Section 3.1) and delivers rich data (Section 3.2). Our results reveal that the majority of research focused on functional monitoring of the elderly or the patients with mental health problems such as Alzheimer’s disease (AD), for whom behavioral changes reflect health status (Section 3.3). Only a few () papers involved patients with heart disease for whom monitoring physiological parameters (e.g., heart rate) is necessary. The phenomenon might be caused by the difficulty of unobtrusively monitoring physiological parameters, as shown in the results (Section 3.2). Physiological, behavioral, and environmental data are the directly obtainable data. Psychological data or information can be derived from physiological and behavioral data and be affected by environmental factors. Finding a common approach to interpret different sensor data is unfeasible. However, linking the categorized sensor data to the scales of clinical instruments might be possible.
So far, studies with a large sample size and long-term monitoring were rarely conducted (Section 3.5). Convincing evidence for the impact of in-home health monitoring on clinical outcomes is still lacking. However, we identified, despite the limited sample size, recent studies showing promising clues in the direction of evidence, particularly in supporting cognitive impairment. Lussier et al. found that the measures based on sensor-based observations (motion, contact, and electric sensors) associated with daily functional performance of older adults and concluded that sensor technology hold potential in detecting MCI [73]. By conducting an observational study, Lazarou et al. concluded that unobtrusive health monitoring has positive impact on guiding intervention to the caring of patients with cognitive impairment [76]. As some disease progression can be slow, randomized clinical trials aiming to demonstrate improved patient health outcomes shall be conducted for many years to reach statistical significance [89]. We encourage evidence-oriented research to offer meaningful medical values of unobtrusive in-home health monitoring [90].
4.5. Wireless vs. Wired Sensor Networks
Wireless communication is a dominant approach to form a sensor network (Section 3.4). Many advantages make wireless communication superior, such as simplified installation, flexibility to the building structure, low costs, and good support for IoT sensors. While all of these advantages popularize wireless sensors, short-term projects (like pilot studies) do not allow permanent installation in scales of building usage duration (typically 30 years). Therefore, wired sensors come into play. They allow an efficient and unobtrusive long-term integration of a broad range of sensors and actuators with the reliability needed by health-related applications and the scalability required for large and long-term trials [91]. A hybrid model would bring both into full play. Secondarily using existing sensors, installed by housing companies or homeowners for comfort or safety and security reasons, to collect in-home health data [92], and then fusing with wearable sensor data, could be a realistic model.
4.6. The Demand for Open Data Sources
We also observed that some papers were based on publicly accessible datasets. In contrast to the open data availability in public health or bioinformatics, there are still rare datasets of in-home health monitoring shared within the research community. The reason for that is evident: Collecting sensor data in the real life of patients or the elderly is expensive, particularly, from the perspective of time. The secondary usage of existing data shall be encouraged to promote the advancement, above all, in developing machine learning methods. Open data policy in levels could be a feasible approach. For example, some datasets in MavHome/CASAS are free to download, whereas some can only be accessed by proposing an application [93]. To ensure the usability, open data sources must provide well-defined and de-identified metadata as well.
4.7. On Data Processing
This work focused on giving an overview of sensor technology and measured health-relevant data in state-of-the-art unobtrusive health monitoring applications. However, we did not focus on the processing techniques when extracting the health information from the measured data. The reason for that lies within the fact the majority of works focuses on sensor data collection and on data processing only to a lesser extent. This is underlined by the fact that 20% of works did not report on the data processing technique. Therefore, there is no clear picture of the used techniques for data processing. In some cases, straightforward techniques (thresholds, frequency distributions, distance functions) or statistical measures (nearest neighbor, linear regression) are applied. Rare cases used machine learning techniques, such as support vector machines and recurrent neural networks. Their dependence on training data, which are costly and time-consuming to acquire in the unobtrusive health monitoring, could explain the fact.
To our knowledge, physiological data collection in unobtrusive in-home monitoring is usually over a long-term. Meanwhile, real life introduces noise sources (e.g., movements), resulting in low signal quality. Data quality assessment methods are required. Therefore, collecting high-quality, large-scale training data in an open format that allows mapping this data to other projects effortlessly is an avenue for future work.
4.8. On Privacy Issues
Last but not least, privacy issues are unavoidable in implementing health monitoring in a private space. Sensors that can intrude privacy shall be avoided. In the papers in this work, a video camera was not used in any research that has done monitoring for longer than a month in real homes. However, a depth camera could be an alternative sensor to balance privacy protection and the richness of delivered information. Only less than half of the included papers considered privacy issues, which may also explain the general few numbers of subjects and short duration of monitoring (Section 3.5). In a design stage, the well-known Fair Information Practice Principles may serve as a guideline or reference for protecting privacy, including seven principles on openness and transparency, individual participation, collection limitation, data quality, use limitation, reasonable security, and accountability [94,95]. Additionally, the Model for the Ethical Evaluation of Socio-Technical Arrangements (MEESTAR) [96] offers a structured way to identify ethically problematic effects.
5. Final Remarks
- The terminology of unobtrusive in-home health monitoring enables a structured analysis of health monitoring in the smart home environment, and may contribute to guiding sensor deployment in in-home health monitoring, designing a monitoring system, and analyzing it comprehensively.
- Locations in a home environment, categorized into room areas, electric appliances, and static facilities, can unobtrusively hold a diversity of sensors (mechanical, electro-magnetic, optical, etc.).
- While behavioral data can be easily acquired, only limited types of physiological parameters are unobtrusively measurable. Physiological sensor technology needs to be further developed to enable more reliable outputs for an ambient placement.
- A combination use of the sensor data makes the smart home a platform for functional, emergency, physiological, safety and security, and social interaction monitoring.
- Convincing proof of a clear effect of these monitoring functions on some clinical outcome using a large sample size and long-term monitoring is still lacking. Sensor data need to be interpreted with corresponding medical concerns to obtain insights.
- Open data policies in this research field should be encouraged to enrich the available data to develop and evaluate new methods.
- Privacy issues must be guided by frameworks that are convincing for multiple stakeholders for the sake of long-term monitoring in practice.
Author Contributions
Conceptualization, J.W. and T.M.D.; methodology, J.W. and T.M.D.; literature review, J.W., N.S., J.M.W., M.H. and J.S.; writing—original draft preparation, J.W., N.S., J.M.W., M.H. and J.S.; writing—review and editing, J.W., N.S., J.M.W., M.H., J.S. and T.M.D.; visualization, J.W. and N.S.; supervision, T.M.D.; All authors have read and agreed to the published version of the manuscript.
Funding
Open Access funding was provided by the Open Access Publication Funds of the Technische Universität Braunschweig.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AAL | Ambient Assisted Living |
| AD | Alzheimer’s Disease |
| ADLs | activities of daily living |
| BADLs | basic ADLs |
| BCG | ballistocardiograph |
| CASAS | Center for Advanced Studies in Adaptive Systems |
| CO | carbon monoxide |
| COPD | chronic obstructive pulmonary disease |
| CO2 | carbon dioxide |
| ECG | Electrocardiography |
| Em | Emergency detection |
| GPRS | General Packet Radio Service |
| HRV | heart rate variability |
| IADLs | instrumental ADLs |
| IoT | Internet of Things |
| ISAAC | Intelligent Systems for Detection of Aging Changes |
| ISM | industrial, scientific and medical |
| LAN | local area network |
| MCI | Mild Cognitive Impairment |
| MEESTAR | Model for the Ethical Evaluation of Socio-Technical Arrangements |
| MIT | Massachusetts Institute of Technology |
| NA | not available |
| ORCATECH | Oregon Center for Aging & Technology |
| Phy | physiological monitoring |
| PIR | passive infrared |
| PPG | photoplethysmogram |
| RH | real home |
| RFID | Radio-frequency identification |
| SaSe | safety and security detection |
| SHL | smart home laboratory |
| SoC | social interaction monitoring |
| TV | television |
Appendix A. Search String
Appendix A.1. ACM Digital Lib
(“in-home monitoring OR home monitoring” OR “home-based monitoring” OR “unobtrusive monitoring” OR “continuous assessment” OR “smart home” OR “smart homes” OR “AAL” OR “ambient assisted living” OR “assistive living” OR “aging in place” OR “intelligent monitoring”)
AND
(“patient” OR “patients” OR “disease” OR “diseases” OR “illness” OR “disabled” OR “geriatric” OR “aging” OR “elderly” OR “senior” OR “seniors” OR “older adults” OR “old adults” OR “people with”)
Appendix A.2. IEEE Xplore
(“Document Title”:in-home monitoring OR “Document Title”:home monitoring OR “Document Title”:home-based monitoring OR “Document Title”:unobtrusive monitoring OR “Document Title”:continuous assessment OR “Document Title”:smart home OR “Document Title”:smart homes OR “Document Title”:AAL OR “Document Title”:ambient assisted living OR “Document Title”:assistive living OR “Document Title”:aging in place OR “Document Title”:intelligent monitoring)
AND
(“Document Title”:patient OR “Document Title”:patients OR “Document Title”:disease OR “Document Title”:diseases OR “Document Title”:illness OR “Document Title”:disabled OR “Document Title”:geriatric OR “Document Title”:aging OR “Document Title”:elderly OR “Document Title”:senior OR “Document Title”:seniors OR “Document Title”:older adults OR “Document Title”:old adults OR “Document Title”:people with)
Appendix A.3. PubMed
(in-home monitoring[Title] OR home monitoring[Title] OR home-based monitoring[Title] OR unobtrusive monitoring[Title] OR continuous assessment[Title] OR smart home[Title] OR smart homes[Title] OR AAL[Title] OR ambient assisted living[Title] OR assistive living[Title] OR aging in place[Title] OR intelligent monitoring[Title])
AND
(patient[Title] OR patients[Title] OR disease[Title] OR diseases[Title] OR illness[Title] OR disabled[Title] OR geriatric[Title] OR aging[Title] OR elderly[Title] OR senior[Title] OR seniors[Title] OR older adults[Title] OR old adults[Title] OR people with[Title])
Appendix A.4. Scopus
TITLE ( ( “in-home monitoring” OR “home monitoring” OR “home-based monitoring” OR “unobtrusive monitoring” OR “continuous assessment” OR “smart home” OR “smart homes” OR “AAL” OR “ambient assisted living” OR “assistive living” OR “aging in place” OR “intelligent monitoring” )
AND
( “patient” OR “patients” OR “disease” OR “diseases” OR “illness” OR “disabled” OR “geriatric” OR “aging” OR “elderly” OR “senior” OR “seniors” OR “older adults” OR “old adults” OR “people with” ) )
AND
( LIMIT-TO ( PUBSTAGE , “final” ) ) AND ( LIMIT-TO ( SUBJAREA , “COMP” ) OR LIMIT-TO ( SUBJAREA , “MEDI” ) OR LIMIT-TO ( SUBJAREA , “SOCI” ) OR LIMIT-TO ( SUBJAREA , “NURS” ) OR LIMIT-TO ( SUBJAREA , “HEAL” ) OR LIMIT-TO ( SUBJAREA , “PSYC” ) OR EXCLUDE ( SUBJAREA , “MATH” ) OR EXCLUDE ( SUBJAREA , “BIOC” ) OR EXCLUDE ( SUBJAREA , “ARTS” ) OR EXCLUDE ( SUBJAREA , “ENER” ) OR EXCLUDE ( SUBJAREA , “BUSI” ) OR EXCLUDE ( SUBJAREA , “CENG” ) OR EXCLUDE ( SUBJAREA , “AGRI” ) OR EXCLUDE ( SUBJAREA , “ECON” ) OR EXCLUDE ( SUBJAREA , “EART” ) OR EXCLUDE ( SUBJAREA , “IMMU” ) ) AND ( EXCLUDE ( DOCTYPE , “re” ) ) AND ( LIMIT-TO ( PUBYEAR , 2020 ) OR LIMIT-TO ( PUBYEAR , 2019 ) OR LIMIT-TO ( PUBYEAR , 2018 ) OR LIMIT-TO ( PUBYEAR , 2017 ) OR LIMIT-TO ( PUBYEAR , 2016 ) OR LIMIT-TO ( PUBYEAR , 2015 ) OR LIMIT-TO ( PUBYEAR , 2014 ) OR LIMIT-TO ( PUBYEAR , 2013 ) OR LIMIT-TO ( PUBYEAR , 2012 ) OR LIMIT-TO ( PUBYEAR , 2011 ) OR LIMIT-TO ( PUBYEAR , 2010 ) ) AND ( LIMIT-TO ( LANGUAGE , “English” ) ) AND ( EXCLUDE ( SRCTYPE , “b” ) ) AND ( EXCLUDE ( DOCTYPE , “ch” ) ) AND ( EXCLUDE ( SRCTYPE , “k” ))
References
- Deserno, T.M. Transforming smart vehicles and smart homes into private diagnostic spaces. In Proceedings of the 2nd Asia Pacific Information Technology Conference (APIT 2020), Bali Island, Indonesia, 17–19 January 2020; Association for Computing Machinery: New York, NY, USA; 2020; pp. 165–171. [Google Scholar]
- Steiner, B.; Elgert, L.; Saalfeld, B.; Schwartze, J.; Borrmann, H.P.; Kobelt-Pönicke, A.; Figlewicz, A.; Kasprowski, D.; Thiel, M.; Kreikebohm, R.; et al. Health-enabling technologies for telerehabilitation of the shoulder: A feasibility and user acceptance study. Methods Inf. Med. 2020, 59 (Suppl. 2), e90. [Google Scholar] [CrossRef] [PubMed]
- Mielke, C.; Voss, T.; Haux, R. Residence as a diagnostic and therapeutic area—A smart home approach. Stud. Health Technol. Inform. 2017, 238, 92–95. [Google Scholar] [PubMed]
- Schwartze, J.; Prekazi, A.; Schrom, H.; Marschollek, M. Substitution of assisted living services by assistive technology—Experts opinions and technical feasibility. Stud. Health Technol. Inform. 2017, 238, 116–119. [Google Scholar] [PubMed]
- Consel, C.; Kaye, J. Aging with the Internet of Things. Bridge 2019, 49, 6–12. [Google Scholar]
- Wang, J.; Bauer, J.; Becker, M.; Bente, P.; Dasenbrock, L.; Elbers, K.; Hein, A.; Kohlmann, M.; Kolb, G.; Lammel-Polchau, C.; et al. A novel approach for discovering human behavior patterns using unsupervised methods. Z. Gerontol. Geriatr. 2014, 47, 648–660. [Google Scholar] [CrossRef]
- Wang, J.; Warnecke, J.M.; Haghi, M.; Deserno, T.M. Unobtrusive health monitoring in private spaces: The smart vehicle. Sensors 2020, 20, 2442. [Google Scholar] [CrossRef]
- Rantz, M.J.; Skubic, M.; Popescu, M.; Galambos, C.; Koopman, R.J.; Alexander, G.L.; Phillips, L.J.; Musterman, K.; Back, J.; Miller, S.J. A new paradigm of technology-enabled ‘vital signs’ for early detection of health change for older adults. Gerontology 2015, 61, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, N.B.; Ryan, L.M.; Carrillo, M.C.; Sperling, R.; Petersen, R.C.; Posner, H.B.; Snyder, P.J.; Hilsabeck, R.; Gallagher, M.; Raber, J.; et al. Assessment of cognition in early dementia. Alzheimers Dement. 2011, 7, e60–e76. [Google Scholar] [CrossRef] [Green Version]
- Marschollek, M.; Becker, M.; Bauer, J.M.; Bente, P.; Dasenbrock, L.; Elbers, K.; Hein, A.; Kolb, G.; Künemund, H.; Lammel-Polchau, C.; et al. Multimodal activity monitoring for home rehabilitation of geriatric fracture patients—Feasibility and acceptance of sensor systems in the GAL-NATARS study. Inform. Health Soc. Care 2014, 39, 262–271. [Google Scholar] [CrossRef]
- Son, H.; Kim, H. A pilot study to test the feasibility of a home mobility monitoring system in community-dwelling older adults. Int. J. Environ. Res. Public Health 2019, 16, 1512. [Google Scholar] [CrossRef] [Green Version]
- Demiris, G.; Hensel, B.K. Technologies for an aging society: A systematic review of “smart home” applications. Yearb. Med. Inform. 2008, 17, 33–40. [Google Scholar]
- Majumder, S.; Aghayi, E.; Noferesti, M.; Memarzadeh-Tehran, H.; Mondal, T.; Pang, Z.; Deen, M.J. Smart homes for elderly healthcare—Recent advances and research challenges. Sensors 2017, 17, 2496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Miguel-Cruz, A.; Rincon, A.R. Smart homes and home health monitoring technologies for older adults: A systematic review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef] [PubMed]
- Cedillo, P.; Sanchez, C.; Campos, K.; Bermeo, A. A systematic literature review on devices and systems for Ambient Assisted Living: Solutions and trends from different user perspectives. In Proceedings of the 2018 International Conference on eDemocracy eGovernment (ICEDEG), Ambato, Ecuador, 4–6 April 2018; pp. 59–66. [Google Scholar]
- Rashidi, P.; Mihailidis, A. A survey on Ambient-Assisted Living tools for older adults. IEEE J. Biomed. Health Inform. 2013, 17, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.J.; Postolache, O.; Cercas, F. Physiological and behavior monitoring systems for smart healthcare environments: A review. Sensors 2020, 20, 2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stavropoulos, T.G.; Papastergiou, A.; Mpaltadoros, L.; Nikolopoulos, S.; Kompatsiaris, I. IoT Wearable sensors and devices in elderly care: A literature Review. Sensors 2020, 20, 2826. [Google Scholar] [CrossRef]
- Troyer, A.K. Activities of Daily Living (ADL); Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 28–30. Available online: https://doi.org/10.1007/978-0-387-79948-3_1077 (accessed on 18 June 2020).
- Mlinac, M.E.; Feng, M.C. Assessment of activities of daily living, self-care, and independence. Arch Clin. Neuropsychol. 2016, 31, 506–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, D.T.; Collin, C. The Barthel ADL Index: A standard measure of physical disability? Int. Disabil. Stud. 1988, 10, 64–67. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Peter, L. Reichertz Institute for Medical Informatics. SNOCAP-HET. 2015. Available online: https://www.plri.de/en/forschung/projekte/snocap-het (accessed on 20 June 2020).
- Papamatthaiakis, G.; Polyzos, G.C.; Xylomenos, G. Monitoring and modeling simple everyday activities of the elderly at home. In Proceedings of the 2010 7th IEEE Consumer Communications and Networking Conference, Las Vegas, NV, USA, 9–12 January 2010. [Google Scholar]
- Lázaro, J.P.; Fides, A.; Navarro, A.; Guillén, S. Ambient assisted nutritional advisor for elderly people living at home. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 198–203. [Google Scholar]
- Klack, L.; Schmitz-Rode, T.; Wilkowska, W.; Kasugai, K.; Heidrich, F.; Ziefle, M. Integrated home monitoring and compliance optimization for patients with mechanical circulatory support devices. Ann. Biomed. Eng. 2011, 39, 2911–2921. [Google Scholar] [CrossRef] [PubMed]
- Kaye, J.A.; Maxwell, S.A.; Mattek, N.; Hayes, T.L.; Dodge, H.; Pavel, M.; Jimison, H.B.; Wild, K.; Boise, L.; Zitzelberger, T.A. Intelligent systems for assessing aging changes: Home-based, unobtrusive, and continuous assessment of aging. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66B, i180–i190. [Google Scholar] [CrossRef] [PubMed]
- Gaddam, A.; Mukhopadhyay, S.C.; Gupta, G.S. Trial & experimentation of a smart home monitoring system for elderly. In Proceedings of the 2011 IEEE International Instrumentation and Measurement Technology Conference, Hangzhou, China, 10–12 May 2011. [Google Scholar]
- Lotfi, A.; Langensiepen, C.; Mahmoud, S.M.; Akhlaghinia, M.J. Smart homes for the elderly dementia sufferers: Identification and prediction of abnormal behaviour. J. Ambient. Intell. Humaniz. Comput. 2011, 3, 205–218. [Google Scholar] [CrossRef]
- Novak, M.; Binas, M.; Jakab, F. Unobtrusive anomaly detection in presence of elderly in a smart-home environment. In Proceedings of the 2012 ELEKTRO, Rajeck Teplice, Slovakia, 21–22 May 2012; pp. 341–344. [Google Scholar]
- Suryadevara, N.K.; Mukhopadhyay, S.C.; Rayudu, R.K.; Huang, Y.M. Sensor data fusion to determine wellness of an elderly in intelligent home monitoring environment. In Proceedings of the 2012 IEEE International Instrumentation and Measurement Technology Conference Proceedings, Graz, Austria, 13–16 May 2012; pp. 947–952. [Google Scholar]
- Survadevara, N.K.; Mukhopadhyay, S.C.; Rayudu, R.K. Applying SARIMA time series to forecast sleeping activity for wellness model of elderly monitoring in smart home. In Proceedings of the 2012 Sixth International Conference on Sensing Technology (ICST), Kolkata, India, 18–21 December 2012; pp. 157–162. [Google Scholar]
- Suryadevara, N.K.; Mukhopadhyay, S.C. Wireless sensor network based home monitoring system for wellness determination of elderly. IEEE Sens J. 2012, 12, 1965–1972. [Google Scholar] [CrossRef]
- Brulin, D.; Benezeth, Y.; Courtial, E. Posture recognition based on fuzzy logic for home monitoring of the elderly. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Rhuma, A.; Naqvi, S.M.; Wang, L.; Chambers, J. A posture recognition-based fall detection system for monitoring an elderly person in a smart home environment. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 1274–1286. [Google Scholar] [PubMed] [Green Version]
- Mahnot, A.; Popescu, M. Early illness recognition using in-home monitoring sensors and multiple instance learning. Methods Inf. Med. 2012, 51, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Rantz, M.J.; Skubic, M.; Miller, S.J.; Galambos, C.; Alexander, G.; Keller, J.; Popescu, M. Sensor technology to support aging in place. J. Am. Med. Dir. Assoc. 2013, 14, 386–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alesii, R.; Graziosi, F.; Marchesani, S.; Rinaldi, C.; Santic, M.; Tarquini, F. Short range wireless solutions enabling ambient assisted living to support people affected by the down syndrome. In Proceedings of the Eurocon 2013, Zagreb, Croatia, 1–4 July 2013; pp. 340–346. [Google Scholar]
- Suryadevara, N.K.; Mukhopadhyay, S.C.; Wang, R.; Rayudu, R.K.; Huang, Y.M. Reliable measurement of wireless sensor network data for forecasting wellness of elderly at smart home. In Proceedings of the 2013 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Minneapolis, MN, USA, 6–9 May 2013; pp. 16–21. [Google Scholar]
- Moretti, G.; Marsl, S.; Basu, D.; Sen Gupta, G.; Group TMUSE. Towards a monitoring smart home for the elderly: One experience in retrofitting a sensor network into an existing home. J. Ambient. Intell. Smart Environ. 2013, 5, 639–656. [Google Scholar] [CrossRef]
- Suryadevara, N.K.; Mukhopadhyay, S.C.; Wang, R.; Rayudu, R.K. Forecasting the behavior of an elderly using wireless sensors data in a smart home. Eng. Appl. Artif. Intell. 2013, 26, 2641–2652. [Google Scholar] [CrossRef]
- Eldib, M.; Bo, N.B.; Deboeverie, F.; Xie, X.; Philips, W.; Aghajan, H. Behavior analysis for aging-in-place using similarity heatmaps. In Proceedings of the International Conference on Distributed Smart Cameras (ICDSC ’14), Venezia Mestre, Italy, 4–7 November 2014; Association for Computing Machinery: New York, NY, USA, 2014. [Google Scholar]
- Cavallo, F.; Aquilano, M.; Arvati, M. An Ambient Assisted Living approach in designing domiciliary services combined with innovative technologies for patients with Alzheimer’s Disease. Am. J. Alzheimers Dis. Other Demen. 2014, 30, 69–77. [Google Scholar]
- Osamu, T.; Ryu, T.; Hayashida, A.; Moshnyaga, V.; Sakamoto, D.; Imai, Y.; Shibata, T. A smart system for home monitoring of people with cognitive impairment. In Proceedings of the 2014 IEEE Canada International Humanitarian Technology Conference—(IHTC), Montreal, QC, Canada, 1–4 June 2014. [Google Scholar]
- Lee, M.L.; Dey, A.K. Sensor-based observations of daily living for aging in place. Pers. Ubiquitous Comput. 2014, 19, 27–43. [Google Scholar] [CrossRef]
- Walsh, L.; Doyle, J.; Smith, E.; Inomata, A.; Bond, R. Continuous real-world gait monitoring in community-based older adults. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 3719–3722. [Google Scholar]
- Karakostas, A.; Lazarou, I.; Meditskos, G.; Stavropoulos, T.G.; Kompatsiaris, I.; Tsolaki, M. Sensor-based in-home monitoring of people with dementia using remote web technologies. In Proceedings of the 2015 International Conference on Interactive Mobile Communication Technologies and Learning (IMCL), Thessaloniki, Greece, 19–20 November 2015; pp. 353–357. [Google Scholar]
- Abeledo, M.C.; Bruschetti, F.; Aguilera, G.; Iriso, P.; Marsicano, M.; Lacapmesure, A. Remote monitoring of elderly or partially disabled people living in their homes through the measurement of environmental variables. In Proceedings of the 2016 IEEE Congreso Argentino de Ciencias de la Informática y Desarrollos de Investigación (CACIDI), Buenos Aires, Argentina, 30 November–2 December 2016. [Google Scholar]
- Nienhold, D.; Dornberger, R.; Korkut, S. Sensor-based tracking and big data processing of patient activities in ambient assisted living. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics (ICHI), Chicago, IL, USA, 4–7 October 2016; pp. 473–482. [Google Scholar]
- Austin, J.; Dodge, H.H.; Riley, T.; Jacobs, P.G.; Thielke, S.; Kaye, J. A smart-home system to unobtrusively and continuously assess loneliness in older adults. IEEE J. Transl. Eng. Health Med. 2016, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Radziszewski, R.; Ngankam, H.; Pigot, H.; Grégoire, V.; Lorrain, D.; Giroux, S. An Ambient Assisted Living nighttime wandering system for elderly. In Proceedings of the 18th International Conference on Information Integration and Web-Based Applications and Services (iiWAS ’16), Singapore, 28–30 November 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 368–374. [Google Scholar]
- Bennett, M.K.; Shao, M.; Gorodeski, E.Z. Home monitoring of heart failure patients at risk for hospital readmission using a novel under-the-mattress piezoelectric sensor: A preliminary single centre experience. J. Telemed. Telecare 2016, 23, 60–67. [Google Scholar] [CrossRef]
- Grace, S.L.; Taherzadeh, G.; Chang, I.S.J.; Boger, J.; Arcelus, A.; Mak, S.; Chessex, C.; Mihailidis, A. Perceptions of seniors with heart failure regarding autonomous zero-effort monitoring of physiological parameters in the smart-home environment. Heart Lung. 2017, 46, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Nishida, Y.; Kitamura, K.; Mizoguchi, H. Handrail IoT sensor for precision healthcare of elderly people in smart homes. In Proceedings of the 2017 IEEE International Symposium on Robotics and Intelligent Sensors (IRIS), Ottawa, ON, Canada, 5–7 October 2017; pp. 364–368. [Google Scholar]
- Akl, A.; Snoek, J.; Mihailidis, A. Unobtrusive detection of mild cognitive impairment in older adults through home monitoring. IEEE J. Biomed. Health Inform. 2017, 21, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Kong, W.; Kasai, R.; Gu, Z.; Shiguematsu, Y.M.; Cosentino, S.; Sessa, S.; Takanishi, A. Development of a low-cost smart home system using wireless environmental monitoring sensors for functionally independent elderly people. In Proceedings of the 2017 IEEE International Conference on Robotics and Biomimetics (ROBIO), Macau, China, 5–8 December 2017; pp. 153–158. [Google Scholar]
- Van Kasteren, Y.; Bradford, D.; Zhang, Q.; Karunanithi, M.; Ding, H. Understanding smart home sensor data for ageing in place through everyday household routines: A mixed method case study. JMIR mHealth uHealth 2017, 5, e52. [Google Scholar] [CrossRef]
- Vildjiounaite, E.; Mäkelä, S.M.; Keränen, T.; Kyllönen, V.; Huotari, V.; Järvinen, S.; Gimel’farb, G. Unsupervised illness recognition via in-home monitoring by depth cameras. Pervasive Mob. Comput. 2017, 38, 166–187. [Google Scholar] [CrossRef]
- Demir, E.; Köseoğlu, E.; Sokullu, R.; Şeker, B. Smart home assistant for Ambient Assisted Living of elderly people with dementia. Procedia Comput. Sci. 2017, 113, 609–614. [Google Scholar] [CrossRef]
- Aramendi, A.A.; Weakley, A.; Goenaga, A.A.; Schmitter-Edgecombe, M.; Cook, D.J. Automatic assessment of functional health decline in older adults based on smart home data. J. Biomed. Inform. 2018, 81, 119–130. [Google Scholar] [CrossRef]
- Daher, M.; Najjar, M.E.B.E.; Diab, A.; Khalil, M.; Charpillet, F. Multi-sensory assistive living system for elderly in-home staying. In Proceedings of the 2018 International Conference on Computer and Applications (ICCA), Beirut, Lebanon, 25–26 August 2018; pp. 168–171. [Google Scholar]
- Ghayvat, H.; Mukhopadhyay, S.; Shenjie, B.; Chouhan, A.; Chen, W. Smart home based ambient assisted living: Recognition of anomaly in the activity of daily living for an elderly living alone. In Proceedings of the 2018 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Houston, TX, USA, 14–17 May 2018. [Google Scholar]
- Casagrande, F.D.; Torresen, J.; Zouganeli, E. Sensor event prediction using recurrent neural network in smart homes for older adults. In Proceedings of the 2018 International Conference on Intelligent Systems (IS), Funchal–Madeira, Portugal, 25–27 September 2018; pp. 662–668. [Google Scholar]
- Alberdi, A.; Weakley, A.; Schmitter-Edgecombe, M.; Cook, D.J.; Aztiria, A.; Basarab, A.; Barrenechea, M. Smart home-based prediction of multidomain symptoms related to Alzheimer’s Disease. IEEE J. Biomed. Health Inform. 2018, 22, 1720–1731. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Ghose, A. Unobtrusive and pervasive monitoring of geriatric subjects for early screening of mild cognitive impairment. In Proceedings of the 2018 IEEE International Conference on Pervasive Computing and Communications Workshops (PerCom Workshops), Athens, Greece, 19–23 March 2018; pp. 179–184. [Google Scholar]
- Chatterjee, S.; Byun, J.; Dutta, K.; Pedersen, R.U.; Pottathil, A.; Xie, H.Q. Designing an Internet-of-things (IoT) and sensor-based in-home monitoring system for assisting diabetes patients: Iterative learning from two case studies. Eur. J. Inf. Syst. 2018, 27, 670–685. [Google Scholar] [CrossRef] [Green Version]
- Caroux, L.; Consel, C.; Dupuy, L.; Sauzéon, H. Towards context-aware assistive applications for aging in place via real-life-proof activity detection. J. Ambient. Intell. Smart Environ. 2018, 10, 445–459. [Google Scholar] [CrossRef]
- Paudel, R.; Dunn, K.; Eberle, W.; Chaung, D. Cognitive Health Prediction on the Elderly Using Sensor Data in Smart Homes. In Proceedings of the Thirty-First International Florida Artificial Intelligence Research Society Conference (FLAIRS 2018), Melbourne, FL, USA, 21–23 May 2018; pp. 317–322. [Google Scholar]
- Lach, H.W.; Lorenz, R.A.; Palmer, J.L.; Koedbangkham, J.; Noimontree, W. Home monitoring to track activity and sleep patterns among older adults. Comput. Inform. Nurs. 2019, 37, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Yoo, B.; Muralidharan, S.; Lee, C.; Lee, J.; Ko, H. KLog-Home: A holistic approach of in-situ monitoring in elderly-care home. In Proceedings of the 2019 IEEE International Conference on Computational Science and Engineering (CSE) and IEEE International Conference on Embedded and Ubiquitous Computing (EUC), New York, NY, USA, 1–3 August 2019; pp. 390–396. [Google Scholar]
- Li, H.; Yang, C.; He, Z.; Imran, M.A.; Ahmad, W. Health activities monitoring and warning system for geriatric daily living in extra care homes. In Proceedings of the 2019 IEEE Intl Conf on Dependable, Autonomic and Secure Computing, Intl Conf on Pervasive Intelligence and Computing, Intl Conf on Cloud and Big Data Computing, Intl Conf on Cyber Science and Technology Congress (DASC/PiCom/CBDCom/CyberSciTech), Fukuoka, Japan, 5–8 August 2019; pp. 386–391. [Google Scholar]
- Yun, G.; Kim, K.; Park, S.K.; Kim, D.H. A monitoring system to support home health care for the elderly with dementia by detecting going out activities based on RGB-D sensors. In Proceedings of the 2019 16th International Conference on Ubiquitous Robots (UR), Jeju, Korea, 24–27 June 2019; pp. 71–76. [Google Scholar]
- Lussier, M.; Adam, S.; Chikhaoui, B.; Consel, C.; Gagnon, M.; Gilbert, B.; Sylvain, G.; Manon, G.; Carolg, H.; Hélène, I.; et al. Smart home technology: A new approach for performance measurements of activities of daily living and prediction of mild cognitive impairment in older adults. J. Alzheimers Dis. 2019, 68, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Susnea, I.; Dumitriu, L.; Talmaciu, M.; Pecheanu, E.; Munteanu, D. Unobtrusive monitoring the daily activity routine of elderly people living alone, with low-cost binary sensors. Sensors 2019, 19, 2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botros, A.; Schütz, N.; Camenzind, M.; Urwyler, P.; Bolliger, D.; Vanbellingen, T.; Kistler, R.; Bohlhalter, S.; Müri, R.M.; Mosimann, U.P.; et al. Long-term home-monitoring sensor technology in patients with Parkinson’s Disease—Acceptance and adherence. Sensors 2019, 19, 5169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarou, I.; Stavropoulos, T.G.; Meditskos, G.; Andreadis, S.; Kompatsiaris, I.Y.; Tsolaki, M. Long-term impact of intelligent monitoring technology on people with cognitive impairment: An observational study. J. Alzheimer’S Dis. 2019, 70, 757–792. [Google Scholar] [CrossRef]
- Rogerson, L.; Burr, J.; Tyson, S. The feasibility and acceptability of smart home technology using the howz system for people with stroke. Disabil. Rehabil. Assist. Technol. 2019, 15, 148–152. [Google Scholar] [CrossRef]
- Liu, D.; Meng, L.; Qiu, X.; Feng, H.; Ghayvat, H.; Chen, W. Intelligent home design for elderly health monitoring and rating based wireless passive sensor network. In Proceedings of the BIBE 2019—The Third International Conference on Biological Information and Biomedical Engineering, Hangzhou, China, 20–22 June 2019; pp. 1–5. [Google Scholar]
- Allaire, J.J.; Ellis, P.; Gandrud, C.; Kuo, K.; Lewis, B.W.; Owen, J.; Russell, K.; Rogers, J.; Sese, C.; Yetman, C.J. NetworkD3: D3 JavaScript Network Graphs from R. 2017. Available online: https://cran.r-project.org/web/packages/networkD3/ (accessed on 7 October 2020).
- Cook, D.J.; Youngblood, M.; Heierman, E.O.; Gopalratnam, K.; Rao, S.; Litvin, A.; Khawaja, F. MavHome: An agent-based smart home. In Proceedings of the First IEEE International Conference on Pervasive Computing and Communications, 2003 (PerCom 2003), Fort Worth, TX, USA, 26 March 2003; pp. 521–524. [Google Scholar]
- Cook, D.J.; Crandall, A.S.; Thomas, B.L.; Krishnan, N.C. CASAS: A smart home in a box. Computer 2013, 46, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Tapia, E.M.; Intille, S.S.; Larson, K. Activity recognition in the home using simple and ubiquitous sensors. In Pervasive Computing; Ferscha, A., Mattern, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2004; pp. 158–175. [Google Scholar]
- Fergenson, M. TigerPlace: An innovative ‘aging in place’ community. Am. J. Nurs. 2013, 113, 68–69. [Google Scholar] [CrossRef] [Green Version]
- Mouser Electronics. Panasonic Industrial Devices PIR IR MOTION Sensors. 2019. Available online: https://www.mouser.de/new/panasonic-industrial-devices/panasonic-pir-motion-sensors/ (accessed on 10 October 2020).
- Ma, C.; Li, W.; Gravina, R.; Fortino, G. Activity recognition and monitoring for smart wheelchair users. In Proceedings of the 2016 IEEE 20th International Conference on Computer Supported Cooperative Work in Design (CSCWD), Nanchang, China, 4–6 May 2016; pp. 664–669. [Google Scholar]
- Sesar, I.; Zubizarreta, A.; Cabanes, I.; Portillo, E.; Torres-Unda, J.; Rodriguez-Larrad, A. Instrumented crutch tip for monitoring force and crutch pitch angle. Sensors 2019, 19, 2944. [Google Scholar] [CrossRef] [Green Version]
- Jeffin Gracewell, J.; Pavalarajan, S. Fall detection based on posture classification for smart home environment. J. Ambient. Intell. Human Comput. 2019. [Google Scholar] [CrossRef]
- Kinnunen, H.; Rantanen, A.; Kenttä, T.; Koskimäki, H. Feasible assessment of recovery and cardiovascular health: Accuracy of nocturnal HR and HRV assessed via ring PPG in comparison to medical grade ECG. Physiol. Meas. 2020, 41, 04NT01. [Google Scholar] [CrossRef]
- Haux, R.; Koch, S.; Lovell, N.H.; Marschollek, M.; Nakashima, N.; Wolf, K.H. Health-enabling and ambient assistive technologies: Past, present, future. Yearb. Med. Inform. 2016, 25, S76–S91. [Google Scholar]
- Wang, J.; Wang, J.; Miao, H.; Marschollek, M.; Wolf, K.H.; Lynch, K.A.; Gong, Y. Leveraging aging in place through sensor-enhanced in-home monitoring. Stud. Health Technol. Inform. 2018, 250, 19–23. [Google Scholar]
- Schrom, H.; Schwartze, J.; Diekmann, S. Building automation by an intelligent embedded infrastructure: Combining medical, smart energy, smart environment and heating. In Proceedings of the 2017 International Smart Cities Conference (ISC2), Wuxi, China, 14–17 September 2017. [Google Scholar]
- Schwartze, J.; Schrom, H.; Wolf, K.H.; Marschollek, M. Facilitating inter-domain synergies in Ambient Assisted Living environments. Stud. Health Technol. Inform. 2016, 228, 476–480. [Google Scholar]
- Center for Advanced Studies in Adaptive Systems. WSU CASAS Datasets. 2009. Available online: http://casas.wsu.edu/datasets/ (accessed on 15 October 2020).
- Ruotsalainen, P.; Blobel, B. Digital phealth—Problems and solutions for ethics, trust and privacy. Stud. Health Technol. Inform. 2019, 261, 31–46. [Google Scholar]
- Langheinrich, M. Privacy by design—Principles of privacy-aware ubiquitous systems. In Ubicomp 2001: Ubiquitous Computing; Abowd, G.D., Brumitt, B., Shafer, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2001; pp. 273–291. [Google Scholar]
- Weber, K. Methoden der ethischen Evaluation von IT. In INFORMATIK 2019: 50 Jahre Gesellschaft für Informatik—Informatik für Gesellschaft (Workshop-Beiträge); Draude, C., Lange, M., Sick, B., Eds.; Gesellschaft für Informatik e.V.: Bonn, Germany, 2019; pp. 431–444. [Google Scholar]
Figure 1.
Terminology of unobtrusive in-home health monitoring.

Figure 2.
Review flowchart.

Figure 3.
Connections between sensors and their locations. A wider connection indicates more included papers supporting the connection in this review. The terms in the same category are illustrated in the same color.
Figure 3.
Connections between sensors and their locations. A wider connection indicates more included papers supporting the connection in this review. The terms in the same category are illustrated in the same color.

Figure 4.
Distribution of sensor occurrences.

Figure 5.
Distribution of smart home functions.

Figure 6.
Distribution of wireless sensor networks.

Figure 7.
Distribution of number of patients and elderly adults.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Recent research on in-home health monitoring. NA: not available. RH: real home. SHL: smart home laboratory.
Table 1.
Recent research on in-home health monitoring. NA: not available. RH: real home. SHL: smart home laboratory.
| Ref. | Year | Sensors & Locations | Data | Functions | Sensor Network | Subject Info | Experiment Setting |
|---|---|---|---|---|---|---|---|
| [24] | 2010 | Contact sensor [doors, windows, cabinets, sinks, toilets, and electric/electronic appliances (e.g., ovens & fridge) | Presence (use of objects) | Fx: ADL recognition & monitoring | Yes, wireless, not specified | 2, 30-year and 80-year | RH, 14 days |
| [25] | 2010 | {Thermometer, humidity sensor} [above cooking area], flow-meter [water flowing], contact sensor [shelves, fridge, drawers], motion sensor [kitchen], camera [kitchen ceiling] | Actions and events during cooking, increased/decreased temperature/humidity, position | Fx: ADL and nutritional habits | NA | 1, unkown info | SHL, duration NA |
| [26] | 2011 | Infrared camera [wall in living room], scale [floor], pressure sensor [floor, living room] | Body temperature, body weight, presence | Phy: vital sign monitoring for heart disease patients | Yes, not specified | 28, 13 with heart disease, and 15 healthy | SHL, < 1 hour |
| [27] | 2011 | Motion sensors [room areas, sofa, kitchen area, toilet, bed], contact sensor [(exit/entry) doors, fridge] | Presence, walking speed, out of home (absence) | Fx: Assessment of aging | Yes, wireless, X10 | 265, elderly persons | RH, average 33 months |
| [28] | 2011 | Electrical current sensor [microwave oven, kettle, TV, toaster, bed lamp], pressure sensor[bed] | Time spent on act. (duration of using appliances) | Fx: ADL monitoring for elderly | Yes, Xbee based on Zigbee | 1, healthy volunteer | RH, 24 hours |
| [29] | 2011 | Motion sensor [room areas], contact sensor [front&back doors] | Presence | Em: Abnormal behavior | Yes, not specified | 1, info NA | RH, 1.5 years |
| [30] | 2012 | Motion sensor [room areas] | Presence, time on act. | Fx: Anomaly detection of behavioral patterns | Yes, wired, X10 | 1, healthy volunteer | SHL, 2 months |
| [31] | 2012 | Electrical current sensor [toaster, oven, kettle, TV, lamp], pressure sensor [bed, chair, toilet], contact sensor [fridge, cabinet], water flow sensor [bath] | Presence, time on act. (duration of using appliances) | Fx: Wellness assessment | Yes, ZigBee | 4, elderly | RH, 6 days |
| [32] | 2012 | Electrical current sensor [toaster, oven, kettle, TV, lamp], pressure sensor [bed, chair, toilet], contact sensor [fridge, cabinet], water flow sensor [bath] | Presence, time on act. (duration of using appliances) | Fx: Sleeping activity monitoring, forecasting sleeping tendency | Yes, ZigBee | 1, elderly | RH, 8 weeks |
| [33] | 2012 | Electrical current sensor [toaster, oven, kettle, TV, lamp], pressure sensor [bed, chair, toilet], contact sensor [fridge, cabinet], water flow sensor [bath] | Presence, time on act. (duration of using appliances) | Fx: assessing performance of basic behaviors | Yes, ZigBee | 4, elderly | RH, 6 days |
| [34] | 2012 | Video camera [bed room] | Video of ADL | Em: Fall detection | No | NA, healthy volunteers | RH, duration NA |
| [35] | 2012 | Video camera [living room] | Video of ADL | Em: Fall detection | No | 15, healthy volunteers | RH, duration NA |
| [36] | 2012 | Motion sensor [room areas], bed sensor [bed], thermometer [stove] | Activity level in apt. and in bed (bed restlessness), heart rate (low pulse), respiration rate (low breathing) | Phy: Early illness recognition for older adults | Yes, X10 | 6, elderly | RH, 1 month -– 2 years |
| [37] | 2013 | Thermometer [stove], Doppler radar sensors [NA], depth camera (MS Kinect) [NA], motion sensor [room areas], bed sensor (pneumatic strip) [bed] | Activity level in apt. and in bed (bed restlessness), heat rate (low/high pulse), respiration rate, time on act. (stove usage), gait (velocity and step time) | Fx, Phy: Detect changes in health status | Yes, X10 | 49, 24 discharged, 25 remained | RH, 1 year |
| [38] | 2013 | Smart lamp (motion sensor, thermometer, humidity sensor, gas sensor) [room areas], + wearable (smart watch) | Presence, gas leak, temperature, humidity | Safety/SaSe: for down syndrome | Yes, ISM 868MHz | NA | SHL, 2 days |
| [39] | 2013 | Electrical current sensor [room heater, kettle, toaster, microwave, TV, and dishwasher], pressure sensor [bed, couch, chair, toilet], contact sensor [fridge, cabinet] | Presence, time on act. (duration of using appliances) | Fx: Predicting the quantitative well-being of an elderly | Yes, ZigBee | 1, elderly person | RH, 8 weeks |
| [40] | 2013 | Motion sensor [room areas], contact sensor [cupboard], light sensor [storage, door], thermometer [stove, bathroom], electrical current sensor [kettle, toaster, wash machine], water flow sensor [sink in kitchen & bathroom], humidity [bathroom] | Presence, appliance use, temperature, humidity, brightness | Fx: ADL monitoring | Yes, wireless, proprietary protocol | 1, elderly | RH, duration NA |
| [41] | 2013 | Pressure sensor [bed, toilet, couch, chair], electrical current sensor [TV, heater, kettle, toaster, microwave], contact sensor [cupboard] | Presence, time spent on act. (appliances) | Fx: ADL monitoring | yes, wireless, Xbee (Zigbee-based) | 4, elderly | RH, 10 weeks |
| [42] | 2014 | (Low-resolution) cameras [room areas] | (low resolution) images, similarity heatmaps | Fx: ADL monitoring | Yes, wired, not specified | 1, 80-year, with hearing impairment and walking abnormalities | RH, 14 days |
| [43] | 2014 | Bed sensor [bed], pressure sensor [chair cushion], contact sensor [door], + wearable sensor | Presence (bed, chair, entry/exit) | SaSe & Fx: ADL monitoring of patients with AD | Yes, wireless, ZigBee | 14, patients with AD | RH, duration NA |
| [44] | 2014 | Pressure sensor [carpet in bedroom], contact sensor [door], bed sensor (air pressure sensor) [bed], motion sensor [NA], + wearable (RFID tags) | Presence, out of home, fall | Fx: ADL and emergency monitoring | Yes, Xbee | 6, healthy volunteers | SHL, a few mins |
| [45] | 2014 | {Contact sensor, accelerometer} [cabinet (pill box)], phone sensor [phone], contact sensor [coffee maker] | Presence (medication taking, coffee making), phone usage | Fx: ADL monitoring | Yes, wireless, not specified | Study-1: 2 older women; study-2: 12 older adults, living alone. | RH, 10 months |
| [46] | 2015 | Motion sensor [room areas], contact sensor [doors], bed sensor [bed], + wearable sensors | Activity level (# sensor firings, # of transition between rooms, in-bed movements), time on act. (time spent per location) | Fx: ADL monitoring | Yes, not specified | 7, info NA | SHL, 4 days |
| [47] | 2015 | Video camera [kitchen], electric current sensor [TV, iron, vacuum, cooking devices, boiler, radio], contact sensor [TV, iron, vacuum, fridge door, drug cabinet, drug box], motion sensor [kitchen, bathroom], bed sensor [bed], + wearable (Jawbone) | Images, sleep interruption, out of home, presence | Fx: ADL monitoring | Yes, wireless | 1, 76 years old, female | RH, 3 months |
| [48] | 2016 | Motion sensor [room areas], gas sensor (CO, air quality, smoke) [room areas], humidity sensor [room areas], thermometer [room areas], sound sensor [room areas] | Presence, humidity, temperature, gas concentration (CO level), sound level. | SaSe: detect or prevent domestic emergency/abnormal situations | Yes, Ethernet, WiFi, GPRS | 7, healthy volunteers | RH, 15 days |
| [49] | 2016 | Motion sensors [room areas], + wearable sensors | Presence | Fx: ADL tracking | Yes, Bluetooth | 20, healthy volunteer, 20–79 years | RH, duration NA |
| [50] | 2016 | Motion sensor [room areas], contact sensor [doors], phone sensor [phone], computer (monitoring software) | Out of home, walking speed, phone usage, time on act. (computer) | Soci: assessing/predicting loneliness | Yes, WiFi, USB cable | 16, older adults (>62), living alone | RH, 8 months |
| [51] | 2016 | Motion sensor [room areas], contact sensor [fridge, cabinet], pressure sensor [bed, chair], water flow sensor [valve], electric current sensor [TV, radio] | Presence | Fx: Profile nighttime routines, detecting wandering | Yes, Z-wave, WiFi | 1, healthy volunteer | RH, 3 months |
Table 2.
Recent research on in-home health monitoring (continued). NA: not available. RH: real home. SHL: smart home laboratory.
Table 2.
Recent research on in-home health monitoring (continued). NA: not available. RH: real home. SHL: smart home laboratory.
| Ref. | Year | Sensors & Locations | Data | Functions | Sensor Network | Subject Info | Experiment Setting |
|---|---|---|---|---|---|---|---|
| [52] | 2016 | Bed sensor (EarlySense piezoelectric sensor) [bed, under the mattress] | Heart rate, respiration rate (rapid and shallow respiration duration), activity level | Phy: Assessing change of physiological patterns correlate with readmission | Yes, LAN or WiFi | 30, patients with systolic left ventricular dysfunction, and those with preserved ejection fraction | RH, 640 nights |
| [53] | 2017 | Accelerometer [blanket in bed], pressure sensor [chair, bed, floor tile in bathroom], ECG sensor (capacitive electrodes) [chair at dining table, couch]), ECG sensor (dry electrodes) [floor tile in bathroom], Infrared thermometer [at TV] | ECG, heart rate, respiration rate, weight, body temperature, BCG (at the chair), blood pressure | Phy: perceptions of seniors with heart failure | Yes, wireless, not specified | 26, heart failure, >65 years, living alone | SHL, <1 h |
| [54] | 2017 | pressure sensor (handrail) [wall of hallway to toilet] | Presence, walking speed | Fx: ADL monitoring | No | 1, elderly (88-year) | RH, 14 months |
| [55] | 2017 | Motion sensor [room areas, bed], contact sensor [doors, fridge] | Activity level (activity distribution per location) | Fx: correlation between activity distribution and MCI | Yes, X10 | 68, aged > 70, living independently, some experiencing MCI) | RH, average 3 years |
| [56] | 2017 | Thermometer [room areas], gas sensor (CO2) [room areas], humidity sensor [rooms areas] | Temperature, humidity, gas level (CO2), presence | Fx: Residence position | Yes, WiFi | 1, volunteers | RH, a few hours |
| [57] | 2017 | Motion sensor [room areas], electrical current sensor [stove/oven, kettle, microwave, etc.], accelerometer [bed], contact sensor [doors], water flow sensor (acoustic) [water sink], temperature/humidity sensor [room areas] | Presence, time spent on act., temperature, humidity, out of home | Fx: ADL routine | NA | 5, age > 70 | RH, 181 days |
| [58] | 2017 | Depth camera [room areas] | Depth image, motion trajectory | Fx: ADL monitoring, abnormal detection | NA | 4, elderly, cognitive problem, Parkinson’s disease | RH, 40–78 days |
| [59] | 2017 | Contact sensor [doors, cupboard, toilet flush tank, garderobe, water faucet], pressure sensor [chair, bed], thermometer [oven], motion sensor [bath], light sensor [room areas], flame sensor [kitchen curtain], rain sensor [kitchen window] | Presence, environmental data (light, rain, flame) | SaSe & Fx: ADL monitoring, forgotten situations | Yes, wireless, Xbee | 1, living alone | RH, duration NA |
| [60] | 2018 | Motion sensor [room areas, chairs, bed, stove, sink, and fridge] | Time on act. (cooking, eating, relaxing movements, and hygiene act., night toilet, out of home, sleep), gait (walking distance) | Fx: assessing functional health decline | Yes, ZigBee | 29, older adults, 13 cognitively healthy, 10 at risk of cognitive difficulties, 6 cognitive difficulties | RH, >2 years |
| [61] | 2018 | Depth cameras (MS Kinect) [-], accelerometer (floor tile in kitchen] | Depth images (walking, standing, sitting, falls, position), presence (via accelerometer) | Fx & Em: In-home ADL recognition and tracking, fall detection | Yes, ZigBee | 6, volunteers | SHL, duration NA |
| [62] | 2018 | Motion sensor [door, sink in kitchen], electric current sensor [kettle, rice cooker, microwave, TV] | Time on act. | Fx & Em: ADL monitoring | Yes, wireless 2.4G ISM Bands | 4, elderly | RH, 7 weeks |
| [63] | 2018 | Motion sensor [room areas, bed], contact sensor [doors, drawer, wardrobe], electric current sensor [lamps, TV, coffee machine] | Presence | Fx: ADL prediction to support older adults | Yes, Z-Wave, xComfort | 10, elderly patients | RH, up to 17 weeks |
| [64] | 2018 | Motion sensor [room areas, chairs, bed, stove, sink, and fridge] | Time on act. (cooking, eating, relaxing movements, and personal hygiene activities, night toilet, sleep), out of home, walking distance | Fx: Symptom prediction of AD patients | Yes, ZigBee | 29, older adults, 13 cognitively healthy, 10 at risk of cognitive difficulties, 6 cognitive difficulties | RH, >2 years |
| [65] | 2018 | Motion sensor [room areas], vibration sensor [bed], thermometer [bed room] | Presence, temperature | Fx: Detecting early symptoms of MCI | NA | 50, info NA | RH, 6 months |
| [66] | 2018 | Contact sensor [doors, medicine cabinet], motion sensor [bed room], pressure sensor [couch], photo sensor [TV], + wearable (BodyMedia) | Presence, time spent on act. | Fx: ADL monitoring, adhere to self-management regimens | Yes, wireless, not specified | 2, 82-year old, male; 60-year-old female; both with type II diabetes | RH, 1–2 months |
| [67] | 2018 | Motion sensor [room areas], contact sensor [door, drawer, cabinet], smart switch [electrical appliances] | Presence | Fx: ADL routine | Yes, wireless, not specified | 7, average 82-year | RH, 8 weeks |
| [68] | 2018 | Motion sensor [room areas], contact sensor [doors], thermometer [NA], light sensor [NA] | Presence, time spent on act., activity level | Functional monitoring: ADL monitoring, health prediction | NA | 10, elderly (80–91), five with MCI | RH, a few months |
| [69] | 2019 | Motion sensor [room areas], pressure sensor [chair, bed], contact sensor [door], + wearable sensors | Presence (kitchen, bathroom, hall), time on act. (bed, chair), out of home | Fx: Tracking activity and sleep patterns | Yes, wired, phone lines | 10, female, living alone, average 86.5 | RH, 3 months |
| [70] | 2019 | {Thermometer / air quality (gas) sensor} [room areas], conductive cushion sensors [wheelchair], camera [bed room] | Temperature, humidity, gas concentration (VoC, fine dust, pollution level), presence, images | Em& SaSe: Unsafe situation detection | Yes, WiFi | 1, healthy volunteer | SHL, duration NA |
| [71] | 2019 | Motion sensor [room areas], pressure sensor [slipper, sofa, bed, toilet, chair] | Presence, time on atc. | Fx & Em: ADL monitoring, abnormal activities detection | Yes, WiFi, Bluetooth | 1, healthy volunteer | RH, 48 hours |
| [72] | 2019 | Depth camera (MS Kinect) [room areas] | (Depth) images, presence | Fx and Em: out of home | Yes, wired, not specified | # NA, healthy volunteers | SHL, duration NA |
| [73] | 2019 | Motion sensor [room areas], electric current sensor [coffee maker, toaster], contact sensor [drawer, fridge, cupboards] | Time spent on act. (some areas usage time) | Fx: Measuring the performance of specific tasks | Yes, Z-Wave | 48, 26 cognitive healthy, 22 MCI | SHL, ca. 4 hours |
| [74] | 2019 | (1) Motion sensor [room areas, chairs and bed, stove, sink and fridge]; (2) contact sensor [door, cupboards], pressure sensor [couch, bed, drawer], motion sensor [room areas], water flow sensor [toilet] | Presence (use of obj.) | Fx: ADL monitoring, activity routines | (1) Yes, Zigbee (2) Yes, RFM wireless network | 1, healthy adult | RH, 1 month |
| [75] | 2019 | Motion sensor [room areas], contact sensor [doors], + wearable sensors | Presence | Fx: ADL monitoring patients with Parkinson’s disease | Yes, Zigbee | 4, 2 male, 2 female, age 65–70, PD disease duration 10 - 14 years | RH, 4 weeks |
| [76] | 2019 | Electric current senor [electronic appliances], contact sensor [drug box, water can], motion sensor [room areas], bed sensor [bed], depth camera [NA], + wearable (Jawbone) | Images, depth data, gestures, activities, devices in use, presence, time spent on atc. (sleep), activity level (steps) | Fx: ADL monitoring of patients with cognitive impairment | Yes, wireless, NA | 18, 12 MCI, 6 AD, >70 years | RH, 4–12 months |
| [77] | 2019 | Contact sensor [door], motion sensor [room areas], electric current sensor [NA] | Behavior routine | Fx: ADL monitoring, routine monitoring | Yes, wireless, NA | 19, stroke survivors, 9 female and 10 male, mean age 71 (SD 11) | RH, 8 weeks |
| [78] | 2019 | Motion sensor [bathroom, bed, dining table, desk], thermometer [hallway] | Presence (sleep, meal, TV) | Fx: ADL monitoring | Yes, Wifi | 1, female, 68 years | RH, 5 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wang, J.; Spicher, N.; Warnecke, J.M.; Haghi, M.; Schwartze, J.; Deserno, T.M. Unobtrusive Health Monitoring in Private Spaces: The Smart Home. Sensors 2021, 21, 864. https://doi.org/10.3390/s21030864
AMA Style
Wang J, Spicher N, Warnecke JM, Haghi M, Schwartze J, Deserno TM. Unobtrusive Health Monitoring in Private Spaces: The Smart Home. Sensors. 2021; 21(3):864. https://doi.org/10.3390/s21030864
Chicago/Turabian StyleWang, Ju, Nicolai Spicher, Joana M. Warnecke, Mostafa Haghi, Jonas Schwartze, and Thomas M. Deserno. 2021. "Unobtrusive Health Monitoring in Private Spaces: The Smart Home" Sensors 21, no. 3: 864. https://doi.org/10.3390/s21030864
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.